Surgical Critical Care
SCC guidelines
- CCS Orientation Material
- Surgical Critical Care Literature
- CCS Logistic Documents
- Neurologic
- Cardiovascular
- Pulmonary
- Gastrointestinal
- Fluids/Electrolytes/Nutrition
- Hematologic
- Bedside ICU Procedures
- Service Specific Protocols
CCS Orientation Material
CCS Orientation
Objectives
• Describe the most current evidence-based medical practices pertaining to the treatment of critically ill patients in the SICU.
• Demonstrate knowledge and competency in resuscitation skills including advanced cardiopulmonary resuscitation, emergent airway management using bag and mask ventilation, and indications for intubation and mechanical ventilation.
• Demonstrate knowledge and competency in ventilator management including the use of PEEP, supplemental oxygen, lung protective ventilation strategies, pressure-cycled, volume-cycled and dual modes of ventilation
• Apply evidence-based guidelines to the care of patients with critical illness or injury such as ventilatory management for patients with ARDS, weaning from mechanical ventilation, hemodynamic monitoring, administration of nutritional support, renal failure, antibiotic administration, blood product transfusion and prevention of ICU related complications.
• Demonstrate knowledge and competency in the evaluation and non-operative management of severe closed head injury with or without intracranial hypertension.
• State the etiology, describe the pathophysiology, and demonstrate the appropriate management of patients with spinal cord injury
• Demonstrate proper performance of brain death certification and apply clinical criteria of brain death and basic principles of support for potential organ donors.
• Demonstrate competency in the performance of procedures, specifically central and arterial lines, and chest tubes and POCUS
• Demonstrate effective daily communication with consultants and other surgical services
• Demonstrate effective discussion of patient diagnosis, prognosis and management plan (including risks, benefits and side effects) with patient and family using simple, easily understood language
• Demonstrate the practice of ethical principals in relation to patient care and confidentiality, including obtaining informed consent, implementing “Do Not Resuscitate” orders, withholding or withdrawing life support, and clarifying goals of care from advanced directives
The Team
• Attending Intensivist (SCC, ACC)
• Advanced Practice Providers (Day and Night)
• Critical Care Fellows (Surgery, Medicine, Anesthesia, EM)
• Residents
• Medical Students
• SICU Nursing Manager
• Critical Care nurses
• Case managers and social workers
• Registered dietician
• Pharmacy
• Respiratory Therapy
• Physical, Occupational and Speech Therapy
Pagers and PerfectServe
888-0282 is the Green CCS (8th fl ICUs) pager
• Resident carries Green CCS pager during day and night
• New consults will route through the green pager - equitable distribution of consults between residents and APPs should occur
• 888-3005 is the Yellow CCS (non 8th fl ICUs) pager
• APP will carry Yellow CCS pager during day and night
• Both pagers are passed off during shift handoff.
• Utilization of PerfectServe is required.
Check to see that Perfect Serve is active on your phone!
SICU Workspace
• Constant physical presence in the SICU is required: Reduces pages, recognizes decline, promotes collaboration
• Workspace in the work room in hall on 8th floor (Across from family waiting room)
• CODE: 3005

CCS Day Flow
12-hour shift: 6AM to 6PM (You do not need to arrive before 6AM)
6AM – Night shift handoff in the Clarkson 8th fl ICU work room. Yellow and Green teams
6AM-8:30AM Preround on assigned patients, review labs and images, physical exam
Daily Rounds (8:30AM) – Multidisciplinary, Systems based rounding. Starting locations: Green – 8th floor SICU Yellow – Discretion of attending
Afternoons: Finish Notes, Bedside Procedures, Tertiary Exams, See new consults
6PM – Day shift handoff in the Clarkson 8th fl ICU work room. Yellow and Green teams.
CCS Day Attending shifts: 7AM – 4PM
Multidisciplinary Rounds
Rounding in the SICU begins @ 8:30 AM
- Multidisciplinary: Attending, Fellow, Residents, APP, Medical Students, Pharmacy, Dietitian, Nursing, PT/OT/ST.
- Systems based presentations
- One person responsible for placing orders in real time.
- If not presenting, stay engaged.
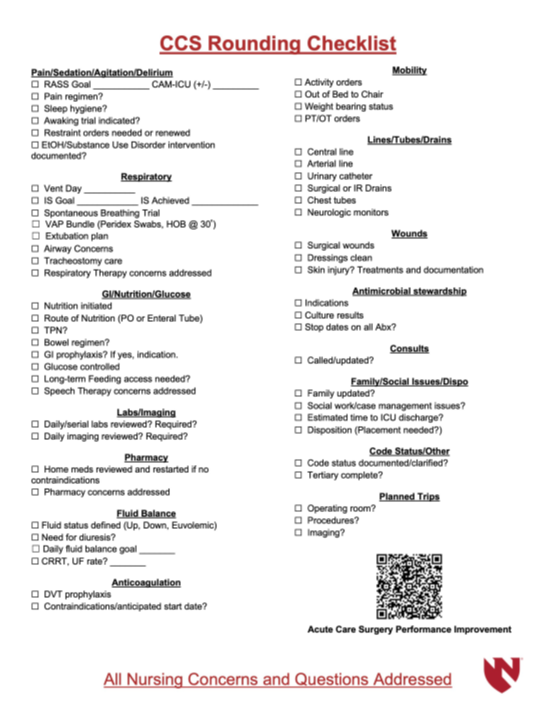
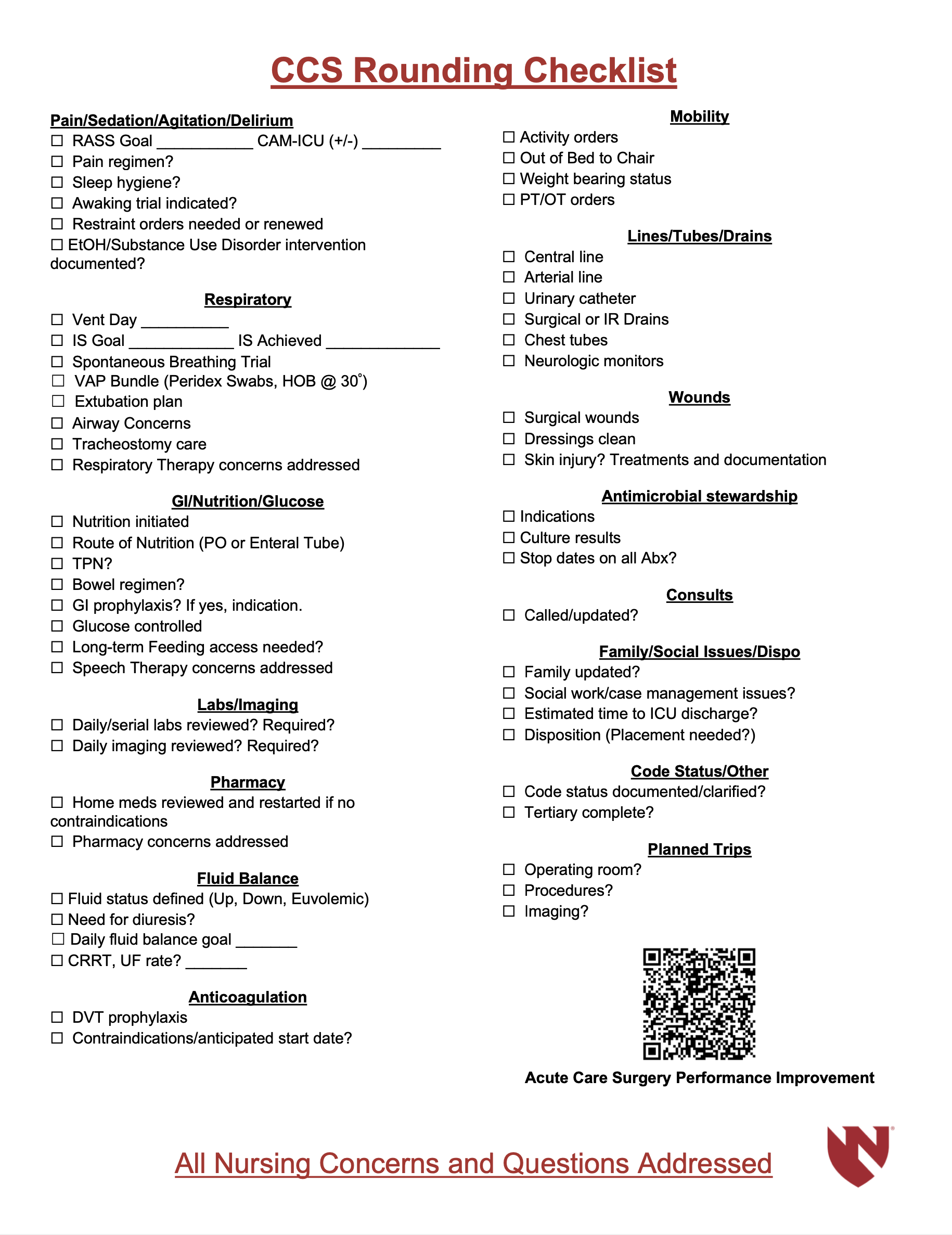
- CCS Rounding Checklist to be completed on every patient daily.
1:00 PM Case Management SICU RADAR Rounds
• Attending/Fellow must attend
• SICU Workroom
• Communicate with case managers and social work for potential discharges
and patient needs
Trauma Care Transition Nurses
• Terese Koubsky- care transitions 402-672-0274
• Molli Kies- care transitions 402-990-0874
1:30 pm Transplant rounds (except Weds, at 1:00 pm)
• One member of the SCC team must be present, and must have adequate
knowledge about every transplant patient
• Can be earlier or later, make friends with the transplant residents and
APPs
• Be engaged, provide additional patient information as needed
CCS is a consult service
- All patients on the CCS service require a consult note.
For important issues, text/call collaborators to discuss before orders are executed
– Examples: Activity, Diet, Transfusions - At least once per day…
CCS must touch base with services (Transplant, Trauma, EGS, MIS, Colorectal) for to discuss issues and plans related to our shared patients
New Patients
• Respond quickly and professionally to ALL requests for patient evaluation
• Physically see the patient in their current location
• Plan formulated as a collaborative effort between both the ICU and primary teams.
• Communicate with attending intensivist
• Call for help if needed early.
• Add to CCS list, place ICU admission orders, write consult note.
Requesting New Consults
• Before calling a consult, make sure:
• Faculty/Fellow is aware
• Is patient following a UNMC physician as an outpatient?
• You have enough patient information to adequately answer consultant questions
• Know what you are asking the consultant to do
• Enter an order in the computer AND
• Make verbal/PerfectServe contact with MD or APP on consult team
Daily Progress Notes
• All patients on the CCS service require a daily progress note.
• Patients with consult note after 12:00 am still require a daily progress note to communicate updated plans.
• Procedural notes, discharge summaries due at time of event
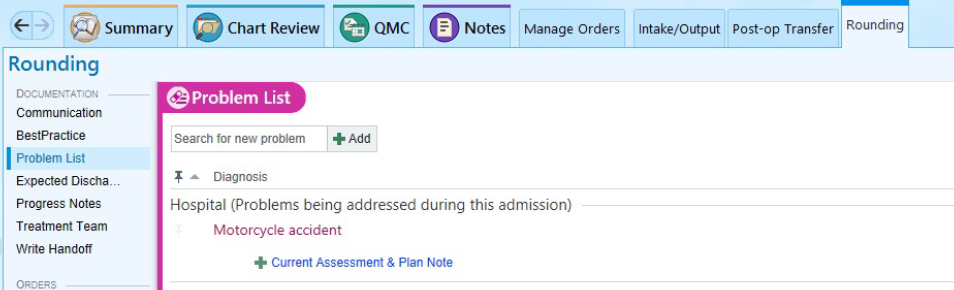
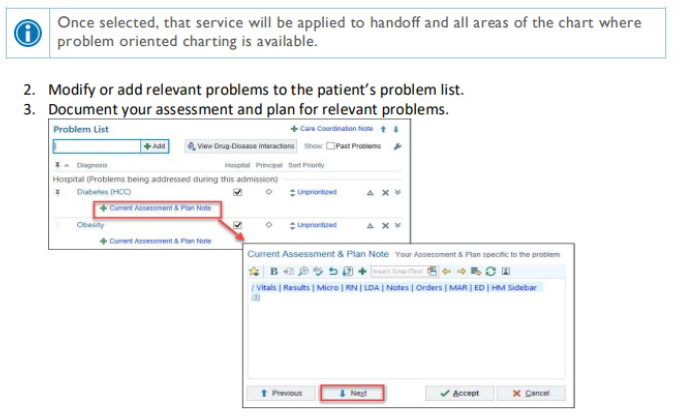
• Create daily progress note through rounding tab. Problem based charting.
