1. Trauma Service Overview
Orientation materials and additional information regarding work flow and requirements of the trauma service to help improve your experience and set expectations.
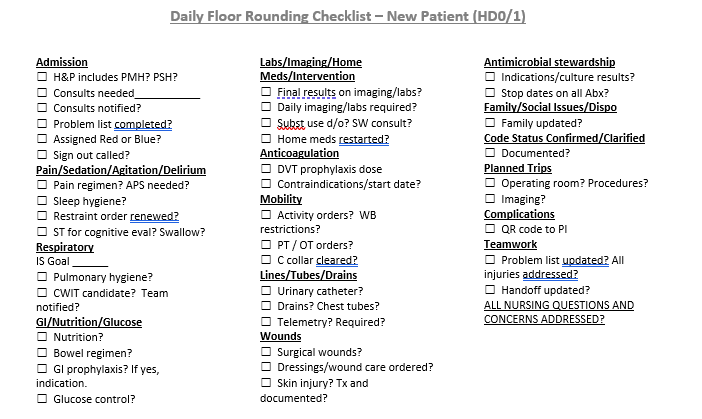
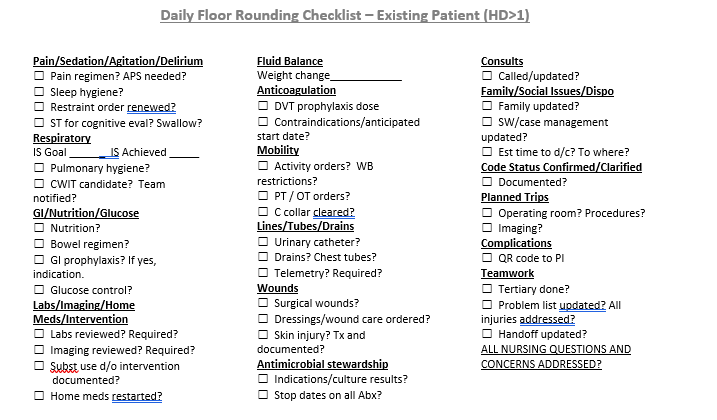
- Daily Floor Rounding Checklist for Trauma Patients
- Important Phone Numbers and Contact Information
- Isolated Orthopedic Transfers to Bellevue Medical Center Requiring Joint Replacement
- Reimplantation Triage and Transfer Pathway
- Trauma Patient Admission Criteria
- Trauma Team Activation (TTA) Criteria
- Trauma Tertiary Survey
- Trauma Quality Indicators
Daily Floor Rounding Checklist for Trauma Patients
Important Phone Numbers and Contact Information
Acute Care Surgery Attendings:
| Attending | Pager | Cell | Office |
| Zachary Bauman, DO | 402-888-1131 | 712-251-0895 | 402-559-4714 |
| Joseph Baus, MD | 402-888-1800 | 614-975-5466 | N/A |
| Christopher Barrett, MD | 402-888-6080 | 651-497-7846 | 402-559-3335 |
| Bennett Berning, MD | 402-888-5527 | 312-208-7465 | 402-559-4706 |
| Keely Buesing, MD | 402-888-0563 | 402-312-0984 | 402-559-8908 |
| Emily Cantrell, MD | 402-888-1201 | 336-775-8889 | 402-836-9142 |
| Mark Carlson, MD | 402-888-5161 | 402-650-4219 | 402-559-4581 |
| Samuel Cemaj, MD | 402-888-1203 | 402-305-5809 | 402-559-7166 |
| Charity Evans, MD | 402-888-0525 | 312-231-0897 | 402-559-2101 |
| Matthew Goede, MD | 402-888-3770 | 402-881-7345 | 402-559-8736 |
| Mark Hamill, MD | 402-888-5484 | 843-324-8252 | 402-559-3048 |
| Joshua Jaramillo, MD | 402-888-6059 | 720-363-1449 | N/A |
| Abigail Josef, MD | 402-888-5525 | 402-715-0029 | 402-559-4567 |
| Andrew Kamien, MD | 402-888-1453 | 716-228-0118 | 402-559-7399 |
| Kevin Kemp, MD | 402-888-2545 | 510-378-2215 | 402-559-8147 |
| Mike Matos, DO | 402-888-5655 | 304-482-2712 | 402-559-7051 |
| David Mercer, MD | 402-888-3758 | 402-889-3431 | 402-559-8272 |
| Olabisi Sheppard, MD | 402-888-5034 | 913-271-7241 | 402-559-2113 |
| John Tierney, MD | 402-888-6079 | 480-703-4556 | 402-559-1866 |
| William Terizian(Hillman), MD | 402-888-5526 | 703-505-1058 | 402-559-5970 |
| Jessica Veatch, MD | 402-888-6154 | 303-726-0736 | 402-559-8979 |
| Brett Waibel, MD | 402-888-0698 | 252-414-8586 | 402-559-6809 |
Acute Care Surgery APPs
| APPs 402-559-7901 / 402-559-9589 / 402-559-8142 | ||
| Tim Baack, NP | 402-888-5843 | 402-640-4084 |
| Jessica Bachmann, NP | 402-888-6252 | 402-660-4017 |
| Maggie Baumann, NP | 402-888-3839 | 402-813-4519 |
| Christina Boje, NP | 402-888-1871 | 402-578-7219 |
| Samantha Cunningham, NP | 402-888-5101 | 402-250-8711 |
| Sam Dellinger, PA | 402-888-6190 | 402-332-8474 |
| Esthefany Estrada, | 402-888-5155 | 308-325-8504 |
| Kelly Fenn, PA | 402-888-1440 | 563-299-5585 |
| Abby Hager, NP | 402-888-5582 | 402-680-9465 |
| Patrick Heavey, PA | 402-888-5675 | 402-699-9119 |
| Kristin Johnson, NP | 402-888-4584 | 308-530-5183 |
| Sophia Ketchmark, PA | 402-888-6189 | 402-926-6229 |
| Shannon Landry, PA | TBD | TBD |
| Ashley Lewis, NP | 402-888-4072 | 402-452-7660 |
| Sonia Malik, PA | 402-888-6008 | 703-994-2553 |
| Evan Meysenburg, NP | 402-888-6083 | 402-741-0970 |
| Erin Panowicz, NP | 402-888-5089 | 402-416-1274 |
| Whitney Petersen, NP | 402-888-0097 | 402-984-3744 |
| Meredith Reittinger, NP | 402-888-5865 | 336-549-2644 |
| Dom Samuel, NP | 402-888-1698 | 402-541-8998 |
| Amber Saltsgaver, NP | 402-888-5153 | 402-651-1250 |
| Megan Samland, NP | 402-888-5597 | 402-350-3564 |
| Emily Ulmer, PA | 402-888-6124 | 308-870-4515 |
| Theresa Vergara, NP | 402-888-2443 | 646-498-3829 |
| Makaela Waddell, NP | 402-888-0303 | 402-536-9460 |
| Becca Witt, PA | 402-888-5846 | 402-250-2134 |
| Cassey Younghans, NP | 402-888-6084 | 308-870-0791 |
Acute Care Surgery Administrators
| Administrative | |
| Jeannie Thomas | 402-559-9696 |
| Jessica Bruno | 402-559-8884 |
| Savannah Reyes | 402-559-5248 |
| Sue Cramer | 402-559-9225 |
