# 12. Pediatric Trauma
Information dedicated to the care of injured children
# Alcohol and Substance Misuse Screening, Brief Intervention and Referral for Treatment (SBIRT) Guidelines for Pediatric Trauma Patients at Nebraska Medicine
Policy and Procedure Statement
The pediatric co-management team will be consulted on all pediatric trauma patients (18 years and younger) admitted to Nebraska Medicine following injury.
As part of their role in the patient’s care, pediatric co-management will assist the trauma team in performing alcohol and substance misuse screening, brief intervention and treatment (SBIRT) as indicated on pediatric trauma patients age 11 years and older.
Screening:
1. Pediatric trauma patients age 12 years and older will be routinely screened for alcohol and substance use on admission by laboratory screening using blood alcohol level and/or urine drug screen (UDS). Pediatric trauma patients less than 12 years of age will undergo laboratory screening as needed based on history or suspicion of alcohol or substance misuse.
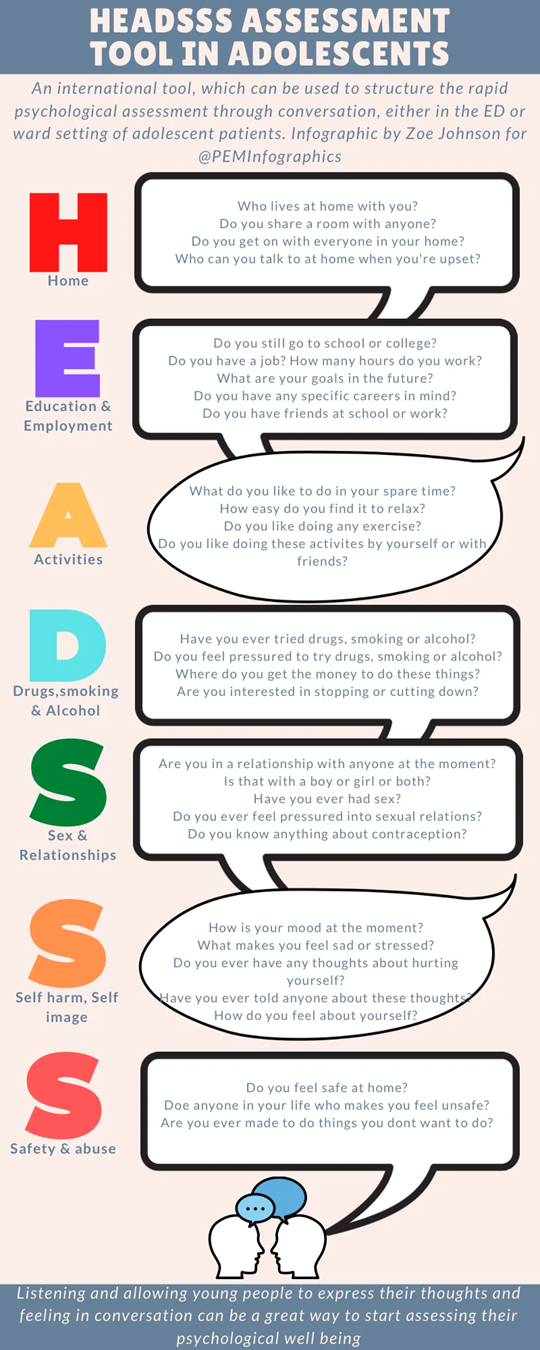
2. A HEADSS assessment will be performed on all admitted pediatric trauma patients age 11 years and older by the pediatric co-management team once the patient reaches floor status.
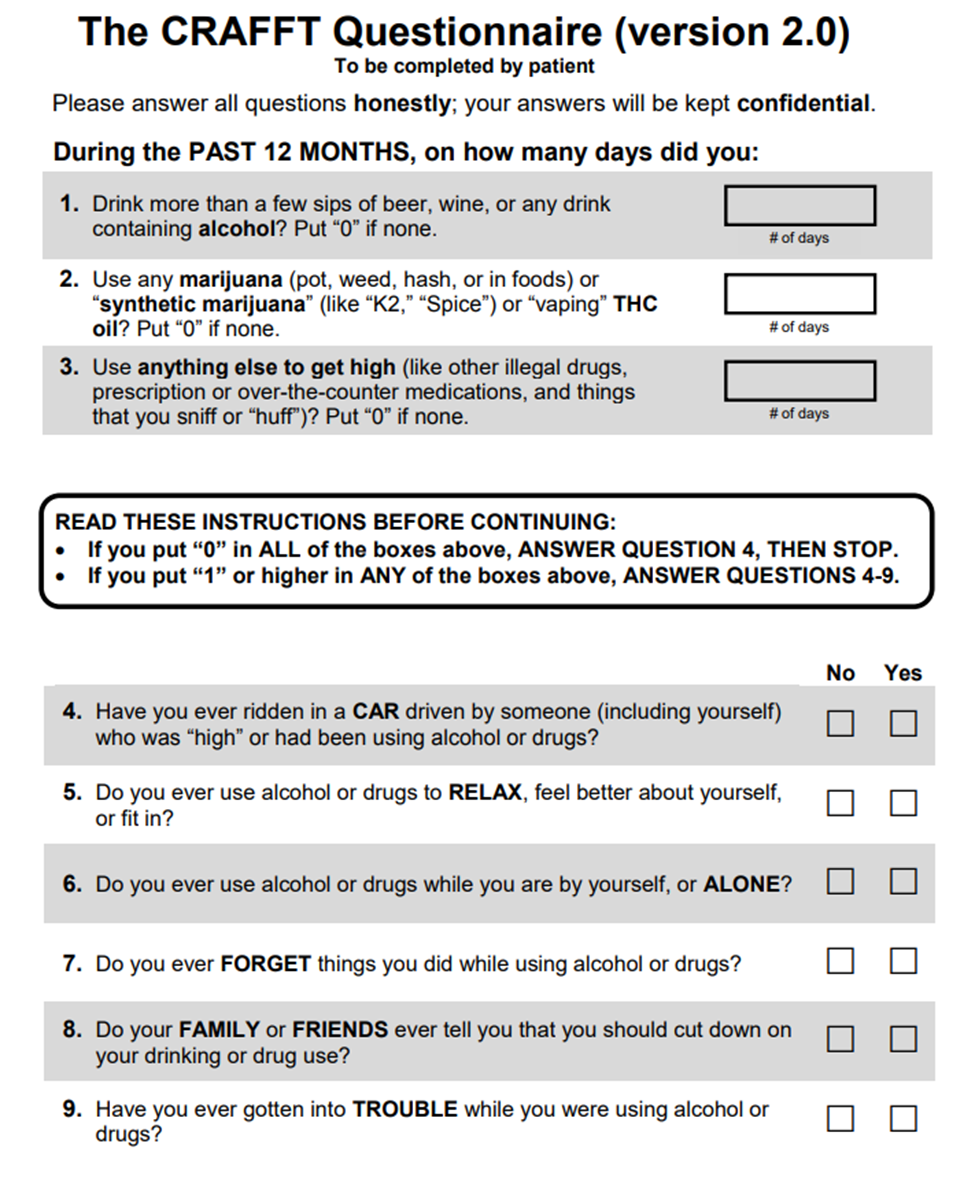
3. If HEADSS assessment is positive for the questions pertaining to drug/alcohol use and exposure AND/OR if blood alcohol (ETOH) or urine drug screen (UDS) testing is positive on admission labs, a CRAFFT screening questionnaire will also be administered.
1. - If the patient is unable to be screened due to the medical condition or refuses, this will be documented in the medical record.
Intervention and Referral for Treatment:
1. A CRAFFT score of 2 or higher indicates a positive screen. Patients with a positive screen will receive a brief intervention conducted and documented by the pediatric co-management provider, social worker or member of child psychiatry team with referrals for outpatient treatment as indicated.
1. - All pediatric patients who screen positive will receive a social work consult for information on area alcohol/substance misuse programs and assistance with referrals as indicated.
- Child psychiatry may be consulted at the discretion of the trauma or pediatric co-management providers for either inpatient or outpatient assessment of alcohol/substance misuse.
Documentation:
The HEADDS assessment, results of alcohol and urine drug screen and CRAFFT assessment (if performed) will be documented in a pediatric co-management team progress note in the patient’s electronic medical record when consulted. For those patients remaining in the ICU for entire hospital course, alcohol and substance misuse screening and interventions will be performed and documented as indicated by the trauma service.
Performance Improvement:
Per American College of Surgeons (ACS) Standards, a minimum of 80% of trauma patients with a hospital stay of >24 hours must be screened for alcohol misuse and a minimum of 80% of patients screening positive must receive an intervention.
Documentation of SBIRT will be done in the trauma registry database.
Any patients that had missed screenings or interventions will be reviewed in the trauma performance improvement process.
References:
1. Cohen E, MacKenzie RG, Yates GL. HEADSS, psychosocial risk assessment instrument: Implications for designing effective intervention programs for runaway youth. *J Adolesc Health* (1991); 12(7):539-544.
2. Katzenellenbogen R, HEADSS: The “Review of systems” for adolescents. *Virtual Mentor* (2005) Mar 1; 7(3): virtualmentor.2005.7.3.cprl1-0503.
3. Knight JR, Sherritt L, Shrier LA, Harris SK, Chang G. Validity of CRAFFT substance abuse screening test among adolescent clinic patients. *Arch Pediatr Adolesc Med*. (2002) Jun;156(6):607-614.