• Update problem list frequently.

Daily Review of All Orders
• Review orders and remove unnecessary orders daily
• Do not use Nursing Communication or verbal order to modify orders or hold medications
• Do not use Nursing Communication or verbal order to change target RASS.
• Enter new target RASS in Ventilator Management order set.
• Restraint Orders expire every 24 hours
• Address all expiring orders during rounds each day (Re-order or D/C)
• When restraints are first ordered:
• Set “Hours” so order will expire around 7 AM next day
Night Flow
• Night ICU attending will round with you between 9-10 pm
• Review all patients before rounds
• Complete items to assist day team:
• Populate the problem list, update the patient list
• Attend Trauma Activations
• Review all orders
• Tertiary Exams
Must call attending for:
- New patients BEFORE arrival
- Unstable patients
- ALL codes, procedures, intubations
- There is no silly question…
We are here to support you and care for patients!
Tertiary Exams
• Should be completed overnight, when applicable
• Must be done within 24 hrs OR prior to patient’s transfer to the floor if less than 24 hrs
• AND repeat once the patient can participate (specifically, in head injured or intubated patients)
• Can be done by a medical student BUT the physical exam MUST BE repeated by a resident or attending, and
documented in the chart
• Review all imaging yourself. Ensure that final reads are submitted for every study, and that every injury has been
addressed (ie. facial fracture--à Face was consulted)
• Called .TraumaTertiarySurvey in One Chart
Handoffs
6 PM/AM Face-to-face handoff between day to night team in 8th fl SICU work room
• Concise, focused, discuss unstable patients in detail
• Entire sign out should take less than 20 minutes
Structure:
Who is present, what is your role?
Any acutely ill, deteriorating patients who need to be addressed first?
CCS reports patient, active problems, anticipated problems, pending tests/consults
Daily Handoff Tool
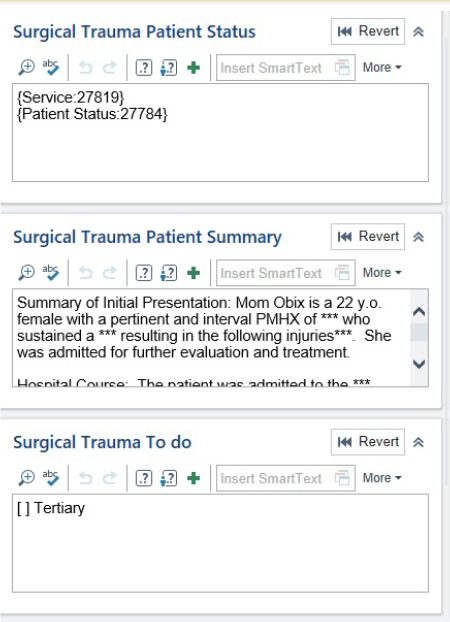
Surgical Patient Status
• Daily APP/Resident Assignment
• Acuity level of patient (stable/watcher)
Surgical Patient Summary
• Utilized as a running discharge and written in a high-level, past-tense overview.
– Use dates as “anchors” for significant events
Surgical Trauma To Do
• [ ] Tertiary will automatically populate on all new patients
• Identify significant imaging/assessment items that need to be followed up on
These sections need to be updated every day
Code Blue Coverage
• All hospital codes will be paged to the CCS pagers.
• If ACS patient, CCS needs to respond.
• A member of the CCS team must be the
TEAM LEADER for all Codes for CCS patients
• Code team will also arrive. Code team is there to assist you.
Significant Event Documentation
All significant events need to be well documented in the chart.
- Includes: Patient status changes, interventions and family conversations
- Communication in both written and verbal forms vital to ensure high quality care for our patients.
ICU to Floor Transfers
1. ICU residents and APPs will place the floor orders when a patient is ready for transfer out of the ICU
2. ICU residents and APPs will communicate to the floor resident or APP at time of decision to transfer.
3. Review orders closely, Discontinue all ICU related orders.
4. The rounding tab needs to be updated. Remove all CCS related rounding information.
5. After these steps are complete, the patient can be removed from the CCS list.
OR to ICU Handoffs
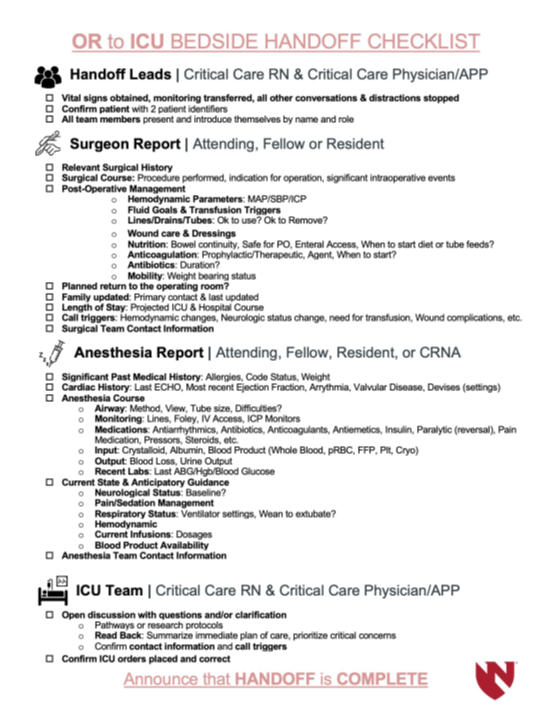
-All patient who return to the ICU directly from the OR require a formal OR to ICU handoff with CCS, Nursing, Anesthesia and Surgery present at bedside.
-45-minute call from lead RN: look the patient up, and intra-op record
-15-minute call: ensure that someone from CCS goes immediately to that ICU room
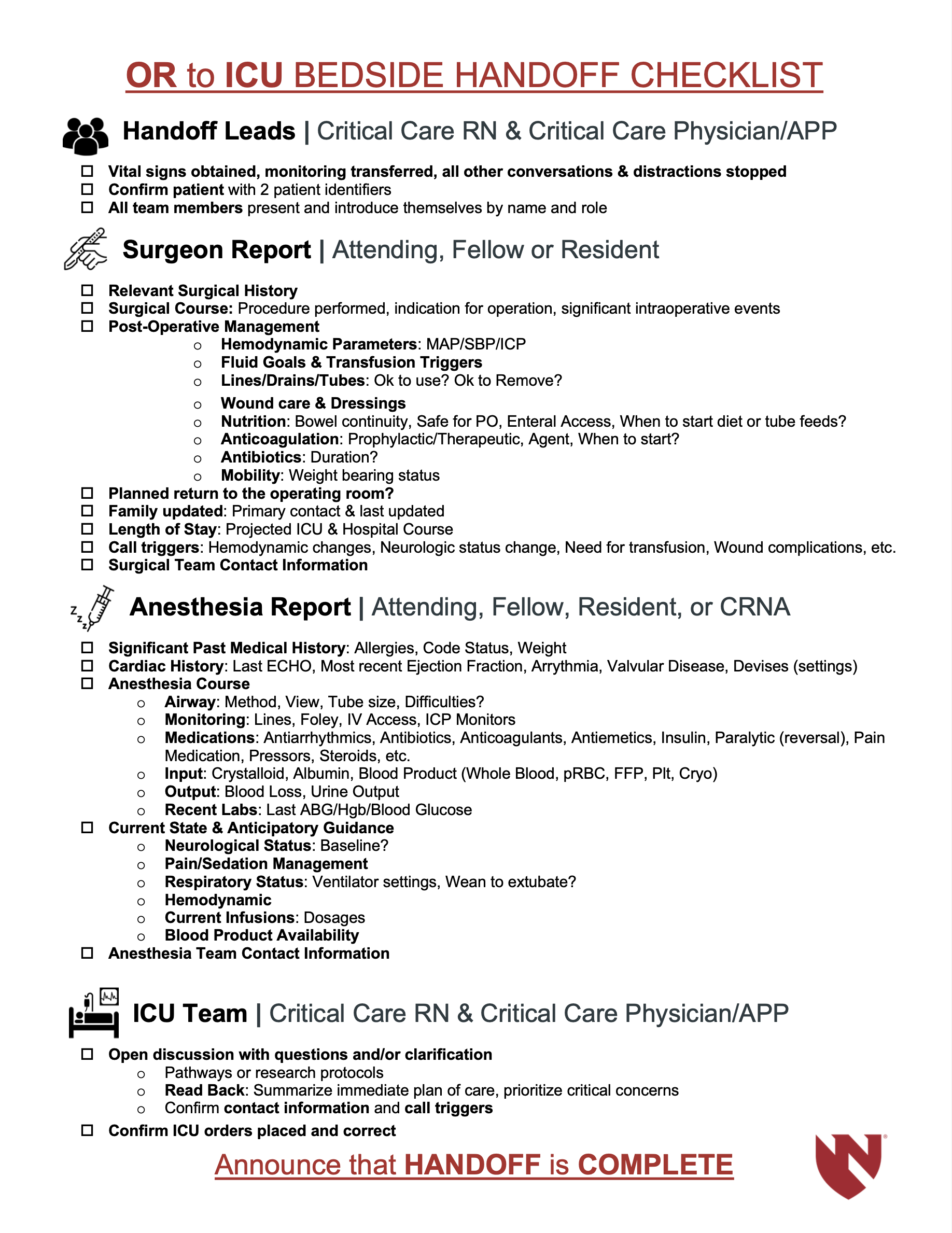
-Use the OR to ICU Handoff Checklist posted in each room to guide handoff between CCS, nursing, anesthesia and surgery teams.
-Post-op note (.APPpostop) or new consult note required.
Procedures
• Notify faculty before performing any invasive procedure
• After procedure, write a procedure note
• Assign note to attending who oversaw the procedure
• Order and follow up on appropriate postprocedural testing (CXR after bronchoscopy or CVC placement)
Vents and Pumps
-Please do not change ventilator settings. Only and Attending/Fellow or RT is allowed to do this.
-You will be asked to change vent orders. Any time a vent setting is changed an order must be placed.
-We do want you to become more comfortable with patients on the vent. Ask Attending/Fellow/RT questions.
-Do not adjust IV infusion pump without prior permission from the RN
Pediatric Patients
• CCS can care for pediatric patients
• Consult PICU service at the discretion of the CCS/Trauma attending
• When co-managing a patient (trauma patient on ECMO, PICU), ensure daily communication with managing service
Intubations on CCS
• Ask the RN to “Call for stat intubation,”
• This gets the Lead RN, anesthesiologist, the RT and the Pharmacist present at bedside
• Know information about your patient
• Current labs, including K
• Prior intubations, ETT size, difficulty
• Current reason for intubation
• Majority of intubations are performed by the anesthesia team.
Departmental Education
• You are excused for your weekly departmental education.
• You are expected to be present before and after this protected education time.
• Please discuss with your program director if you are required to be present on a scheduled day off.
• Please support each other in ensuring all can attend their department’s education, while maintaining safe and high-quality patient care.
• Division Education
Tuesday: 7:30 AM - ACS Resident Education
12:00 PM – Surgical Critical Care Fellows Lecture
Surgical Critical Care Literature
New Page
CCS Logistic Documents
CCS Rounding Checklist
OR to ICU Handoff
Neurologic
Indications to Consult Neuro Critical Care
Overview: The UNMC Neurocritical Care Service will provide consult service to assist in the care of patients in adult ICUs. The Neurocritical Care Consult service will not replace either the Neurology Consult Service or the Stroke Service. The goal is to assist in management of critical neurologic issues in patients being managed with other critical care needs.
The inpatient Neurocritical care service is available: 24/7. The team can see youth ages 6 and above, and all adults.
For youth ages <5, pediatric Neurology is available to interpret EEGs.
Patients for whom consultation would be appropriate:
- Need EEG (POC or continuous) with concern for seizure
- Management of seizures/status epilepticus
- Evaluation of encephalopathies
- Meningitis/encephalitis
- Prognosis of anoxic injury
- Traumatic brain injury
- Patient requiring Tier 2 treatment with neuromuscular paralysis for intracranial hypertension or MAP challenge
- Patient requiring Level 3 treatment with barbiturate coma for intracranial hypertension
- Other critical neurologic issues
A neurocritical care attending will round daily on all consults and in conjunction with SCC team (time TBD)
Stroke Codes should continue to be called for all acute events where stroke is suspected in order to expedite appropriate evaluation and acute intervention by the Stroke Service.