| Karen Kroupa | 402-559-9960 |
| Copy Machine Code: | 10278 |
| Conf Room Code: | 51243 |
Acute Care Surgery Inpatient and Outpatient Team Contacts
| Inpatient Team Contacts | |||
| Molli Kies, Care Transition Nurse | 531-557-1135 | 402-559-6145 | 402-990-0874 |
| Angel Erwin, Care Transition Nurse | 531-557-0827 | 402-5522738 | 402-650-3038 |
| Ginny Rogers, Peds Care Transition Nurse | 531-5579166 | 402-552-2505 | 402-917-2593 |
| Barb Robertson, Nutritionist | 402-888-1848 | ||
| Dennis Brown, Care Transition nurse for EGS | 402-552-6588 | 402-981-9431 | 531-551-5031 |
| Social Worker | 402-888-1643 | 402-559-6145 | 531-557-3822 |
| Elizabeth Hawkins, Pharmacist | 531-557-7456 | 402-714-2787 | 402-552-3541 |
| Alli Gabriel, Pharmacist | 402-637-6454 | 402-552-3965 | 531-557-3983 |
| Ashley Farrens, Trauma Prog Manager | 402-612-7702 | 402-552-3997 | |
| Stacey Roode - PI Coordinator | 402-618-0375 | ||
| Liz McIntosh - PI Coordinator | 714-651-7733 | ||
| Kayla Petersen - PI Coordinator | 515-729-9289 | ||
| Lora Hofstetter - Peds PI Coordinator | 913-709-0923 | ||
| Brian Lake, 9N Manager | 402-552-3873 | ||
| Chad Himmelberg, SICU Manager | 402-552-7963 | ||
| Outpatient Team | |||
| Jenn Dickey, Case Manager | 402-888-3629 | 402-672-6081 | 402-559-6075 |
| Clinic Scheduling (# for pts) | 402-559-4075 | ||
| Clinic | 402-559-4737 | ||
| Clinic Workroom | 402-559-2028 | ||
| Trauma Clinic: Mon & Thurs @ 1-3pm | |||
| EGS Clinic: Wed @ 1-3pm | |||
| Elective EGS Clinic: Thurs @ 9am | |||
Service Pager and Consultant Contacts
| RED TRAUMA TEAM PAGER: | 402-888-1938 | GREEN SICU Pager: | 402-888-0282 | ||
| Blue APP TRAUMA TEAM PAGER: | 402-888-4774 | YELLOW CCS TEAM PAGER: | 402-888-3005 | ||
| EGS PAGER: | 402-888-0447 | General Surgery/Night Float Pager: | 402-888-0316 |
| Orthopedic Surgery Pager: | 402-888-0586 |
| Neurosurgery Pager: | 402-888-1866 |
| Pediatric Surgeons | Pager | Cell | Office |
| Angela Hanna, MD | N/A | 801-550-4482 | N/A |
| Abdalla Zarroug, MD | N/A | 507-271-5656 | N/A |
| ENCOMPASS TEAM | ||
| Ashley Raposo, Program Supervisor | 402-559-9154 | 402-980-1731 (cell) |
| Melissa Inzauro, Social Worker | N/A | 402-250-6336 (cell) |
| Allie Sothan, Social Worker | N/A | 531-375-8334 |
| Tia Manning, Mental Health Specialist | N/A | 402-250-9813 |
| Violence Intervention Specialists | ||
| Kam Wayne | N/A | 402-250-4324 (cell) |
| TiShara Wardlow | N/A | 402-830-7986 (cell) |
Departmental Contacts
| Department Contacts | |
| Handheld/Battery-Powered Bronch OR RT 402-559-1615 | 402-650-5748 |
| Anesthesia CD | 402-559-4078 / 402-552-3224 |
| OR | 402-889-0931 |
| OR Charge | 402-559-9900 / 402-552-3224 |
| Scheduling | 402-559-5257 |
| Preop | 402-559-9087 / 402-552-3288 (CCE) |
| PICU | 402-559-1420 |
| Anesthesia | 402-552-2090 |
| Micro | 402-559-5031 |
| Psychology | 402-559-1030 |
| Lab | 531-557-3980 |
| ICU Pharmacist | 531-557-7452 |
| SDCC Pharmacist | 402-559-7235 |
| Inpatient Pharmacy | 402-559-6502 |
| Trauma Bay | 402-559-4583 |
| ECHO | 402-559-6694 / 402-559-6637 |
| ER | 7-3600 |
| ED Charge Nurse | 402-559-1000 / 402-559-3216 |
| Radiology Dictation | 402-888-1898 |
| Radiology Resident | 402-559-8953/888-1314/888-1415(res) |
| IR | 402-559-8953 |
| Radiology Reading Rooms | |
| Body CT: | 402-559-1005 |
| Neuro: | 402-559-1008 |
| Bone: | 402-559-1006 |
| US: | 402-559-1023 |
| Nights: | 402-559-1233 |
Isolated Orthopedic Transfers to Bellevue Medical Center Requiring Joint Replacement
Purpose:
· To Identify which patients can appropriately be transferred to Bellevue Medical Center (BMC) who have sustained an isolated fractures requiring total or partial joint replacement
Background/definitions:
· Lack of OR availability at Nebraska Medicine main campus for partial or total joint replacement in trauma patients has put a strain on the system and delayed definitive surgical treatment for these patients.
Guideline Inclusion Criteria:
