ACS Resources
Acute Care Surgery information
- Acute Care Surgery Performance Improvement
- Fellow Resources
- WELLNESS/RESILIENCY RESOURCES DOCUMENT
- DIVERSITY, EQUITY, AND INCLUSION RESOURCE DOCUMENT
- ACGME Competencies and UNMC Scholarly Activities
- Preventing Physician Depression and Suicide
- Physician Impairment and Substance Use Disorder
- Resident Resources
- ACS Roles & Responsibilities (2025-2026)
- ACS Clinic Referral Patterns
- Trauma orientation manual
- ACS First Start OR Protocol
- AGAC-NPs Caring for Pediatric Trauma Patients
Acute Care Surgery Performance Improvement
Acute Care Surgery Performance Improvement Form

Fellow Resources
WELLNESS/RESILIENCY RESOURCES DOCUMENT
The University of Nebraska Medical Center has several resources in place to address workplace stress, burnout, depression and suicide. These resources will be useful in proactively identifying any colleagues exhibiting any signs and symptoms of burnout, depression or suicidality, referring them to the appropriate personnel and thereby improving wellbeing.
AVAILABLE RESOURCES AND ACCESSIBILITY:
On Campus
| Resource |
Contact |
| Susan Smith, RN, BS, CEAP House Officer Assistance Program (HOAP) Manager Available 24/7 by phone- unlimited access, no payment. Susan Smith works exclusively with house officers. |
-402.689.1033 (Mobile) Call or text -402.559.5323 (Office) |
| Arbor Family Counseling- available 24/7 by phone- At UNMC or offsite- 5 free sessions | -402.330.0960/1.800.922.7379 -For Offsite: Web-Ex (HIPAA compliant) via smartphone/tablet or computer -www.arborfamilycounseling.com |
| UNMC Counseling in Bennet Hall- 6th floor David Carver Ph.D, 24/7/Unlimited access/No payment |
-402.559.7276 -402.203.0592 (after hours) |
| Spiritual Care at UNMC A chaplain is available for spiritual counsel, emotional support, prayer, or a nonjudgmental presence while you work through a concern or worry. | To reach spiritual care Monday through Friday, 8 a.m. to 4:30 p.m., please call the main office at 402.552.3219. After hours, call the on-call Chaplain at 531.557.4559 |
| Peers in Need of Support (PiNS) Colleagues are matched with one of our behavioral health responders, made up of Nebraska Medicine and UNMC psychologists, psychiatrists, social workers, marriage and family therapists, staff chaplains and other trained staff. This is not a formal evaluation or treatment, but a supportive peer to listen, offer suggestions, share resources and make referrals when needed. | Complete this confidential form or email pins@nebraskamed.com (Requests for 1:1 support should only be made by colleagues themselves, and not by their peers or supervisors) |
Off Campus
| Resource |
Contact |
| Suicide & Crisis Lifeline (call or text) | 988 |
| Metro Omaha Medical Society anonymous online screening | https://omahamedical.com |
UTILIZATION OF RESOURCES: Susan Smith works exclusively with the house officers. In addition to Susan Smith, other available resources are listed above. After visiting with Susan Smith or other resources, further referrals can be made to Psychiatry services if required.
CONFIDENTIALITY: All UNMC internal resources are kept confidential unless required for health reasons (impairment or imminent danger). The house officers program or department leadership will not be aware of these consultations. If further referrals are made to Psychiatry services, they are covered under HIPAA for confidentiality.
VIGILANCE: We request everyone to be vigilant to identify in self or of any peers demonstrating signs of distress/depression/burnout or suicidal thoughts and refer to the above resources. The attached Powerpoint- “Preventing Physician Depression and Suicide” will help in identifying any individuals at risk.
CRISIS RESPONSE TEAM: The Crisis Response Team (CRT) is available to prevent further tragedies. The CRT will also be activated to develop a coordinated response in the aftermath of any potential tragic events. Please see contact details of CRT personnel in the Appendix.
ADDITIONAL RESOURCES:
- ACGME
- AMA (Steps Forward)
- APA Wellness Resources
- Agency for Healthcare Research and Quality
- SAMHSA-HRSA Wellness Strategies
- Physician Depression and Suicide ppt from UNMC-Psychiatry
- Resilience Webinars
- Other Recommended
- Mindfulness/Anxiety Mobile Apps
-
- Headspace
- 10 percent happier meditation (use the gift code HEALTHCARE)
- Insight Timer (free with thousands of guided meditations)
- PTSD Coach (Not just for PTSD; has numerous relaxation exercised in the Manage Symptoms- Tools section)
- Mindfulness Coach
- CBT-i Coach (cognitive behavioral therapy for insomnia)
-
- Mindfulness/Anxiety Websites
-
- The BHECN Serenity Project- Free Yoga (UNMC)
- Three 2-3 minute lessons on deep breathing (Harvard Vanguard Medical Associates)
- 3 minute body scan (UC Berkeley Greater Good Science Center)
- 5 minute body scan (The Sleepy Aardvark)
-
- Mindfulness/Anxiety Mobile Apps
DIVERSITY, EQUITY, AND INCLUSION RESOURCE DOCUMENT
DIVERSITY, EQUITY, AND INCLUSION (DEI) LEARNING RESOURCES AND TOOLKITS
ACGME Equity Matters: https://www.acgme.org/what-we-do/diversity-equity-and-inclusion/ACGME-Equity-Matters/
ACGME DEI Officers Forum: Email diversity@acgme.org to join
American Academy of Family Physicians Health Equity Curricular Toolkit: https://www.aafp.org/family-physician/patient-care/the-everyone-project/health-equity-tools.html
Association of American Medical Colleges (AAMC) Diversity and Inclusion Video Learning Series: https://www.aamc.org/what-we-do/equity-diversity-inclusion/learning
AAMC Unconscious Bias Resources for Health Professionals: https://www.aamc.org/about-us/equity-diversity-inclusion/unconscious-bias-training
AAMC IDEAS Learning Series: https://cloud.email.aamc.org/ideas
American Hospital Association (AHA) Health Equity Toolkit: https://www.aha.org/toolkitsmethodology/2020-12-14-health-equity-snapshot-toolkit-action
AHA Inclusion Dashboards: https://ifdhe.aha.org/system/files/media/file/2020/12/ifdhe_inclusion_dashboard.pdf
Association of Family Medicine DEI Milestones: https://meridian.allenpress.com/jgme/article-supplement/480333/pdf/jgmed21007231/
American Surgical Association DEI E-textbook: https://americansurgical.org/files/2018/Equity.pdf
American Society for Gastrointestinal Endoscopy LGBTQ+ On-Demand Webinar: https://learn.asge.org/Public/Catalog/Home.aspx?Criteria=26&Option=174&tab=2
Centers for Disease Control (CDC) Health Equity Video Series: https://www.cdc.gov/healthequity/whatis/videos/index.html
CDC Resources and Style Guides for Framing Health Equity and Avoiding Stigmatizing Language: https://www.cdc.gov/healthcommunication/Resources.html
The DEI Shift Podcast Series: https://www.thedeishift.com/
Harvard University Project Implicit: https://implicit.harvard.edu/implicit/research/
Institute for Healthcare Improvement (IHI) Triple Aim Curriculum: https://www.ihi.org/education/ihi-open-school/Pages/Curriculum.aspx
National Institutes of Health (NIH) Advancing Racial Equity: https://www.edi.nih.gov/people/resources/advancing-racial-equity
NIH Scientific Workforce Diversity Toolkit: https://diversity.nih.gov/toolkit
Nebraska Medicine Guide to Understanding Gender Pronouns: https://onfirstup.com/nebraskamedicine/nebraskamedicine/contents/35828486
Ohio State Kirwan Institute Implicit Bias Modules: https://kirwaninstitute.osu.edu/implicit-bias-training
Stanford Unconscious Bias in Medicine CME Course: https://online.stanford.edu/courses/som-ycme0027-unconscious-bias-medicine-cme
READING COLLECTIONS, PODCASTS, PROCEEDINGS, AND BLOGS
• AAMC Diversity, Equity, and Inclusion reading collection: https://www.mededportal.org/dei
• AAMC Anti-Racism reading collection: https://www.mededportal.org/anti-racism
• AAMC Proceedings of the Diversity and Inclusion Innovation Forum: Unconscious Bias in Academic Medicine: https://store.aamc.org/proceedings-of-the-diversity-and-inclusion-innovation-forum-unconscious-bias-in-academic-medicine.html
• CDC Conversations in Equity Blog: https://blogs.cdc.gov/healthequity/
• National Institutes of Health Equity Diversity and Inclusion Blog: https://www.edi.nih.gov/blog
• UNMC podcast on unconscious bias by Dr. Jasmine Marcelin: https://podcasts.apple.com/us/podcast/jasmine-marcelin-md-facp-on-unconscious-bias-being/id1414936358?i=1000479025567
UNMC/NEBRASKA MEDICINE PEOPLE AND RESOURCES
• Shirley Delair, MD, Associate Dean of Diversity, Equity, and Inclusion, is an active member of the GMEC Committee and provides orientation on DEI topics to new house officers. Her office is devising initiatives to enhance recruitment and retention of a diverse workforce.
• Sheritta Strong, MD, Assistant Vice Chancellor of Inclusion, leads the Conversations for Inclusive Excellence virtual series for all UNMC faculty, staff, and students, at 2 PM on the second Thursday of every month. She also leads the UNMC Inclusion and Equity Council, which meets at noon on the fourth Thursday of every month.
• Nada Fadul, MD, Assistant Dean for Diversity, Equity and Inclusion Education Programs, provides faculty development sessions on DEI. She also provides consultative services for graduate medical education programs on addressing DEI in their educational programming.
• Offices of Inclusion and Equity: The UNMC Office of Inclusion focuses on educational and leadership opportunities in a safe environment, particularly in the areas of awareness/advocacy, developmental opportunities, and DEI initiatives. The UNMC Office of Equity focuses on identifying and addressing inequities in a safe environment, particularly in the areas of awareness/advocacy, collation of efforts, and data-based systems. The UNMC community can provide anonymous feedback on culture or report a bias incident at the Offices of Inclusion and Equity website: https://www.unmc.edu/diversity/
• The Office of Faculty Development partners with the Offices of Inclusion and Equity to offer trainings and workshops to UNMC faculty.
• McGoogan Library DEI collections (https://unmc.libguides.com/sb.php?subject_id=203853) on DEI in Ability, in BIPOC communities, and in LGBTQIA2S+ communities
• McGoogan Library inclusive spaces: https://www.unmc.edu/library/spaces/inclusive-spaces.html
• Nebraska Medicine Employee Resource Groups (https://www.nebraskamed.com/diversity-inclusion/employee-resource-groups)
ARTICLES OF NOTE
1. Boatright D, London M, Soriano AJ, Westervelt M, Sanchez S, Gonzalo JD, McDade W, Fancher TL. Strategies and Best Practices to Improve Diversity, Equity, and Inclusion Among US Graduate Medical Education Programs. JAMA Network Open. 2023 Feb 1;6(2):e2255110- https://jamanetwork.com/journals/jamanetworkopen/article-abstract/2801104
2. Gonzaga AM, Appiah-Pippim J, Onumah CM, Yialamas MA. A framework for inclusive graduate medical education recruitment strategies: meeting the ACGME standard for a diverse and inclusive workforce. Academic Medicine. 2020 May 1;95(5):710-6. https://journals.lww.com/academicmedicine/Fulltext/2020/05000/A_Framework_for_Inclusive_Graduate_Medical.20.aspx
3. Usoro A, Hirpa M, Daniel M, Harris V, Ware A, Kernodle A, Elliott T, Piggott DA, Bienstock JL. Promoting diversity, equity, and inclusion: building community for underrepresented in medicine graduate medical education trainees. Journal of Graduate Medical Education. 2021 Feb 1;13(1):33-6. https://meridian.allenpress.com/jgme/article/13/1/33/451599/Promoting-Diversity-Equity-and-Inclusion-Building
4. Capers IV Q. How clinicians and educators can mitigate implicit bias in patient care and candidate selection in medical education. ATS Scholar. 2020 Sep;1(3):211-7. https://www.atsjournals.org/doi/full/10.34197/ats-scholar.2020-0024PS
FOR MORE INFORMATION
An expanded version of this list with additional specialty-specific resources is available in the GMEC Teams folder. If you’re aware of a useful resource, please contact Arianne Marcoux with the UNMC Office of Graduate Medical Education (arianne.marcoux@unmc.edu) to have it added.