To arrange for neurocritical care consultation in EPIC order the academic Neurology consult and in the perfect serve communication add “neurocritical care consult”.
A Perfect Serve link for communication with the Neurocritical Care Service exists.
For questions, concerns, problems call Dr Gress, (434) 981-9366
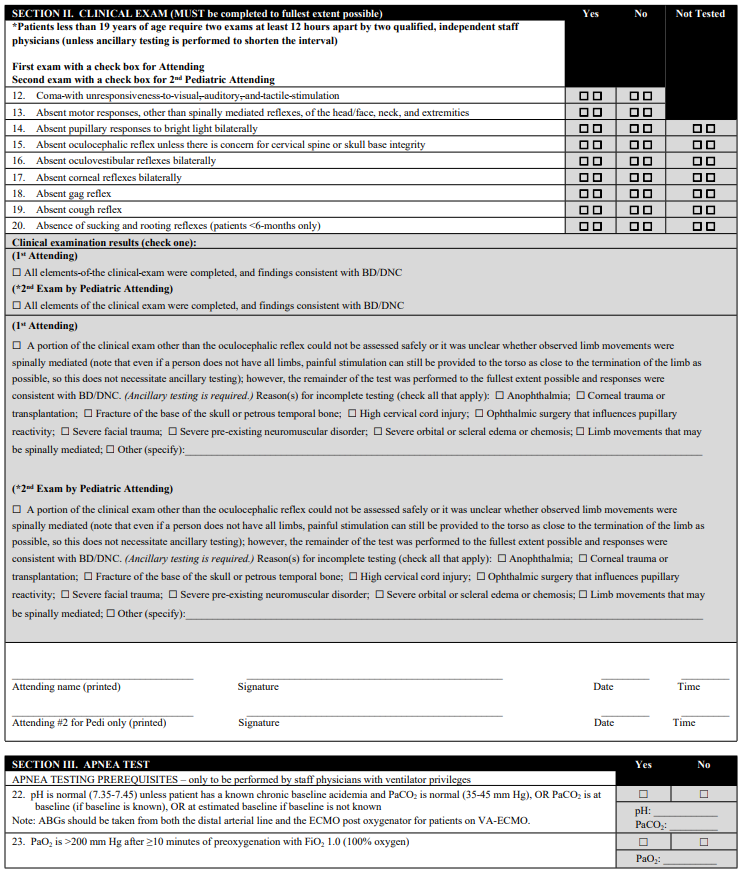
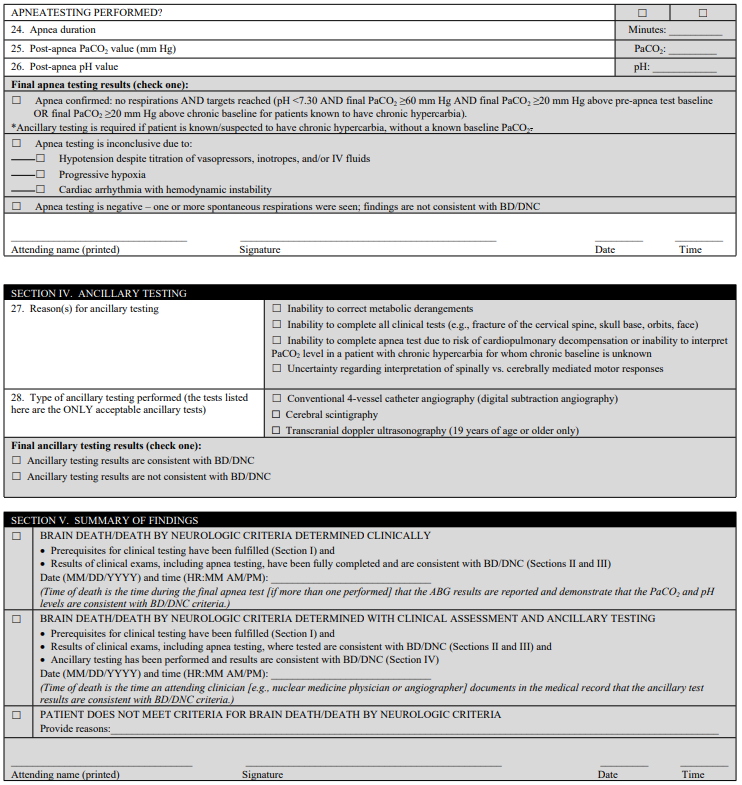
Nebraska Medicine Brain Death Criteria
Nebraska Medicine Policy Number: MS 29
Purpose
To give an accurate and complete description required to establish a diagnosis of breath death/Death by Neurological Criteria (BD/DNC), and to describe the roles and responsibilities of various clinicians and staff members in the process.
Scope
This policy applies to all patients at least 37 weeks corrected gestational age or older at Nebraska Medicine for whom a diagnosis of BD/DNC is considered.
Background
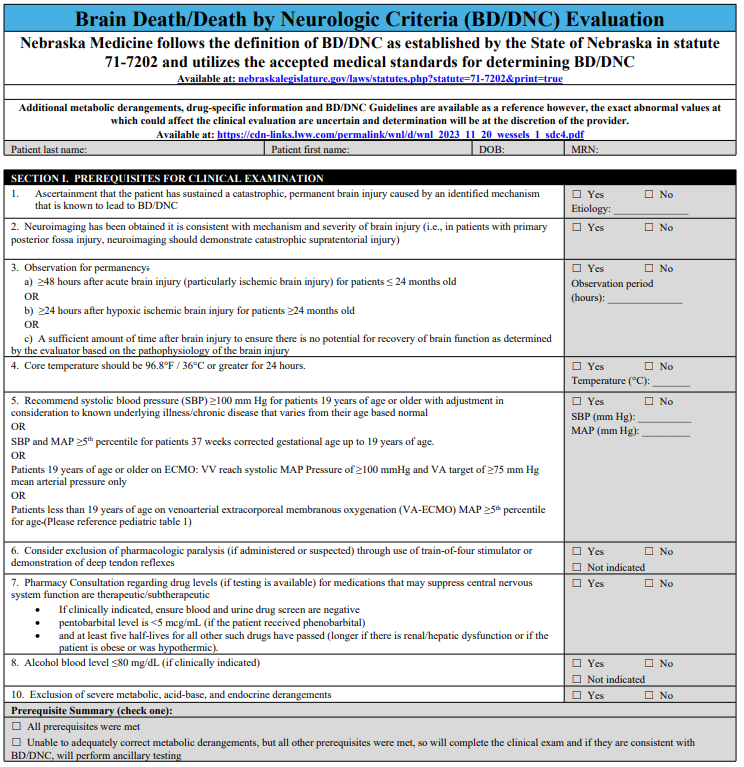
Nebraska Medicine follows the definition of BD/DNC as established by the State of Nebraska in statute 71-7202 and utilizes the accepted medical standards for determining BD/DNC.
A diagnosis of breath death is a clinical diagnosis that can only be established by a staff physician with privileges in neurology or critical/intensive care medicine. The staff physician will document the results of the brain death evaluation in the medical record. The time of death is determined at the time the evaluation is complete. Physicians in training, who are at an advanced level of training and deemed appropriate by the staff physician and working under the staff physician's direct supervision, can perform parts of the examination. The staff physician is fully responsible for the diagnosis, declaration, and documentation of brain death.
Brain Death Evaluation
A complete brain death evaluation consists of three components. All three components must be completed to establish a diagnosis of brain death:
- Establish permanent and proximate cause of coma
- Establish absence of cortical function and brain stem reflexes by neurologic examination
- Establish absence of spontaneous respirations by performing an apnea test
Completion of the three components of the brain death evaluation is sufficient to establish a diagnosis of brain death.
Ancillary Testing
Ancillary testing is not required if all three of the above components are completed. Ancillary tests may be used to support the diagnosis of brain death when uncertainty exists about the reliability of parts of the neurologic exam, when parts of the exam cannot be performed, or to shorten the interval between exams. the current acceptable ancillary tests are: Cerebral angiography, cerebral scintigraphy, and transcranial doppler (if age appropriate).
The interpretation of these tests must be interpreted by a staff physician with the required level of expertise.
Special circumstances:
- Physicians with recognized or potential conflicts of interest in relation to the outcome of the patient's care must remove themselves from the BD/DNC evaluation. For instance, a transplant service physician whose patient expires and has the potential for organ donation should excuse himself/herself from declaring the patient brain dead.
References
- Nebraska State Statute 71-7202. Determination of death. Source: Laws 1992, LB 906, 2.
- Pediatric and Adult Brain Death/Death by Neurologic Criteria Consensus Guideline. Neurology. Dec 12, 2023 issue: 101(24):1112-1132. Greer DM, Kirschen MP, Lewis A, Gronseth GS, Rae-Grant A, Ashwal S, Babu MA, Bauer DF, Billinghurst L, Corey A, Partap S, Rubin MA, Shutter L, Takahashi C, Tasker RC, Varelas PN, Wijdicks E, Bennett A, Wessels SR, Halperin JJ.
- The 2023 AAN/AAP/CNS/SCCM Pediatric and Adult Brain Death/Death by Neurologic Criteria Consensus Practice Guideline. A Comparison with the 2010 and 2011 Guidelines. Ariane Lewis, MD https://orcid.org/0000-0002-075807320, Matthew P. Kirschen MD, PhD https://orcid.org/0000-0003-358502687, and David Greer, MD https://orcid.org/0000-0002-2026-8333 AUTHORS INFO & AFFILIATIONS. December 2023 issue.
Related Policies and Procedures
Acute Bereavement Care -- TX02
Staff Accountability:
- Critical Care Medicine (09/2024)
- Medical Ethics Committee (09/2024)
- Pediatric Quality Committee (11/2024)
- Medical Staff Bylaws Committee NMC (11/2024)
- Medical Staff Medical Executive Committee NMC (11/2024)
- Board of Directors (11/2024)
Cardiovascular
Evaluation and Management of Atrial Fibrillation
Purpose
- Establish a unified guideline for the diagnosis and treatment of atrial fibrillation (AF) in Acute Care Surgery patients.
Background/Definitions
- Primary AF: AF with no precipitating cause
- Secondary AF: AF precipitated by a secondary or reversible cause (e.g., volume overload, surgery, sepsis, etc. --most of your ICU patients)
Inclusion Criteria
- Patients with new onset atrial fibrillation.
Exclusion Criteria
- Patients with chronic atrial fibrillation.
Diagnostic Evaluation
- History:
- previous history of arrhythmia?
- currently on anticoagulation?
- Physical:
- irregular heart rhythm
- Imaging/Labs/Tests:
- ECG
- BMP+Mg+Phos
- Other labs at discretion of provider (CBC, blood cultures/infectious work-up, cardiac enzymes, etc)
Practice Recommendations for Management
- New-onset, secondary AF is an organ dysfunction that signals something is wrong--need to address underlying cause while seeking to control rate/rhythm.
- Helpful questions to guide initial approach of patient with AF:
- 1) is the AF causing an immediate problem?
- 2)why is AF happening now (is this primary or secondary AF)?
- 3) should I worry about longer-term problems from the AF? ?
- Is the AF causing an immediate problem?
- When to consider rhythm control first:
-
- Emergent AF with severe decompensation:
-
- hypotension (SBP<100 or <110 for patients 65 and older), acute heart failure, altered mental status, cardiac ischemia
- if yes --> DCCV (direct current cardioversion)
- consider pairing DCCV with anti-arrhythmic such as amiodarone to increase probability of longer-term success.
-
- Non-emergent AF:
-
- consider a rhythm control strategy first if you think the patient needs atrial kick (i.e. severe mitral stenosis, aortic stenosis) or cannot tolerate nodal blocker (Wolf Parkinson White Syndrome)
-
- Emergent AF with severe decompensation:
-
- When to consider rate control first:
-
- Note: in most instances you can use rate control FIRST.
- Heart rate is higher than it would be with acute illness, but not immediately life threatening to require DCCV.
- Patient has contraindications to anticoagulation.
- Evidence to support a rate control strategy first during secondary AF: success of DCCV is low in secondary AF (as in ICU) --43% at 1 hr, 23% at 24 hrs remain in NSR.
-
- When to consider rhythm control first:
- Why is AF happening now?
- Fix electrolytes (magnesium is an effective rhythm control treatment).
- Fix volume status.
- Look for untreated infection.
- Remove beta-agonists.
- Should I worry about long-term problems from the AF?