4. American College of Surgeons, Resources for the Optimal Care of the Injured Patient, 2022 Standards.
# Behavioral Consultation Team Contact Information

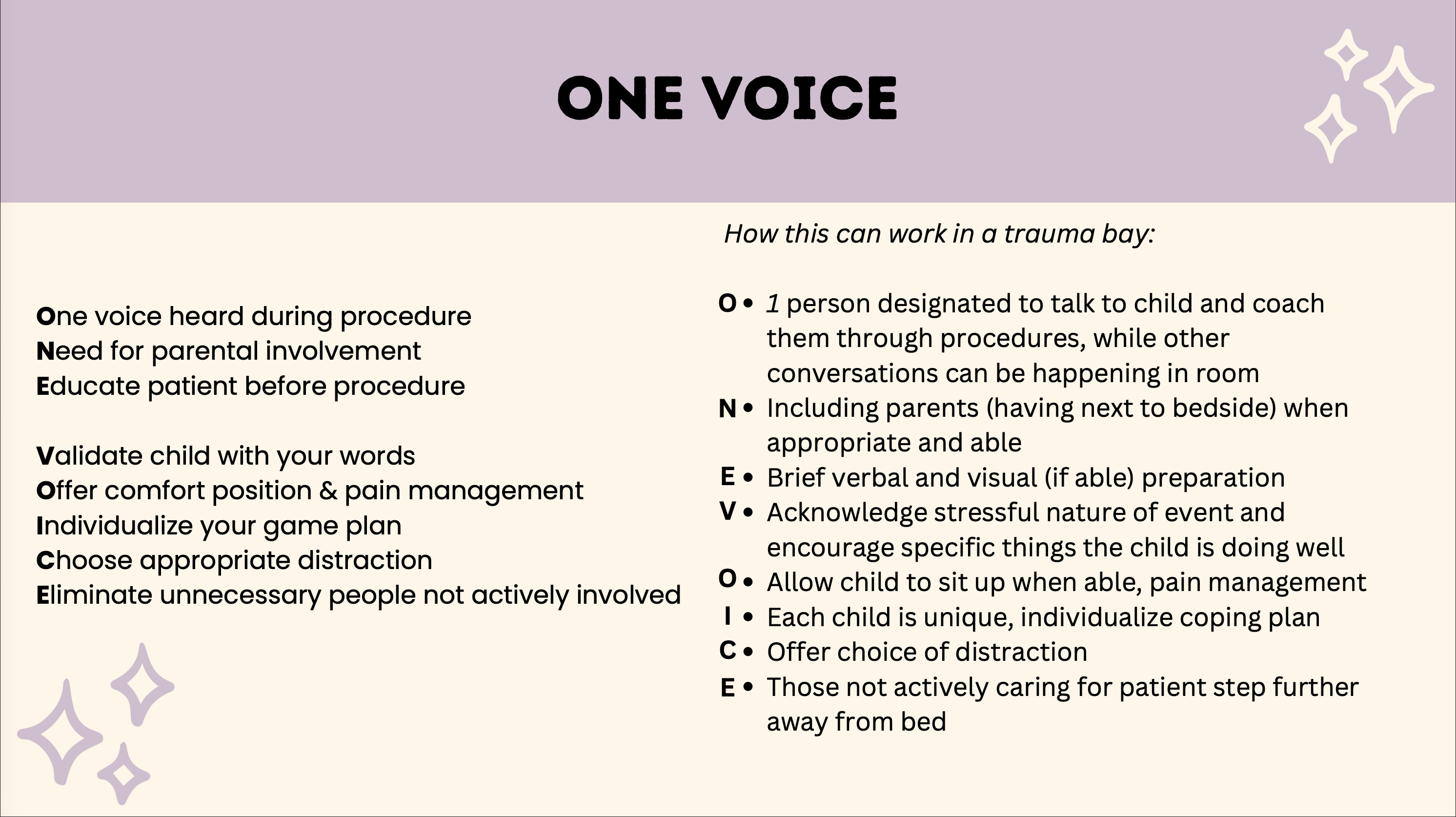
# Child Life in Trauma Resuscitations
[Child Life ED Presentation.pdf](https://paths.trauma.ai/attachments/7)
[](https://paths.trauma.ai/uploads/images/gallery/2026-01/3NGimage.png)
[](https://paths.trauma.ai/uploads/images/gallery/2026-01/0YGimage.png)
[](https://paths.trauma.ai/uploads/images/gallery/2026-01/Zd1image.png)
[](https://paths.trauma.ai/uploads/images/gallery/2026-01/NNfimage.png)
[](https://paths.trauma.ai/uploads/images/gallery/2026-01/l2Jimage.png)
[](https://paths.trauma.ai/uploads/images/gallery/2026-01/4igimage.png)
[](https://paths.trauma.ai/uploads/images/gallery/2026-01/zvvimage.png)
[](https://paths.trauma.ai/uploads/images/gallery/2026-01/Aicimage.png)
[](https://paths.trauma.ai/uploads/images/gallery/2026-01/UDoimage.png)
[](https://paths.trauma.ai/uploads/images/gallery/2026-01/LfIimage.png)
[](https://paths.trauma.ai/uploads/images/gallery/2026-01/cbrimage.png)
[](https://paths.trauma.ai/uploads/images/gallery/2026-01/JMHimage.png)
[](https://paths.trauma.ai/uploads/images/gallery/2026-01/hzzimage.png)
# Discharging a Pediatric Trauma Patient Against Medical Advice (AMA)
#### PURPOSE:
To establish guidelines for addressing situations when minor/pediatric trauma patients depart prior to dismissal by provider (discharge against medical advice) and recognize the right of the patient’s legally recognized representative to make that determination, unless otherwise limited by law.
When any patient leaves prior to dismissal or elopes, it is the policy of Nebraska Medicine to act in accordance with the welfare of the patient and the public while respecting the patient’s rights and complying with applicable laws.
These guidelines are created specifically for the pediatric trauma patient and may not be applicable to adult trauma patients or other service lines. For more information regarding Nebraska Medicine hospital policy, please refer to LD21—Patient Departure Prior to Dismissal (AMA).
#### DEFINITIONS:
- **Departure Prior to Dismissal** (also known as departure against medical advice – AMA): departure of a patient who is admitted to the hospital as an inpatient, outpatient or observation status, or who is in a dedicated Emergency Department but has had a medical screening examination completed; patient may or may not make their intention known to staff.
- **Elopement:** unauthorized departure of a patient from a staffed, around the clock care setting, including the Emergency Department.
- **Imminent Risk for Harm**: immediate and impending threat of physical harm to self or others, as assessed by provider.
- **Minor (pediatric) patient**: any individual receiving care under the age of 19 (as defined by Nebraska state laws)
- **Legally** **recognized representative**: A parent, guardian, or other person with legal authority to make healthcare decisions on behalf of the minor child.
#### POLICY
1. The legally recognized representative (i.e. parent, legal guardian) of a minor patient has the right to terminate the care encounter and remove the patient from the premise at any time, except when prohibited by law.
1. - Patients who are under a legal hold may not have the right to leave the premises at a time of their choose (see policy LD 12-Legal Status Holds).
- Questions about restrictions related to specific legal holds should be referred to Legal or Risk Management.
2. If staff believe that the minor patient may be at risk for serious or imminent harm (i.e medical neglect) if removed from the care environment, it may be appropriate to consider reporting the concern an appropriate authority, such as Child Protective Services or law enforcement.
1. - If there are questions or further discussion regarding the specific situation is warranted, providers are encouraged to call Risk Management at 402-559-0060 (24/7 hotline).
3. Nebraska Medicine will make reasonable efforts to ensure that the minor patient and the legally recognized representative for the minor is informed of the risks of leaving against the advice of the provider.
4. Nebraska Medicine respects the minor patient’s/legally recognized representative’s right to choose to accept or decline care. A patient’s or representative’s decision to leave against medical advice of the provider will not negative influence the patient’s ability to receive future care with Nebraska Medicine.
#### PROCEDURE
- If a minor patient or a patient’s legally recognized representative expresses the desire to leave the premises prior to dismissal against medical advice:
1. - **AND** the patient’s legally recognized representative has **the capacity** to make healthcare decisions AND **is not under a legal hold**:
1. 1. Staff will attempt to request that the patient and legally recognized representative stay to speak with the trauma provider.
2. Staff will notify the trauma provider of the plan to leave against medical advice and may initiate a care discussion, to the extent that the patient and legally recognized representative is willing to participate.
1. - The trauma provider will subsequently notify the trauma attending immediately following notification of a minor patient/representative expressing desire to leave premises against medical advice.
3. The trauma attending will discuss and inform patient and/or legally recognized representative of the risks and benefits of leaving against medical advice, to the extent that the patient is willing to participate.
1. - If staff or providers believe the patient may be at imminent risk for harm if removed from the current care environment, contact Child Protective Services (CPS) or law enforcement as indicated.
- If there are questions regarding case or presence of imminent risk for harm/medical neglect, contact Risk Management at 402-559-0060.
4. The trauma attending/trauma providers, with appropriate assistance from staff, will provide plan for care outside the hospital and instructions appropriate to the patient’s specific needs (i.e. prescriptions, follow-up appointments, DME, etc), to the extent that the patient/representative are willing to participate.
5. Encounter will be documented in the electronic medical record by the trauma attending or designee using the AMA note template (.AMA) and should include the following information:
1. - Patient/representative’s intent to leave and reasons for leaving, if known.
- Specifics of case/injuries known
- Decision making capacity of the patient’s legally recognized representative
- Description of attempts to inform the patient/representative of risks of leaving against medical advice and their response.
- Parent or legal guardian sign the *Informed Refusal of Healthcare Services Form.* This document will be included in the patient's electronic health record (EHR) as a part of the permanent medical record. If the patient or legal guardian refuses to sign the form, ED personnel (or trauma attending if the patient is already admitted) will complete the form noting patient/legal guardian's refusal to sign. When a patient/legal guardian refuses to sing, two witnesses should sign the form.
- Time of departure and condition of the patient as assessed by provider.
- If CPS report filed or law enforcement contact.
- Mode of departure and plans for care outside the hospital and instructions given to patient/representative, as applicable.
#### RELATED POLICIES/PROCEDURES
- Patient Departure Prior to Dismissal (AMA) – LD21
- Legal Status Hold – LD12
- Patients Leaving Against Medical Advice -- OPS17
KEY CONTRIBUTORS
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Manager | Co-Author
---
# Evaluation and Management of Blunt Solid Organ Injuries in Pediatric Trauma Patients
**Purpose:**
These guidelines are meant to help guide the provider through the initial evaluation and management of pediatric trauma patients sustaining blunt solid organ injuries to the liver, spleen, or kidney at Nebraska Medicine.
**Background/definitions:**
Solid organ injuries may occur to the liver, spleen or kidney. Non-operative management of solid organ injuries in the setting of blunt trauma is preferred when possible and is considered the standard of care in hemodynamically stable pediatric patients, irrespective of the grade of injury. Literature reveals that non-operative management of pediatric blunt solid organ injuries is associated with a low overall morbidity and mortality and does not result in increased length of stay, need for blood transfusions, bleeding complications or associated hollow viscous injuries as compared with operative management.
**Guideline Inclusion Criteria:**
- Pediatric trauma patients less than 15 years of age with a radiographically identified blunt liver, splenic or kidney injury at Nebraska Medicine.
**Guideline Exclusion Criteria:**
- Penetrating mechanism of injury
- Trauma patients 15 years of age and older (See separate adult guidelines for management of blunt solid organ injuries).
**Diagnostic Evaluation: **
- All trauma patients should be initially evaluated per ATLS guidelines with work-up as mechanism and clinical presentation dictate.
- Resuscitative measures should be initiated as clinical status/presentation dictates.
- Labs, imaging and additional tests should be obtained as clinical status/presentation dictates. (See “Guidelines For
- Imaging the Pediatric Trauma Patient”)
- If a patient is hemodynamically UNSTABLE, minimal testing/imaging should occur prior to interventions for hemorrhage control.
**Practice Recommendations for Management:**
- Once solid organ injury is suspected and/or confirmed, management of that injury is dictated largely by the clinical status of the patient.
- Initial Evaluation/Resuscitation:
- - oManagement of the hemodynamically **UNSTABLE** patient as evidence by moderate to severe tachycardia and/or hypotension
- - Initial resuscitative measures should include the following:
- - Placement of 2 large bore peripheral IVs (or equivalent central venous access as able)
- Bolus 20 ml/kg NS or LR (if blood not immediately available)
- Type and Cross 2-4 units PRBC (age and weight dependent)
- Transfuse uncrossed PRBC (or whole blood if age≥13 and available) 20mL/kg if hypotension unresponsive to crystalloid bolus.