ACGME Competencies and UNMC Scholarly Activities
UNMC Graduate Medical Education: Meeting the ACGME Core Competencies
| Competency |
Definition |
UNMC GME |
| Professionalism |
CPR IV.B.1.a) : Residents/Fellows must demonstrate a commitment to professionalism and an adherence to ethical principles. | • COPIC • Annual Compliance Training (Apollo) • Excellence for Building Cultural Differences (annual compliance - Canvas) • HIPAA (annual compliance -Canvas) • Title IX (Orientation and annual compliance – Canvas) • Student Mistreatment (Orientation and annual compliance – Canvas) • Residents as Teachers (Orientation) • Program-specific initiatives and training |
|
Patient Care & Procedural Skills |
CPR IV.B.1.b) : (1) Residents/Fellows must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health. (2) Residents/Fellows must be able to perform all medical, diagnostic, and surgical procedures considered essential for the area of practice. | • Annual Compliance Training (Apollo) • Zero Harm (Orientation) • Institutional Quality Goals/Patient Safety (Orientation) • Infection Control (Orientation) • Program-specific initiatives and training |
| Medical Knowledge |
CPR IV.B.1.c) : Residents/Fellows must demonstrate knowledge of established and evolving biomedical, clinical, epidemiological and social behavioral sciences, as well as the application of this knowledge to patient care. | Program initiatives and training to include • In-training examinations • Journal club • Specialty-specific curricula |
| Practice Based Learning & Improvement |
CPR IV.B.1.d) Residents/Fellows must demonstrate the ability to investigate and evaluate their care of patients, to appraise and assimilate scientific evidence, and to continuously improve patient care based on constant self-evaluation and lifelong learning. | Program initiatives and training to include • Self evaluations • M&M conferences • Journal club |
| Interpersonal & Communication Skills |
CPR IV.B.1.e) Residents/Fellows must demonstrate interpersonal and communication skills that result in the effective exchange of information and collaboration with patients, their families, and health professionals. | • COPIC • Annual Compliance Training (Apollo) • Excellence for Building Cultural Differences (annual compliance - Canvas) • Zero Harm (Orientation) • Residents as Teachers (Orientation) • IHI Module – Teamwork and Communication (onboarding requirement) • Program-specific initiatives and training |
| Systems Based Practice |
CPR IV.B.1.f) Residents/Fellows must demonstrate an awareness of and responsiveness to the larger context and system of health care, including the social determinants of health, as well as the ability to call effectively on other resources to provide optimal health care. | • COPIC • Annual Compliance Training (Apollo) • Zero Harm (Orientation) • Institutional Quality Goals/Patient Safety (Orientation) • ResQ (regular GME meeting) • IHI Modules: o Introduction to Patient Safety o Responding to Adverse Events o Root Cause Analyses and Actions o Achieving Total Systems Safety o Teamwork and Communication (onboarding requirement) • Program-specific initiatives and training |
UNMC Graduate Medical Education: House Officer Scholarly Activity
The GME Office that has created multiple resources to promote scholarly activity for residents and their involved faculty mentors. The GME Office offers the following resources to promote scholarly activity for residents/fellows and their involved faculty members:
1. GME Patient Safety/Quality Improvement/Disparities Research Collaborative: This Research Collaborative promotes research in various aspects related to patient safety, quality improvement and addressing disparities in health care. The Collaborative consists of the Associate Dean, a Ph.D in statistics and two Master’s level statisticians. All of them possess significant experience in clinical research and help residents with: study design, methodology, statistical support, data acquisition, IRB approval, abstract and manuscript preparation. The Collaborative meets every Tuesday to help residents with research.
2. GME Educational Research Collaborative: This Research Collaborative promotes research in various aspects related to medical education. The Collaborative consists of the Associate Dean, and MD, Ph.D in education. Both of them possess significant experience in educational research and can help with: study design, methodology, statistical support, data acquisition, IRB approval, abstract and manuscript preparation. The Collaborative meets every Wednesday to help residents with research.
3. Annual GME Research Symposium: This campus-wide event provides the opportunity for residents/fellows to present their research abstracts
4. Graduate Medical Education Research Journal (GMERJ): This peer-reviewed journal was started on our campus to provide an avenue for the house officers to publish their scholarly activity. Started in 2019 (with DOI), the journal has provided a good platform for residents/fellows to publish their articles.
Davis Global Center Resource for GME Programs
The Dr. Edwin G. & Dorothy Balbach Davis Global Center (Davis Global Center) is a highly advanced clinical simulation facility purposefully designed to promote simulation-based training for all health professionals and foster the practice of safe patient care in highly-functioning and effective interprofessional teams. The 192,000 sq.ft. center is spread out over five distinct floors with each floor focusing on a specific domain such as cognitive and psychomotor domains etc. This creates a safe, highly effective and innovative training environment that benefits all health professionals in training and in practice.
The Davis Global Center is one of the world’s largest simulation center with some of the most advanced simulation technologies in the world that help with house officer training in all the domains ranging from cognitive, psychomotor, affective and team-based training.
Add additional information about how your program uses the space
Web site: Davis Global Center | iEXCEL | University of Nebraska Medical Center (unmc.edu)
Preventing Physician Depression and Suicide
Department of Psychiatry UNMC
Top causes of death among residents
#1 Neoplastic
#2 Suicide
Higher rates of death early in residency (first two years)
Unchanged over the last 15 years
Yaghmour et al. Causes of Death of Residents in ACGME-Accredited Programs 2000 Through 2014: Implications for the Learning Environment. Acad Med. 2017 Jul;92(7):976-983
Suicides cluster at certain times of year
Higher in the first (July) and third quarters (after winter holidays) of academic year
Physician Suicide Is a
Multi-Faceted Problem
Individual factors
The training environment
Culture of medicine
An estimated 400 physicians die by suicide in the US per year
Center C, Davis M, Detre T, Ford DE, Hansbrough W, Hendin H, Laszlo J, Litts DA, Mann J, Mansky PA, Michels R, Miles SH, Proujansky R, Reynolds CF 3rd, Silverman M M (2003). Confronting Depression and Suicide in Physicians. JAMA, 289(23), 3161.
Risk Factors for Suicide (1/2)
Mental disorders (particularly depression)
Alcohol and/or other substance use disorders
Previous suicide attempt(s)
Family history of suicide
Impulsive or aggressive tendencies
Easy access to lethal means (e.g., firearms)
Losses and other events (e.g., the breakup of a relationship or a death, academic failures, legal difficulties, financial difficulties, or bullying)
Isolation, a feeling of being cut off from other people
Feelings of hopelessness
US Public Health Service, The Surgeon General's Call to Action to Prevent. Suicide. Washington, DC: 1999.
Risk Factors for Suicide (2/2)
Trauma or abuse history
Chronic physical illness, including chronic pain
Exposure to the suicidal behavior of others
Cultural and religious beliefs (e.g., belief that suicide is noble resolution of a personal dilemma)
Unwillingness to seek help because of the stigma attached to mental health and substance use disorders or to suicidal thoughts
Barriers to accessing mental health treatment
US Public Health Service, The Surgeon General's Call to Action to Prevent. Suicide. Washington, DC: 1999.
Suicide Warning Signs – Talk
A person who is considering suicide may talk or write about:
Killing themselves
Death or dying
Feeling hopeless, helpless or worthless
Having no reason to live
No sense of purpose in life
Being a burden to others
Feeling trapped
Unbearable pain
Suicide Warning Signs – Behavior
Concerning behaviors, especially if related to a painful event, loss or change:
Increased alcohol and/or drug misuse
Searching for a way to end their lives, e.g., searching online for materials or means
Withdrawing from activities
Isolating from family, friends and community
Reckless behavior or more risky activities, seemingly without thinking
Sleeping too much or too little
Tying up loose ends
Visiting or calling people to say “goodbye”
Giving away valued possessions to others
Aggression
Fatigue
Not making plans or looking forward to future events
Suicide Warning Signs – Mood
A person who is considering suicide may display one or more of the following:
Depression
Anxiety
Loss of interest
Dramatic mood changes
Irritability
Humiliation
Agitation
Rage
Sudden improvement in mood after he/she had appeared depressed for a while
Predictors of Depression in Physicians
Difficult relationships with senior doctors, staff, and/or patients
Lack of sleep
Dealing with death
Making mistakes
Loneliness
24-hour responsibility
Self-criticism
Bright RP, Krahn L. Depression and suicide among physicians. Current Psychiatry. 2011; 10(4):16-30.
Protective Factors Against Suicide
Effective clinical care for mental, physical and substance use disorders
Easy access to a variety of clinical interventions and support for help seeking
Connectedness– Strong connections to individuals, family, community and social institutions
Support from ongoing medical and mental health care relationships
Skills in problem solving, conflict resolution and nonviolent ways of handling disputes
Cultural and religious beliefs that discourage suicide and support instincts for self-preservation
US Public Health Service, The Surgeon General's Call to Action to Prevent. Suicide. Washington, DC: 1999.
Barriers to Treatment
Fear of recrimination by colleagues, facilities where they work, credentialers, or licensing boards
Perceived lack of confidentiality–
Fear that his/her illness will be documented in his/her academic record
Accessibility–
Difficulty finding a local provider who he/she trusts, but is not a colleague
Reluctance to seek treatment
Time constraints
Affordability
An attempt to diagnose and treat themselves
Seeking and receiving “VIP treatment” from other health care providers
Belief that treatment does not work
Bright RP, Krahn L. Depression and suicide among physicians. Current Psychiatry. 2011; 10(4):16-30.
Lack of Mental Health Treatment (1/2)
Fears about the potential for seeking mental health care to negatively impact one’s professional reputation, ability to get or maintain licensure, or malpractice insurance are largely unfounded
What is more likely to harm a physician’s reputation, licensure and insurance, are unaddressed and worsening mental health conditions
Gold KJ, Sen A, Schwenk TL. Details on suicide among US physicians: Data from the National Violent Death Reporting System. General Hospital Psychiatry. 2013; 35(1), 45-49.
Lack of Mental Health Treatment (2/2)
In cases where physicians died by suicide, depression is found to be a significant risk factor leading to their death at approximately the same rate as among non-physician suicide deaths
Physicians who took their lives were less likely to be receiving mental health treatment compared with non-physicians who took their lives
Gold K J, Sen A, & Schwenk T L. Details on suicide among US physicians: Data from the National Violent Death Reporting System. General Hospital Psychiatry. 2013; 35(1), 45-49.
Burnout
Emotional exhaustion–
Tired, nothing left to give, no pleasure
Depersonalization–
Cynicism, going through the motions, like a robot, automatic pilot
Decreased sense of accomplishment–
Never good enough, not worthwhile
Stress and Productivity
Approaching a Depressed Colleague
Take the lead and be gently assertive–
As a general rule, it is easier and safer for healers to be in the healing role and much harder to be in a position of vulnerabiReach out and do not wait for them to come to you
Normalize their experience–
Remind him/her of the difficult realities of medicine
Your training and your work is inherently stressful and challenging
Hence, feeling distressed or overwhelmed is natural at times
If you are comfortable, self-disclosure or sharing examples of others who have struggled can be powerfully validating
Be a good observer–
Do not tell someone how you think they may be feeling, as this could be experienced as either threatening or condescending
Rather, observe and reflect their behavior, and ask them to ascribe meaning (e.g., “I notice you have been late to clinic/class a lot lately. How are things going for you?”)
Be reassuring–
Even though depression and other emotional problems can impact work performance at times, it does not mean you are a bad physician
It means you need to take steps to take better care of yourself
Be willing to offer flexibility and space for the person to get the help they need–
All the compassionate listening and caring for our students, trainees and colleagues will not amount to much if we do not offer opportunities for them to avail themselves of the resources they need in times of emotional distress
Furthermore, individuals probably need to hear very clearly that there will be no negative repercussions for them seeking and receiving help in times of need
Speak clearly and directly–
Once the conversation is opened, do not be afraid to use words like “depression” or “suicide”
If people are struggling with these issues, it can a relief to have an opportunity to discuss them
Know your resources–
Be ready to offer real help in the form of information about how a person in your environment can get help quickly, if necessary
Please see “Suicide Prevention” Resource Document provided by the GME office.
Physician Impairment and Substance Use Disorder
UNMC Psychiatry presentation
Physician Impairment
“The inability to practice medicine with reasonable skill and safety to patients by reason of physical or mental illness,
including deterioration through the aging process, the loss of motor skills, or the excessive use or abuse of drugs, including alcohol.”
AMA Code of Medical Ethics.
““…physical or mental health conditions that interfere with a physician’s ability to engage safely in professional activities...”
AMA Code of Medical Ethics.
AMA’s Code of Medical Ethics
Opinion 8.15
“It is unethical for a physician to practice medicine while under the influence of a controlled substance, alcohol, or other chemical agents which impair the ability to practice medicine.”
AMA Code of Medical Ethics.
AMA’s Code of Medical Ethics
Opinion 9.3.1 (b)
“Take appropriate action when their health or wellness is compromised, including:
(iv) seeking appropriate help as needed, including help in addressing substance misuse or substance use disorders. Physicians should not practice if their ability to do so safely is impaired by use of a controlled substance, alcohol, other chemical agent or a health condition”
AMA Code of Medical Ethics.
Alcohol Misuse
Alcohol misuse is a common response to unmanageable stress
Alcohol increases impulsivity and the risk of a suicide attempt
US Public Health Service, The Surgeon General's Call to Action to Prevent. Suicide. Washington, DC: 1999.
15-20% (1,2) of health care professionals will misuse substances at one point in their career
Alcohol – Most commonly used
Opioids & stimulants – Next most common
Recreational drugs (cannabis, cocaine) use is less than the general population
Men > women likely to misuse substances
Women have higher prevalence of alcohol use and choose alcohol over other substances
Female physicians have higher alcohol misuse rates than general population
Oreskovich MR, Kaups KL, Balch CM, Hanks JB, Satele D, Sloan J, Meredith C, Buhl A, Dyrbye LN, Shanafelt TD. Prevalence of alcohol use disorders among American surgeons. Arch Surg. 2012 Feb;147(2):168-74. doi: 10.1001/archsurg.2011.1481. PMID: 22351913.