- Isolated traumatic fracture patients only needing partial or total joint replacement for their injury as opposed to ORIF of the hip fracture alone.
- Deemed appropriate for transfer to Bellevue Medical Center by the Trauma Service.
Guideline Exclusion Criteria:
- Poly-trauma patients with fractures requiring total or partial joint replacement.
- Deemed inappropriate for transfer to Bellevue Medical Center by the Trauma Team or Orthopedic Surgery Team.
Diagnostic Evaluation:
- Routine trauma lab work.
- Body region X-ray and/or CT scan
- Pan scan CT as indicated by mechanism or provider discretion
- Trauma Team consultation to make sure trauma work up is complete and no other injuries are present.
- Orthopedic Surgery consultation to make sure patient needs total or partial joint replacement (as opposed to non-operative management or routine ORIF of the fracture) and is appropriate for transfer to expidite surgical repair.
Practice Recommendations for Management:
- Patients transferred in from an outside institution will be directed to Nebraska Medicine ED (ER→ER). Trauma Team will do the initial trauma evaluation and work-up in the emergency department.
-
- If a fracture is identified along with other injuries, Orthopedic Surgery will be consulted as well as other consulting services as needed
-
- Patient will be admitted to Nebraska Medical Center (NMC) by the Trauma Service for further trauma management as deemed appropriate.
-
- If an isolated fracture is identified, Orthopedic Surgery will be consulted for their recommendations
- If a fracture is identified along with other injuries, Orthopedic Surgery will be consulted as well as other consulting services as needed
-
- If patient requires fixation via a partial or total joint replacement, is deemed appropriate for transfer to Bellevue Medical Center (BMC) by the Trauma Service, and has an accepting physician, the patient will then be transferred to BMC from the NMC ED for further isolated fracture management. BMC hospitalist is the accepting primary service for BMC transfer and ensures appropriate medical resources are in place for patient to be cared for at BMC. (Example- If patient has a hip fracture but is ESRD on dialysis, patient stays at NMC)
-
- Transfer to BMC will be arranged by the Orthopedic Surgery resident by contacting the PPU (aka BMC bed desk, 402-559-2337) and requesting transfer to the BMC hospitalist service.
- PPU informs Ortho resident of approximate inpatient BMC bed wait time.
- If there is an inpatient bed wait time at BMC, patient is sent to BMC Pre-Op as long as a same day BMC OR time can be assigned. If BMC OR time cannot be assigned the same day, patient is prioritized to BMC inpatient bed with all BMC ED admissions, the purpose of this prioritization is to transfer patient out of NMC ED expeditiously.
- No admission orders are placed to admit the patient to NMC. While the patient awaits transfer to BMC in the NMC ED, Trauma service continues to care for the patient.
-
- If Orthopedic Surgery resident determines patient would be more expeditiously cared for at main campus due to BMC bed wait
-
- Trauma service is contacted again and admits the patient.
- Trauma or Ortho provider contacts HM surgical co-mgmt service for pre-op evaluation and medical co-mgmt.
-
- If prolonged inpatient bed wait at both BMC and NMC campuses, On-Call Trauma attending and On-Call Orthopedic attending (& if needed BMC hospitalists for medical needs) determine whether it is best to transfer to BMC versus admit to NMC. PPU can help coordinate the conference call on the rare chance that all 3 physicians are needed to determine best location. Once location is determined, follow steps outlined above in A. to transfer to BMC or B. if admitting to NMC.
- The trauma tertiary survey will be completed by Orthopedic resident at BMC 24 hours after initial injury and documented as preferred by Trauma Service.