- Obtain labs (VBG, CBC, PT/INR, etc.)
- Obtain eFAST.
- If eFAST is positive and/or patient remains UNSTABLE (i.e. tachycardia and hypotension persist) despite appropriate resuscitative measures:
- - Activate the Massive Transfusion Protocol (MTP; see policy TX-36 “Massive Transfusion/Severe Coagulopathy/Emergency Release Blood” and PRO09 “Massive Transfusion in Trauma Guidelines”)
- Consider proceeding to OR for emergent laparotomy or IR for angioembolization.
- - Management of the hemodynamically **STABLE** patient as evidenced by mild tachycardia without hypotension OR patients that **become STABLE** with initial resuscitative measures listed above (responders)
- - Initial resuscitative measures as listed above should be performed as indicated based on clinical status of child. At minimum,
- - Ensure and maintain IV access
- If fluid resuscitation not indicated, initiate maintenance IV fluids at weight-based rate, typically with NS or LR
- Send type and screen on all patients and consider type and cross 2 units PRBC depending on any patient with history of hemodynamic instability or those with higher grade injuries.
- Obtain multi-phase CT abdomen/pelvis with IV contrast as indicated by Imaging guidelines for pediatric trauma patients to diagnose/confirm presence of solid organ injury.
- - If renal injury identified, also obtain a delayed imaging phase to assess for involvement of the collecting system.
- Determine appropriate management strategy based on grade of injury, presence of blush/contrast extravasation on imaging, and clinical status/injury burden of the patient.
- Consult urology for renal injuries with disruption/involvement of the collecting system
- Disposition and cares following initial resuscitation:
- - Admission Level of Care
- - Decision for level of care should be based on clinical status of patient, not grade of injury, and is ultimately at the discretion of the trauma attending.
- ICU admission is indicated for the following patients
- - Patients with current hemodynamic instability
- Patients with transient response to initial volume resuscitation
- Patients requiring intervention for hemorrhage control (i.e. IR angioembolization or operative intervention)
- Floor or Progressive Care should be considered for hemodynamically stable patients or those who become stable with sustained response to initial volume resuscitation.
- Activity
- - Bedrest until vitals normal
- Once hemodynamically stable, activity as tolerated with no restrictions.
- Labs
- - CBC on admission and Q6hr until vitals normal and Hb/HCT stable x 2
- Renal function should be monitored with BUN/CRT in setting of kidney injury.
- Diet and IV fluids
- - NPO until vitals normal and Hb/HCT stable
- Once hemodynamically stable, regular diet as tolerated
- Continue maintenance IV fluids until meeting oral hydration goals
- Vital Signs
- - Per unit protocol (ICU-q1hr, Progressive Care-q2hr, Floor-q4hr)
- Transfusion
- - Unstable vitals after 20 mL/kg bolus of isotonic IVF
- Hemoglobin <7
- Signs of ongoing or recent bleeding
- Other Orders
- - Strict Intake and Output (I&O)
- Pain control: Tylenol PRN, additional medications at discretion of trauma provider.
- Be mindful of using aspirin or ibuprofen/NSAIDs and limit use when able.
- VTE prophylaxis per “VTE prophylaxis in Trauma Patients” (PRO 10) guidelines
- Angioembolization or Operative Exploration
- - Should be considered in patients with signs of ongoing bleeding despite blood product transfusion
- Angioembolization is NOT indicated for contrast blush on admission CT without unstable vitals
- Operative exploration may be indicated when additional procedures or information are needed
- Patients presenting with or who develop peritonitis should undergo operative exploration.
- Discharge Criteria
- - Hb/HCT stable x 2
- Acceptable pain control with oral pain medications
- Tolerating diet
- Vital signs within normal limits
- Late Presentation
- - Management of stable patients presenting 24-48 hours post injury is at the discretion of the trauma surgeon and may be based on the reason for finally seeking care (pain, ileus, etc.)
- Consider observation for serial exams vs discharge home with follow up and ground level activity.
- Hemoglobin rechecks are optional and based on clinical status
- Diet and activity restrictions are based on clinical status
- Repeat Imaging
- - Routine follow-up imaging is not required. Decision to obtain repeat imaging should be based on clinical status of patient and at discretion of trauma attending.
- Post splenectomy vaccines
- - Patients undergoing splenectomy as management of their splenic injury should obtain the following vaccines prior to discharge or at 14 days post-op (whichever date comes first)
- - Quadravalent meningococcus (Menactra or Menomune)
- Pneumococcus (Pneumovax 23)
- H.influenzae B (HIB, ActHIB)
- Viral influenza vaccine (depending on time of year)
**Follow-up Care:**
- Upon discharge from hospital, patient may return to school and resume ground level activities with restrictions as noted below:
- - Grade of Injury + 2 weeks = # weeks of activity restrictions (for example: Grade 2 injury + 2 weeks = 4 weeks of activity restrictions)
- Activity restrictions include: no gym/PE, recess, playground play, sports, no wheeled equipment, manual labor, farm labor, large animal care, or other activities where one could fall/sustain blow to abdomen.
- Patient should be instructed to call trauma surgery with any increasing pain, pallor, dizziness, vomiting, worsening shoulder pain, GI bleeding or black tarry stools, or jaundice.
- Follow-up in trauma surgery clinic:
- - Grade 1 and 2 injuries = 2 weeks or with a follow up phone call
- Grade 3, 4, or 5 injuries or those undergoing operative/IR intervention = 2 weeks.
- Routine follow-up imaging is not required. Repeat imaging should be based on clinician determination and clinical situation.
- For kidney injuries, refer to primary care provider/pediatrician for ongoing blood pressure monitoring.
**Outcome Measures and Guideline Adherence:**
- Time to OR/IR and interventions for all hemodynamically unstable patients and patients failing non-operative management will be tracked through our performance improvement process.
**Related Policies:**
- Adult guidelines for management of blunt solid organ injuries