- Arterial thromboembolism and AF recurrence are long-term concerns after new-onset AF in critically ill patients
-
- 44% af AF recurrence in 1 year after new-onset AF in sepsis.
-
- Cardiology follow-up (either inpatient or outpatient) for long-term rhythm monitoring and treatment plan should be considered.
- Arterial thromboembolism and AF recurrence are long-term concerns after new-onset AF in critically ill patients
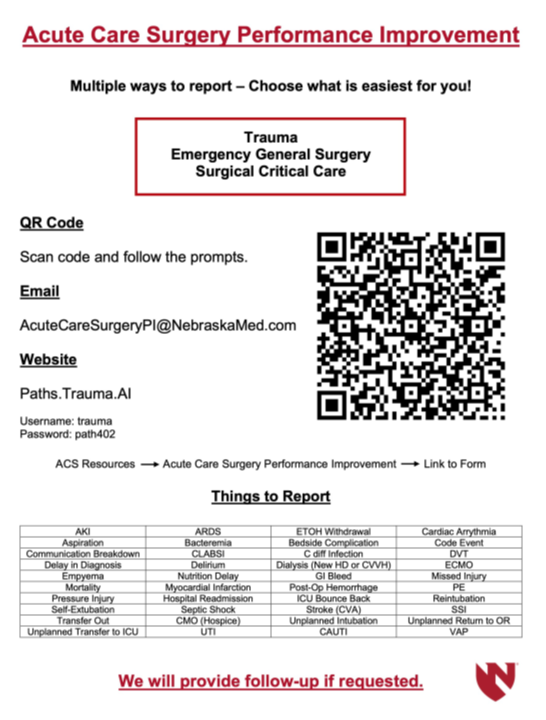
Outcome Measures and Guideline Adherence
- AF (arrhythmia) is a PI filters for Trauma and Critical Care Surgery that is actively tracked/monitored.
Related Policies
Key Contributors
- Keely Buesing ,MD, FACS, Acute Care Surgery Division
Last Updated
February, 2023
References
- 2019 AHA/ACC/HRS Update
- 2014 AHA/ACC/HRS Guideline
- Um K et al. Pre- and post-treatment with amiodarone for elective electrical cardioversion of atrial fibrillation: a systematic review and meta-analysis. Europace. 2019;21(6):856-863.
- Arrigo M et al. Disappointing success of electrical cardioversion for new-onset atrial fibrillation in cardiosurgical ICU patients. Crit Care Med. 2015;43(11):2354-2359.
- Walkey AJ et al. Practice patterns and outcomes of treatments for atrial fibrillation during sepsis: a propensity-matched cohort study. Chest. 2016;149:74-83.
- Bosch NA et al. Comparative effectiveness of heart rate control medications for the treatment of sepsis-associated atrial fibrillation. Chest. 2021;159(4):1452-1459.
- Davey MJ et al. A randomized controlled trial of magnesium sulfate, in addition to usual care, for rate control in atrial fibrillation. Ann Emerg Med. 2005;45(4):347-353.
- Onalan O et al. Meta-analysis of magnesium therapy for the acute management of rapid atrial fibrillation. Am J Cardiol. 2007;99(12):1726-1732.
- Bosch NA et al. Atrial fibrillation in the ICU. Chest. 2018;154:1424-1434.
Supplemental Materials
- “Etiology of Atrial Fibrillation” schematic.
Pulmonary
Airway Pressure Release Ventilation (APRV, Bivent)
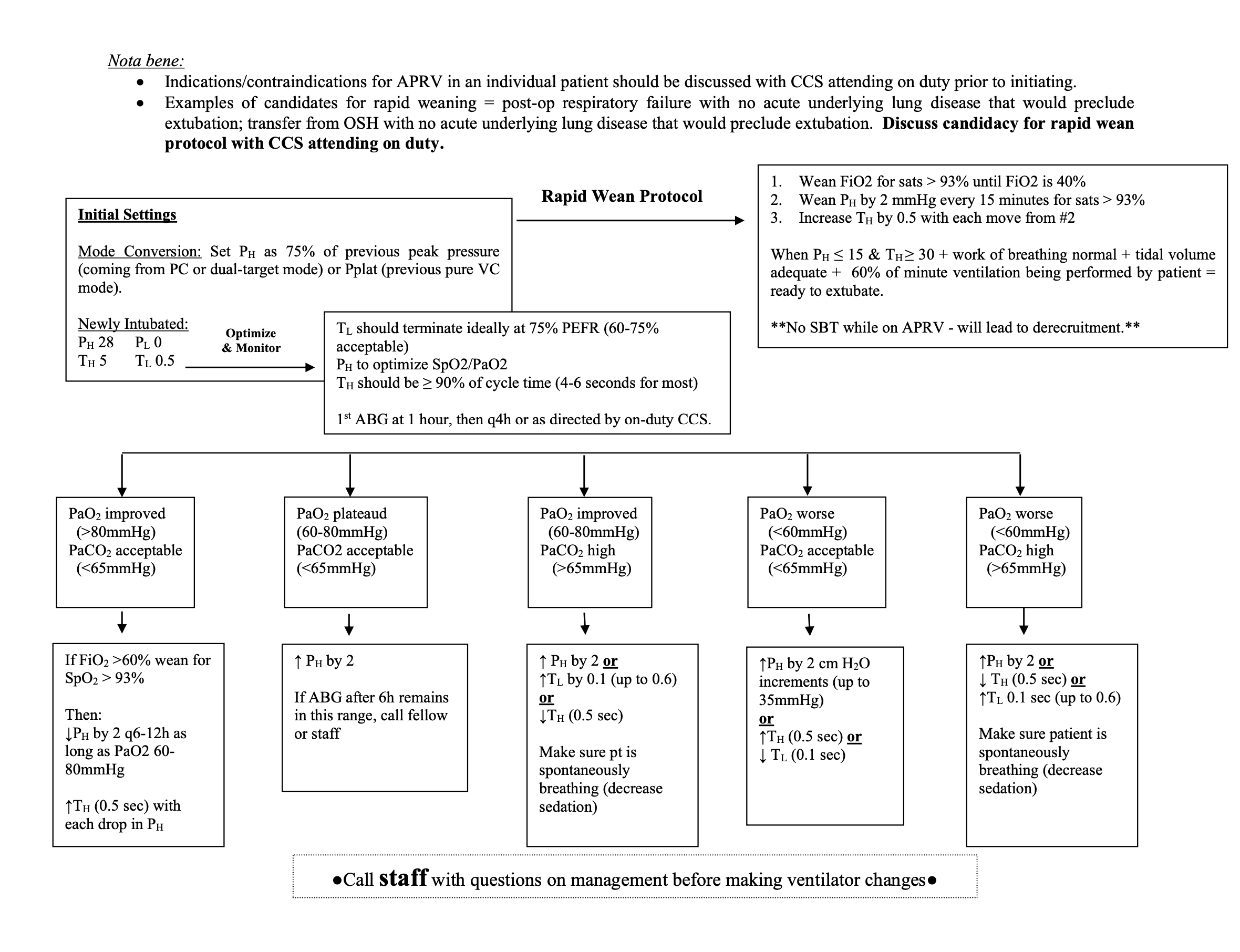
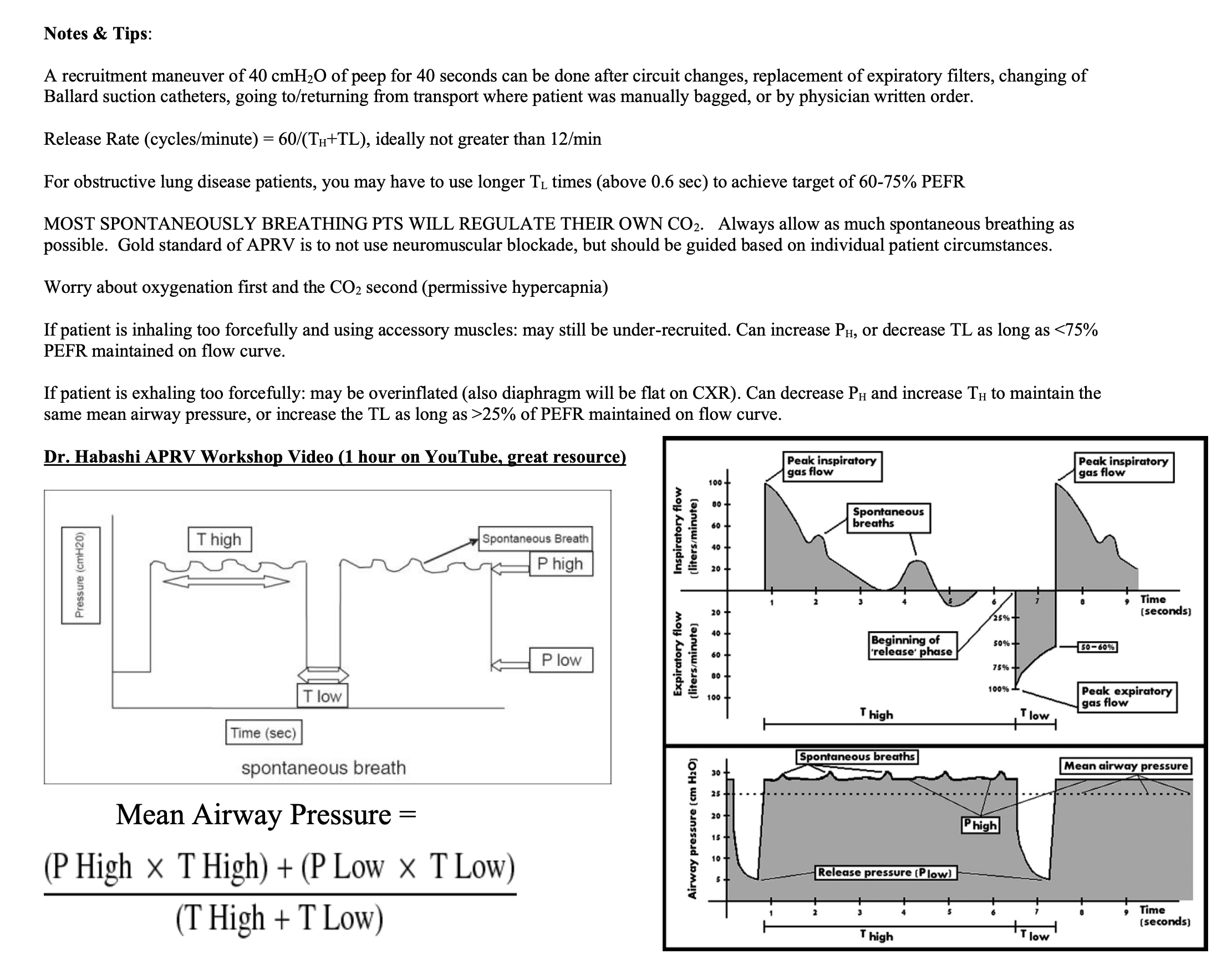
Updated 8/20/24
Authors: Buesing, Bauman, Berning
Gastrointestinal
Direct Peritoneal Resuscitation
Background, including pathophysiology
The advent of damage control surgery (DCS) has led to a staged approach to the patient in extremis with intra-abdominal hemorrhage and shock that has undoubtedly saved lives. However, massive resuscitation associated with severe hemorrhagic shock involves fluid administration in volumes far in excess of estimated blood loss because of the shift of fluid from the intravascular to the extravascular space. This massive volume load usually results in substantial tissue edema, which can delay abdominal closure.9,10 Acute tissue edema with swelling of the interstitial space secondary to resuscitation is a dominant factor in the inability to close many DCS patients.
Direct peritoneal resuscitation (DPR) is a validated resuscitation strategy in patients with open abdominal wounds. The practice consists of suffusing the peritoneal cavity with a 2.5% glucose-based peritoneal dialysis solution along with traditional intravenous resuscitation. The process leads to microvascular vasodilation and increases visceral and hepatic blood flow1; reverses endothelial cell dysfunction2; improves survival and down regulates the inflammatory response3; reverses established microvascular constriction4; normalizes capillary perfusion density5; and normalizes systemic water compartments6; preserves hepatic blood flow improving survival and preventing hepatic inflammation following hemorrhagic shock7; improves obesity-induced hepatic dysfunction after trauma8; accelerates primary abdominal wall closure after damage control surgery and prevents complications associated with open abdomen9, 10. In addition to observed effects on microcirculation, it has marked ability to decrease visceral edema and normalize body water ratios. In the pediatric population, it has been shown to augment ideal blood flow in necrotizing enterocolitis11. The technique improves inflammation, liver blood flow, and pulmonary edema in brain death12. The technique has been demonstrated safe and effective in humans with no untoward physiologic events or complications9, 10.