-
- If injuries discovered on tertiary appropriate consultations will be initiated by BMC Orthopedics team, including BMC service consults or remote NMC consultation.
-
- If the patient requires fracture fixation via routine ORIF, the patient will be admitted to the Trauma Service at Nebraska Medicine and follow the standard Nebraska Medicine Enhanced Recovery after Surgery (NERAS) pathway that has been established for isolated fracture patients.
-
- If the patient does not require fixation, the patient will be admitted to the Trauma Service at Nebraska Medicine and follow the standard NERAS pathway that has been established for isolated fracture patients.
-
- If patient primarily presents to Nebraska Medicine, patient will be activated based on criteria and both the Emergency Medicine and Trauma Team will respond appropriately and the trauma work-up will be conducted as per usual.
-
- If a fracture is identified along with other injuries, Orthopedic Surgery will be consulted as well as other consulting services as needed
-
- Patient will be admitted to Nebraska Medicine by the Trauma Service for further trauma management as deemed appropriate.
-
- If an isolated fracture is identified, Orthopedic Surgery will be consulted for their recommendations
-
- If patient requires fixation via a partial or total joint replacement, is deemed appropriate for transfer to BMC by the Trauma Service, and has an accepting physician, the patient will then be transferred to BMC from the ED for further isolated hip fracture management.
-
- Transfer to BMC will be arranged by the Orthopedic resident.
- The trauma tertiary survey will be completed by Orthopedic resident at BMC 24 hours after initial injury.
-
- If injuries discovered on tertiary appropriate consultations will be initiated by BMC admitting team, including BMC service consults or remote NMC consultation.
-
-
- If the patient requires fracture fixation via routine ORIF, the patient will be admitted to the Trauma Service at Nebraska Medicine and follow the standard NERAS pathway that has been established for isolated fracture patients.
- If the patient does not require fracture fixation, the patient will be admitted to the Trauma Service at Nebraska Medicine and follow the standard NERAS pathway that has been established for isolated fracture patients.
- If patient requires fixation via a partial or total joint replacement, is deemed appropriate for transfer to BMC by the Trauma Service, and has an accepting physician, the patient will then be transferred to BMC from the ED for further isolated hip fracture management.
-
- If a fracture is identified along with other injuries, Orthopedic Surgery will be consulted as well as other consulting services as needed
-
- If the patient does not meet activation criteria, Emergency Medicine will perform the initial evaluation.
-
- ***If a fracture is identified, Trauma should be consulted for additional trauma evaluation***
- If a fracture is identified along with other injuries, Orthopedic Surgery will be consulted as well as other consulting services as needed
-
- Patient will be admitted to Nebraska Medicine by the Trauma Service for further trauma management as deemed appropriate.
-
- If an isolated fracture is identified, Orthopedic Surgery will be consulted for their recommendations
-
- If patient requires fracture fixation via a partial or total joint replacement, is deemed appropriate for transfer to BMC by the Trauma Service, and has an accepting physician, the patient will then be transferred to BMC from the ED for further isolated fracture management.
-
- Transfer to BMC will be arranged by the Orthopedic resident.
- The trauma tertiary survey will be completed by Orthopedic resident at BMC 24 hours after initial injury.
-
- If injuries discovered on tertiary appropriate consultations will be initiated by BMC admitting team, including BMC service consults or remote NMC consultation.
-
-
- If the patient requires fracture fixation via routine ORIF, the patient will be admitted to the Trauma Service at Nebraska Medicine and follow the standard NERAS pathway that has been established for isolated fracture patients.
- If the patient does not require fracture fixation, the patient will be admitted to the Trauma Service at Nebraska Medicine and follow the standard NERAS pathway that has been established for isolated fracture patients.
- If patient requires fracture fixation via a partial or total joint replacement, is deemed appropriate for transfer to BMC by the Trauma Service, and has an accepting physician, the patient will then be transferred to BMC from the ED for further isolated fracture management.
-
-
Follow-up Care:
- If the patient is a poly-trauma patient, discharge and follow-up recommendations will be provided by all consulting services as needed and PT/OT.
-
- All attempts will be made to discharge patient to appropriate location based on patient/family preferences, PT/OT recommendations, and discretion of the Trauma Service
-
- If the patient is an isolated fracture patient admitted to Nebraska Medicine, discharge and follow-up recommendations will be provided by Orthopedic Surgery and PT/OT.
-
- All attempts will be made to discharge patient to appropriate location based on patient/family preferences, Orthopedic Surgery and PT/OT recommendations, and discretion of the Trauma Service.
-
- If the patient is an isolated fracture patient transferred to BMC, discharge and follow-up recommendations will be at the discretion of the teams managing the patient at BMC
Outcome Measures and Guideline Adherence:
- All patients transferred to BMC will be reviewed by the PI team at Nebraska Medicine.
-
- If the patient is admitted to a non-surgical service @ BMC, and if there is no identified opportunity for improvement, the following may be closed in primary review:
-
- ISS<9
-
- As part of secondary review, the Trauma Medical Director must review any that meet any of the following criteria:
-
- ISS>9
- Cases with an opportunity for improvement identified at primary review
-
- Patients that get transferred to BMC and for some reason transferred back to Nebraska Medicine, will undergo a tertiary review by the Trauma PI team and by all providers involved.
