Emergency General Surgery
EGS guidelines
- Adhesive Small Bowel Obstruction (ASBO) Management
- Perforated Peptic Ulcer Disease (PUD) Management
- Ogilvie’s (Acute Colonic Pseudo-obstruction) Management
- EGS Wound Evaluation and Management Guidelines
- Referral Guidance for Surgical Oncology Patients
- STAT Emergency General Surgery Consult Protocol
- Acute Appendicitis Management
- ACS Guidelines for Discharging Patients Home with TPN
Adhesive Small Bowel Obstruction (ASBO) Management


Perforated Peptic Ulcer Disease (PUD) Management


Ogilvie’s (Acute Colonic Pseudo-obstruction) Management


EGS Wound Evaluation and Management Guidelines
Except for wounds and acute infections located in specific anatomic locations managed by other services such as (but not limited to) urology, ENT, breast surgery, and neurosurgery, many of the wounds and acute infections at UNMC will be evaluated and managed by EGS. The decision to defer management to another specialty or subspecialty (e.g., colorectal) may be made at the discretion of the EGS team, but EGS is expected to ensure that proper communication has occurred with that team and, if there is ultimately disagreement over whose responsibility it is to manage that wound or acute infection, EGS will initiate an attending-to-attending discussion to resolve the disagreement. EGS may also be asked by the bed desk (through the trauma phone) to engage in conversations between UNMC inpatient medical services and outside facilities regarding the transfer of inpatients for surgical evaluation.
Necrotizing soft tissue infections:
- EGS is usually consulted early; if another service is better served based on below criteria (e.g., hand surgery or vascular surgery for wounds below the knee), EGS will ensure communication with that team has been facilitated if the appropriate team was not contacted.
- If NSTI is distal to elbow, hand surgery should be on initial transfer call
- If NSTI is distal to knee, vascular surgery should be on initial transfer call
- EGS should not accept NSTIs distal to the elbow or knee without communicating with hand surgery or vascular surgery
- If an ED consult has been placed for an NSTI in these locations to EGS, it is our practice to ensure patient stability and facilitate communication to the appropriate team
Wounds distal to elbow:
- Forearm:
- Superficial infections or simple abscesses of the forearm can be managed by EGS (EGS may consult hand surgery with concern)
- Deep or complex infections of the forearm to be managed by hand surgery
- Wrist or hand:
- Any wound or infection in this location to be managed by hand surgery
Wounds distal to knee:
- Vascular surgery to evaluate and manage
- If hardware is involved, vascular may involve orthopedics at their own discretion
Sacral wounds:
- EGS to manage acutely infected sacral wounds with support from wound care at EGS’ discretion
- Chronic sacral wounds that are not infected may be managed by wound care without an EGS consultation
- Plastic surgery referral is generally done outpatient when reconstruction can be considered
- If plastic surgery operated on a sacral wound within the last six months, plastic surgery should be consulted inpatient to evaluate wound
Post-op infected or dehisced surgical wounds:
- The surgical service that performed the operation should be initially consulted prior to EGS evaluation
- EGS is available to assist with evaluation and management of all post-op surgical wound complications at the operating surgeon’s discretion or if a patient is presenting from an outside facility
Frostbite:
- Acute frostbite (<72 hours since cold exposure):
- Admit to trauma
-
- Consult orthopedics for management and outpatient follow-up
- Consult hand for upper extremity frostbite and outpatient follow-up
-
- Admit to trauma
- Chronic wounds secondary to frostbite (>72 hours since cold exposure):
- If no other injuries or hypothermia, admit to primary home admitting service (Hospital Medicine, UNMC family medicine, or Clarkson Family Medicine)
-
- Consult orthopedics for management and outpatient follow-up
- Consult hand for upper extremity frostbite and outpatient follow-up
-
- If no other injuries or hypothermia, admit to primary home admitting service (Hospital Medicine, UNMC family medicine, or Clarkson Family Medicine)
- Frostbite re-admissions:
- Admit to primary home admitting service (Hospital Medicine, UNMC family medicine, or Clarkson Family Medicine), NOT trauma
-
- Consult orthopedics for management and outpatient follow-up
- Consult hand for upper extremity frostbite and outpatient follow-up
-
- Admit to primary home admitting service (Hospital Medicine, UNMC family medicine, or Clarkson Family Medicine), NOT trauma
Osteomyelitis:
- Orthopedics consultation is not mandatory if the problem can be managed by another service such as EGS, hand, or vascular surgery since orthopedics’ role is largely limited to aggressive debridement and/or amputation
Wound clinic referrals:
- If a patient needs to be expediated to wound clinic, please contact Drs. Sean Figy, James Willcockson, or Kai Yang directly or through EPIC to discuss