Goals of therapy
The goal of Direct Peritoneal Resuscitation is to decrease organ dysfunction, decrease intra-peritoneal inflammatory response, decrease or prevent complications associated with damage control surgery and planned open abdomens and help facilitate early abdominal closure.
The ultimate goal is that patients receiving direct peritoneal resuscitation will achieve significant reduction in time to abdominal closure, decreased number of re-exploration operations as well as higher rate of primary fascial closure.
Indications and Contraindications
Direct Peritoneal Resuscitation is indicated in the treatment of patients with planned open abdomen after damage control surgical procedures where the surgeon is unable to achieve primary fascial closure or in situations where is inadvisable to attempt primary abdominal closure due to planned re-operation, significant peritoneal contamination or inflammation, need to second look due to bowel viability, or other indications. Its use requires the fascia to remain open, with peritoneal contents and fluid controlled ideally with a commercial system such as the Abthera wound vac. However, other temporary abdominal closure strategies are also acceptable as long as they support a system for controlled abdominal fluid affluent.
Contraindications are closed abdominal wall or inability to adequately remove infused peritoneal fluid.
Technique- Equipment and set up with pictures
Operative phase
Surgeon performing procedure places drain prior to temporary abdominal closure. Ideally this will involve a standard 19fr round ‘Blake’ type drain placed around the root of the mesentery, though other alternative drains with leur-lock adaptors are acceptable. The Blake drain will have a Medtronic DLP 3mm vascular cannula attached, secured in place with surgical ties (tie several tight silks around the end of the Blake) as needed to ensure watertight connection.


Once in place – the vessel cannula will be capped with a standard IV tubing cap.
Of note- an alternative to the DLP vascular cannula is the following catheter adapter with the Christmas tree on one side and leur lok on the other. These may be more accessible in SICU if for some reason the vascular cannula was not added or available. There were previous reports of leakage but has since been tested and none leak as long as you secure them in there as tight as humanly possible.

ICU
Once the patient arrives in the ICU – the nurse will confirm the order for Direct Peritoenal Resuscitation. A 5000 ml bag Delflex 2.5% peritoneal dialysis solution, will be obtained from pharmacy along with an Alaris IV pump on a separate IV pole and standard Alaris IV tubing. The Alaris IV pump, IV tubing and DPR catheter should be clearly marked “FOR DPR USE, NOT FOR IV INFUSION”.
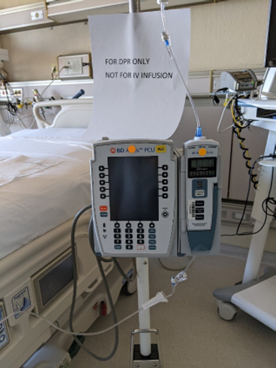
After ensuring proper function of the temporary abdominal closure device, the DPR IV pump and tubing is connected to the DPR catheter and the infusion initiated at the ordered rate. It should be labeled “DPR only, do not inject” as per the One Chart order.
The infusion is continued until the order is discontinued by the surgical service or the patient is returned to the operative room for abdominal re-exploration. It is acceptable to hook up the Abthera or temporary wound closure to wall suction (at a setting of less than 120 mmHg), but patients should have a KCI VAC unit at bedside as an alternative if needed for fluid removal. Canisters on the temporary abdominal closure device are changed as needed, anticipating that approximately 500cc of fluid will be evacuated from the peritoneal cavity per hour. If using wall suction, the Abthera tubing fits directly into suction tubing and can be secured with tape or tegederm.
Administration/management
ADMINISTRATION:
1. Follow standard steps for nursing procedures.
2. Obtain 5000ml bag of 2.5% Delflex peritoneal dialysis solution from pharmacy.
3. Prime standard Alaris pump IV tubing with solution. For safety, all Direct Peritoneal Dialysis should be infused using an independent Alaris pump separate from all other infusions. Tubing should be labeled to distinguish it from IV infusions and should be reviewed during bedside shift report.
4. To set up, the red frangible pin on the 5L bag should be broken. The bag is connected to IV tubing as usual. The patient should have an abdominal drain in place for infusion. The tubing is connected to the DPR drain using Medtronic 3mm Vascular catheter or other catheter with a leur lock connection. If the connector is not present, the operating physician should be contacted as this is a unique connection device. Insert the “christmas tree” end of the connector into the Blake drainand connect the pump tubing using the leur lock end.
5. Program pump according to administration instructions in ACP orders. RN should expect orders for 500ml bolus, then continue infusion at a rate of 1.5ml/kg/hr until AbThera would vac is removed or orders are discontinued. A new bag of Delflex solution should be used every 24 hours while resuscitation is ongoing.
6. The dialysate must be on a separate pole and pump.
7. Label the Blake drain most distal from the site indicating the type of drain.
8. Label the fluid tubing most distal from the bag with type of fluid.
9. The solution will automatically circulate in the peritoneal cavity and be evacuated through the negative pressure AbThera wound vacuum, either to the VAC canister or wall suction <120 mmHg.
10. DPR solution infused should be recorded as “input” by the Registered Nurse in the patient’s EHR in the row for the Abdominal Drain DPR and wound vac output should be included as “output” in the medical record under the row included with the LDA for the incision.
11. Change wound vac containers as needed. STOP the DPR infusion anytime the wound vac is not running/functioning for more than a short period of time.
12. NEVER clamp the wound vac tubing while the infusions are running. If you need to trouble shoot the wound vac, STOP the DPR infusion pump until wound vac is functioning. Contact the surgical team for assistance as needed.
Ordering/order sets
See flier for order set details. Please note the rates of infusion for the initial bolus and maintenance rates should not be adjusted.
Ins and outs will be recorded as shown in the flier also.
Complications and concerns
Inadequate removal of peritoneal fluid leading to potential increased intra-abdominal pressure, intra-abdominal hypertension and potential abdominal compartment syndrome.
Leakage of dialysate from instillation or evacuation process due to improper/inadequate set-up.
If either of the above is a concern, stop the infusion, call the provider. Do not stop the suction on the VAC or wall.
Abby Josef, MD
References
1. Hurt RT, Zakaria el R, Matheson PJ, Cobb ME, Parker JR, Garrison RN. Hemorrhage-induced hepatic injury and hypoperfusion can be prevented by direct peritoneal resuscitation. J Gastrointest Surg. 2009;13(4):587-94.
2. Zakaria el R, Li N, Garrison RN. Mechanisms of direct peritoneal resuscitation-mediated splanchnic hyperperfusion following hemorrhagic shock. Shock. 2007;27(4):436-42.
3. Garrison RN, Conn AA, Harris PD, Zakaria el R. Direct peritoneal resuscitation as adjunct to conventional resuscitation from hemorrhagic shock: a better outcome. Surgery. 2004;136(4):900-8.
4. Zakaria el R, Garrison RN, Kawabe T, Harris PD. Direct peritoneal resuscitation from hemorrhagic shock: effect of time delay in therapy initiation. J Trauma. 2005;58(3):499-506; discussion -8.
5. Zakaria el R, Li N, Matheson PJ, Garrison RN. Cellular edema regulates tissue capillary perfusion after hemorrhage resuscitation. Surgery. 2007;142(4):487-96; discussion 96 e1-2.
6. Zakaria el R, Matheson PJ, Flessner MF, Garrison RN. Hemorrhagic shock and resuscitation mediated tissue water distribution is normalized by adjunctive peritoneal resuscitation. J Am Coll Surg. 2008;206(5):970-80; discussion 80-3.
7. Hurt RT, Matheson PJ, Smith JW, Zakaria el R, Shaheen SP, McClain CJ, Garrison RN. Preservation of hepatic blood flow by direct peritoneal resuscitation improves survival and prevents hepatic inflammation following hemorrhagic shock. Am J Physiol Gastrointest Liver Physiol. 2012;303(10):G1144-52.
8. Matheson PJ, Franklin GA, Hurt RT, Downard CD, Smith JW, Garrison RN. Direct peritoneal resuscitation improves obesity-induced hepatic dysfunction after trauma. J Am Coll Surg. 2012;214(4):517-28; discussion 28-30.
9. Smith JW, Garrison RN, Matheson PJ, Franklin GA, Harbrecht BG, Richardson JD. Direct peritoneal resuscitation accelerates primary abdominal wall closure after damage control surgery. J Am Coll Surg. 2010;210(5):658-64, 64-7.
10. Smith JW, Neal Garrison R, Matheson PJ, Harbrecht BG, Benns MV, Franklin GA, Miller KR, Bozeman MC, David Richardson J. Adjunctive treatment of abdominal catastrophes and sepsis with direct peritoneal resuscitation: indications for use in acute care surgery. J Trauma Acute Care Surg. 2014;77(3):393-8; discussion 8-9.
11. Maki AC, Matheson PJ, Shepherd JA, Garrison RN, Downard CD. Intestinal microcirculatory flow alterations in necrotizing enterocolitis are improved by direct peritoneal resuscitation. Am Surg. 2012;78(7):803-7.
12. Smith JW, Ghazi CA, Cain BC, Hurt RT, Garrison RN, Matheson PJ. Direct peritoneal resuscitation improves inflammation, liver blood flow, and pulmonary edema in a rat model of acute brain death. J Am Coll Surg. 2014;219(1):79-87.
13. Walker SK, Matheson PJ, Schreiner MT, Smith JW, Garrison RN, Downard CD. Intraperitoneal 1.5% Delflex improves intestinal blood flow in necrotizing enterocolitis. J Surg Res. 2013;184(1):358-64.
14. Downard CD, Matheson PJ, Shepherd JA, Maki AC, Garrison RN. Direct peritoneal resuscitation augments ileal blood flow in necrotizing enterocolitis via a novel mechanism. J Pediatr Surg. 2012;47(6):1128-34.
15. Matheson PJ, Mays CJ, Hurt RT, Zakaria ER, Richardson JD, Garrison RN. Modulation of mesenteric lymph flow and composition by direct peritoneal resuscitation from hemorrhagic shock. Arch Surg. 2009;144(7):625-34.
16. Matheson PJ, Hurt RT, Franklin GA, McClain CJ, Garrison RN. Obesity-induced hepatic hypoperfusion primes for hepatic dysfunction after resuscitated hemorrhagic shock. Surgery. 2009;146(4):739-47; discussion 47-8.
17. Zakaria el R, Tsakadze NL, Garrison RN. Hypertonic saline resuscitation improves intestinal microcirculation in a rat model of hemorrhagic shock. Surgery. 2006;140(4):579-87; discussion 87-8.
18. Cryer HM, Gosche J, Harbrecht J, Anigian G, Garrison N. The effect of hypertonic saline resuscitation on responses to severe hemorrhagic shock by the skeletal muscle, intestinal, and renal microcirculation systems: seeing is believing. Am J Surg. 2005;190(2):305-13.
19. Zakaria el R, Garrison RN, Spain DA, Harris PD. Impairment of endothelium-dependent dilation response after resuscitation from hemorrhagic shock involved postreceptor mechanisms. Shock. 2004;21(2):175-81.
20. Zakaria el R, Hurt RT, Matheson PJ, Garrison RN. A novel method of peritoneal resuscitation improves organ perfusion after hemorrhagic shock. Am J Surg. 2003;186(5):443-8.
21. Zakaria el R, Garrison RN, Spain DA, Matheson PJ, Harris PD, Richardson JD. Intraperitoneal resuscitation improves intestinal blood flow following hemorrhagic shock. Ann Surg. 2003;237(5):704-11; discussion 11-3.
22. Weaver JL, Smith, JW. (2016). Direct Peritoneal Resuscitation: A review. International Journal of Surgery 2016; 33:237-241.