Female Impaired Physicians
More likely to report past (51.8% vs. 29.9%; OR = 2.51) or current (11.4% vs. 4.8%; OR = 2.54) suicidal ideation
More likely to have made a suicide attempt whether under the influence or not
More likely to misuse sedative hypnotics than men (11.4 vs. 6.4; OR = 1.87)
Less likely to have family problems, specifically in the marital realm (OR 0.50; 0.32-0.76) and with their children (OR 0.52; 0.28-0.97)
Less likely to have a mandatory referral as a presenting problem at treatment (OR 0.61; 0.39-0.95) and less likely to have had loss of staff privileges (OR 0.46; 0.26-0.83)
No gender differences in employment problems (65.3% vs. 67.5%) or legal problems
By Specialty
Most studies have reported a consistently higher rate of drug and alcohol use in emergency room physicians, psychiatrists, anesthesiologists and physicians in solo practice
ER physicians – Cannabis (10.5 vs. 4.6%) and cocaine
Psychiatrists – Benzodiazepines (26 vs. 11%)
Anesthesiologists – Major opioids (although more have alcohol use disorders than opioid use disorders)
Pediatricians, pathologists, radiologists, and obstetricians and gynecologists have the lowest rates of substance use among physicians
Easy Access Creates Risk
Physicians have easy access to medications that can be misused:
When administering to patients
By self-prescription
Alcohol is available to physicians as it is to anyone in our society
Identifying Impairment
Family and marital problems (often occur first)
Financial issues, legal issues (DUI)
Work performance is typically not impaired until the more advanced stages (Can be 6-7 years from diagnosable SUD to treatment)
Physicians are likely to protect their work performance until the disease has neared the end stage
43% of opioid-using doctors had been using opioids for more than 2 years before detection
The physician with substance use disorder often retains the ability to protect his/her practice performance at the expense of other dimensions of life
Social, family, and emotional problems will often occur prior to practice impairment
No one sign signifies impairment
Collectively, however, they may define a pattern and provide warning that a potential problem exists
Early identification can help remediation and assure patient safety
Burden and Implications
Substance use disorder is very disabling among physicians
Addiction has been directly associated with physician suicide
Accidental death may occur while intoxicated
Patient safety
Substandard care by physicians also affects colleagues
Legal ramifications
Loss of job – Difficulty finding other jobs
Loss of medical license
Loss of DEA Registration Number
The Conspiracy of Silence Related to Stigma
The key barrier to intervention is denial:
By the impaired physician
By colleagues
By family
By associates
Shame –
Physician as weak, selfish, bad person
Fear of Reprisal
Loss of prestige and livelihood
The Need for Intervention
Intervention may be necessary when an individual is either unaware of her/his addiction or, because of shame, fear, or denial, is psychologically unable to recognize the seriousness of the disease or the need to seek treatment.
Physical or mental illnesses often co-occur with substance use disorders and requires intervention in their own right – Have to treat the whole person
Code of Medical Ethics
Opinion 9.3.1
When physician health or wellness is compromised, so may the safety and effectiveness of the medical care provided. To preserve the quality of their performance, physicians have a responsibility to maintain their health and wellness, broadly construed as preventing or treating acute or chronic diseases, including mental illness, disabilities, and occupational stress.
Collectively, physicians have an obligation to ensure that colleagues are able to provide safe and effective care, which includes promoting health and wellness among physicians.
State laws that require reporting of specified physician conduct to state agencies vary considerably by jurisdiction
AMA’s Code of Medical Ethics
Opinion 9.3.2
Providing safe, high-quality care is fundamental to physicians’ fiduciary obligation to promote patient welfare. Yet a variety of physical and mental health conditions—including physical disability, medical illness, and substance use—can undermine physicians’ ability to fulfill that obligation. These conditions in turn can put patients at risk, compromise physicians’ relationships with patients, as well as colleagues, and undermine public trust in the profession.
In carrying out their responsibilities to colleagues, patients, and the public, physicians should strive to employ a process that distinguishes conditions that are permanently incompatible with the safe practice of medicine from those that are not and respond accordingly.
Steps for Intervening if Physician Addiction is Suspected
(Physicians Helping Physicians)
Contact the state physician health program (PHP) Nebraska Does Not Have a PHP – Consider LAP or EAP
Recruit others to assist you (avoid having a conversation with the physician alone – Should not be a confrontation)
Express positive regard for the physician’s abilities (demonstrate respect for the individual)
Describe specific, observable problem behaviors of concern
Avoid accusation or blame; be kind and empathetic
Avoid negotiating, arguing, or bargaining (do not engage the individual in attempts to avoid the intervention)
Present a specific plan of action for assessment and treatment (consider working with the state PHP to develop a plan first)
Indicate clearly the consequences of not following through with the plan
Insist on immediate action; do not consider requests for “one more chance”
Provide for safe transition and transportation to the next step in the plan (typically, assist the physician in attending a professional assessment )
Activities of PHP for Physicians with Substance Use Disorders
Usually Required
Abstinence from all substances, including alcohol
Group therapy with other physicians with a professional facilitator
Individual psychotherapy
Mutual help meetings (Multiple times per week)