- Guidelines For Imaging the Pediatric Trauma Patient
- Massive Transfusion for Trauma Guidelines (PRO 10)
**Key Contributors:**
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Abby Josef, MD | Division of Acute Care Surgery, Faculty | Reviewer
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Coordinator | Reviewer
**Last updated:**
·August, 2024
**References:**
1. Williams RF, Grewal H, Jamshidi R et al. Updated APSA guidelines for the management of blunt liver and spleen injuries. *J Pediatr Surg.* 2023; 58:1411-1418.
2. Gates RL, Price M, Cameron DB, et al. Non-operative management of solid organ injuries in children: an American pediatric surgical association outcomes and evidence based practice committee systemic review. *J Pediatr Surg.*2019 Aug: 54(8):1519-1526.
3. Linnaus MR, Langlais ME, Garcia NM, et al. Failure of nonoperative management of pediatric blunt liver and spleen injuries: A prospective Arizona-Texas-Oklahoma-Memphis-Arkansas Consortium Study. *J Trauma and Acute Care.* 2017; 82(4):672-679.
**Appendix/supplemental materials:**
1. ******Updated American Pediatric Surgical Association (APSA) Blunt Liver/Spleen Injury Guidelines**
[](https://paths.trauma.ai/uploads/images/gallery/2024-09/embedded-image-zlw6w91c.png)
**2.****AAST Injury Grading Scales**
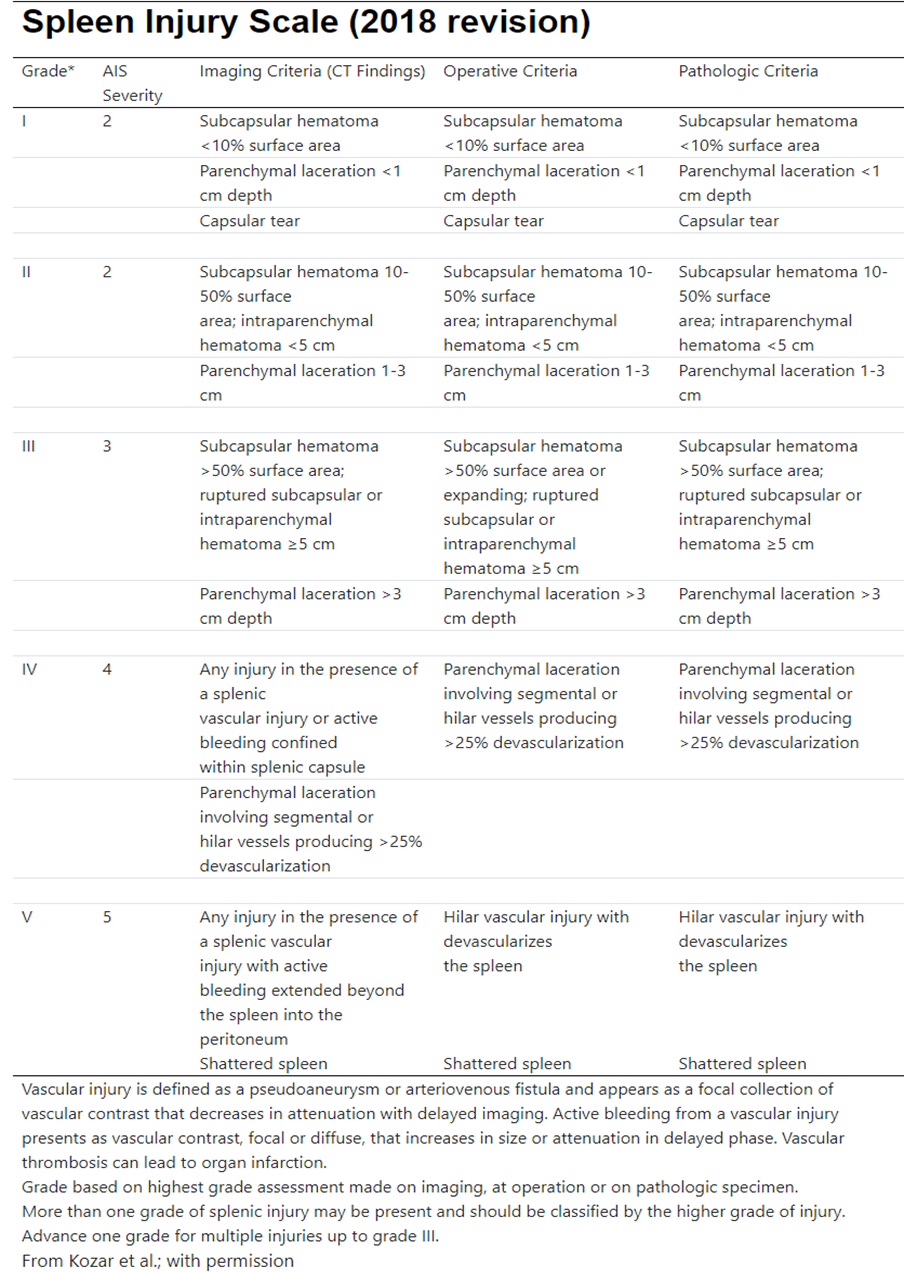
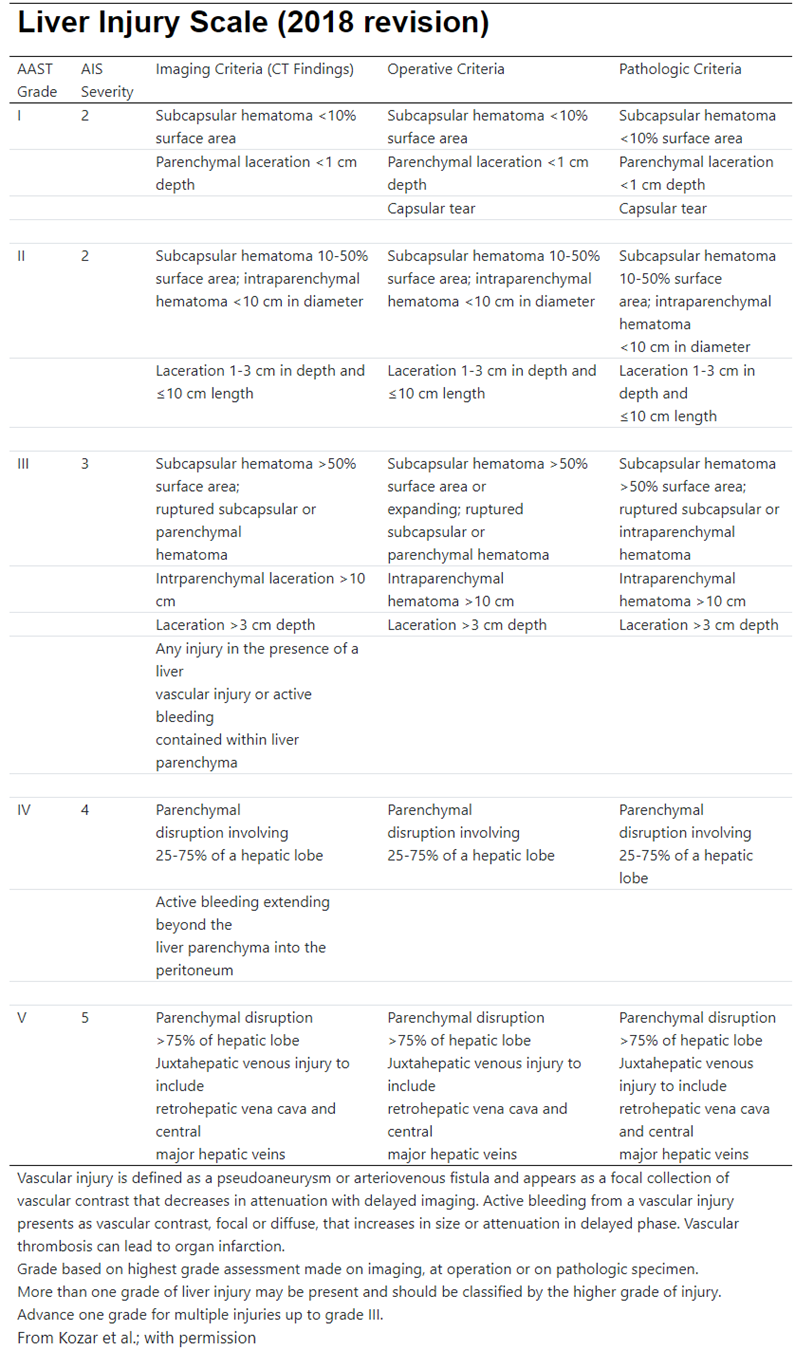
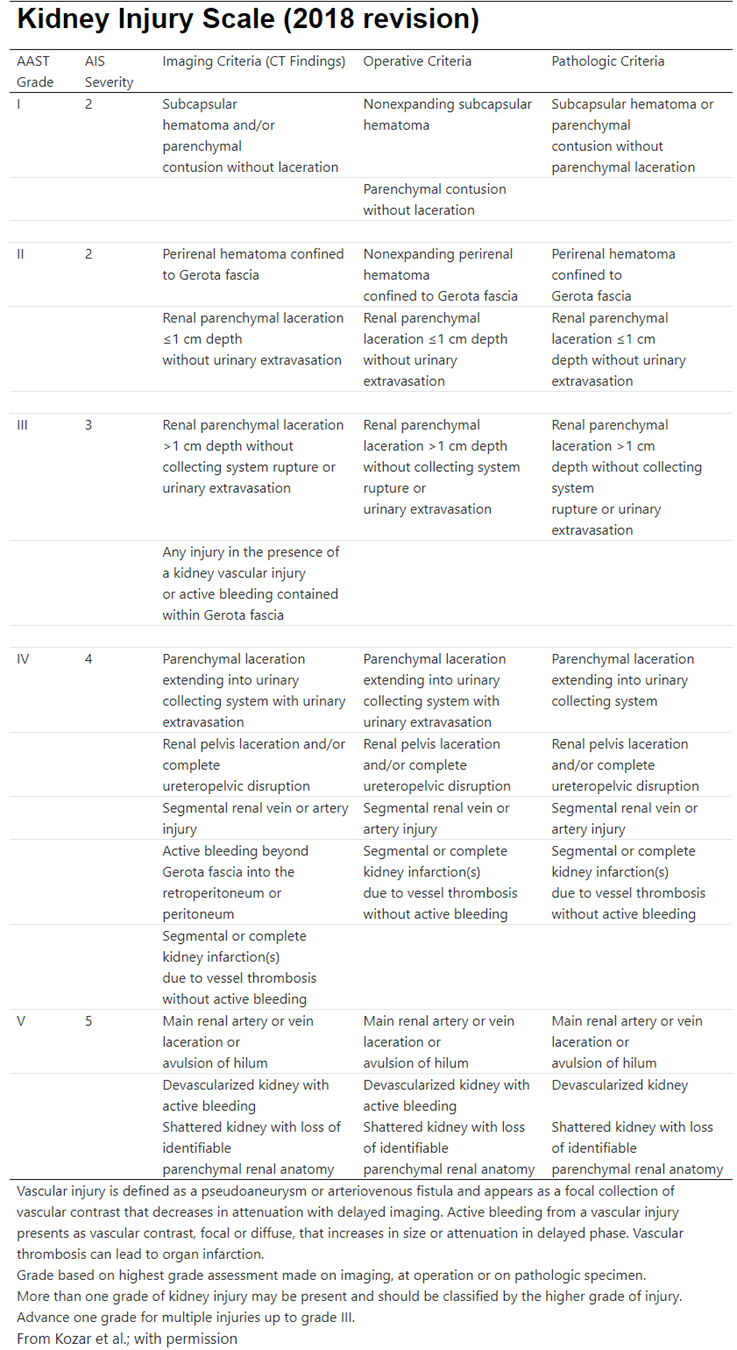
# Evaluation and Management of Non-Accidental Trauma (NAT) in Children at Nebraska Medicine
#### **Purpose:**
To provide guidance and a standardized approach for the initial evaluation, management and reporting of children with injuries concerning for abuse.
#### **Background/Definitions:**
Annually, nearly 1 million children are victims of child maltreatment in the United States. It is estimated that 1:4 children will experience some form of child abuse or neglect in their lifetime (1:7 in the past year) accounting for a total lifetime economic cost upward of $124 billion. The Centers for Disease Control (CDC) defines child maltreatment as “any act or series of acts of commission or omission by a parent or other caregiver that results in harm, potential for harm, or threat of harm to a child.”
- Physical abuse, sexual abuse, and psychological abuse are types of abuse resulting from acts of commission.
- Acts of omission or neglect (e.g. delays in seeking treatment/care, inappropriate supervision, not using vehicle restraints) can worsen outcomes when the child is abused. The Child Abuse Prevention and Treatment Act (CAPTA) establishes that standard legal definition ofchild abuse and neglect as “any recent act or failure to act on the part of the parent or caretaker which results in death, serious physical or emotional harm, sexual abuse or exploitation; or an act or failure to act, which presents an imminent risk of serious harm.” In 2019, there were approximately 656,000 victims of child abuse and/or neglect in the United States as confirmed by state child protective service agencies.
- This equates to a national rate of 8.9 victims per 1,000 children in the population.
- Approximately 28% of victims were in the range of birth through 2 years old. 14.9% of all victims were younger than 1 year. The rate is highest for children younger than 1 year old at 25.7 per 1,000 children in the population of the same age.Nationally, there were an estimated 1,840 children who died from abuse and neglect in 2019.
- This is a rate of 2.5 deaths per 100,000 children in the population. This is an approximate 10.8% increase from the 2015 estimation.
- Approximately 70% of all child fatalities were younger than 3 years old and close to half (45.4%) of all child fatalities were younger than 1 year old.
- The child fatality rates mostly decrease with age. Younger children are the most vulnerable to death as the result of child abuse and neglect.
- Nearly 80% of all fatalities involved one or both of the parents. Sentinel injuries are injuries suspicious for physical abuse with rates of abuse high enough to warrant routine evaluation of abuse if the injury is present. Sentinel injuries can seem minor, and high level of suspicion and familiarity with high-risk injuries is critical for identification. For the purposes of this guidelines, a non-ambulatory child is a child who cannot take two independent steps without the assistance of a person or inanimate object for support. Cruising is not considered ambulatory.
#### **Guideline Inclusion Criteria:**
·Children from newborn through adolescence (18 years and younger) with an injury concerning for physical abuse.
#### **Guideline Exclusion Criteria**:·Injured patients age >18 years. ·Children involved in a motor-vehicle collision, regardless of age or ambulatory status, are excluded from this guideline.
#### **Diagnostic Evaluation: **
While any injury can be the result of physical abuse, there are NO injuries that are pathognomonic. The following are reasons to be concerned that injuries could be related to physical abuse (this list is not exhaustive):History:
- No explanation or vague explanation of injury.
- An important detail of the explanation changes significantly.
- An explanation that is inconsistent with the pattern, age or severity of the injury or injuries.
- An explanation that is inconsistent with the child’s physical and/or developmental capabilities.
- Different caregivers provide different explanations for the injury or injuries, or a single caregiver provides history that changes over time.
- Unwitnessed injury
- Delay in seeking care for an injury.
- Prior ED visits for injury
- Domestic violence in home
- Premature infant (<37 weeks)
- Low birth weight/IUGR
- Presence of chronic medical conditionsPhysical Exam:
- Age:
- - All ages
- Non-ambulatory and non-verbal children are particularly vulnerable.
- Bruising:
- - Bruising in children <9 months of age
- Any bruise in non-ambulatory children
- Patterned bruising
- Extensive or clustered bruising
- Intraoral injuries (i.e. frenulum tears, pharyngeal injury) <9 months or non-ambulatory
- The **TEN-4-FACESp** Bruising Clinical Decision Rule is a highly sensitive and specific tool in identifying bruising that is concerning for abuse.
- - “**TEN**”: bruising on **T**orso (chest, abdomen, back buttocks, GU region, hips), **E**ars or **N**eck.