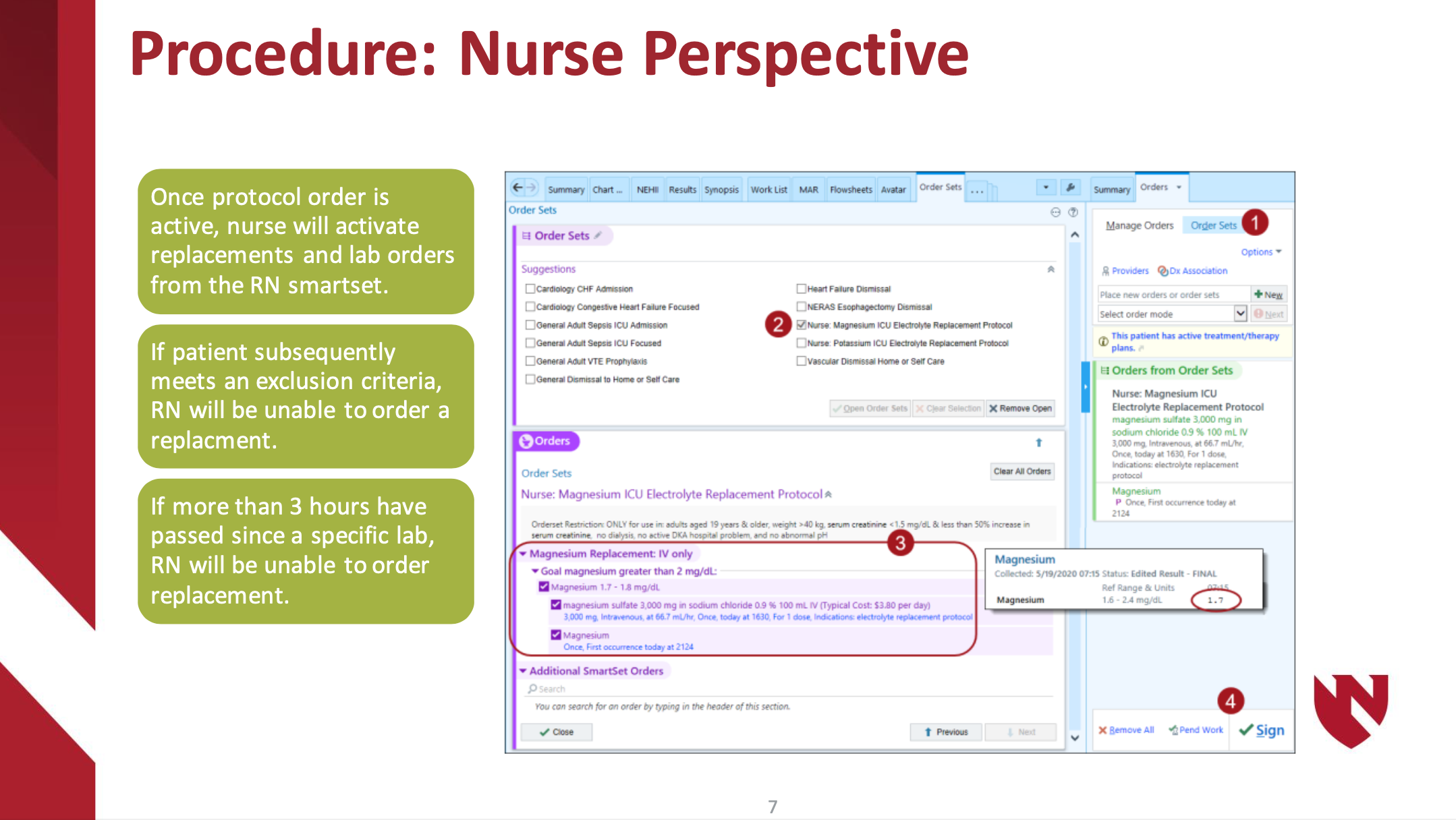
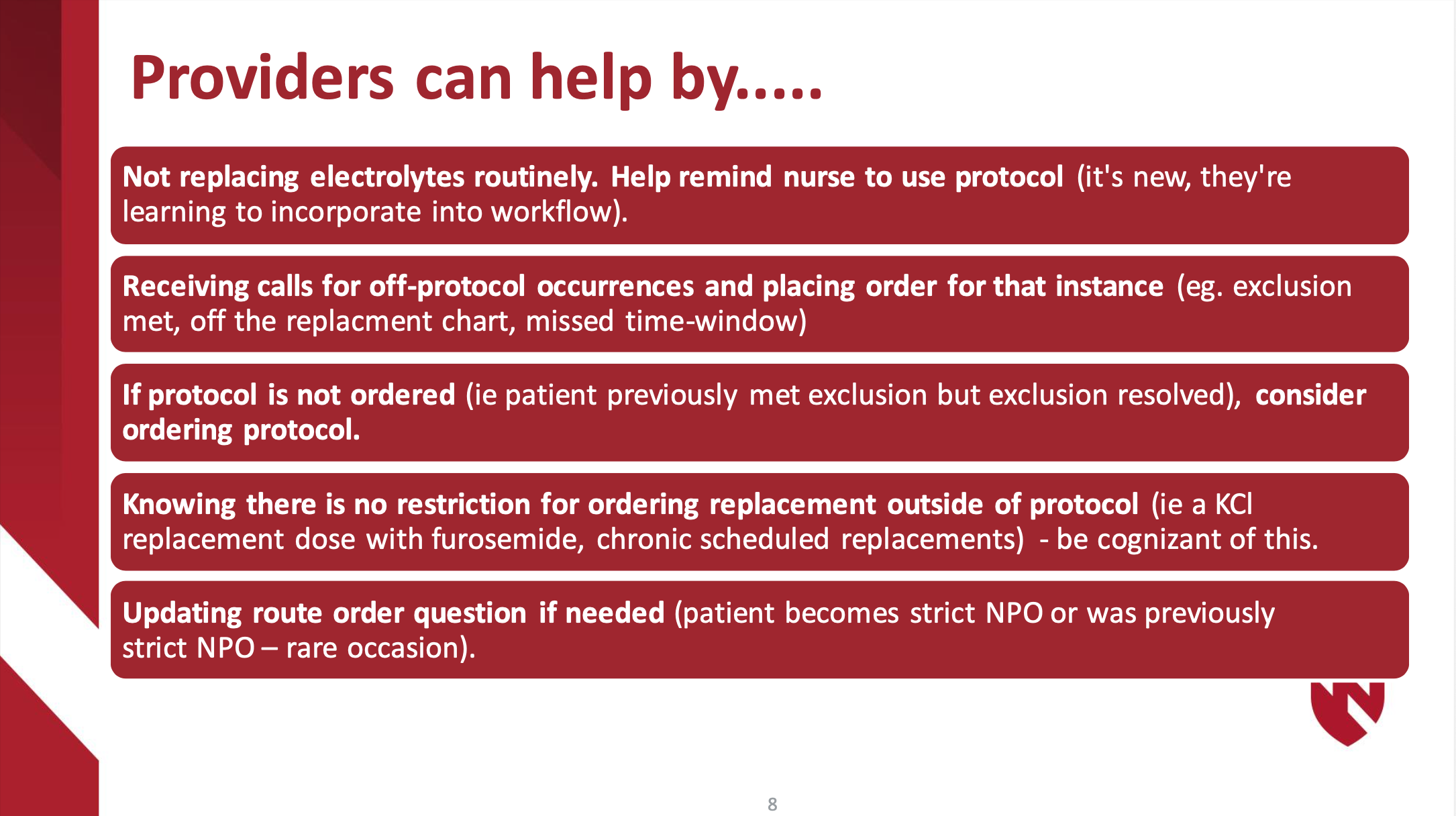
Fluids/Electrolytes/Nutrition
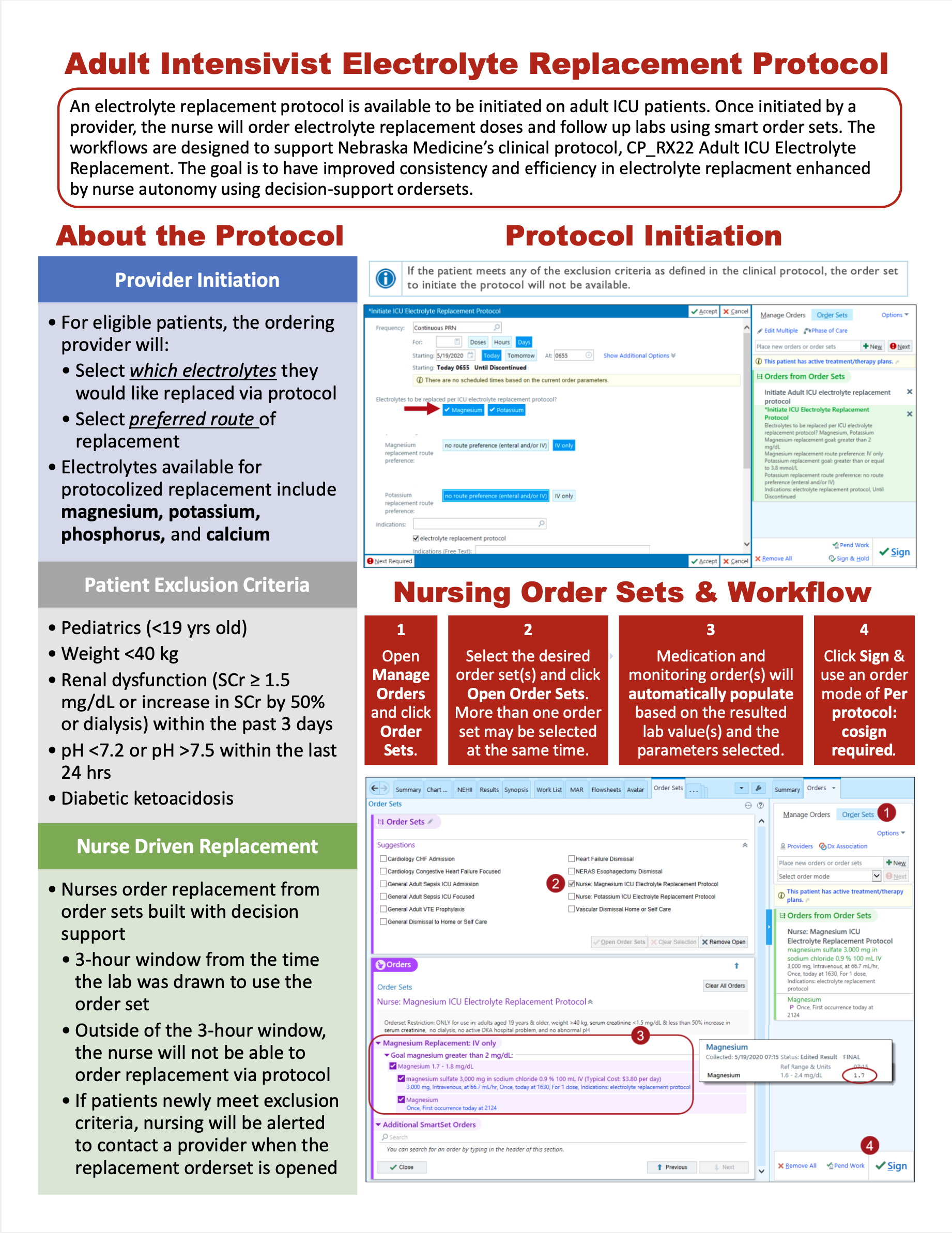
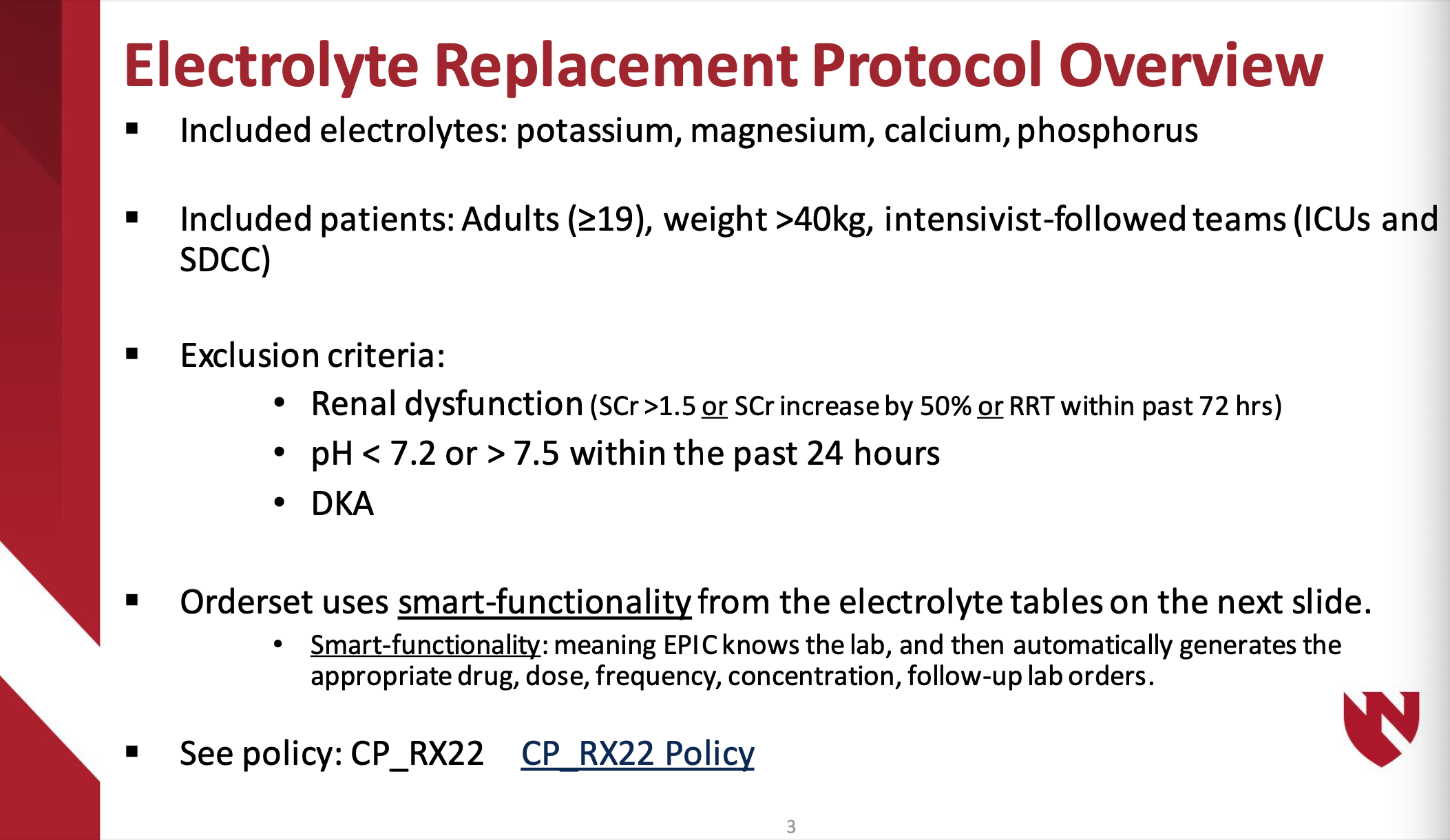
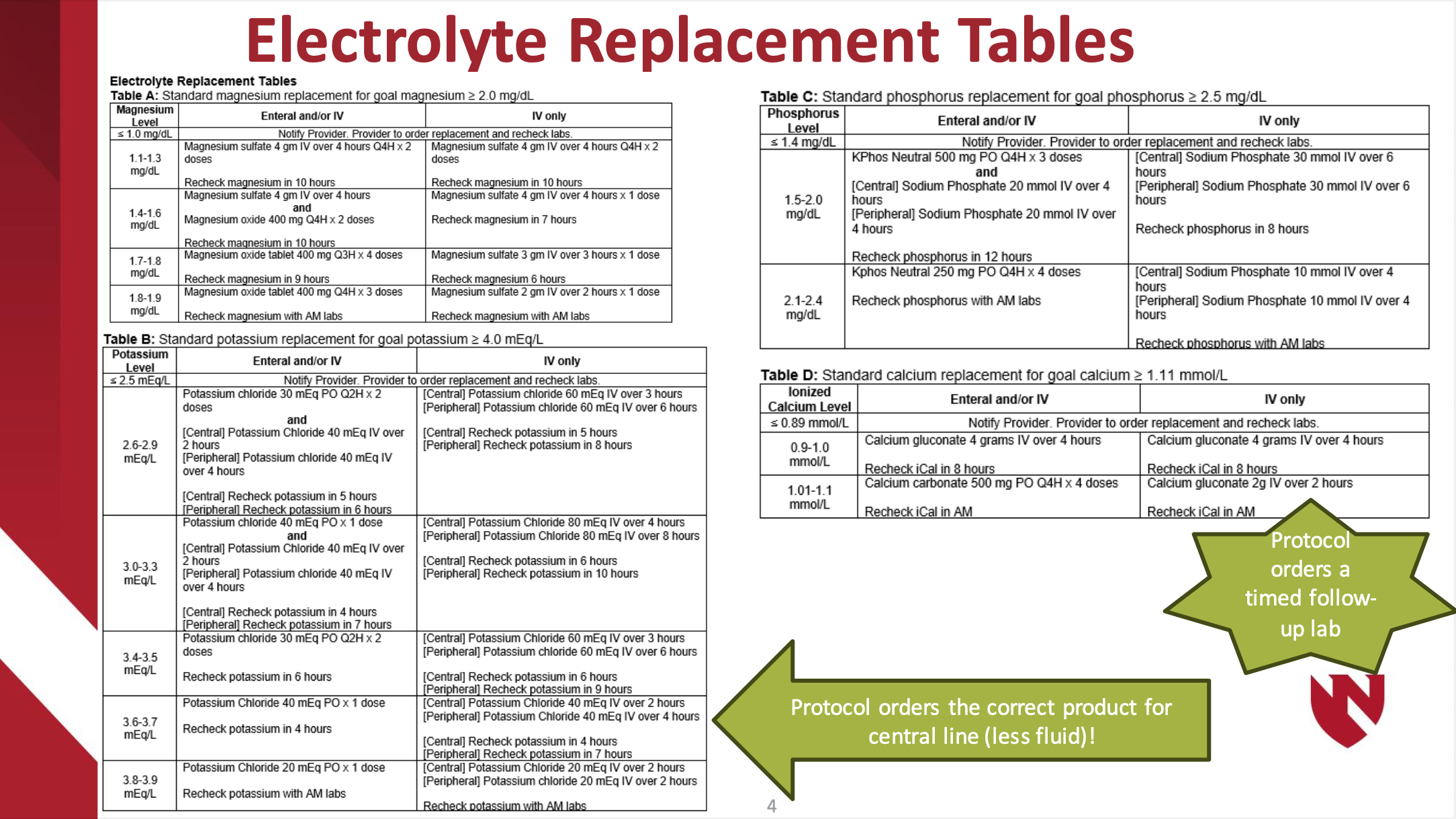
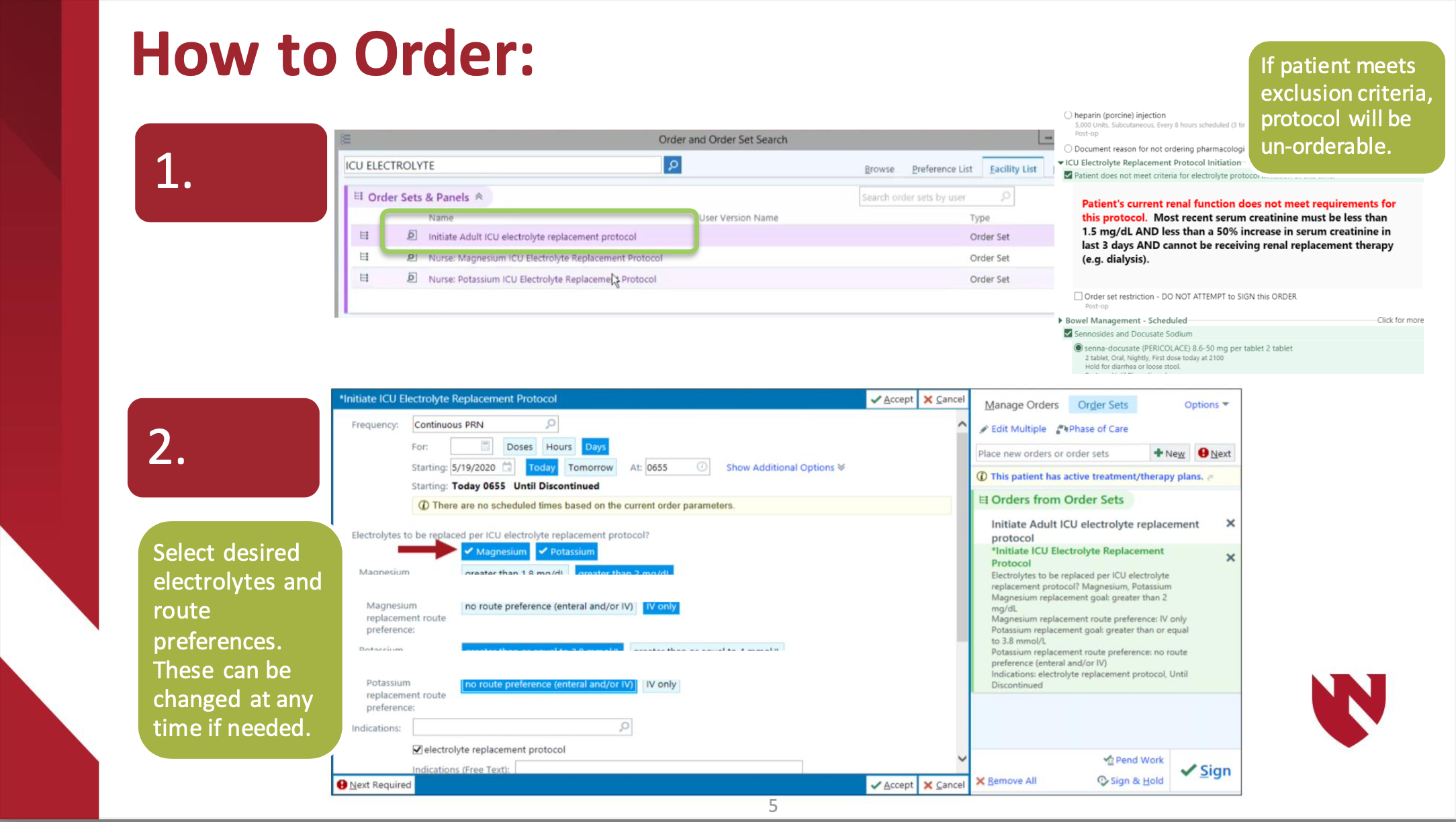