Body fluid screening, random as well as for cause (Multiple times per month)
Possibly Required
Psychiatry Care
PCP (No self prescribing and ask advice on OTC medications)
Family Therapy
Workplace limitations (No opioids or procedures with opioids)
Prescribing limitations
Work hours limited
Neurocognitive testing
Return to work evaluation, if disability requires several months’ absence
Resident Resources
CCS Orientation
Trauma Orientation
___
___
EGS Orientation
ACS Roles & Responsibilities (2025-2026)
Acute Care Surgery - Roles and Responsibilities
2025-2026
Purpose: The purpose of this document is to outline the roles and responsibilities for each team member providing patient care on the Acute Care Surgery service in order to provide coordinated and timely care. This document serves as a guideline that can and should be adjusted according to the needs of the patient and the needs of other patients requiring concurrent care.
Guiding Principles
- Teamwork: Acute Care Surgery includes multiple service lines, each unique to their patient population and staff coverage. In addition, we are one team with one mission- to offer the highest level of care to our patients. We will support each other in any way needed to achieve our mission.
- Communication: Caring for acutely injured and ill patients requires clear, closed loop communication delivered in a respectful and professional manner.
- Leadership: Acute Care Surgery is present in all arenas of Nebraska Medicine- including the ER, OR, floor, ICU and clinic. Given our large footprint, all members of the Acute Care Surgery team must act as leaders and a resource to any person or patient at Nebraska Medicine who asks for our help or input.

Contents
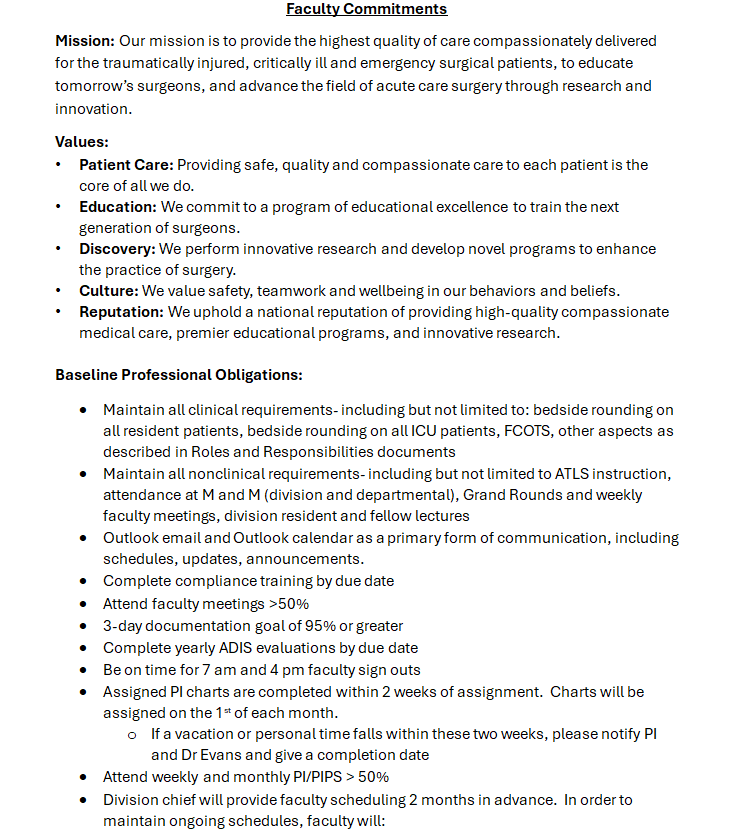
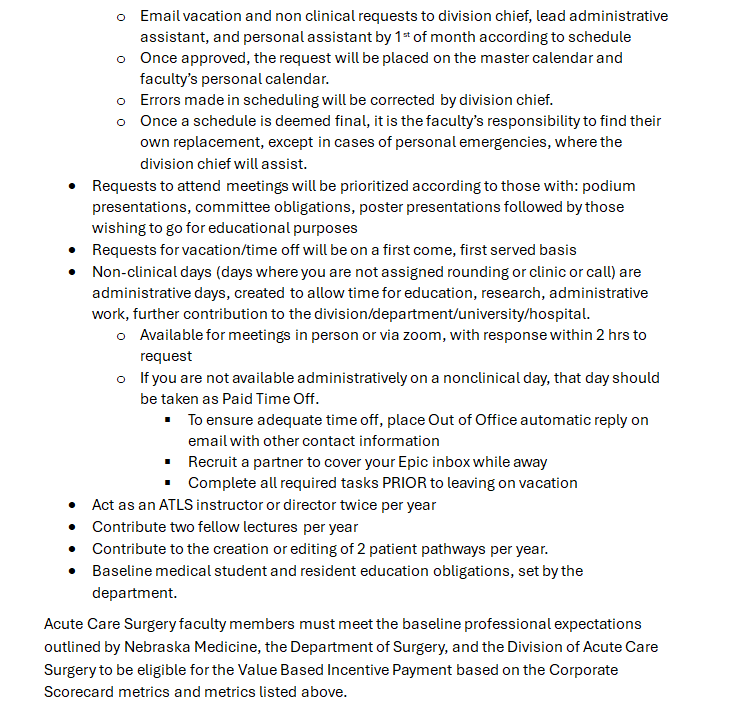
- Faculty Commitments
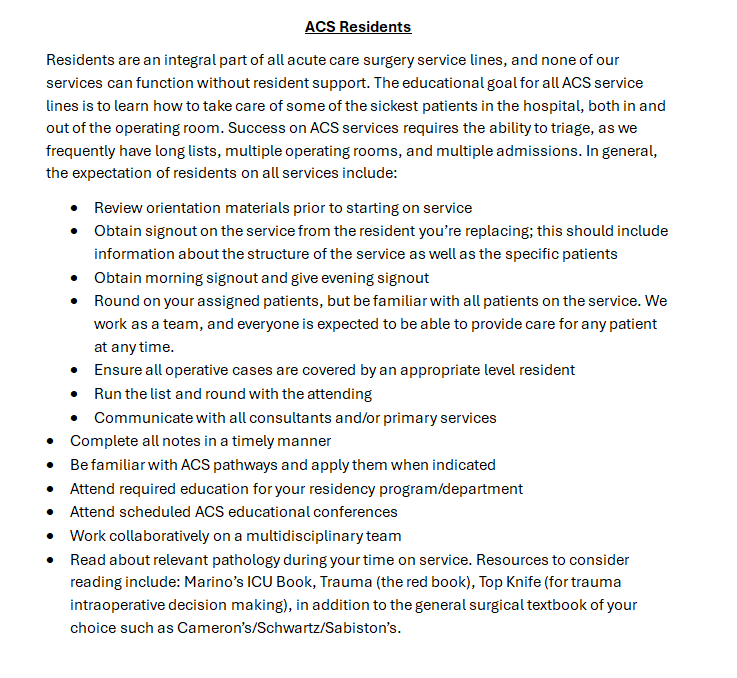
- ACS Residents
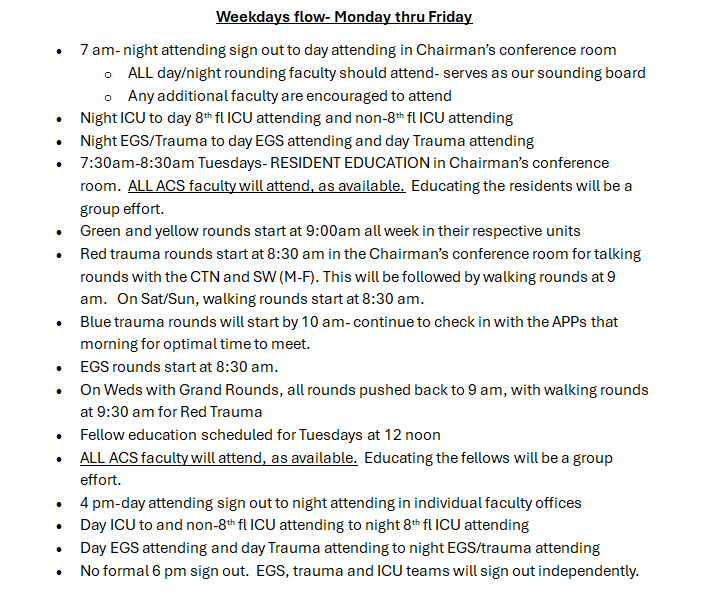
- Weekdays flow- Monday thru Friday
- CCS Provider Team Roles and Responsibilities
- CCS Attendings (Green and Yellow)
- CCS Fellows
- CCS Residents
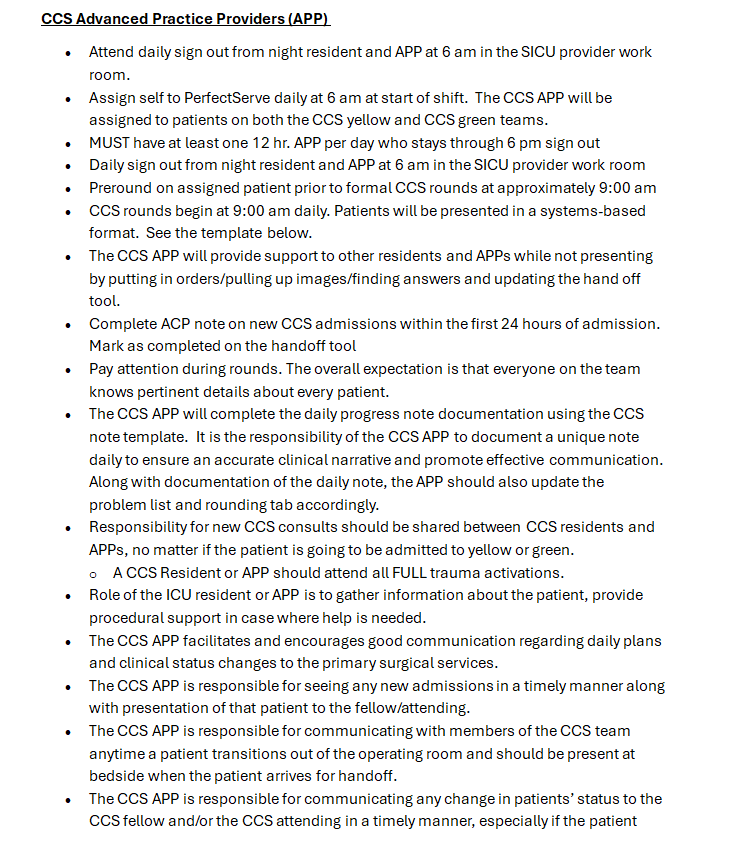
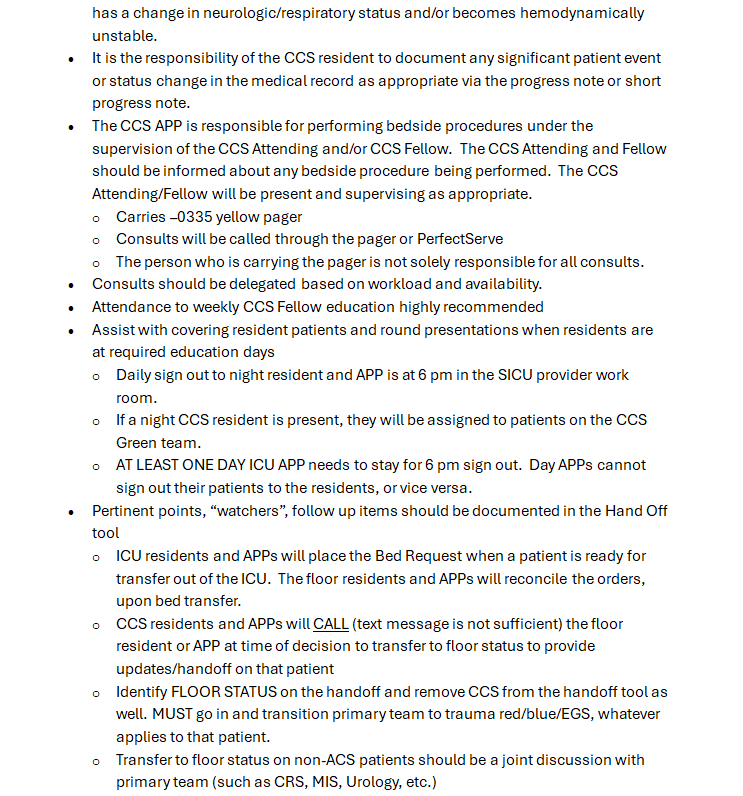
- CCS Advanced Practice Providers (APP)
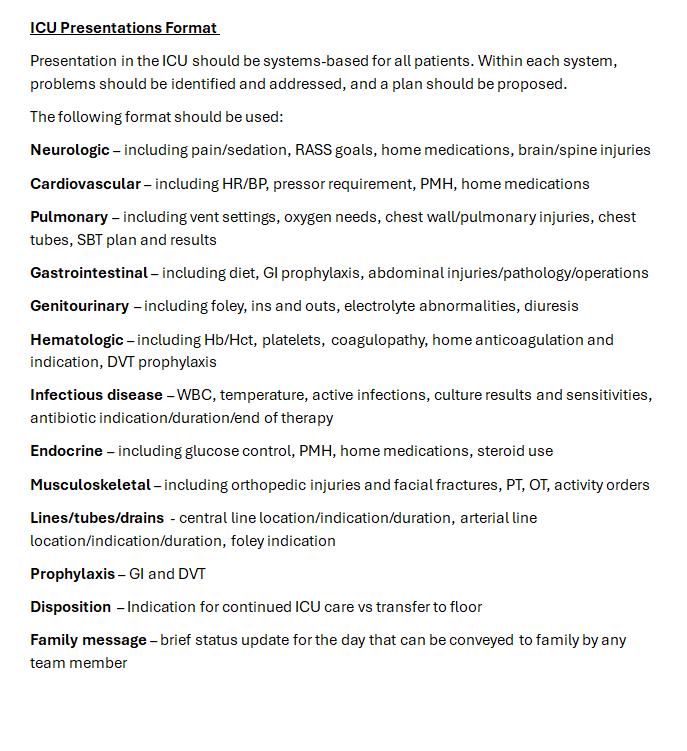
- ICU Presentations Format
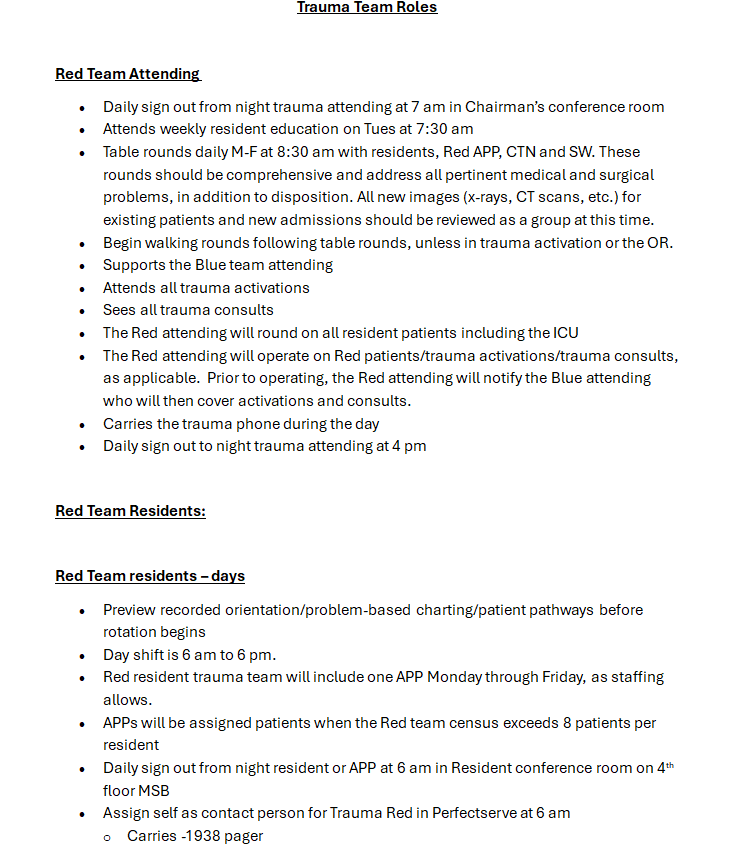
- Trauma Team Roles and Responsibilities
- Red Team Attending
- Red Team Residents
- Red Team residents – days
- Red Team residents – nights
- Red Team APP
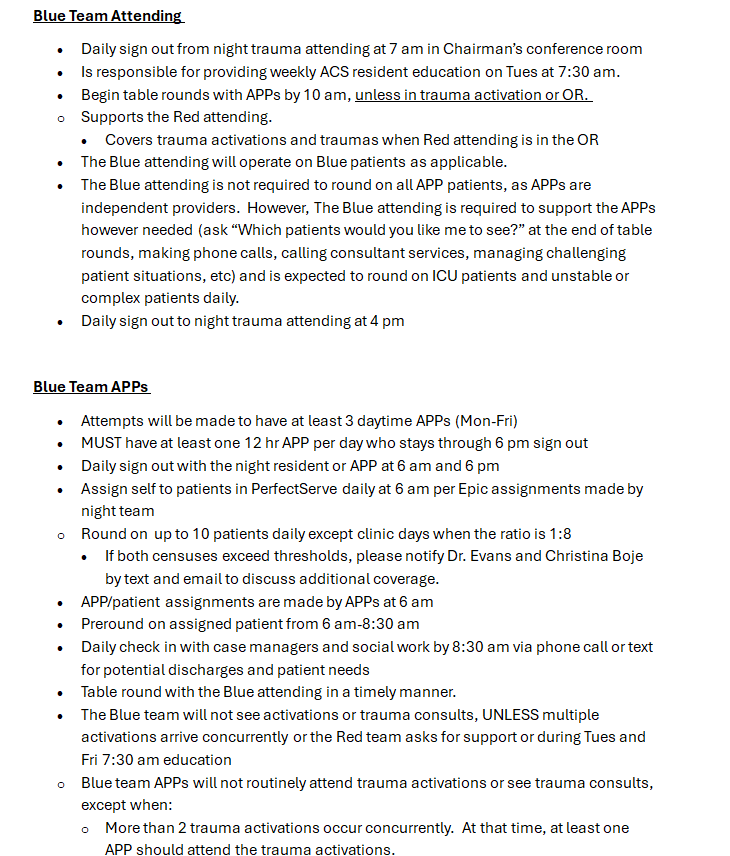
- Blue Team Attending
- Blue Team APP
- Trauma Clinic Coverage
- Chest Wall Injury Attending
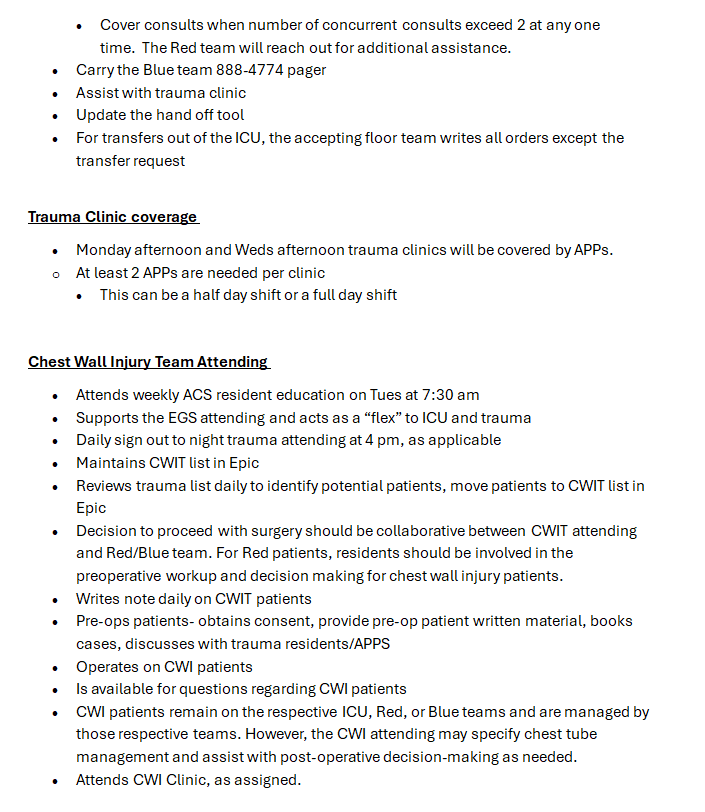
- Nights APPs Roles and Responsibilities
- Night CCS APP
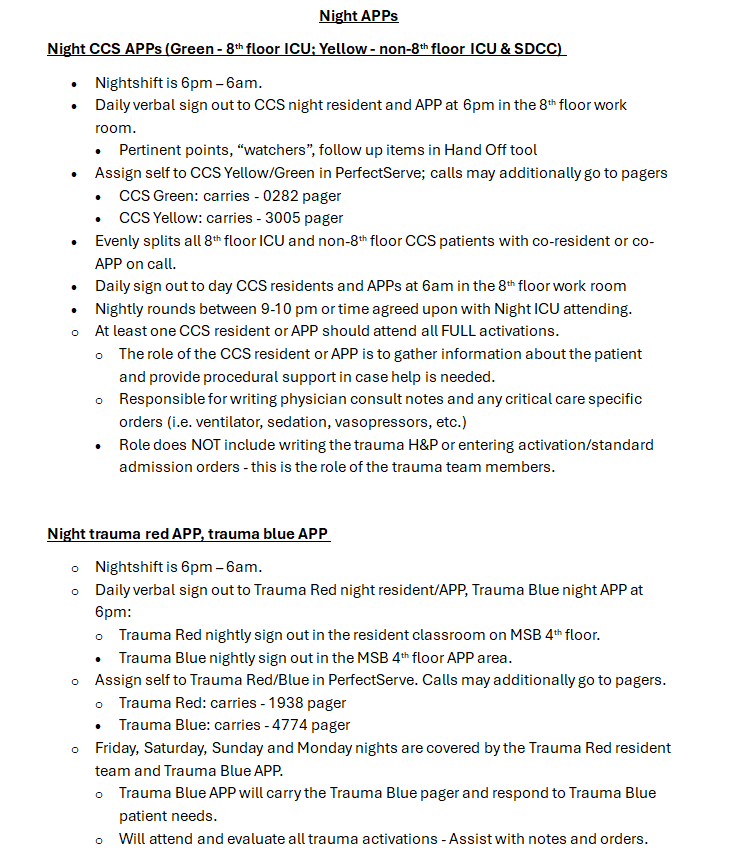
- Night trauma red APP, trauma blue APP
- EGS Team Roles and Responsibilities
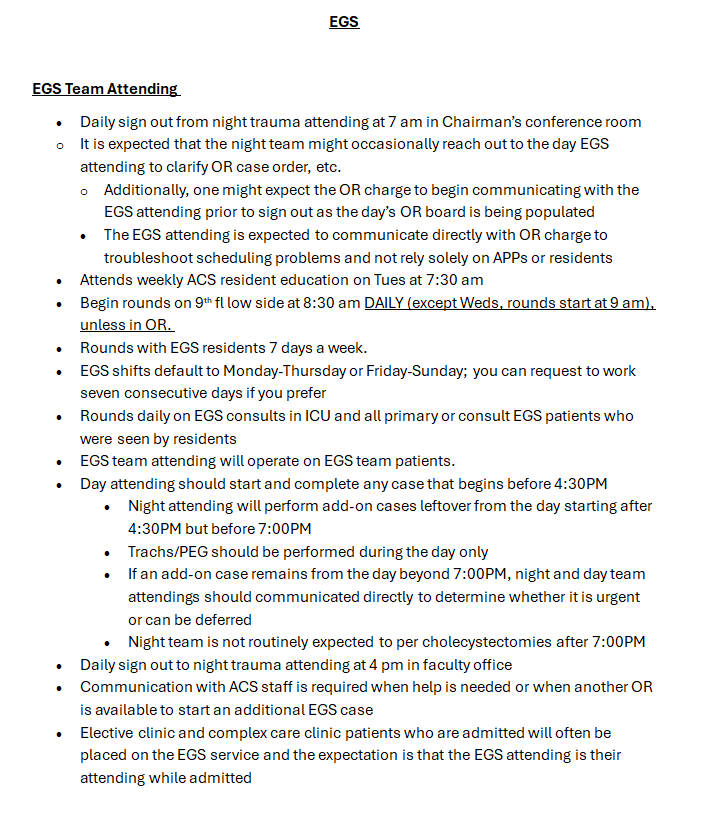
- EGS team attending
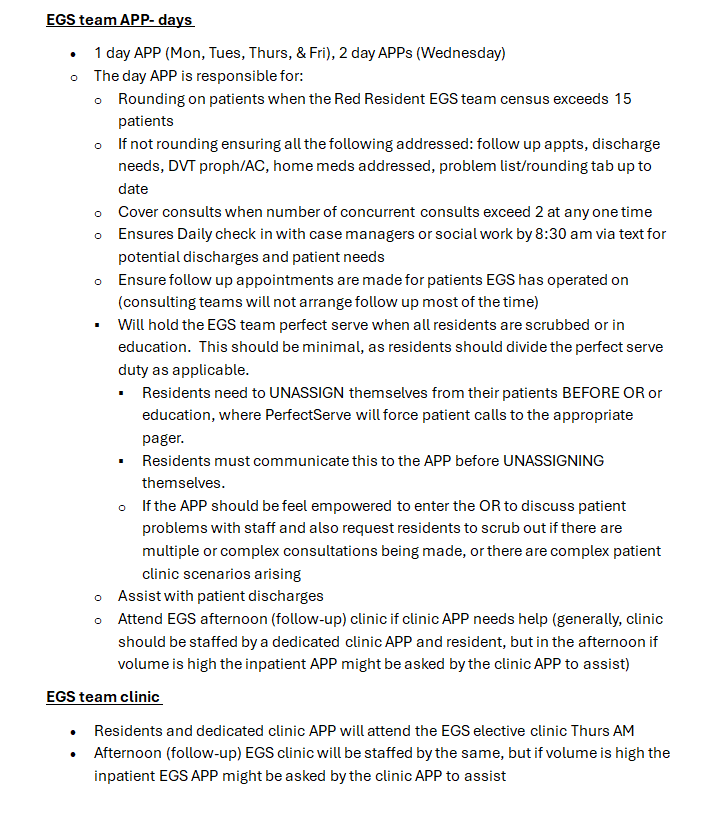
- EGS team APP-days
- EGS team clinic
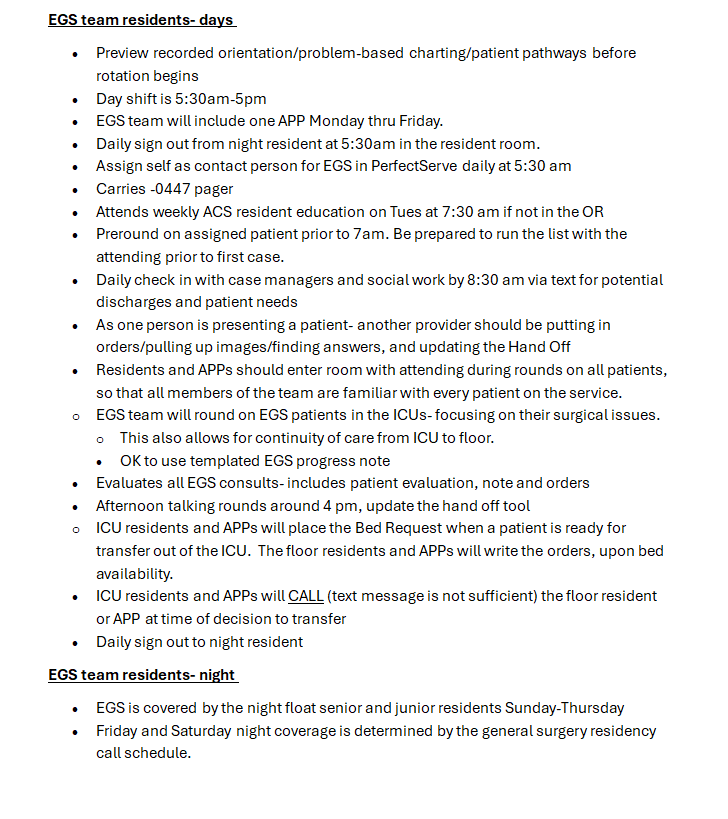
- EGS team residents-days
- EGS residents-night
1. Faculty Commitments
2. ACS Residents
3. Weekday Flow - Monday thru Friday
4. CCS Provider Team Roles & Responsibilities
5. Trauma Team Roles and Responsibilities
6. Nights APPs Roles and Responsibilities
7. EGS Team Roles and Responsibilities
ACS Clinic Referral Patterns
|
Monday PM (CWIT) |
Wednesday AM (ENCOMPASS) |
Wednesday PM (Trauma) |
Thursday AM (EGS Elective) |
Thursday AM (APP Follow-up) |
Thursday PM (EGS Follow-Up) |
Friday AM (Complex Care) |
|
•Discharged from hospital after rib plating •Discharged from hospital with rib fractures requiring further evaluation •Follow-up rib-related problems from Monday PM (CWIT) clinic |
•All patients enrolled in ENCOMPASS should be seen here •Patients may require additional appointments in Wednesday PM (Trauma) clinic or Friday AM (Complex Care) clinic depending on needs |
•Follow-up trauma-related problems from Monday PM (CWIT) clinic |
•New elective general surgery consultations •Discharged from ED or hospital after EGS evaluation who still need an operation (e.g., non-operative appendicitis) •Percutaneous cholecystostomy tubes ok •Patients previously discharged from any ACS service who are returning for follow-up or a new problem (e.g., inguinal hernia recurrence one-year post-op) |
•Discharged from the hospital after EGS operated on the patient (inpatient or elective) •Patient overflow from Wednesday PM (Trauma) clinic or Thursday PM (EGS Follow-Up) clinic •Do NOT schedule percutaneous cholecystostomy tube patients in this clinic •Do NOT schedule patients here who might need additional operations (e.g., non-operative appendicitis) |
•Discharged from the hospital after EGS operated on the patient (inpatient or elective) •Follow-up general surgery-related problems from Thursday (EGS Follow-Up) clinic •Do NOT schedule percutaneous cholecystostomy tube patients here •Do NOT schedule patients here who might need additional operations (e.g., non-operative appendicitis) |
•Patients requiring long-term or multi-disciplinary care such as ventral hernias with EC fistulas or complex wounds •Percutaneous cholecystostomy tubes ok •Admission to this clinic requires approval from Berning, Terzian, Tierney, or Veatch •Jenn Dickey will identify patients in Wednesday PM (Trauma) clinic or EGS PM (Follow-Up) clinic who should be transitioned to this clinic •Most patients should not typically schedule here from ED or hospital at discharge |
Trauma orientation manual
Welcome to Trauma Surgery! Our vision for your rotation is to offer the highest level of care to our patients while teaching residents and students to provide outstanding clinical care to injured and critically ill patients. You will care for patients in a team comprised of residents from general surgery, surgical subspecialities, and emergency medicine, as well as advanced practice providers, and will interact regularly with a variety of consulting services. All residents are expected to be present and ready to work and function on the service on the FIRST day of the rotation.
Our Team- Physicians
|
Attending |
Pager |
Cell |
|
Zachary Bauman, DO |