- “**FACES**”: bruising on **F**renulum, **A**ngle of jaw, **C**heek (fatty portion), **E**yelids, **S**ubconjunctivae
- “**4**”: “TEN-FACES” bruising on a child younger than **4 years** old or any bruising in an infant **4 months** or younger.
- “**p**”: **P**atterned bruising
- Burns
- - Patterned burns (i.e. suspected cigarette burns or other burns with a particular shape)
- Stocking or glove immersion burns
- Burns in non-ambulatory patients.
- Fractures (Highly specific for physical abuse)
- - Classic metaphyseal lesions (i.e. long bone fractures at the infant growth plate)
- Rib fractures (particularly posteromedial)
- Scapular or sternal fractures
- Spinous process fractures
- Fractures (moderately specific for physical abuse)
- - Non-ambulatory child
- Digit fractures
- Complex skull fractures
- Vertebral body fractures/subluxations
- Epiphyseal separations
- Fractures of varying ages
- Multiple fractures, especially bilateral
- Pelvic fractures
- Abusive head trauma (AHT)
- - Vague presenting signs and symptoms may be associated with AHT. AHT should be considered in the differential diagnoses of young children with non-specific history of/findings such as:
- - Altered mental status (lethargy, fussiness)
- Seizures/seizure-like activity
- Vomiting
- Cyanosis
- Marked change in muscular tone
- Apnea/reported apnea
- Decreased or irregular breathing
- Enlarging head circumference
- Diffuse intracranial hemorrhage
- Mixed density intracranial hemorrhage
- Bilateral intracranial hemorrhage
- Intracranial hemorrhage with altered mental status
- Intracranial hemorrhage with no history of trauma
- Intracranial hemorrhage with ischemic parenchymal injury
- Intracranial hemorrhage with spinal/paraspinal hemorrhage and/or spinal ligamentous injury
- Intracranial hemorrhage with other evidence of injury (cutaneous, skeletal, intraabdominal)
- Parenchymal injury (contusion, tear, diffuse axonal injury)
- Diffuse cerebral edema without identifiable intracranial hemorrhage on head CT.
- Retinal hemorrhages (those that are too numerous to count/diffuse in one or both eyes, present in multiple layers of retina, and extending into the retinal periphery are most concerning)
#### **Practice Recommendations for Management:**
Injured children presenting to Nebraska Medicine should be initially evaluated and managed in accordance with ATLS guidelines. Clinicians should first ensure the child is medically stable. If during the assessment concerns for physical abuse/non-accidental trauma are raised, the following additional work-up should ensue as early as practical based on the severity of injuries and clinical status of the child. Initial Management:
**Children 0 to 24 months meeting at least one of the following criteria:**
1. Less than 24 months with an injury concerning for abuse
2. Non-ambulatory with a skeletal fracture
3. Less than 12 months with a skeletal fracture
- Thorough history
- - Detailed description of illness/injury from the time the child was last well. Include any history of trauma as well as circumstances leading to the discovery of the injury.
- It is important to document the history as early as practical in the process.
- Note inconsistencies and changing histories as well as delays in care.
- Full medical history of the child (birth history, prior hospitalizations/ED visits/injuries/wellness visits), development (normal vs abnormal) and social history (all caregivers and other who live in household, domestic violence prior CPS/police contact)
- Head to toe physical assessment
- - Review vital signs, neurologic exam, thorough skin assessment including ears and frenula.
- Detailed documentation of all the abnormal findings.
- Social work consultation.
- - Social worker can assist in obtaining a detailed psychosocial history and assessment from family/caregivers, assist in communication with law enforcement and CPS as indicated, and communication with the Children’s Advocacy Team.
- Children’s Advocacy Team (CAT) consultation (Most consults can be called during regular business hours, M-F, 8am-5pm).
- Make report to Child Protective Services (CPS).
- - Report may be made by any provider/person involved in child’s care who has reasonable cause to believe that the child subjected to abuse or neglect. It is a criminal offense to NOT report if abuse/neglect is suspected.
- - CPS report number should be documented in a progress note in the patient’s electronic medical record.
- Trauma attending must be notified that a CPS report has been filed.
- Inform parents/caregivers of child if a CPS referral has been filed and should ideally be done by trauma attending or next most senior provider or social worker involved in child’s care.
- If child is felt to be in imminent danger, involve law enforcement/police (based on location of where the alleged abuse/neglect occurred)
- Skeletal survey
- Transaminase levels (AST/ALT) and serum lipase
- Head CT without contrast
- - All children less than 6 months
- Children 6-12 months with neurologic abnormality and/or external evidence of head injury.
- See “abusive head trauma” (AHT) section
- Photo documentation in the electronic medical record of all external injuries, including burns, if the injury is concerning for abuse.
**Children >24 months with an injury concerning for abuse will receive the following: **
- Thorough history
- - Detailed description of illness/injury from the time the child was last well. Include any history of trauma as well as circumstances leading to the discovery of the injury
- It is important to document the history as early as practical in the process.
- Note inconsistencies and changing histories as well as delays in care.
- Full medical history of the child (birth history, prior hospitalizations/ED visits/injuries/wellness visits), development (normal vs abnormal) and social history (all caregivers and other who live in household, domestic violence prior CPS/police contact)
- Head to toe physical assessment
- - Review vital signs, neurologic exam, thorough skin assessment including ears and frenula.
- Detailed documentation of all the abnormal findings.
- Social work consultation.
- - Social worker can assist in obtaining a detailed psychosocial history and assessment from family/caregivers, assist in communication with law enforcement and CPS as indicated, and communication with the Children’s Advocacy Team.
- Children’s Advocacy Team (CAT) consultation (Most consults can be called during regular business hours, M-F, 8am-5pm).
- Make report to Child Protective Services (CPS).
- - Report may be made by any provider/person involved in child’s care who has reasonable cause to believe that the child subjected to abuse or neglect. It is a criminal offense to NOT report if abuse/neglect is suspected.
- - CPS report number should be documented in a progress note in the patient’s electronic medical record.
- Trauma attending must be notified that a CPS referral has been filed.
- Inform parents/caregivers of child if a CPS referral has been filed and should ideally be done by trauma attending or next most senior provider or social worker involved in child’s care.
- If child is felt to be in imminent danger, involve law enforcement/police (based on location of where the alleged abuse/neglect occurred).
- Skeletal survey—recommended only in children up to 5 years on a case by case basis:
- - i.e. unconscious patient, non-verbal patient, non-ambulatory patient, or inadequate exam.
- Transaminase levels (AST/ALT) and serum lipase
- - Recommended with multiple or severe injuries or with concern for abdominal or pelvic trauma
- Head CT without contrast
- - Children with neurologic abnormality and/or external evidence of head injury.
- See “abusive head trauma” (AHT) section
- Photo documentation in the electronic medical record of all external injuries, including burns, if the injury is concerning for abuse. Additional Laboratory and Diagnostic Evaluation Additional labs, imaging and testing may be obtained as indicated specific to the injury or individual circumstances. If there are questions regarding what additional testing is needed, please discuss with the CAT.
- Laboratory:
- - Urine and serum toxicology
- - Concern for ingestion
- Evidence of neurologic abnormality
- - - If CT head is obtained due to concerns for abusive head trauma (fussiness, vomiting, seizures, brief resolved unexplained event (BRUE), etc.), urine and serum toxicology is also indicated.
- Report or suspicion of substance abuse in caregiver, either by history or presentation.
- CBC, PT/INR, PTT, vW panel, Factor VIII and IX levels
- - Intracranial hemorrhage (ICH) concerning for abusive head trauma
- Consider in patient with diffuse cerebral edema without identifiable ICH on CT head.
- Bruising concerning for inflicted injury
- - - Factors which increase the likelihood of abusive bruising include:
- - <9 months of age
- Non-ambulatory child
- Bruising which meets the TEN-4-FACESp Bruising Clinical Decision Rule Criteria.
- Other injuries associated with bleeding
- - Solid organ injury concerning for inflicted trauma
- Children with clinically significant bleeding
- Bone abnormality evaluation (25-hydroxy-Vit D, bioactive PTH, Alkaline Phosphatase, Calcium, Phosphorus levels)
- - Recommended in children with >1 skeletal fracture concerning for abuse
- Recommended in children with a skeletal fracture(s) with radiographic concern for osteopenia or metabolic bone disease
- Special consideration (after discussion with CAT team)
- - Ionized calcium
- - Children with hypoalbuminemia or who appear malnourished or concern for failure to thrive
- Serum copper, ceruloplasmin, and vitamin C
- - Consider in children at risk for scurvy or copper deficiencies in the setting of metaphyseal irregularities
- Imaging:
- - CT Abdomen/Pelvis with IV contrast
- - Abnormal abdominal exam such as bruising, distention, tenderness, vomiting
- Consider with >10 RBCs per HPF on urinalysis
- ALT or AST >80 mg/dL or Lipase >100
- - Or admit to trauma service for observation and serial abdominal exams.
- May be indicated as per CAT.
- MRI/MRV brain with and without contrast
- - May be indicated with ICU to further delineate injury, per Trauma, Neurosurgery, or CAT.
- MRI cervical, thoracic, lumbar spine without contrast
- - May be indicated with ICU to further delineate injury, per Trauma, Spine (neurosurgery or orthopedic surgery), or CAT. Consultation
- Social Work Consult
- - All patients with history or exam/diagnostic findings that may be concerning for abuse warrant a comprehensive psychosocial social work evaluation, preferably performed in the ED on initial evaluation or as soon as practical following admission.
- Child Protective Services (CPS)
- - In accordance with federal and state laws, any person with concerns about the safety of a minor must initiate a referral to CPS. If made, the trauma attending provider must be made aware of this referral.
- Children’s Advocacy Team (CAT)
- - Consultation indicated when there are concerns of abuse identified by social work or trauma team provider. Most consults can be placed during regular business hours, M-F, 8am-5pm.
- Orthopedic surgery
- - All children with bony fracture identified must have orthopedic consultation prior to disposition from the emergency department.
- Neurosurgery
- - Children with skull fractures or intracranial hemorrhage must have neurosurgical consultation prior to disposition from the emergency department.
- Ophthalmology
- - Indicated in children with intracranial hemorrhage and injuries to the face/neck/eyes that are felt to be secondary to or concerning for abuse OR for eye findings concerning for genetic disorders.
- Hematology consultation
- - Consult for cases where lab or other clinical findings are concerning for bleeding disorders.
- Pediatric Co-management
- - Consulted on all admitted pediatric trauma patients (18 years and younger) and can assist in the work up of NAT as well as communication with CAT. Admission/Disposition
- **For children with injuries requiring admission** for medical or surgical management, the TRAUMA SERVICE will be the primary admitting service with CAT, Pediatrics (either pediatric critical care or pediatric co-management team depending on level of care), and subspecialty consultation as indicated.
- - - - The family should be informed of the plan to involve CAT if applicable.
- Isolated injuries with no ongoing concerns for abuse may be admitted to the appropriate surgical subspecialty as appropriate (i.e. orthopedics, neurosurgery, etc.).