- Emerging trends will signal a need to review this pathway and modify as necessary
- If the patient is admitted to a non-surgical service @ BMC, and if there is no identified opportunity for improvement, the following may be closed in primary review:
-
Key Contributors:
· Zachary Bauman, DO, MHA
Last updated:
· 1/16/2023
References:
· American College of Surgeons 2022 Trauma Standards
Reimplantation Triage and Transfer Pathway
Reimplantation Triage and Transfer Pathway
Purpose: As an American College of Surgeons, verified level I trauma center, we are responsible for thorough assessment of the traumatically injured patient. This document is to aid in the triage and transfer process of patient requiring reimplantation services.
Background: Nebraska Medicine has multidisciplinary coverage (orthopedics, plastics, vascular, and urology) for patients requiring reimplantation services for traumatic injury (ie: severed limb, digit, or other body part).
Please reference the three identified injury types for appropriate treatment plan:
Mangled Extremity
Treatment of a mangled extremity is a collaborative effort amongst the Trauma service, Orthopedic surgery, and Vascular surgery. When a patient is determined to have a mangled extremity or extremity requiring re-implantation, all three services are involved to determine the overall best course of action for the patient given other injuries, hemodynamic status, and the ability to salvage the extremity. We utilize a mangled extremity score (see table below) to help with this management decision. Once all three service lines have agreed to re-implantation and/or attempting to salvage the extremity, the patient is taken to the OR where Orthopedic surgery and Vascular surgery will re-attach/re-construct bones and vessels as needed. Both services are available and on-call 24/7.

Upper Extremity/Hand Re-implantation
Nebraska Medicine has three experienced hand surgeons that are willing and skilled to perform hand/digit reimplantation when they are on call. Unfortunately, between the three of them, they cannot cover the hand service 24/7.
When these surgeons are unavailable, calls should be made to transfer to our regional implantation centers. See list of resources with contact information.
Our usual workflow for this is when we get a call from an outside hospital wanting to transfer a patient to us who potentially needs a hand/digit re-implantation, we will do a conference call with our on-call hand surgeon to see if this is something they are able to care for at our institution. If they are, we will have the patient transferred. While the patient is in route, our hand surgeon will get the OR organized and ready to go when the patient arrives. If the patient is unable to be cared for at our institution, we will help the outside hospital coordinate care to the regional hand re-implantation center by providing phones numbers and contact information. The same process applies if the patient comes to our institution directly from the field. Our on-call hand surgeon will assess to see if this patient needs to be transferred or not (not all our hand surgeons do re-implantations).
University Hospital – University of Missouri Health Care
1 Hospital Drive, Columbia, MO 65212
1-573-882-6985 - line 1
1-573-771-7860 – line 2
University of Iowa
200 Hawkins Drive, Iowa City, IA 52242
1-319-384-5000
Option – 2 (adult)
Option – 1 (trauma) or Option 2 (ED to ED)
Mayo Clinic
200 First Street, Rochester, MN 55905
1-507-255-2910
Denver Health Medical Center
777 Bannock Street, Denver, CO 80204
1-303-602-5000
Hand Trauma Center Network | About Us | ASSH
We do recognize that in some trauma scenarios it is life over limb. Any poly-trauma patient with potential life-threatening injuries will come to or remain at our Level 1 trauma center where all these issues will be addressed. If a patient is too unstable to be transferred due to other injuries, we will address these life-threatening injuries first. Furthermore, if an outside hospital has a poly-trauma patient with a potential re-implantation, those patients will be directed to our facility given the amount of travel time to nearest re-implantation center. In these situation, we do have the ability to call our hand surgeons that do re-implantations when they are not on-call to inquire for urgent consultation.
Penile Re-implantation
For penile re-implantation, Urology will be consulted for reimplantation or re-creation. They will reestablish a urethra for urinary drainage. Time of reimplantation is determined by Urology and if assistance is required by Plastic surgery, they too will be involved. Both services are available and on-call 24/7.
Trauma Patient Admission Criteria
Trauma patients can be complex with multiple injuries requiring various management strategies, interventions, and care. As a result, determining the appropriate level of care for admission can be challenging. The following represents a list of criteria/conditions that may help guide level of care decision making for the trauma patient.
ICU ADMISSION
- Grade IV or greater solid organ injury or Grade III injury with blush/active extravasation
- Any hemodynamic instability
- Base deficit >6
- Pelvic fractures requiring blood transfusion or IR angiogram/embolization
- Any spine fracture with neurologic deficit
- Mandible fracture with edema or hematoma
- Traumatic brain injury with GCS<13
- Patient >55 yrs of age, on anticoagulation with abnormal CT head
- Risk of airway compromise
- High risk rib fracture patient with FRC<1000mL
- Presence of pulmonary co-morbidities
- Blunt myocardial injury with new
-
- arrythmia
- hemodynamic instability
- cardiac failure
-
- Unstable spine injury
- Frontal contusions >2cm
- Solid organ/pelvis/abdominal injuries with evidence of active extravasation on CT scan
- need for q1hr vital signs/neuro-vascular checks/interventions/etc.
- Trauma attending discretion
SDCC Admission
- Grade II/III solid organ injury without blush/active extravasation on CT
- presence of multiple injuries
- Rib fractures with FRC between 1000mL--1500mL
- Any patient on pre-injury anticoagulation therapy with an injury not requiring ICU
- Major soft tissue trauma in patients on anticoagulation therapy
- Need for q2hr vital signs/neuro-vascular checks/interventions/etc.