402-888-1131 |
712-251-0895 |
|
Chris Barrett, MD |
402-888-6080 |
651-497-7846 |
|
Joseph Baus, MD |
402-888-1800 |
614-975-5446 |
|
Bennett Berning, MD |
402-888-5527 |
312-208-7465 |
|
Keely Buesing, MD |
402-888-0563 |
402-312-0984 |
|
Emily Cantrell, MD |
402-888-1201 |
336-775-8889 |
|
Samuel Cemaj, MD |
402-888-1203 |
402-305-5809 |
|
Charity Evans, MD |
402-888-0525 |
312-231-0897 |
|
Matthew Goede, MD |
402-888-3770 |
402-881-7345 |
|
Mark Hamill, MD |
402-888-5484 |
843-324-8252 |
|
Reginald Henry, MD |
402-888-6336 |
408-203-8272 |
|
Abigail Josef, MD |
402-888-5525 |
402-715-0029 |
|
Andrew Kamien, MD |
402-888-1453 |
716-228-0118 |
|
Kevin Kemp, MD |
402-888-2545 |
510-378-2215 |
|
Gina Lamb, MD |
402-888-6333 |
802-681-5911 |
|
Mike Matos, DO |
402-888-5655 |
304-482-2712 |
|
David Mercer, MD |
402-888-3758 |
402-889-3431 |
|
Olabisi Sheppard, MD |
402-888-5034 |
913-271-7241 |
|
William (Hillman) Terzian, MD |
402-888-5526 |
703-505-1058 |
|
John Tierney, MD |
402-888-6079 |
480-703-4556 |
|
Jessica Veatch, MD |
|
303-726-0736 |
|
Brett Waibel, MD |
402-888-0698 |
252-414-8586 |
|
Levi Zehr, MD |
|
402-380-4086 |
Trauma Protocols/Patient Pathways
Current treatment protocols and guidelines for the service are available on the Acute Care Surgery pathways website, which is available at paths.trauma.ai
Login: trauma
Password: path402
PLEASE ADD THIS WEBSITE TO THE HOME SCREEN ON YOUR PHONE FOR QUICK ACCESS during the rotation.
This website is updated constantly. Please refer to it regularly to ensure that all trauma patients receive consistent high-quality care. Up-to-date contact information for trauma faculty, APPs, and support staff is also available on the website.
Trauma Services
There are two trauma services – the Red Resident Service and the Blue APP Service. Any patient can be admitted to either service. In general, however, the following criteria should be followed as a guideline:
Assignments to Red resident team
-
Operated on by Red Resident team, excluding PEGs and trachs
-
Injury patterns that will likely require a trauma surgery (excluding ribs, see below)
-
Requiring serial abdominal exams
-
Grade 3 or higher solid organ injuries
-
Greater than 5 rib fractures or bilateral (not all rib fractures go to red. Rib fractures can go to either team)
-
Pts which will greatly enhance the resident’s education
-
Operated on by Blue APP team
-
APPs should come to OR to assist with surgeries on Blue pts where residents are not assisting. Please communicate that day with the trauma attending to ensure operative coverage of those patients.
-
Isolated head or extremity injury
-
Blue team should carry more of the LTC patients
Work Hours
Each resident is responsible for his or her own duty hours. It is expected and mandated by the ACGME, University of Nebraska Medical Center, the Department of Surgery, and the trauma service that residents will average no more than 80 hours per week averaged over four weeks, and receive one day off per week, averaged over four weeks. The call schedule has been designed so that all residents will be in compliance with duty hours. If you anticipate duty hour violations, you must communicate these issues with Dr. Tierney immediately.
Pagers/PerfectServe
888-1938 is the Red trauma pager- is carried by a Red resident during day and nights Fri-Mon. (APP will carry T, W, Th nights)
888-4774 is the Blue trauma pager- is carried by a Blue APP day and night
888-0282 is the Green SICU pager- is carried by a Green resident during day and night
888-3005 is the Yellow Non 8th Fl pager- is carried by an APP day and night
888-0447 is the EGS pager
All residents are required to have PerfectServe downloaded and active. All patient calls will go through PerfectServe. The pagers listed above serve as back up to PerfectServe.
One person is assigned daily per team in PerfectServe to receive patient inquires:
-Intern/junior on Red
-Senior resident on 8th floor ICU
-APP on Blue
-Backup in PerfectServe is senior resident
-Second backup is service pager
EVERYONE needs a trauma pager, because activations still go through the pager system and are not available on PerfectServe. See the Acute Care Surgery admins outside Dr. Bauman’s office to obtain one.
Equitable distribution of consults - run consults thru chief or upper level resident first, but ensure that they are staffed with attending in timely manner. If the Red attending is not available, please staff consults or urgent issues with the Blue, Green or Yellow attending. During sterile procedures or difficult conversations, you must ask a colleague or RN to return your pages in real time, as they are received, in order to facilitate care.
Team Member Responsibilities
Red Attending:
The Red attending is the primary attending who rounds on Red patients, covers activations, and does operative cases and procedures on all Red patients.
Blue Attending:
The Blue attending rounds on the Blue service with APP support, and also serves as the backup trauma attending for activations when the Red attending is not available. The Blue attending will operate on Blue patients who need operations. Typically, these are chest tubes, trachs, PEGs, wound debridements. Although the patients are admitted to the Blue service, these procedures and cases should still be covered by a resident.
Chest Wall Attending:
One attending is assigned to cover the Chest Wall Injury Team on weekdays. This attending will do any chest wall injury cases. The decision to refer a patient to the Chest Wall Injury Team should be discussed with the primary rounding Red or Blue attending. Chest wall cases on both Red and Blue patients should be covered by residents depending on the needs of the service.
Surgery Chief:
-
The on-call surgery chief is responsible for the workings of the entire service and should lead all activations.
-
The chief resident should be at the foot of the bed during activations and oversee the junior resident, who is performing the primary and secondary surveys.
-
Know all protocols/pathways and formulate workup plan for all patients, with attending supervision.