- Other considerations:
- - Non-surgical admissions
- - - - In general, children with traumatic injury felt to be secondary to abuse should NOT be admitted to a non-surgical service unless it is felt to be in the best interest of the patient (i.e. medically complex with minor traumatic injury not requiring intervention). If the child is being admitted to a non-surgical service, the attending trauma surgeon must explicitly document why he/she feels the child would be better served by a non-surgical service.
- Children admitted for a medical/non-traumatic diagnosis (i.e. seizures, failure to thrive, etc.) and are later suspected or discovered to have a traumatic injury should have a trauma consultation as soon as the injury is discovered. Trauma team consultation should not be delayed for a sub-specialty surgical consult.
- **For children with injuries that do NOT require admission** for medical/surgical management but have **reasonable concern for abuse**,
- - Consult the ED social worker who will email CAT ([CATRN@childrensnebraska.org](mailto:CATRN@childrensnebraska.org)) with details of the case for review.
- - CAT will contact the family if follow-up is indicated.
- Do not instruct the family to call CAT.
- CPS report is made.
- - Request CPS involvement for discharge. If/when a safe disposition has been established by CPS and agreed upon by ED/Trauma/SW providers, the patient may be discharged from the ED.
- If a safe disposition cannot be developed by CPS in the ED in a timely fashion, the patient will be admitted to the Trauma Service for observation until a plan is in place.
- **For children with injuries that do NOT require admission** for medical/surgical management, but provider is **unsure** if there is reasonable concern for abuse,
- - - - During normal business hours (M-F, 8a-5p), provider to call CAT at 402-955-6250 or by calling the Children’s Physician Priority line at 855-850-KIDS (5437) and asking for provider on call for CAT.
- If after hours/weekends, provider to call the on-call CAT provider by calling the Children’s Physician Priority line at 855-850-KIDS (5437)
- ED social worker emails CAT ([CATRN@childrensnebraska.org](mailto:CATRN@childrensnebraska.org)) with details of case for review.
- Provider is to call the on-call CAT provider to discuss and develop a plan.
- - CAT will contact the family if follow-up is indicated.
- Do not instruct the family to call CAT.
- CPS report at discretion of providers/SW/CAT
- - If CPS is notified, request CPS involvement for discharge. Once a safe disposition has been established by CPS and agreed upon by ED/Trauma/SW providers, the patient may be discharged from the ED.
- If a safe disposition cannot be developed by CPS in the ED in a timely fashion, the patient will be admitted to the Trauma Service for observation until a plan is in place.
**\*\*\*Please see algorithm from Pediatric Trauma Society and Western Trauma Association below as an additional guide to what is stated above\*\*\***
Reminders:
- Do not accuse or treat families/caregivers any differently than others. Keep the discussion neutral and patient centered/focused.
- Discuss suspected abuse reporting requirements with family/caregivers.
- Consider having the senior staff (APP or attending) or senior resident as the primary providers for these cases.Important phone numbers:
- Nebraska Child Protective Services Hotline: 800-652-1999
- Iowa Department of Human Services Hotline: 800-362-2178
- Children’s Advocacy Team: 402-955-6250
- Children’s Social Work Department: 402-955-5418
- Children’s Physician Priority Line: 855-850-KIDS (5437)
- Omaha Police Department, Child Victim/Sexual Assault Unit: 402-222-5636 or 402-444-4135
- Bellevue Police Department: 402-293-3100
- Children’s Advocacy Team (CAT) email: [CATRN@childrensnebraska.org](mailto:CATRN@childrensnebraska.org)
**Follow-up Care:**
- Injured children may follow-up with trauma and consulted subspecialty teams as indicated for injuries.
- Children’s Advocacy Team as indicated for all aspects of care related to and sequela of abuse/neglect.
**Outcome Measures and Guideline Adherence:**
- All cases of traumatic injury secondary to non-accidental trauma will be reviewed by the pediatric trauma medical director and pediatric trauma program manager at a primary level. Additional levels of review will be performed on a case-by-case basis and involve consultant teams and Child Advocacy Team as needed.
**Related Policies:**
- Nebraska Medicine Policy PE02, “Identification of Abuse or Neglect”
- Nebraska Medicine Policy PE 03, “Reporting of Abuse, Neglect, or Injury”
**Key Contributors:**
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principal Author
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Coordinator | Co-Author
- Suzanne Haney, MD, MS, FAAP | Division Chief, Child Abuse Pediatrics | ReviewerLast updated:·June 2024
**References**:
1. Prevention CDCa. *Child Maltreatment: Fact-Sheet.* Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention; 2014. [http://www.cdc.gov/ncipc/factsheets/cmfacts.htm](http://www.cdc.gov/ncipc/factsheets/cmfacts.htm).
2. Prevention CDCa. *Child Abuse and Neglect Prevention.* Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention; 2017. [http://www.cdc.gov/violenceprevention/childmaltreatment/](http://www.cdc.gov/violenceprevention/childmaltreatment/).
3. Finkelhor D, Turner HA, Shattuck A, Hamby SL. Violence, crime, and abuse exposure in a national sample of children and youth: an update. *JAMA Pediatr.* 2013;167(7):614-21.
4. Leeb RT, Paulozzi L, Melanson C, et al. *Chile Maltreatment Surveillance: Uniform Definitions for Public Health and Recommended Data Elements,* Version 1.0. In: Center for Disease Control and Prevention NCflPaC, editor. Atlanta, GA. 2008.
5. U.S. Department of Health and Human Services ACYF, Administration on Children, Youth and Families, Children’s Bureau. *Child Maltreatment 2016.* Washington, D.C.: Children’s Bureau (Administration for Children, Youth, and Families, Administration for Children and Families) of the U.S. Department of Health and Human Services, 2018.
6. Berger RP, Lindberg DM. Early recognition of physical abuse: Bridging the gap between knowledge and practice. *J Pediatr*. 2018; 204:16-23.
7. Pierce MC, Kaczor K, Aldridge S, O’Flynn J, Lorenz DJ. Bruising characteristics discriminated physical child abuse from accidental trauma. *Pediatrics,* 2010: 125(1); 67-74.
8. Pierce MC, Kaczor K, Lorenz DJ, Bertocci G, Fingarson AK, Makoroff K, Berger RP. Validation of a clinical decision rule to predict abuse in young children based on bruising characteristics. *JAMA Netw Open.* 2021; 4(4):e215832.
9. Kleinman PK, ed. Diagnostic Imaging of Child Abuse. 3rd ed. Cambridge University Press, 2015.
10. ACS Trauma Quality Programs Best Practice Guidelines for Trauma Center Recognition of Child Abuse, Elder Abuse, and Intimate Partner Violence. [abuse\_guidelines.pdf (facs.org)](https://www.facs.org/media/o0wdimys/abuse_guidelines.pdf) November, 2019.
11. Burg B, Dougherty M, Snyder K, Shanghvi D, Naiditch J, et al. Dell Children’s Medical Center, Evidence-based Outcome Center, “Evaluation for Occult Injury Guideline”. February, 2022.
12. Rosen NG, Escobar MA, Brown CV, et al. Child physical abuse trauma evaluation and management: A Western Trauma Association and Pediatric Trauma Society critical decisions algorithm. *J Trauma Acute Care Surg*.2021; 90(4): 641-651.Western Trauma Association and Pediatric Trauma Society complete algorithm for the evaluation and management of children with Child Physical Abuse (CPA) trauma.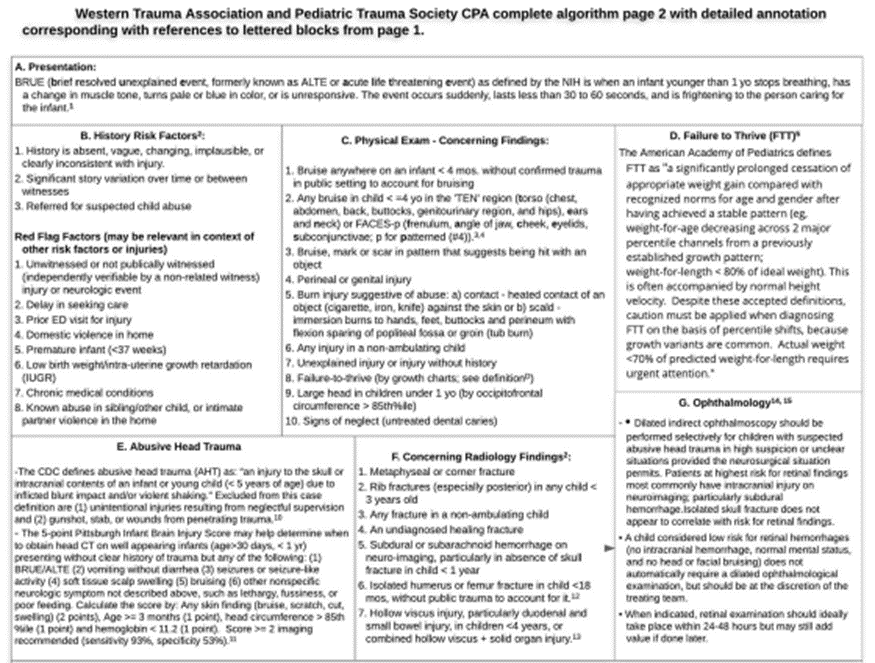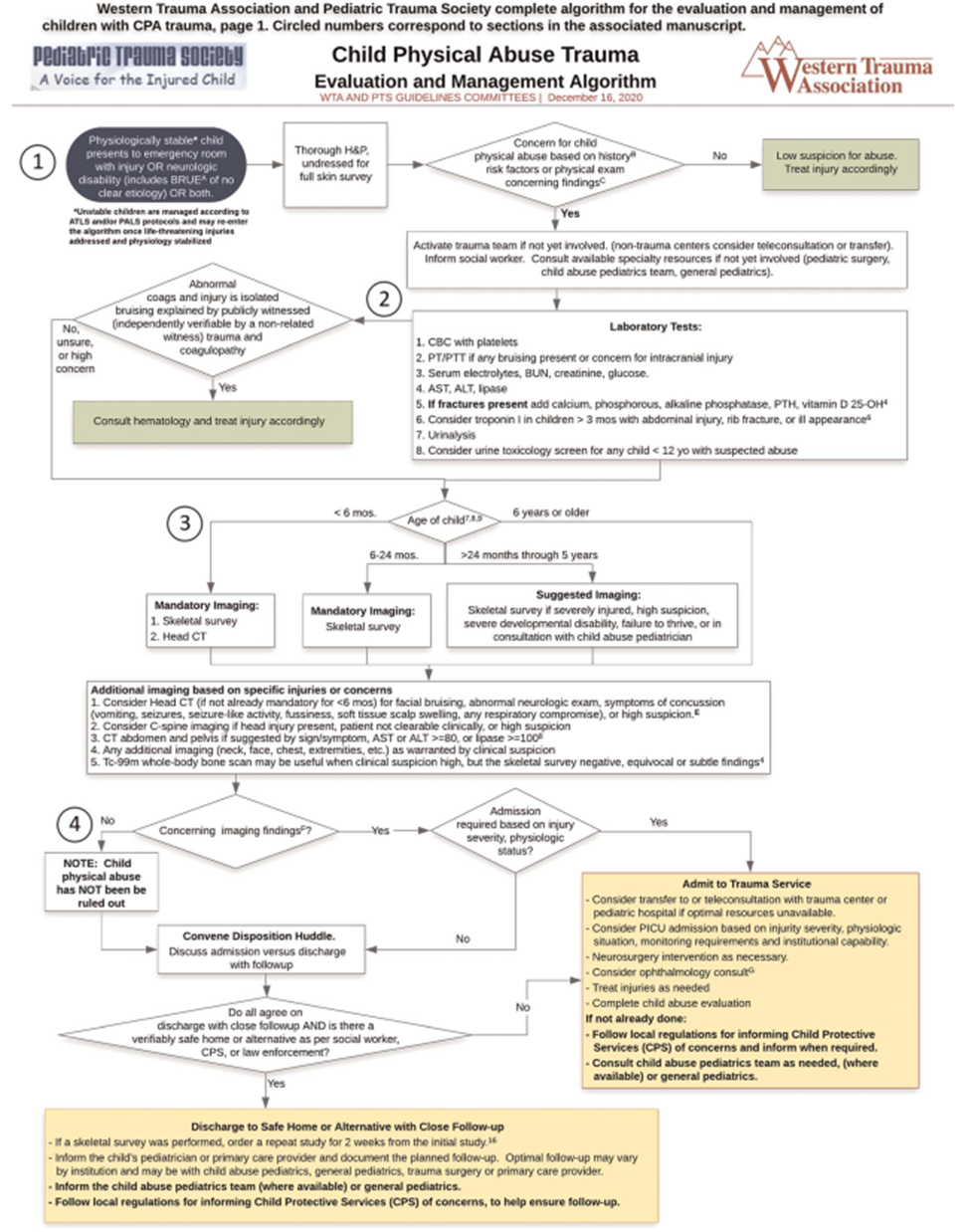
# Guidelines for Imaging the Pediatric Trauma Patient
**Purpose:**
These guidelines are meant to help guide the provider’s decision-making regarding imaging of the pediatric trauma patient during the initial trauma evaluation.