- Presence of multiple co-morbidities
- Age > 70
- C-spine fractures exclusive of spinous and transverse process fractures (without neurologic injury)
- History of sleep apnea who needs narcotics
- New CPAP/BiPAP requirements
- Trauma attending discretion
FLOOR Admission
- all other trauma patients who do not meet criteria for ICU or SDCC admission
Trauma Team Activation (TTA) Criteria
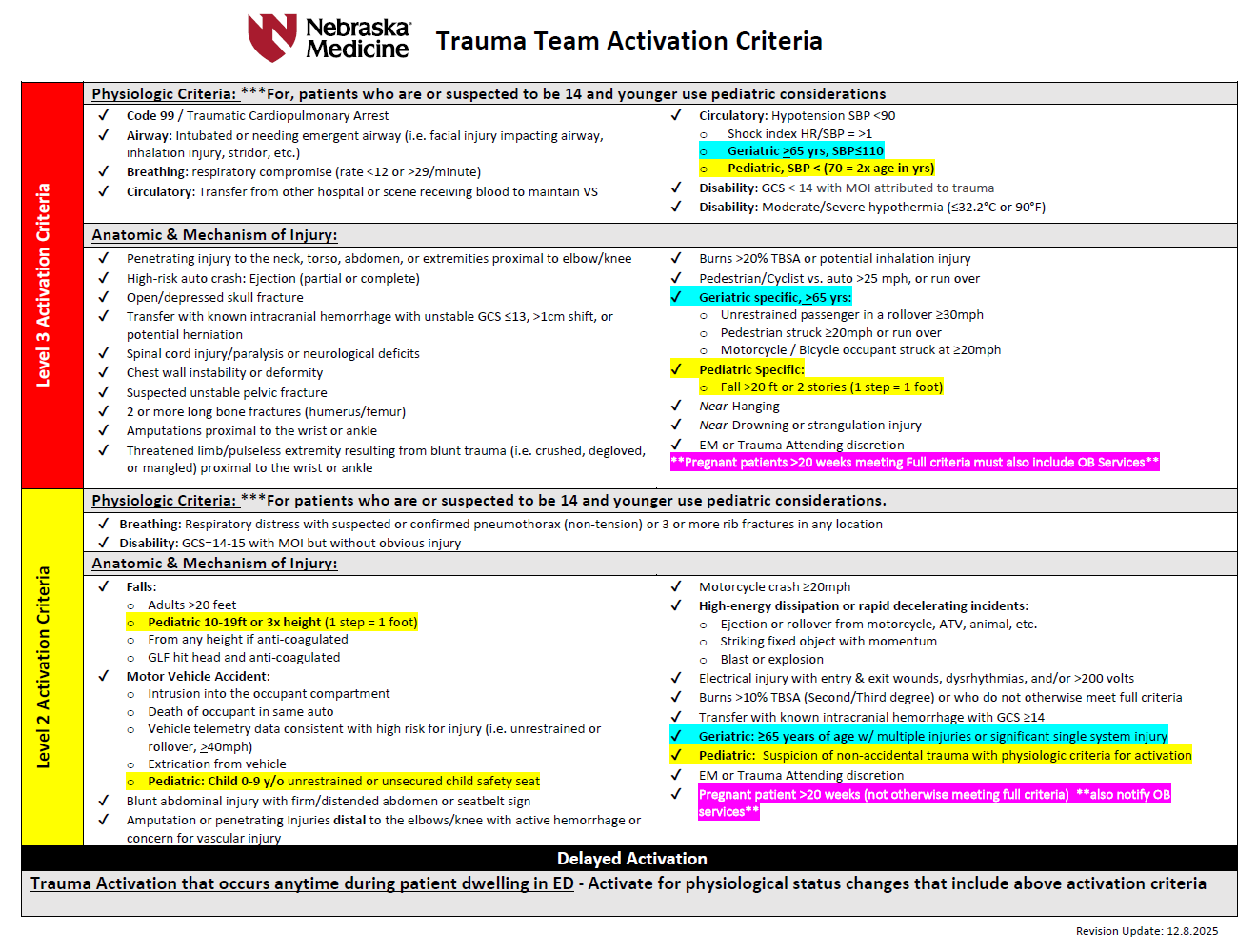
LEVEL 3 trauma team includes:
- Trauma attending
- Emergency medicine (EM) attending and resident
- PGY 4 or 5 surgical resident when available in house
- Junior surgical or EM residents on trauma service
- Trauma advanced practice providers (APP)
- Anesthesia resident (with immediate backup by anesthesia attending)
- Emergency department nurses and technicians
- Pharmacy
- Radiology technician
- Lab technician
- OR RN
- Blood bank (receives page to alert-do not respond in person)
- Spiritual care
- Respiratory therapy
LEVEL 2 trauma team includes:
- EM attending and resident
- General surgery resident(s)
- Trauma advanced practice provider(s) (APP)
- Emergency department nurses and technicians
- Pharmacy
- Radiology technician
- Lab technician
- OR RN (receives page to alert--do not respond in person)
- Spiritual care
- Respiratory therapy
- Trauma attending must respond if PGY4 or 5 surgical resident is not available and must evaluate the patient within 30 minutes of patient arrival.
- If the trauma attending is not in attendance, the EM attending has overall responsibility.
LEVEL 1 - Trauma CONSULTATION
These patients do not meet trauma activation criteria, but merit the expertise of trauma surgeon consultation and/or evaluation, i.e. isolated/single system injuries. A trauma service resident or APP will evaluate these patients within 30 minutes of consult being called and disposition of the patient will be determined within 60 minutes. If the patient requires admission, the trauma attending will evaluate these patients within 8 hours of consult regardless of patient location.