-
Perform or supervise all procedures in the ED and on the floor
-
Know all information about all patients on service prior to formal rounds with attending. (This does not require that you have seen every patient personally, but does require that you know information in the chart, have run the list with the team, and have assigned appropriate level providers to see each patient.)
-
Ensure that all OR cases are covered by an appropriate level resident.
-
Round on all ICU patients and communicate with the ICU team regarding plans.
Surgery Junior:
-
Preround on assigned patients. The surgery junior should in general be assigned to see post-operative patients.
-
Be at bedside during all activations to do the primary and secondary survey.
-
Assist with or perform all bedside procedures on the floor or in the trauma bay, with supervision from the chief resident.
Off-service Surgery Intern, EM Intern:
-
Preround on assigned patients.
-
Do primary and secondary surveys at bedside during activations when surgery junior is not available
-
-
Outside hospital transfers: If you receive a page or call regarding an outside hospital transfer, please refer the caller to the attending on call. All transfers need to be approved by the Attending on call.
-
Start H&P and problem list and place orders during activations when surgery junior is available to bedside
-
Be familiar with all patients admitted to the service and with their plans for the day, so that patient care is not compromised when the chief/junior are in the OR
-
Participate in bedside procedures
-
If the rest of the team is in the OR, work with the Red APP to ensure that the patient care continues to progress for the remainder of the service.
-
The Blue attending is the backup attending during the day, and the ICU attending is the backup at night. If a patient has a change in status (new tachycardia, arrhythmia, hypotension, hypoxia, altered mental status, hemorrhage, sepsis, etc), and the rest of the team is in the operating room, it is your responsibility to alert the backup attending immediately.
-
If you have a question regarding the existing plan of care that cannot be answered by the Red APP, go to the operating room to ask for help.
Red APP:
An APP is assigned to the Red service Monday-Friday. The primary role of the APP is to support the team, and not to serve as a primary rounder. The APP should:
-
Assist with notes and order on activations
-
Help facilitate communication with therapy, case management, and social work
-
Assist with discharges.
-
Be familiar with all patients on the service, and should hold the pager/PerfectServe and continue to advance care on the entire service when all residents are scrubbed or in education.
The APP is responsible for rounding on patients when the Red census exceeds a 1:10 provider-to-patient ratio.
On the weekends, there is no Red APP, but the Blue APPs are expected to attend and assist with activations.
Workspace
The trauma APPs have workspace on MSB 4th fl. We also encourage regular use of the 9th floor trauma work room, so that you are immediately available to a large number of our patients.
Departmental Education
Tues: 7:30 am Acute Care Surgery education conference in the Chairman’s conference room MSB 45119
**This is mandatory for all residents on trauma and EGS. If there is an operative case, one resident can leave conference once the patient is being prepped. The attending is expected to get patients back to the OR without resident support for first start cases on Tuesday mornings.
Residents are required to attend their department’s regularly scheduled education conferences.
Wed: 7a-12noon General Surgery
Thurs: 8a-1p ER
Hand offs
6 am: Sign out from night resident and/or APP in 9th floor trauma room
6:00-8:30am: Preround on assigned patients. Ensure that your name is listed in the Epic column “Surg Pt Status” for the patients you are rounding on.
8:30am: Round with attending. This can be adjusted depending on OR schedule, activations, or at attending discretion. If there are significant changes in patient status, do not wait for rounds to tell your chief/senior/attending.
6 pm: Face-to-face handoff from day to night team in MSB 45119
-
Concise, focused (not rounds), discuss unstable patients in detail
-
Entire sign out should take less than 20 minutes
Bedside Multidisciplinary Rounds
After sign out, begin pre-rounding
-
Bedside Multi-disciplinary rounds will start around 8:30 am (at rounding attending’s discretion)
-
Expectations for rounds:
-
-See your patients in advance
-
-Know all injuries
-
-Know vital signs (Tmax, T current, HR, RR, BP, O2 saturation and oxygen needs)
-
-Know ins and outs (total ins/outs for 24 hour period, urine/ostomy/drain/tube outputs broken down by 12 hour shifts)
-
-Know today’s labs and imaging results
-
-Know up-to-date plans from consultants
-
-Know PT/OT recommendations for discharge (home vs SNF vs rehab)
-
-Examine every wound every day before attending rounds, unless specifically directed otherwise
Text or page Pharmacy just before start of rounds
Patient’s bedside RN should be involved in the patient’s discussion and engaged in rounds
Resident or APP must be logged into a computer at all times:
-
Laboratory results/trends
-
Pull up daily imaging and other data
-
Enter orders in real time
-
Resident or APP presenting the patient should not be the person entering orders at the computer
Daily Flow
Following bedside multidisciplinary rounds……….
-
Get work done.
-
Call Consults first
-
Then do Discharges- requires close collaboration with Case Management and Social Work
-
Attend trauma activations
-
Do tertiary exams – should occur as close to 24 hours after admission as possible
-
Do bedside procedures and operations (trauma floor residents operate on trauma ICU patients)
If surgery residents are in the OR, APP and non-surgical residents are expected to carry the pager, continue responding to activations, and advance care for all patients on the entire service (even patients who were seen in the morning by an operating resident). Each resident is expected to know the general plan for every patient on service to ensure that all patients receive high-quality care at all times.
4:00 PM - Afternoon rounds with APPs and residents
-
Review new patients
-
Swift and focused updates on stable existing patients
-
Address questions from RNs, RTs
-
New plans for unstable or deteriorating patient
Night Flow
-
APP coverage Tuesday-Thursday
-
Resident coverage Friday-Monday
-
Attend trauma activations
-
Complete items to assist day team:
-
Tertiary exams
-
Populate the problem list, update the patient list through the Problem List tab
-
Review all orders, cancel duplicate orders
Trauma Activations
-
All team members should respond to trauma activations
-
Once in activation, can determine if some members can return to other clinical duties. Upper-level residents and APPs will assist with this process
-
It is not uncommon to get multiple traumas at once. Dispatch will provide the following information over the pagers for full or limited activations as instructed by ED Lead/Charge RN or designee
Trauma Roles and Responsibilities during Trauma Activation
Roles and Responsibilities of the Trauma Team
Purpose: The purpose of this document is to outline the roles and responsibilities for each team member present during the Resuscitation of the seriously injured trauma patient in order to provide coordinated and timely care. This document serves as a guideline that can and should be adjusted according to the needs of the patient and the needs of other trauma patients requiring concurrent care.
Guiding Principles
· Leadership: Good communication and leadership are keys to a well-organized and efficient trauma resuscitation.
· All PRIMARY trauma team members must report to the Documenting Nurse so that he/ she can document the team member’s time of arrival to the trauma.
· All listed team members should wear gown, gloves, and protective eye wear for universal precaution for patient and staff safety and to be easily identified as trauma team members.
· The assignment of specific roles and responsibilities for defined team members is essential to provide high quality trauma care. As an academic hospital, we have a responsibility to our medical education mission while providing the highest level of trauma care possible. Residents rotating on the Trauma service or residents rotating in the Emergency Department will be preferentially assigned to the Trauma Primary role, followed by APPs staffing the trauma service. Residents or APPs involved in the care of the trauma patient must be present at the time of arrival of the trauma patient and remain until the initial resuscitation efforts are complete.
· Closed loop communication should be utilized throughout the resuscitation in order to avoid misunderstanding or miscommunication.
· Noise Control: Individual conversations ARE NOT permitted in the trauma resuscitation area. One voice should be heard by the entire trauma team. NO ONE should be talking while EMS is giving report.
· Non-essential personnel may be asked to step outside of the trauma bay at any time.

Activation
· Call is received from EMS en route. ED lead nurse completes intake. ED lead nurse confirms with ED attending/3rd year resident activation level. ED lead nurse calls dispatch to send out trauma activation page.
· If patient arrives and ED staff note that the activation was not sent via the paging system, another page should be sent, and the trauma attending should be notified via trauma phone call 402-990-5113
· If patient arrives and acuity does not match the trauma level (consult, limited or full), ED staff or Trauma team should notify charge to change activation level. Dispatch must be called to change trauma level and re-page activation level.
· If the patient is being sent from an outside hospital, they should have been identified and their name/MRN entered into EPIC for identification prior to arrival.
· If the patient is coming straight from scene, they should be given an “unidentified” name which should remain with the patient for 6 hours at which time their actual name can be entered into EPIC. (Designate for limited and full traumas) If the patient is still “unidentified” after 6 hours, their name should not be changed until full identification has been established. Refer to policy REG195 for information on how patients are identified.
Prebrief
· Prior to patient arrival, a pre- brief should be initiated and led by the Trauma or ED attending when the majority of the team has arrived in the trauma bay. The Trauma Bedside Nurse should initiate this process before the patient’s arrival if not initiated by the Trauma/ED attending.
· The pre-brief consists of the introduction of the team members (name, role (see diagram above) & discipline) and includes known patient information, preparation (including assignment of procedures), and ensuring PPE.
** Recognizing trauma is unpredictable and can be fluid or change rapidly, if the Trauma or ED attending is unable to perform the pre-brief, the Trauma Bedside Nurse should perform the pre-brief prior to patient arrival.
** If not part of the primary trauma resuscitation team (depicted in the attached diagram and further described below), please stay behind Trauma attending and await to be called upon for assistance with patient care.
Trauma Resuscitation Team/Personnel Responsibilities
· Trauma Team
o Trauma Lead
§ Stands at the foot of the bed
§ Directs overall resuscitation (e.g. fluid resuscitation, blood products, interventions, disposition)
§ Responsible for majority of communication during resuscitation
§ Responsible for determining need for major invasive procedures performed (e.g. central lines, chest tubes, thoracotomy)
§ Accountable for determining whether the patient is safe for transport to CT scanner vs the need for immediate operative therapy for suspected injuries
§ Will not perform procedures in order to focus on directing the resuscitation (if Trauma Senior Resident or APP is needed in a procedure, then the direction of overall delegation will be turned over to the Trauma Attending)
§ May delegate additional tasks to others not explicitly mentioned here (ie. FAST exam, dressing wounds, etc.)
o Trauma Surgery Attending
§ Performs the Pre-brief and assigns defined team member roles, including possible procedures
§ Assumes overall responsibility for the resuscitation
§ Collaborates with ED Attending
§ Performs debrief per protocol with team following trauma resuscitation (must be performed with Trauma Bedside Nurse, at minimum)
· Airway Team
o Airway Resident
§ Stands at head of the bed
§ Is responsible for primary assessment of the A: Airway
§ Accountable for ensuring that the airway checklist is performed and that necessary materials needed for safe emergent intubation are available
§ Evaluates “B: breathing”, lung auscultation & tactile exam for subcutaneous emphysema. If unable to do so, this will be the responsibility of the Primary Trauma Provider (description below).
§ Provides/ Discusses mechanical ventilator settings with RT
§ Performs the neurologic and D: Disability component of the primary survey. If the patient needs to be intubated, all attempts should be made to assess the neurologic/disability (including GCS) prior to intubation.
§ Communicator to the patient. Relays key information to patient and obtains patient feedback.
§ Cervical spine stabilization during patient turning
§ Assist with secondary assessment of HEENT, neck, etc.
§ Once primary and secondary assessments are complete, may either perform or supervise the performance of procedures or FAST exam as designated by Trauma Team Lead.
o EM Attending
§ Responsible for supervising the ED Resident during Primary Assessment of the airway
§ Supervises or assumes management of the airways (including induction plan & techniques)
§ Assumes the role of supervising the Trauma Team when the Trauma attending is not available or during multiple traumas
§ Supervises doctor delegated to perform FAST exam
§ Collaborates with Trauma attending and rest of trauma team once airway is secured
· Trauma Primary Provider
o Starts on the left side of the patient, but is free to move about the patient to perform adequate primary and secondary survey
o Responsible for C: Circulation and E: Exposure of the patient by removing clothing. If the Airway Resident unable to complete their portion of the primary survey (ie. B: Breathing), this becomes the responsibility of the Trauma Primary Provider
o Responsible for secondary survey assessment
o Performs all procedures as delegated by Trauma Team (IO, CVC, thoracostomy tubes, arterial line) under Trauma Attending Supervision
o Additional responsibilities as delegated by Trauma Team
o “Travels” with the patient to CT or the operating room
o Responsible for keeping the Trauma & ED attending, and Trauma Lead informed of patient’s condition and any diagnostic findings
o May perform other tasks as delegated by Trauma/ED attending
· Trauma Secondary Provider
o Starts on the right side of the patient, near foot of patient (see diagram)
o Assist with E: Exposure of patient as needed- needs to carry trauma shears
o Assist with secondary survey as needed
o Assist with procedures as needed. If multiple procedures are needed to be performed at the same time, the Trauma Secondary Provider will be responsible for procedures the Trauma Primary Provider is not performing which will be assigned and supervised by the Trauma/ED attending.
o Trauma Secondary Provider will complete the FAST exam, when indicated, as long as that provider is competent to complete the procedure. If not, EM resident or faculty will move to right of patient to complete the FAST exam.
o May perform other tasks as delegated by Trauma Team
· Trauma Techs
o One stands to the mid/upper right of the patient
o Second stands to the upper left of the patient if present
o Pulls red cart to bedside
o Obtains first set of vitals (including temp) within 30 minutes
o Places patient on cardiac monitor
o Helps remove clothing
o Pulls supplies as needed (see separate checklist for supplies to be pulled before an Agonal Resuscitation)
o Set up necessary equipment for procedures (ie: chest tube, splinting, lac repair)
o Assists with bedside procedures as directed by trauma surgeon, assists nursing staff as called upon, otherwise steps away from bedside once tasks complete
o Performs CPR if necessary
o Completes patient belonging list
o Reconciles supply checklist following trauma resuscitation completion
o Restocks supplies/supply carts
· Trauma Bedside Nurse (TNS trained)
o Initiates the Prebrief before patient’s arrival in the trauma bay
§ If Trauma and EM attendings are not present, the ED Trauma Lead Nurse (or ED Lead) should perform the prebrief, including assignment of defined team member roles
o Directs care to trauma tech
o Assists with retrieval of equipment
o Assists with crowd control
o Confirms EMS IV patency and obtains 2nd IV access, if able
o Inserts foley/NG/OG if indicated
o Administers medications as ordered
o Places patient on the telemetry monitor (shared with tech)
o Primes tubing for Belmont prior to patient’s arrival, when applicable
o Administers blood products and fluids as ordered
o Places patient on defibrillator pads
o “Travels” with the patient to CT, OR or IR
o Assists with obtaining laboratory blood vials
o Performs debrief with team following trauma resuscitation (must be performed with Trauma Attending, at minimum)
o ***In complex traumas/Code 99s/CPR in progress situations, more than 1 Trauma Bedside Nurse is required. In these cases, another bedside nurse will assist with tasks listed above under the leadership of the ED Lead Nurse
· Documenting Nurse
o Responsible for keeping a written record of the resuscitation events on trauma narrator
o Maintains closed loop communication with entire team
o Assists with crowd control
· Additional Trauma or EM residents, APPs, medical students observing or other learners
o Starts behind the “red line”
o Are not immediately involved in the trauma resuscitation unless there is a vacant role
o Are recruited as needed for the care of the patient
o May assist with electronic orders, gathering equipment
· Respiratory Therapist
o Assist with intubation
o Provide ETCO2 monitoring post intubation
o Secure ETT
o Provide suctioning
o Assist with vitals and monitoring the patient (SpO2, HR, RR, measured parameters, etc.)
o Provide transport to CT/MRI (NIV, MV, etc.)
o Restock/check airway cart
· Pharmacist
o Prepares drugs, assures appropriate doses, identifies potential interactions, provides clinical support
o Serves as timekeeper during codes
o Operates defibrillator machine upon guidance of Trauma and EM attendings
Additional Information
Who is the Trauma Team Lead?