**Background/Definitions:**
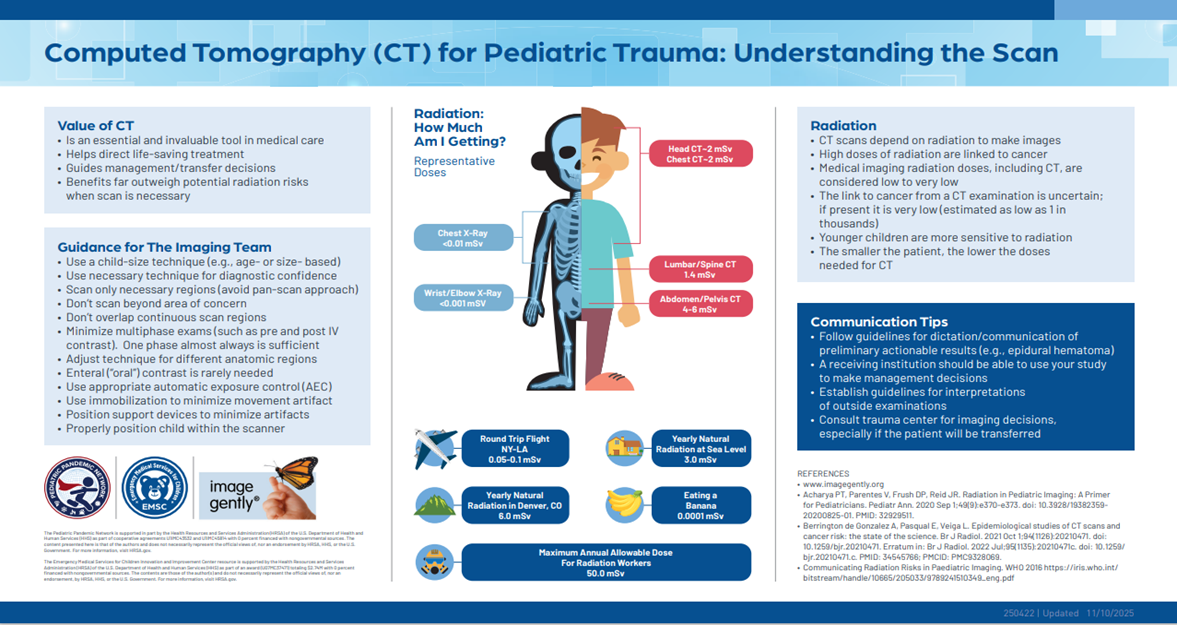
There is considerable agreement that diagnostic imaging, particularly with computed tomography (CT), results in significant radiation exposure in children. In addition, while the precise implications of this radiation exposure have not been defined, there is consensus that it is associated with a low, but real, increase in the long-term development of fatal malignancy. Children are particularly sensitive to the effects of radiation given their small size (increase dose per unit area) and the long latent times between exposure and the resultant cancer. Exposure to diagnostic radiation in children has increased dramatically in recent years with increasing use of CT. The primary indication for these scans is for the evaluation of trauma and appendicitis. Both the American Academy of Pediatrics and the American Pediatric Surgical Association have recently published statements encouraging their members to adhere to the ALARA principle, “As Low as Reasonably Achievable,” when obtaining imaging in pediatric patients (1, 2).While the use of CT to diagnosis injuries in children has been increasing, there is a growing body of literature to suggest that CT is not required for routine evaluation resulting in the creation of several prediction rules to help guide the physician on what type and when imaging might be indicated to adequately assess the pediatric trauma patient. In light of this evidence, we recommend adherence to the ALARA principle when imaging pediatric trauma patients. Specifically, we recommend:
1. Avoidance of the use of protocols which automatically result in the performance of multiple CT scans (i.e. head, cervical spine, chest, and abdomen and pelvis) in pediatric patients.
2. Avoid further CT imaging once the decision to transfer to definitive care is made, unless the accepting institution specifically requests a scan prior to transfer.
3. All CT scans on children should be performed using “pediatric” weight-based dose-reduction protocols per Nebraska Medicine radiology procedures.
4. Accepting institution should avoid repeating scans unnecessarily and when possible utilize alternative imaging strategies.
**Guideline Inclusion Criteria:**
- Pediatric trauma patients less than 19 years of age.
**Guideline Exclusion Criteria:**
- Patients 19 years of age and older.
**Practice Recommendations for Management:**
**Initial Assessment:**
- Pediatric trauma patients should be assessed per ATLS guidelines on arrival to ED.
- - Chest x-ray and pelvis x-ray should be used as adjuncts to the primary survey as indicated by patient’s clinical status and mechanism of injury.
- - Can consider not obtaining chest x-ray in low-grade mechanisms of injury if patient is able to be observed following injury.
- Chest x-ray should be obtained in setting of high-grade mechanism of injury, abnormal physiology and/or intubation.
- Routine use of eFAST in pediatric trauma patients is not supported by literature due to decreased sensitivity and specificity in pediatric patients when compared to adults. eFAST, however, may still be beneficial in decision making for certain clinical scenarios (i.e. hypotensive, blunt trauma patient) and should be utilized at the discretion of the trauma provider.
- The use of a skilled child life specialist to help minimize the injured child’s fear and anxiety can markedly reduce the amount of sedation required during the initial assessment and subsequent imaging. Their liberal use is recommended when available.
- If the child requires sedation to complete the trauma assessment or imaging, experienced pediatric personnel with credentials to administer sedation are recommended.
**Additional Imaging:**
- **Pediatric Head Imaging**
- - Decision to obtain CT imaging of the head in pediatric trauma patients should be based on PECARN (Pediatric Emergency Care Applied Research Network) criteria which are as follows:
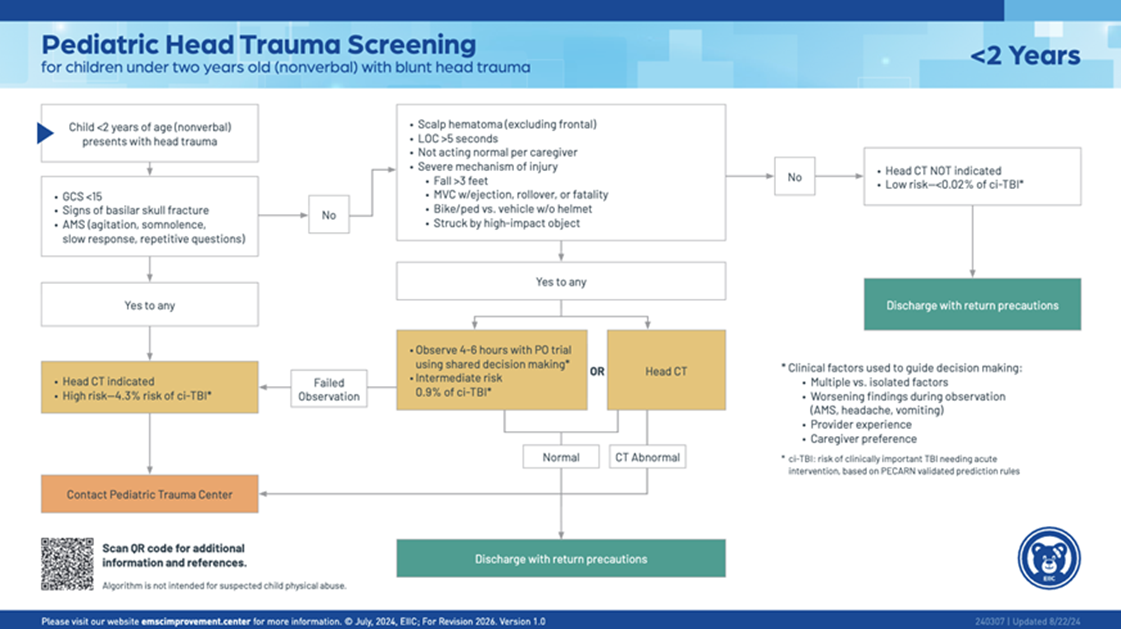
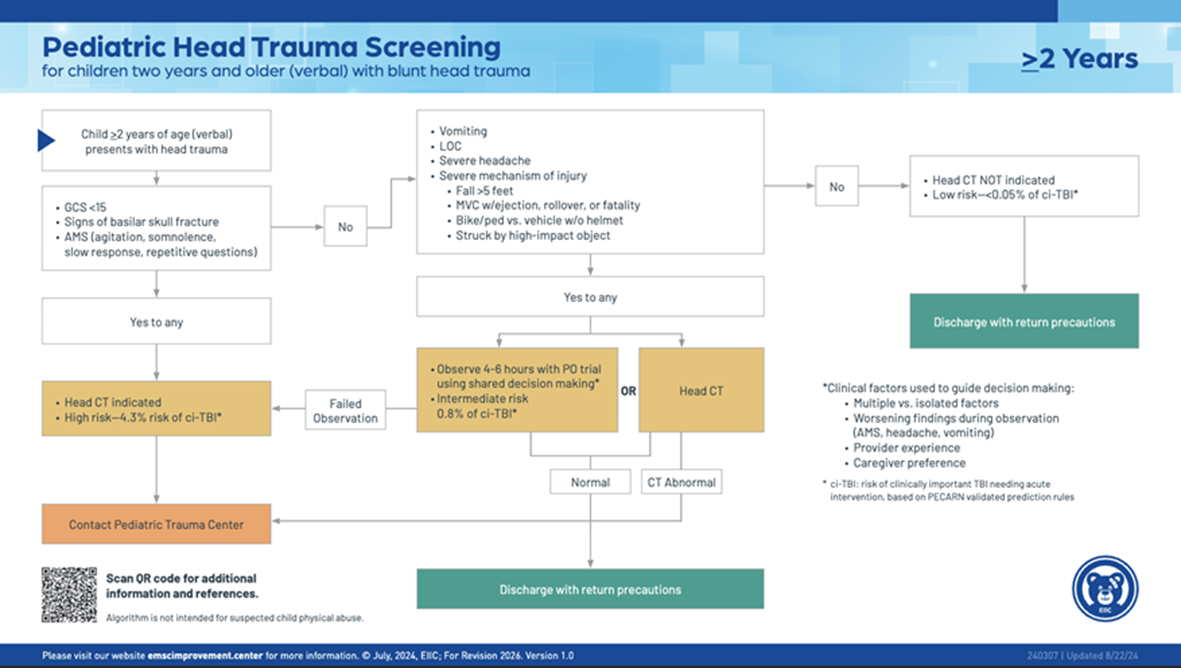
- - - Routine repeat CT head is not recommended but should be considered if there is a decline in GCS/worsening neurological exam, in sedated patients who cannot be evaluated, or at discretion of neurosurgical team.