The EM physician or admitted physician will consult the trauma team for any patient requiring admission to the hospital for any traumatic injury that does not meet trauma activation criteria. This will include but is not limited to the following patients:
- Any patient with significant single system injury or multiple injuries
- Stable pelvic fractures (excludes isolated hip fractures)
- Stable chest injuries--rib fracture, sternal fracture, pneumothorax, seatbelt sign
- Minor brain injury (confirmed or suspected) with GCS 13-15
- Abdominal pain with significant mechanism of injury or seatbelt sign
- Spine fractures
- Pregnant patients who require admission to the OB floor for fetal monitoring
- Frostbite
- Any patient returning to the ED for care following treatment for a traumatic injury within the last 60 days
Patients who bypass the ED as a direct admit who are admitted for any injury meeting trauma criteria, will require a trauma consultation after notification of the admitting physician.
Trauma Tertiary Survey
A tertiary survey (exam) should be performed on all patients admitted to the trauma service approximately 24 hours following admission/initial evaluation.
The tertiary survey is a repeat head-to-toe examination of the trauma patient that is designed to identify injuries (usually more minor) that were not identified on the initial evaluation. Ideally the patient should be able to participate in the exam. EXCEPTION--intubated/sedated ICU patients should still receive a tertiary exam ~24 hrs following admission and also AGAIN, when his/her clinical status allows for them to participate in the exam.
The following is included in a trauma tertiary exam:
- complete physical exam
- review of any outstanding or follow-up imaging/labs/tests following initial examination/work-up
- review of previously diagnosed injuries and ensure injury is being addressed (i.e. consults called, treatment plans in progress, etc)
- review of patient's medical history
- ensure home medications have been reconciled and resumed as indicated
- review current status of patient (i.e. are existing lines/tubes still needed? VTE prophylaxis initiated? Activity restrictions? PT/OT/Speech consults? etc)
- update the patient's problems list in electronic medical records
How to complete a trauma tertiary survey at UNMC/Nebraska Medicine
Step 1: perform the tertiary survey
- thorough physical exam
- review all imaging, labs, etc.
- order additional imaging, labs, consults, etc. as indicated
- review injuries, treatment plans, etc and ensure plans are progressing appropriately
Step 2: document your tertiary survey
- New note
- Note type: Trauma Tertiary Survey

Step 3: complete tertiary survey template FULLY and ACCURATELY
- once trauma tertiary survey is selected as note type, a trauma tertiary template will autopopulate.
- fill in ALL values/categories based on your repeat assessment/examination at ~24 hours following admission
-
- this includes the Tertiary Trauma Quality Improvement (TQI) Section
-
- it appears in RED on the tertiary survey template
- this section includes certain pre-existing conditions that will be included in the trauma registry/TQIP database that help accurately capture the patient's status.
- to fill out this section, click on the TERTIARY TRUAMA QUALITY IMPROVEMENT (TQI) ADVANCED button at the top of the note template
- this will pull up a second screen/menu with a list of pre-existing conditions where conditions can be selected as appropriate (see pictures below)
-
- this includes the Tertiary Trauma Quality Improvement (TQI) Section
-


Trauma Quality Indicators
Background:
From the time a trauma patient is picked up by EMS on scene through the patient's initial assessment, hospital course, and discharge, our trauma program is carefully monitoring each patient and collecting data. Data collected includes demographic information, injury information, prehospital and hospital information, past medical history, traumatic injuries, in-hospital events and outcomes. Data is entered into our trauma registry and analyzed regularly through various performance improvement programs to ensure the trauma service is providing high quality care to each patient.
Much of the data collected for the registry is gathered by trauma registrars doing extensive chart reviews and depends greatly on complete and accurate documentation from our trauma providers. While we should be practicing complete and accurate documentation as part of being a good healthcare provider, it is also essential for our trauma program to able to monitor and analyze the care of our trauma patients to ensure that high quality care is provided and patient outcomes are optimized.
Pre-Existing Conditions
Several pre-existing conditions are captured in the trauma registry that help us risk stratify patients for observed and expected outcomes. These pre-existing conditions should be documented in the Trauma H&P and/or the Trauma Tertiary Survey as well as added to the patient's problem list in the electronic medical record.
The pre-existing conditions captured in the trauma registry are as follows:
- Advanced directive limiting care
-
- the patient has a written request to limit life-sustaining treatment that restricts the scope of care for the patient during this patient care event signed/dated by patient or designee prior to arrival.
-
- Alcohol use disorder
-
- can be actual diagnosis OR factors consistent with the diagnosis based on American Psychiatric Association, DSM 5 present prior to injury.
- only report on patients 15 yrs of age or older.
-
- Anticoagulant therapy
-
- administration of medication (including anticoagulants, antiplatelet agents, thrombin inhibitors, thrombolytic agents) that interferes with blood clotting. Exception: chronic aspirin.
-
- Attention deficit disorder/attention deficit hyperactivity disorder (ADD/ADHD)
-
- a disorder involving inattention, hyperactivity, or impulsivity requiring medication for treatment present prior to injury.
-
- Bipolar I/II disorder
-
- only report on patients 15 yrs of age or older.