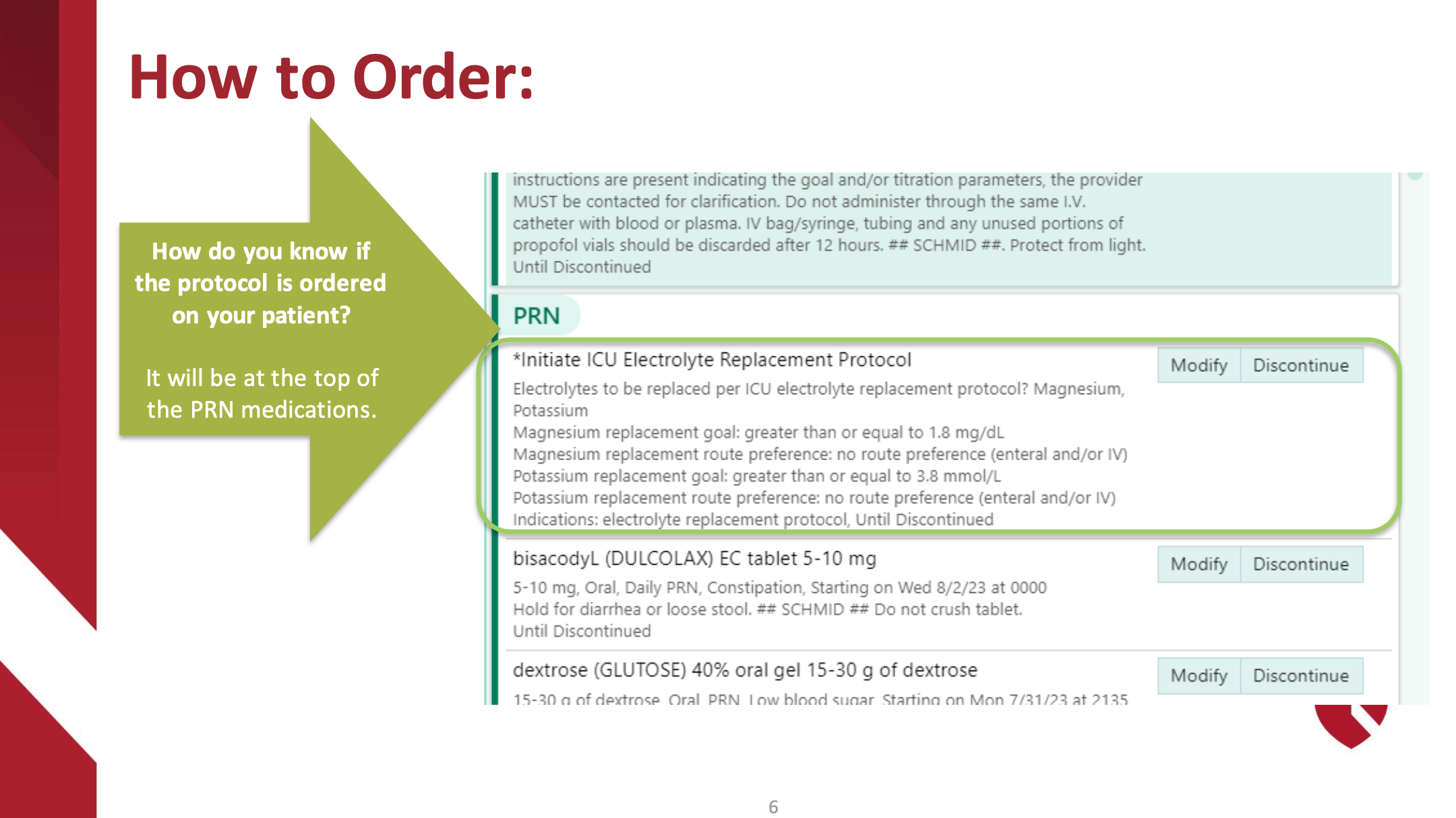
Electrolyte Replacement Protocol
Hematologic
Massive Transfusion in the ICU
Bedside ICU Procedures
Percutaneous Tracheostomy Protocol
Purpose
To provide guidance on safe practices to perform percutaneous tracheostomy in the operating room and ICU settings.