The Trauma Team Lead is the General Surgery resident when present. During educational time or when General Surgery resident is not present, it is the ACS APP or Trauma attending.
Who is the Airway Resident?
The Airway Resident is the EM PGY 2 or 3 when present. During educational time when a senior EM resident is not present, it is the EM attending. If EM is not available, Anesthesia will manage the airway.
Who is Trauma Primary?
The Trauma Primary is the General Surgery resident, off service resident rotating on the trauma service, or available ED resident when present. During educational time or when General Surgery resident is not present, it is the ACS APP. Residents or APPs involved in the care of the trauma patient must be present at the time of prebrief and arrival of the trauma patient and remain until the initial resuscitation efforts are complete.
Who is Trauma Secondary?
The Trauma Secondary is the General Surgery resident, or off service resident rotating on the trauma team, when present. This role may also be filled by the ER resident, if present and in PPE at the time of the prebrief. During educational time or when General Surgery or ER resident is not present, it is the ACS APP. A medical student rotating on trauma or in the ER may assist in this role.
It seems like the Primary Survey is divided between 2 different providers?
That is correct. The Airway Resident tasked with airway management, which is closely tied to the pulmonary exam, will perform A: & B: [ZB1] Trauma Primary, who has access to the extremities to evaluate distal pulses and cap refill, fills the C: component. Disability (D:) is then assessed by the Airway Resident who can easily examine the pupils and talk with the patient to obtain a GCS score. The secondary exam then returns to Trauma Primary and Secondary providers. ALL findings should be CALLED OUT with closed loop communication with the Trauma Lead and ED Nurse Scribe.
ATLS primary exam consists of ABCDE, which should be called out first and reported in that order. The findings in the secondary survey should not be called out until the primary survey is completed.
What is the role of Trauma Secondary if there are no procedures required on the right?
Do not under-estimate the importance of the physical exam and participation in the work up of a trauma patient. It is imperative that the Trauma Secondary is learning from & collaborating with the Trauma Team Lead in preparation for them to ultimately assume this role. They are also integral in CT interpretation, and “closing the loop” on the patient disposition after CT scan interpretation.
What if EM attending or trauma attending has to perform a procedure?
If either attending is pulled into a procedure, or is called away from bedside to attend to another patient, the other attending should take over as “in charge”. Both attendings should remain fully available during the resuscitation to supervise residents and APPs involved in the resuscitation. If an attending is involved in a procedure and can no longer adequately supervise, then additional attending support (either EM or trauma) should be called upon.
Who is “In Charge” of the whole Process?
Trauma bay resuscitations are a joint collaboration between the ED & Trauma attendings and teams. Patient Management Guidelines are based on medical evidence and/or consensus of medical providers at Nebraska Medicine, and are intended to be a guide for the trauma resuscitation team. Final management decisions are at the discretion and responsibility of the admitting physician.
***Note: This is not a comprehensive document that addresses all possible situations, and challenges or desired changes will work through the Trauma Resuscitation Committee.
-
CXR for all blunt trauma patients, PXR for pts with unstable pelvis or pelvic pain (discuss with attending), FAST for blunt unstable or penetrating wounds to cardiac box.
-
Penetrating trauma patients need early exposure to look for wounds. Wounds should be marked with paper clips, then x-rays should be obtained of all cavities with a wound.
-
CXR must be reviewed by senior resident before CT
-
Secondary survey then CTs (only when patient is stable)
-
Trauma team member must accompany patient to CT
-
Follow up FINAL reads on all patients; go to radiology to review scans
-
ADD PATIENT TO Epic Trauma list
H&P and Progress Notes
-
Full = Full trauma activation
-
Limited = Limited trauma activation
-
Consult = No trauma activation but seen in the ED. This includes patient worked by EM first AND transfers from outside that are seen in the ED by trauma. The ED does not see transfers that are “consults.”
-
Direct Admit = Transfer from outside that goes directly to an inpatient bed, never seen in ED at any point.
-
Any trauma patient with a traumatic injury or physical/social circumstance which requires observation is admitted to Trauma
Tertiary Exams -
-
Must be done within 24 hrs.
-
AND repeat once the patient can participate (specifically, in head injured or intubated patients)
-
Use the tertiary note template. Include preexisting conditions by clicking on the Tertiary Trauma Quality Improvement button
- Include a ITSS and SBIRT survey
New Patients/Consults
-
Respond quickly and professionally to ALL requests for patient evaluation
-
Physically go see the patient in their current location
-
Make sure they are added to the Trauma team list
-
NO “FYI” or curbside consults and no consults are turned down without attending approval
Requesting New Consults
-
Before calling a consult, make sure:
-
Faculty are aware
-
You have enough patient information to adequately answer consultant questions
-
Know what you are asking the consultant to do
-
Enter an order in the computer AND
-
Make verbal contact with MD or APP on consult team
-
No consults should be called without discussing with trauma faculty first
-
Neurosurgery and ortho have 30 minutes to see the patient
-
If IR is consulted for emergent hemorrhage control, they have 60 minutes from the time of consult to sticking the patient. If you have any issues communicating with IR, notify the trauma faculty immediately.
-
If the consulting resident is unable to provide a plan regarding severely injured patients in a timely fashion (i.e. whether a patient with a severe TBI will get an ICP monitor or craniectomy, timing for fixation of unstable spine), obtain contact information for the consulting attending, and the trauma faculty will call them.
Procedures
-
Notify faculty before performing any invasive procedure
-
After procedure, write a procedure note
-
READ your note and make it accurate
-
Assign note to attending who oversaw the procedure
-
Order and follow up on appropriate post-procedural testing (CXR after bronch or CVC placement). You should not go home after completing a procedure until you review post-procedural imaging.
-
Sterile technique is required for all invasive procedures (ie. arterial and CVC lines, chest tubes, suturing). Chest tubes and central lines should be done with full gown, gloves, mask, and drapes, if clinical condition allows.
Transferring Pts from one level of care to another
-
Call the receiving team to communicate comprehensive handoff information
-
CCS will enter floor orders on ICU patients leaving the ICU for the floor
-
Do not transfer patients to the ICU without discussing with attending
Documentation
Accurate and complete documentation is necessary to ensure proper communication between members of the care team. There are also certain documentation requirements that might not seem clinically relevant, but that are required to maintain trauma program accreditation. The trauma service uses problem-based documentation for H&Ps and progress notes.
-
Do NOT use the "Generate Note" button!
-
Use the Rounding tab and click on Progress Notes, or
-
Use the Admission tab and click H&P Notes, or
-
Use the Discharge tab and click Discharge Summary.
Update the problem list every day and every night, and whenever a new problem is identified.

Handoff Tool
Surg Trauma Check-In: This box of the handoff tool is intended to be used by the overnight APP/resident to communicate with the day team. Any events that occurred overnight or tests that require follow up should be documented in this box. Every order or page needs to be entered in this box. You should also document your decision making process. Include the date of the entry, so that old events can be deleted by the day team.
Present on Admission Trauma Quality Measure


PAWS: Alcohol withdrawal is potentially lethal, but is preventable. Accurately assessing whether a patient is at risk for withdrawal is essential. A PAWS Score must be documented on every trauma patient. If unable to be obtained at the time of admission, it should be documented in tertiary note.
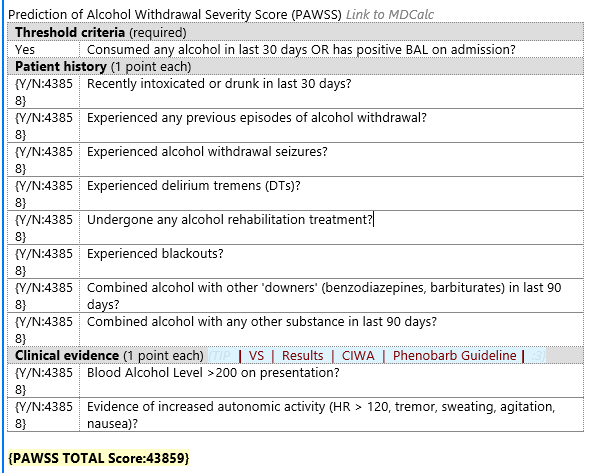
Tertiary Exam
Note type “Trauma Tertiary Survey”
“Tertiary Trauma Quality Improvement” hyperlink located within note or box at the top

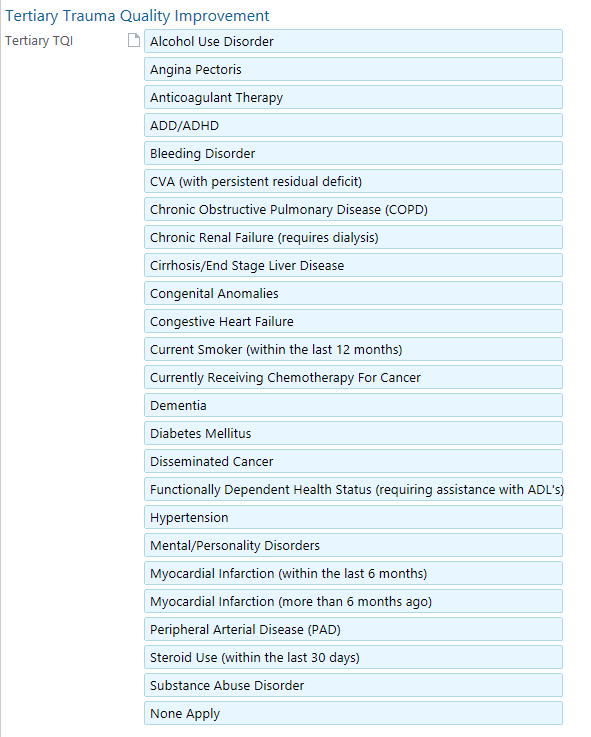
Advanced Care Planning
-
Within first 24 hrs of admission (ideally, at time of trauma tertiary), complete an advanced care planning discussion and assessment with every patient.
-
The ACP discussion should be documented in EPIC under the note type “advanced care planning” using the dotphrase .ACSACPINITIALDISCUSSION
-
All Category II patients require a family meeting within 72 hrs of admission. This follow-up ACP discussion should be documented in EPIC using the note type “advanced care planning” using the dotphrase “.ACSACPFOLLOWUP”



Trauma PI
The trauma team is mandated by American College of Surgeons to review all trauma morbidities and mortalities. In order to review, we need you to report that a morbidity or mortality has occurred.
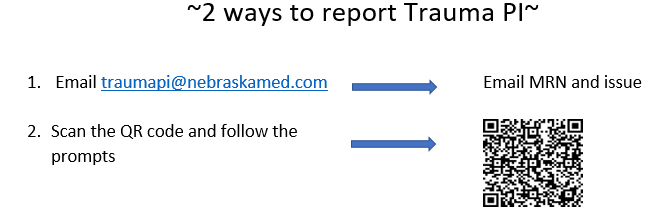
Hospital Based Violence Intervention Program EncompassOmaha
Refer patients by emailing encompass@nebraskamed.com
This program is available for any victim of violence (GSW, SW, assault, etc). It provides culturally competent case management, trauma psychology, and violence intervention resources to patients both in the hospital and in long-term follow up.