-
- Bleeding disorder
-
- any condition that results in the blood not clotting properly (e.g. hemophilia, von Willenbrand disease, Factor V Leiden)
-
- Cerebral vascular accident (CVA)
-
- history prior to injury of stroke/CVA (embolic, ischemic, thrombotic, or hemorrhagic) with persistent residual motor, sensory or cognitive dysfunction (e.g., hemiplegia, hemiparesis, aphasia, sensory deficit, impaired memory).
-
- Chronic obstructive pulmonary disease (COPD)
-
- lung disease characterized by chronic obstruction of lung airflow that interferes with normal breathing and is not fully reversible. Includes more familiar terms such as "chronic bronchitis" and "emphysema".
- only report on patients 15 yrs of age or older.
-
- Chronic renal failure
-
- chronic renal failure prior to injury that requires periodic peritoneal dialysis, hemodialysis, hemofiltration, or hemodiafiltration.
-
- Cirrhosis
-
- replacement of normal liver tissue with non-living scar tissue related to other liver diseases often resulting in hepatic insufficiency/dysfunction and based on diagnostic imaging studies or laparotomy/laparoscopy. May also be referred to as end-stage liver disease.
-
- Congenital anomalies
-
- documentation of a pre-existing cardiac, pulmonary, body wall, CNS/Spinal, GI, renal, orthopedic, or metabolic anomaly.
- only report on patients less than 15 yrs of age
-
- Congestive heart failure (CHF)
-
- inability of the heart to pump a sufficient quantity of blood to meet the metabolic needs of the body or can do so only at an increased ventricular filling pressure.
- condition must be noted in medical record as CHF, congestive heart failure or pulmonary edema with onset of increasing symptoms within 30 days prior to injury.
-
- Current smoker
-
- includes patients who report smoking cigarettes every day or some days within the last 12 months.
- excludes patients who smoke cigars, pipes or smokeless tobacco.
-
- Currently receiving chemotherapy for cancer
-
- includes both oral and parenteral treatments
-
- Dementia
-
- includes, but not limited to, Alzheimer's, Lewy body dementia, frontotemporal dementia (Pick's disease), and vascular dementia.
-
- Diabetes mellitus
-
- diabetes mellitus that requires exogenous parenteral insulin or an oral hypoglycemic agent.
-
- Disseminated cancer
-
- cancer that has spread to one or more sites in addition to the primary site (i.e. metastatic or Stage IV cancer)
-
- Functionally dependent health status
-
- patients whom, prior to injury, and as a result of cognitive or physical limitations relating to a pre-existing medical condition, were partially or completely dependent upon equipment, devices or another person to complete some or all activities of daily living.
-
- Hypertension
-
- history of persistently elevated blood pressure requiring antihypertensive medication.
-
- Major depressive disorder
-
- only report on patients 15 yrs of age and older.
-
- Myocardial infarction (MI)
-
- history of MI in the 6 moths prior to injury
-
- Other mental/personality disorders
-
- a diagnosis of any of the following prior to injury: antisocial personality disorder, avoidant personality disorder, borderline personality disorder, dependent personality disorder, generalized anxiety disorder, histrionic personality disorder, narcissistic personality disorder, obsessive-compulsive disorder, obsessive-compulsive personality disorder, panic disorder, paranoid personality disorder, and schizotypal personality disorder.
- only report in patients 15 yrs of age and older
-
- Peripheral arterial disease (PAD)
-
- narrowing or blockage of vessels that carry blood from the heart to the legs. It is primarily caused by the buildup of fatty plaque in the arteries, which is called atherosclerosis. PAD can occur in any blood vessel but is most commonly found in the legs vs arms.
- only report in patients age 15 yrs of age or older.
-
- Post-traumatic stress disorder (PTSD)
-
- only report on patients 15 yrs of age or older.
-
- Pregnancy
-
- pregnancy confirmed by lab, ultrasound or other diagnostic tool OR diagnosis of pregnancy documented in the patient's medical record prior to arrival at your center.
-
- Prematurity
-
- babies born before 37 weeks of pregnancy are completed.
- only report in patients less than 15 years of age.
-
- Schizoaffective disorder
-
- only repot on patients 15 yrs of age or older
-
- Schizophrenia
-
- only report on patients 15 yr of age or older
-
- Steroid use
-
- regular administration of oral or parenteral corticosteroid medications within 30 days prior to injury for a chronic medical condition.
- excludes topical, inhaled, or rectally administered corticosteroids
-
- Substance use disorder
-
- diagnosis or symptoms/patient factors consistent with American Psychiatric Association, DSM 5 present prior to injury.
- only report on patients 15 yrs of age or older.
-
Hospital Events
Events reviewed through our performance improvement program include the following:
- Acute Kidney Injury (AKI)
- Acute Respiratory Distress Syndrome (ARDS)
- Alcohol withdrawal syndrome
- Cardiac arrest with CPR
- Catheter-associated urinary tract infection (CAUTI)
- Central line-associated blood stream infection (CLABSI)
- Deep surgical sight infection
- Deep vein thrombosis (DVT)
- Delirium
- Myocardial infarction (MI)
- Organ/space surgical site infection
- Osteomyelitis
- Pressure ulcer
- Pulmonary embolism (PE)
- Severe sepsis
- Stroke/CVA
- Superficial surgical site infection
- Unplanned admission to the ICU
- Unplanned intubation
- Unplanned visit to the operating room
- Ventilator-associated pneumonia (VAP)
If you are caring for a trauma patient that experiences one of the above stated hospital events, please notify our trauma program/performance improvement coordinators at traumapi@nebraskamed.com.