Preprocedural Planning
- Indications for tracheostomy at the discretion of the attending surgical intensivist.
- The procedure should be scheduled through the operating room by calling OR Charge Nurse.
- Two Attending Physicians must present at bedside to safely perform the procedure. One provider with perform the tracheostomy and one will be managing sedation. A procedure note and a sedation note need to be completed upon completion of the tracheostomy.
- Bronchoscopic guidance is required
- Medications for the procedure consist of an anxiolytic, a narcotic pain medication, and a neuromuscular paralytic. Additionally, local anesthetic may be requested.
- An intubation/airway cart with associated equipment is required at the bedside should reintubation or emergent airway be needed.
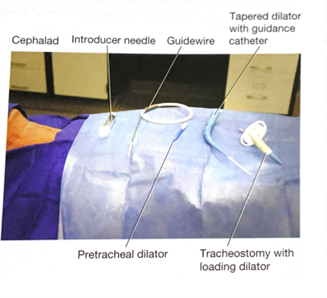
Equipment
- Blue Rhino Percutaneous Tracheostomy Kit
- Cuffed Tracheostomy (Size 6 and/or Size 8)
- Sterile Drapes and Chlorohexidine Prep
- Sterile Gowns and Gloves
- Eye protection and Head Coverings
- Bronchoscope
- Sterile water and Lubrication
- Airway cart (associated supplies needed for reintubation if needed)


Team
- Attending Intensivist to perform the tracheostomy
- Attending Intensivist to manage sedation
- Trainees (ICU Fellows, Surgical Residents, Medical Students)
- Critical care Nurse
- Respiratory Therapist
- OR Nursing Staff
Room Set-up and Patient Positioning
- The patient should be positioned supine with the neck slightly hyperextended with a shoulder roll if possible. If there is concern for or confirmed cervical spine injury, inline stabilization with the neck in a neutral position must be maintained with securely placed tape.

- The patient’s arms should be placed at patient’s side to ensure access to the neck bilaterally. The bed needs to be positioned to allow for access to the head of the bed so that orotracheal reintubation can be performed if needed.
- For right-handed surgeons, the bronchoscopy cart is generally placed on the patient’s left with the person performing the tracheostomy on the patient’s right. The respiratory therapist should be at the head of the bed with easy access to the patient’s airway. A second provider will be at the head of the bed performing the bronchoscopy. The patient’s nurse needs to have easy access to the patients IV in order to administer medications in a timely manner and the monitor with vital signs and pulse oximetry with audio easily visible to all.

- Set the ventilator to deliver a set volume and rate with 100% FiO2 to preoxygenate the patient. The ICU monitor should set so the pulse oximeter is audible. Continuous hemodynamic monitoring should be achieved with ekg and arterial line or frequent BP cuff monitoring (every 3 minutes).
Technical Steps
- Prior to the start of the procedure, a through “timeout” should be performed. All members of the team should be present and attentive.
- Adequate sedation should be achieved with anxiolytic and narcotic pain medications. This is followed by paralysis.
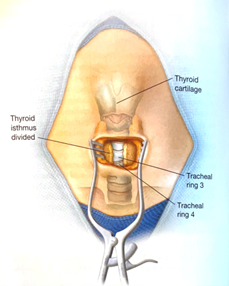
- Palpate the neck to identify relevant anatomy. Ideal location for placement of the tracheostomy is between the 2nd and 3rd tracheal ring.

- Don all appropriate PPE. Standard sterile surgical technique should be implemented.
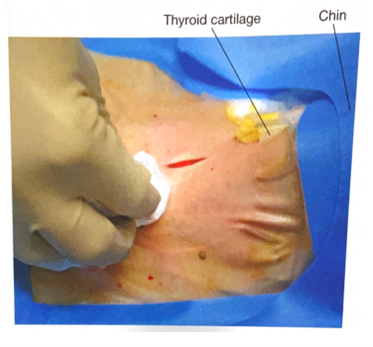
- Surgically prepare neck and upper chest with chlorohexidine skin prep. Standard sterile technique and draping should be performed. Consideration for easy access to the endotracheal tube to allow for easy airway exchange after trach is placed.
- Anesthetize the skin and subcutaneous tissue with local anesthetic.

- Using a #15 scalpel, make a 2-3 cm vertical, midline incision approximately 40 mm cephalad (1-2 finger breaths) to the sternal notch and just below the cricoid cartilage. If an anterior jugular vein is encountered in the incision (even if no injury is suspected), consider ligation proximally and distally as this is easiest to perform before the tracheostomy tube has been placed.

- Using a hemostat, bluntly dissect the subcutaneous tissue and muscle in midline to the pretracheal tissue along the length of the incision to better palpate the trachea to determine the point of entry.
- With the bronchoscope adaptor in place, advance the bronchoscope into the airway. Inspect the trachea and bronchial trees and clear any secretions.
- With the assistance of the respiratory therapist, while keeping the bronchoscope at the end of the endotracheal tube, retract both the endotracheal tube and bronchoscope simultaneously until the subglottic structures are visualized and one can see the anterior wall of trachea being palpated by the surgeon. The bronchoscope should be always kept within the endotracheal tube during this portion of the procedure in order to maintain control of the airway and ensure that the bronchoscope is not damaged.
- ***Although usually unnecessary, cautery may be used prior to entering the trachea with the introducer needle. After entry into the trachea, cautery should not be used do to the risk of fire with open oxygen source.***
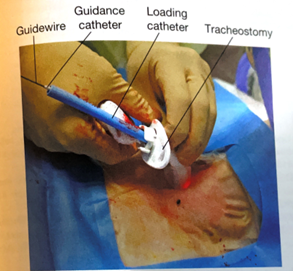
- An introducer needle is used the enter the anterior portion of the trachea between the 2nd and 3rd tracheal ring (approximately 1 finger breadth below the cricoid cartilage). With the bevel of the needle facing downward, the guidewire is passed into the trachea. Visualization of the guide wire going in the direction of the carina is required. Advance the guidewire slightly passed the carina into the right or left mainstem bronchus.



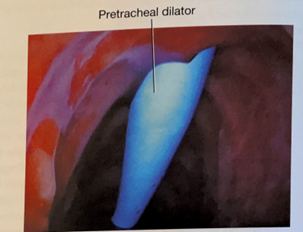
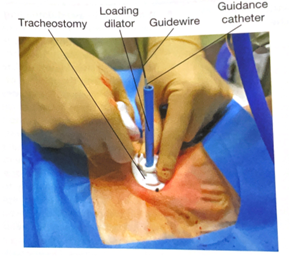
- Using the Seldinger technique, with constant Bronchoscopic visualization and control of the wire within the trachea, the trachea is sequentially dilated. The dilator handle is hydrophobic which makes it less likely to slip in a wet environment while the actual dilating portion is hydrophilic which only requires water/liquid to be lubricated. First the small tracheal dilator is advanced over the wire to dilate the pretracheal tract. Next the single-stage tapered dilator and the guiding catheter are advanced as a unit over the wire to dilate the trachea. Markings on the side of the progressive dilators guide the depth to which they are inserted. All catheters (pretracheal dilator, tapered dilator, and guiding catheter) should enter perpendicular to the trachea as to prevent pretracheal dissection or false passage. If the patient has limited ventilatory reserve prior to the procedure, the bronchoscope can be removed prior to the dilation portion of the procedure.




- The tapered dilator is removed from the guiding catheter and the guidewire, leaving the guiding catheter and the guidewire in place. If there is a longer distance between the tracheal surface and the skin surface, a finger can be used to dilatate the tract to help facilitate placement of the tracheostomy during the next step.
- Next, an appropriately sized and well lubricated tracheostomy tube with introducer is advanced over the wire and guiding catheter into the trachea. The wire, guiding catheter and loading trocar is then removed, keeping the tracheostomy in place.


- Inflate the tracheostomy cuff, insert the inner canula and connect tracheostomy to ventilator circuit. The presence of end-tidal carbon dioxide after ventilation resumes confirms placement in the airway.
- A bronchoscopy should be performed through the newly placed tracheostomy to visually confirm that it is within the trachea in proper position. Only remove ET tube after placement of tracheostomy tube within the trachea is confirmed.
- The tracheostomy is secured with a tracheostomy collar or ties to help prevent accidental dislodgement and provide time for adequate to tract formation.
- Obtain a chest x-ray to confirm appropriate positioning of the tracheostomy tube, rule out pneumothorax, and evaluate for bronchial obstruction.







Tracheostomy Care
- Following tracheostomy placement, standardized tracheostomy care bundles should be implemented. These protocols include steps to ensure the tracheostomy is secure, suctioning techniques, daily stoma hygiene and knowledge of emergency protocols should the newly placed airway be compromised. Special attention should be given to prevent pressure ulceration, particularly along the inferior aspect of the tracheostomy faceplate, especially if the flange is sutured to the skin.
- The tracheostomy tube should be exchanged no sooner than post-operative day 7.
- Once the patient is liberated from the ventilator and secretions are reasonably managed the process of tracheostomy tube downsizing can occur. The downsizing if the tracheostomy tube allows for improved patient comfort and the ability to participate in speech therapy.
- After the tracheostomy is no longer necessary, the patient can be decannulated. The stoma is covered with sterile occlusive dressing generally closes within two to four days.
Key Contributors
Bennett Berning, MD
Last Updated
March, 2023
References
- Cheung NH, Napolitano LM. Tracheostomy: epidemiology, indications, timing, technique, and outcomes. Respir Care. 2014 Jun;59(6):895-915; discussion 916-9.
- Young D, Harrison DA, Cuthbertson BH, Rowan K, TracMan Col- laborators. Effect of early vs late tracheostomy placement on survival in patients receiving mechanical ventilation: the TracMan randomized trial. JAMA 2013;309(20):2121-2129.
- Holevar M, Dunham JC, Brautigan R, Clancy TV, Como JJ, Ebert JB, Griffen MM, Hoff WS, Kurek SJ Jr, Talbert SM, Tisherman SA. Practice management guidelines for timing of tracheostomy: the EAST Practice Management Guidelines Work Group. J Trauma. 2009 Oct;67(4):870-4.
- Delaney A, Bagshaw SM, Nalos M. Percutaneous dilatational tracheostomy versus surgical tracheostomy in critically ill patients: a systematic review and meta-analysis. Crit Care 2006;10(2):R55.
- Hashimoto DA, Axtell AL, Auchincloss HG. Percutaneous Tracheostomy. N Engl J Med. 2020 Nov 12;383(20):e112.
- Hawn, M. T., Berning, B. J., & de Moya, M. A. (2023). Tracheostomy: Open and Percutaneous. In Operative techniques in surgery (2nd Edition, Vol. Volume Two, pp. 2506–2512). Wolters Kluwer.
Service Specific Protocols
ENT Flap Managment
Order set to be used by CCS team when assisting in the management of a flap preformed by the ENT service.
- Q1h Doppler and flap checks by nursing
- Q4h flap checks by ENT
- Decadron 8mg q8h x24h
- Daily labs
- Daily ASA x30days
- Judicious volume use to prevent congesting flap. Prefer vasopressors and MAP >65.
- Plus or minus IV abx x5days.