Initial Management and Resuscitation
Trauma Team Activation Criteria
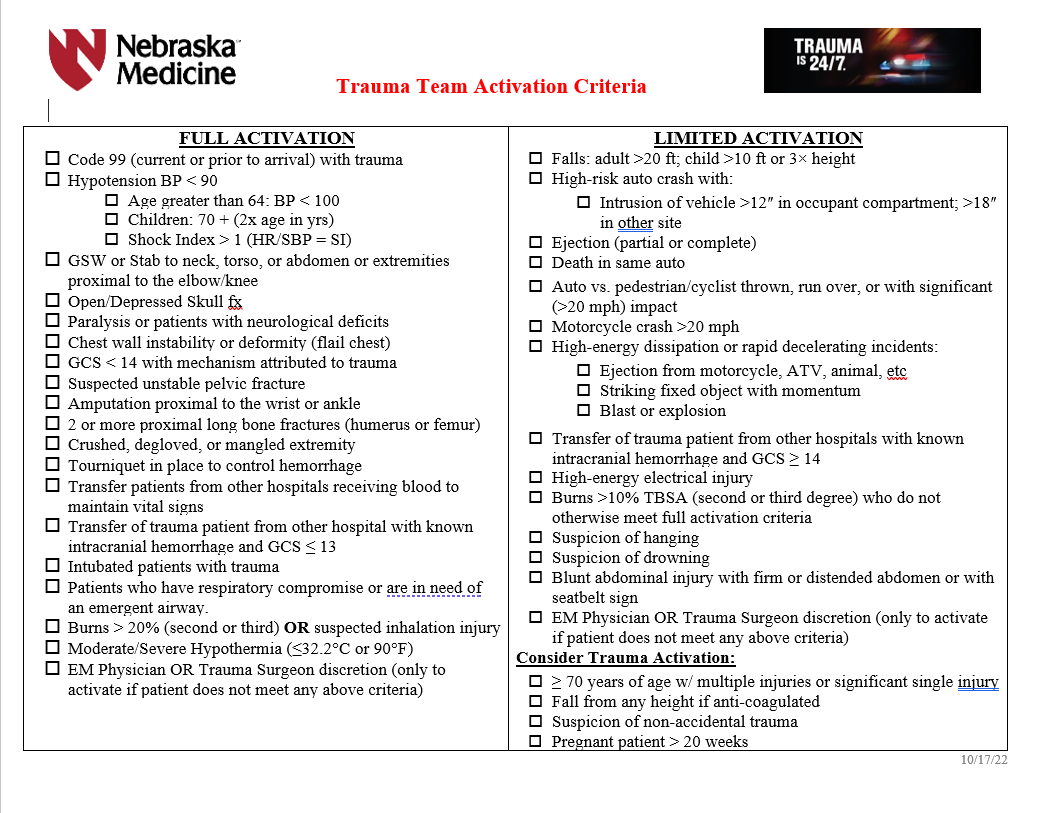
Admission Criteria
ICU ADMISSION
-
Grade IV or greater solid organ injury or Grade III injury with blush/active extravasation
-
Any hemodynamic instability
-
Base deficit >6
-
Pelvic fractures requiring blood transfusion or IR angiogram/embolization
-
Any spine fracture with neurologic deficit
-
Mandible fracture with edema or hematoma
-
Traumatic brain injury with GCS<13
-
Patient >55 yrs of age, on anticoagulation with abnormal CT head
-
Risk of airway compromise
-
High risk rib fracture patient with FRC<1000mL
-
Presence of pulmonary co-morbidities
-
Blunt myocardial injury with new
-
arrythmia
-
hemodynamic instability
-
cardiac failure
-
Unstable spine injury
-
Frontal contusions >2cm
-
Solid organ/pelvis/abdominal injuries with evidence of active extravasation on CT scan
-
Need for q1hr vital signs/neuro-vascular checks/interventions/etc.
-
Trauma attending discretion
SDCC Admission
-
Grade II/III solid organ injury without blush/active extravasation on CT
-
presence of multiple injuries
-
Rib fractures with FRC between 1000mL—1500mL
-
Any patient on pre-injury anticoagulation therapy with an injury not requiring ICU
-
Major soft tissue trauma in patients on anticoagulation therapy
-
Need for q2hr vital signs/neuro-vascular checks/interventions/etc.
-
Presence of multiple co-morbidities
-
Age > 70
-
C-spine fractures exclusive of spinous and transverse process fractures (without neurologic injury)
-
History of sleep apnea who needs narcotics
-
New CPAP/BiPAP requirements
-
Trauma attending discretion
FLOOR Admission
-
All other trauma patients who do not meet criteria for ICU or SDCC admission
Isolated hip fractures requiring total or partial joint replacement may be transferred to Bellevue Medical Center by Orthopedics after full trauma evaluation---Refer to Isolated Orthopedic Transfers to Bellevue Medical Center Requiring Joint Replacement pathway on trauma website
Some isolated pediatric fractures may be transferred to Children’s Nebraska by Orthopedics after full trauma evaluation---this needs to be verbally approved by Dr. Bauman or Dr. Evans before transfer is initiated. Talk to Red attending.
Daily Floor Rounding Checklist for Trauma Patients
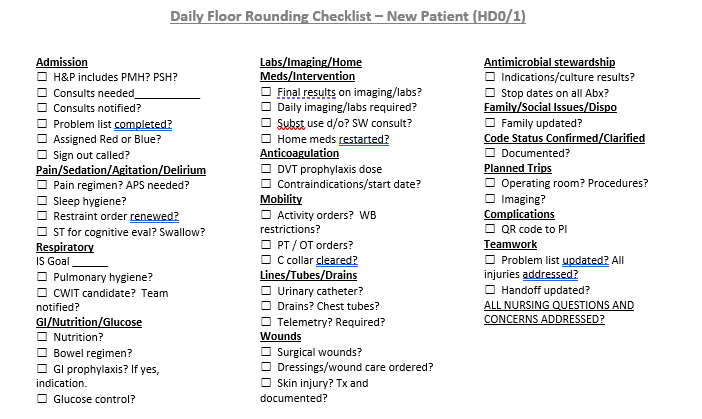
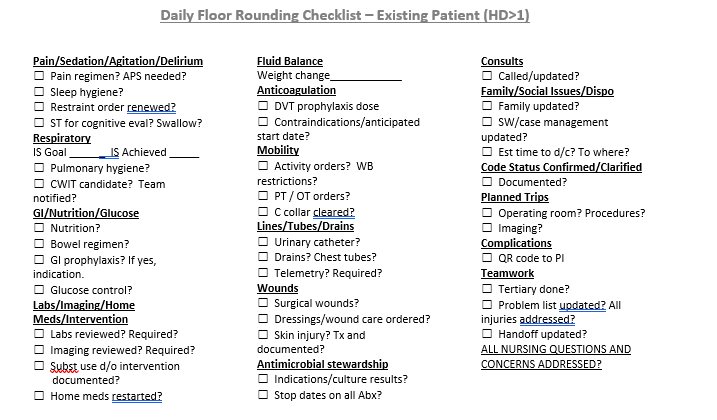
Neurological Trauma
All blunt trauma patients should be placed in c-spine precautions until the cervical spine can be appropriately evaluated and cleared---Refer to Cervical Spine Evaluation and Management on trauma website for C spine precautions, evaluation and clearance
-
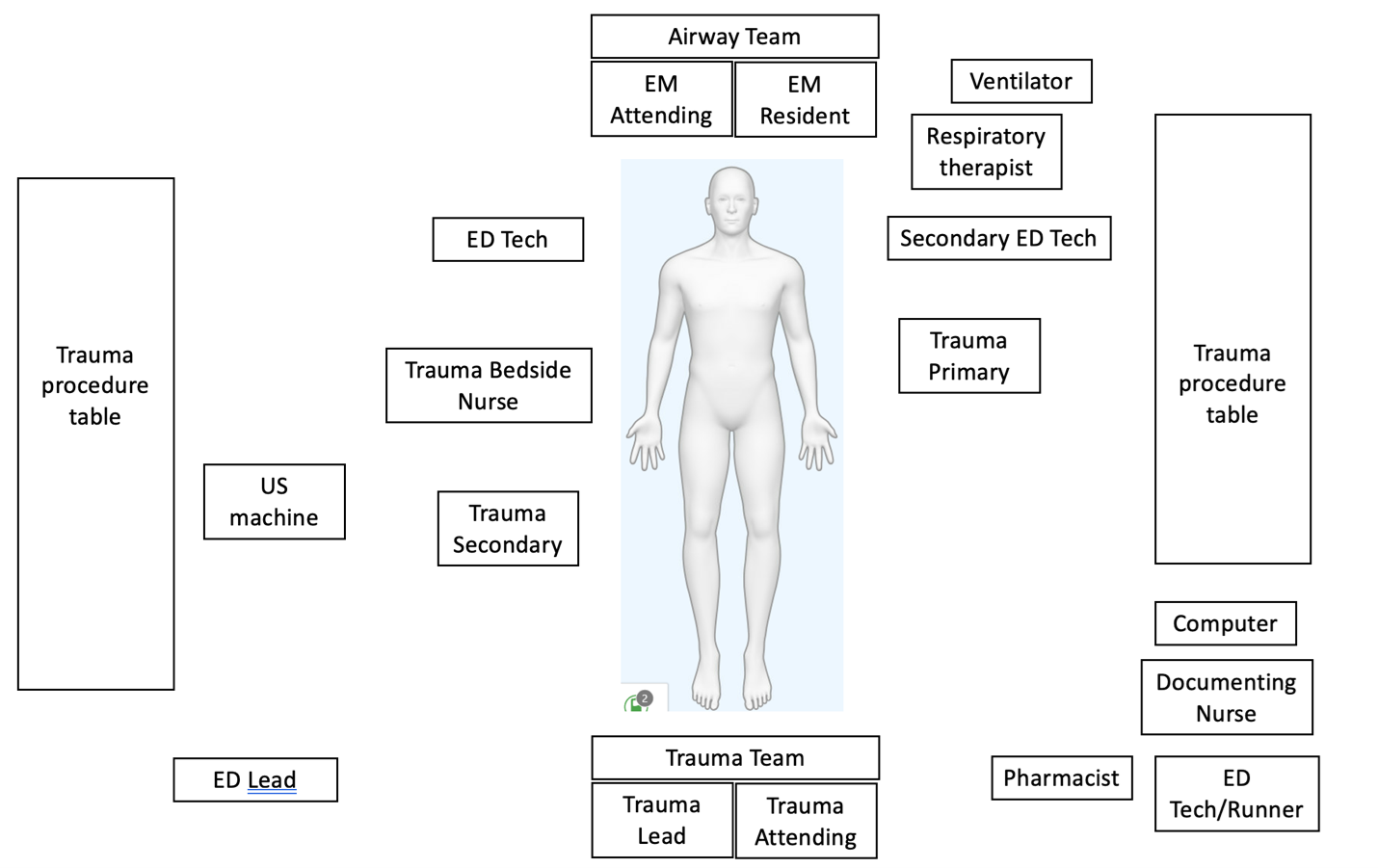
ACS First Start OR Protocol
Purpose
To ensure efficient utilization of operating room (OR) resources and timely case starts by outlining responsibilities for case reassignment at 6:00 a.m
Scope
Applies to all ACS surgeons, OR charge nurses, and ACS staff involved in scheduling and assignment OR cases
Proposed Plan
1. Morning Check
- At 6:00 a.m., the OR charge nurse will review the schedule for OR 1.
- If multiple cases are scheduled in OR 1 and additional rooms are available, the OR charge nurse will text the attending surgeon who has the first-start case scheduled under their name
2. Case Reassignment by Surgeon Type
- Elective-case or Trauma Red Surgeons:
- Upon receiving the text, the surgeon should direct the OR to move the next case (if scheduled under another surgeon) into the additional room.
- It is understood that the surgeon will arrive in time for a 7:30 a.m. case start.
- Emergency General Surgery (EGS) Surgeon:
- The EGS surgeon may choose which case to move into the additional room.
- The moved case should be assigned under the CWIT surgeon.
- If No CWIT Surgeon Available:
- If the CWIT surgeon is unavailable (e.g., already operating), the case should be assigned under the Trauma Blue surgeon.
3. Coverage During Morning Hand-off
- During morning hand-off, if the CWIT or Trauma Blue surgeon is unavailable at the time of case start, an alternate covering surgeon will be identified.
- The OR charge nurse will be notified of the assigned covering surgeon.
4. Surgeon Responsibility for Case Timing
- Any surgeon scheduling a case in advance who cannot be present to start the case as a first-start must indicate this during the case request process.
- This ensures the OR charge nurse will not move the case earlier inadvertently.
Compliance
Adherence to this protocol ensures timely starts and efficient use of OR resources.
Approved on 11/19/2025 by Dr. Charity Evans and Dr. W. T. Hillman Terzian
AGAC-NPs Caring for Pediatric Trauma Patients
Situation: The trauma team at Nebraska Medicine provides care for patients with traumatic injuries throughout the lifespan (neonate to the elderly). Our team consists of faculty physicians, advance practice providers (APPs), fellows, residents, and support staff working in collaboration. Background: APPs on the trauma team include physician assistants (PAs) and nurse practitioners (NPs) with various professional certifications. Specifically, NPs may have Adult Gerontology Acute Care (AGAC-NP), Acute Care Nurse Practitioner (ACNP) or Family Nurse Practitioner (FNP) certification. AGACNP and ACNP scope of practice is generally recognized to be from adolescence into adulthood. FNP scope of practice includes pediatric patients. Assessment: Based on discussion with experts, the DHHS Nursing Practice Consultant and the DHHS Nursing Program Manager, NMC nursing leadership and ACS/trauma APP leadership, experts from DHHS provided the following feedback: The Nebraska Nurse Practice Act is intentionally vague to allow for flexibility in emergent situations. In an emergent situation, the AGAC-NP should do whatever is necessary to stabilize the patient until a pediatric-trained provider is available. Additionally, the DHHS experts emphasized that the person who is (1) available and (2) most qualified to care for the pediatric trauma patient should do so. Recommendation: It is acceptable for NPs with AGAC-NP or ACNP certification (without FNP or pediatric NP certification) to stabilize a pediatric patient until a pediatric-trained provider is available. If a pediatric trained provider and an adult-only trained NP are working together, the pediatric-trained provider should assume care of a pediatric patient as soon as possible. Approved on 1/15/2026 by Kelly Vaughn.