Approved 11/19/2025 by W. T. Hillman Terzian, MD (EGS Medical Director), John Tierney, MD (EGS), Sara Putnam, MD (Orthopedics), Jonathan Thompson, MD (Vascular), Sean Figy, MD (Plastics), James Willcockson, MD (Plastics/Hand), Kai Yang, MD (Plastics/Hand), Daniel Firestone, MD (Hand), Joseph Morgan, MD (Hand), Tabatha Matthias, DO (Hospital Medicine), and Morgan Walgren, MD (Hospital Medicine)
Referral Guidance for Surgical Oncology Patients
Lymph node biopsies- Surgical Oncology
Abdominal issues in cancer patients:
- Patient established with UNMC surgical oncology division for malignancy, seen within three years, and issue is related to previous intervention (for example, SBO) - Surgical oncology
- Presenting manifestation related or likely related to primary malignancy - Surgical Oncology or to the appropriate Cancer focused surgery team (e.g., colorectal)
- If discovered intraoperatively, Surgical Oncology consultation is at discretion of EGS staff
i. If surgical oncology assumes care intraoperatively - Surgical oncology
ii. If malignancy determined to not change treatment strategy - EGS
- General surgical conditions (symptomatic cholelithiasis or acute/chronic cholecystitis, acute appendicitis, incarcerated hernia, small bowel obstruction) in patient with active cancer issue (on or off active treatment) or history of malignancy – EGS
Approved by Josh Mammen, MD and Hillman Terzian, MD 6/25/2025
STAT Emergency General Surgery Consult Protocol
STAT Emergency General Surgery Consult Protocol
This protocol is applicable to the timely notification of an emergent patient condition requiring STAT consultation of the Emergency General Surgery (EGS) Service.
CLINICAL MANAGEMENT
A. Notify the EGS team immediately if a patient presents with any of the following known or suspected diagnoses:
1. Unstable patient with high suspicion of surgical abdomen as source
a. Hypotension (SBP < 90, requiring vasopressors)
b. Persistent tachycardia (HR > 120)
c. Signs of end organ failure (mental status changes, renal failure, respiratory failure, etc.)
2. Necrotizing soft tissue infection (NSTI) by physical exam or radiographic evidence
3. Pneumoperitoneum (excluding contained perforation from diverticulitis or appendicitis)
4. Mesenteric ischemia, pneumatosis intestinalis
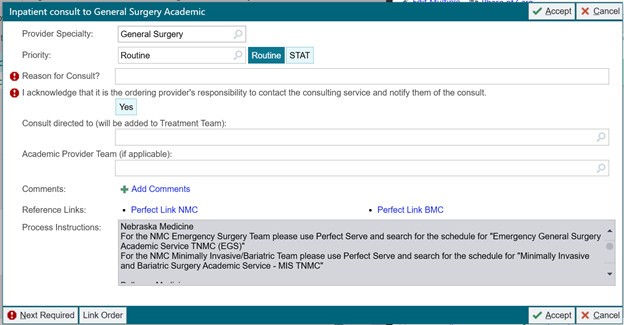
B. Place a “General Surgery” consult order and identify it as “STAT” in the electronic medical record --- see screenshot below
a. Include Emergency General Surgery in the “reason for consult,” along with the indication for consult
C. Send Urgent Perfect Serve message the first-call resident/APP for EGS
D. Patients with a STAT consult will be seen by an EGS provider within 30 minutes of consult order time
E. The EGS provider completing initial patient evaluation will document time the patient was seen in the EGS Consult note
F. Patients requiring emergent surgical intervention will be prepared for the OR and the OR Lead will be notified following current protocols
![]()
Acute Appendicitis Management
![]()
![]()
![]()
![]()
ACS Guidelines for Discharging Patients Home with TPN
ACS Guidelines for Discharging Patients Home with TPN
- Patients should be formally discussed by ACS Faculty at either weekday morning faculty sign-out, Tuesday 7:30 conference, or Wednesday CCC meeting prior to making plans to discharge on outpatient TPN
- First choice is contact the patient’s PCP to see if they can do the TPN
- If the PCP is unable to manage TPN, identify a Complex Care Clinic (CCC) member to take ownership:
- Default to Dr. Tierney. Can consider other CCC Faculty including: Dr. Berning, Dr. Josef, Dr. S. Kemp, Dr. Terzian, and Dr. Veatch
- In general, most of these patients will probably need to be seen in the CCC so consideration should be given to scheduling them there instead of the regular trauma or EGS follow-up clinic
- Unless the discharging surgeon plans to manage the TPN and patient themselves, they must discuss the patient with the staff seeing the patient in follow up at the time of discharge
- IRP will not do TPN for a patient until they have seen them for consultation on outpatient basis in their clinic
- A formal discussion of an ACS patient, that includes at least two CCC members, is required before IRP consultation
- Ensure adequate long-term access plan
- PICC is acceptable. Patient needs to understand care instructions
- Ensure home health care orders are entered.
- Confirm that CTN has identified what specialty pharmacy the patient will be using and provide them with the CCC Faculty’s name and fax number (402-836-9459) for them to send TPN adjustment orders
- We have used Option Care with success for those in the Omaha area, although there are other options including the Nebraska Medicine infusion center
- Ensure weekly labs are ordered (CMP, phosphorus, magnesium, CBC, triglycerides) with results going to the pharmacy and the surgeon; it’s possible that the CCC member will have to order these labs personally for them to be routed back correctly
- For the surgeon managing the TPN, after 3 months of stability consider checking iron panel and trace elements (chromium, copper, manganese, selenium, and zinc) if the patient is still on TPN that we are managing
Approved 6/3/2026 by Margaret A. Baumann, APRN, Emergency General Surgery Program Leader and W. T. Hillman Terzian, MD, Emergency General Surgery Medical Director