- **Pediatric Cervical Spine Imaging:**
- - The asymptomatic child with a reliable normal exam does not require imaging to clear the cervical spine, regardless of mechanism.
- The overall incidence of c-spine injury in children is low (<1%). However, may be seen in up to 30% of pediatric TBI patients and overall incidence of approximately 15% in non-accidental trauma.
- Injury is most difficult to assess in the 2-5 year age group.
- The risk for a higher anatomical injury is greater the younger the child.
- - Younger children are more likely to suffer ligamentous injury than fracture.
- Canadian C-spine Rule (CCR) and NEXUS criteria are standard for adults but are not sensitive or specific enough to be used for children <10 years of age.
- Decision to obtain c-spine imaging in pediatric patients following blunt trauma should be based on PECARN criteria or the AAST scoring system for patients less than 3 years of age.
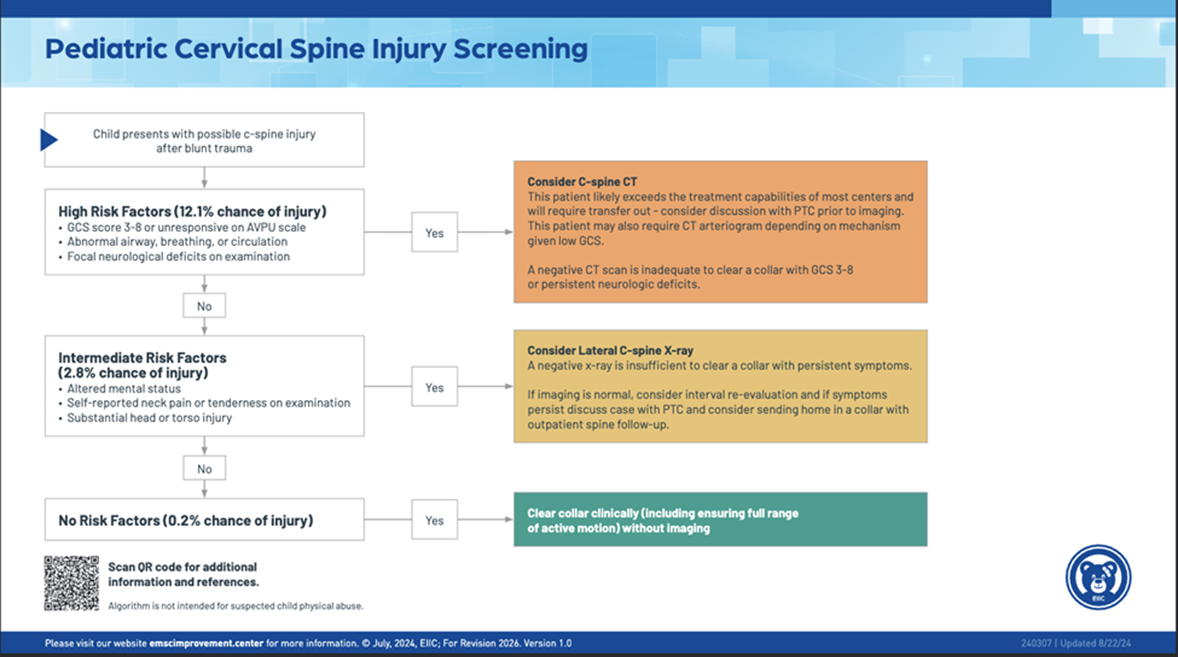
- - PECARN Criteria:
- - Consider CT c-spine in the following:
- - GCS 3-8 or AVPU =U
- Abnormal airway, breathing, or circulation
- Focal neurologic deficits
- Consider c-spine x-rays in the following:
- - GCS 9-14, AVPU=V or P, or other signs of altered mental status
- Self-reported neck pain or neck tenderness on examination
- “substantial” head or torso injury (“substantial” injuries defined as warranting inpatient observation or surgical intervention such as skull fracture, pneumothorax, solid organ injury, spine fracture, pelvic fracture)
- If none of the above listed risk factors are present, then consider clinical clearance.
[](https://paths.trauma.ai/uploads/images/gallery/2024-09/image.png)
- - - - - AAST scoring system for patients less than 3 years:
- - Criteria examined:
- - GCS<14 = 3 points
- GCS (eye criterion) =1 = 2 points
- Motor vehicle crash (MVC), fall from height>10ft, intentional injury as mechanism of injury = 2 points
- Age 24-36 months = 1 point
- Scoring:
- - 0-1 = no imaging
- 2-4 = imaging a clinician discretion
- 5-8 = imaging (CT c-spine) recommended
- Non-contrast CT c-spine is generally the recommended study of choice for evaluating the cervical spine, as the sensitivity and specificity of c-spine x-rays is inconsistent.
- Consider MRI c-spine if neck pain is out of proportion to CT results or concerned for spinal cord injury or ligamentous injury.
- SCIWORA—(spinal cord injury without radiographic abnormality) term used to descript neurologic deficit in the absence of findings on plain radiographs or CT scan. MRI is recommended next, but up to 40% of affected patients do not have an injury detected by MRI.
- **Screening for Blunt Cerebrovascular Injury (BCVI) in pediatric trauma patients**
- - Routine use of CTA neck for BCVI screening in pediatric trauma patients should be avoided due to the associated radiation exposure and low incidence of BCVI in the population.
- The McGovern Score should be utilized to help determine if a patient should undergo CTA neck for screening of BCVI.
- - A score of ≥3 points is high-risk for BCVI and CTA neck should be performed. 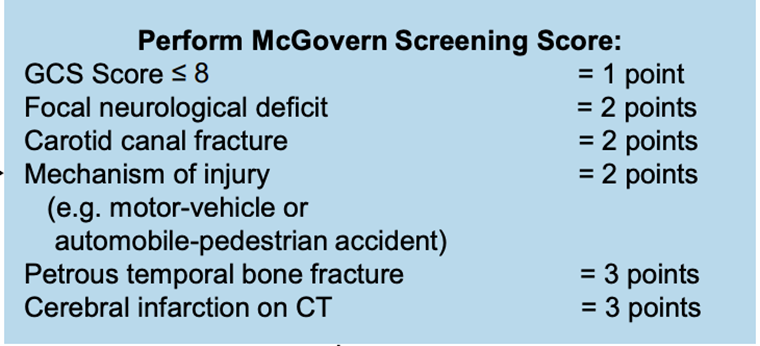
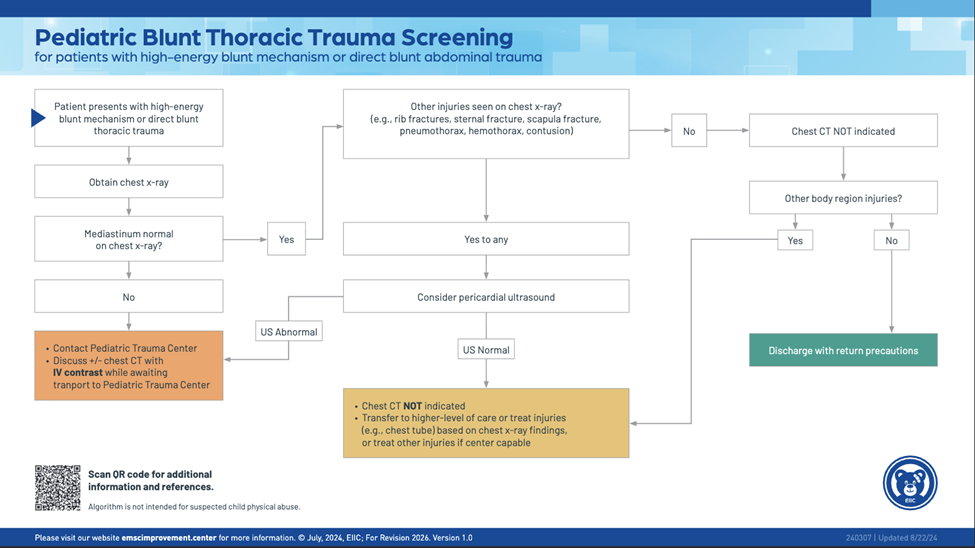
- **Pediatric Chest Imaging**
- - X-ray
- - Chest x-ray is recommended in the initial evaluation of all pediatric trauma patients, regardless of age, in the presence of abnormal physiology, high-grade mechanism of injury, or intubation.
- Ultrasound
- - a pericardial US should be considered if the chest x-ray reveals a normal mediastinum, but other injuries (e.g. rib fractures, sternal fracture, scapula fracture, pneumothorax or contusion) are present.
- CT scan
- - CT chest should be used selectively in the evaluation of pediatric trauma patients to reduce unnecessary imaging.
- - A CT chest is reported to have no impact on management of the pediatric trauma patient with absent or minor abnormalities on chest x-ray (ex. simple pneumothorax, simple hemothorax, pulmonary contusion, or isolated rib fractures).
- if indicated, a CT chest should be obtained with IV contrast.
- A CT chest is recommended for children with abnormal mediastinal contour of an age-appropriate shaped chest, more significant abnormalities on chest x-ray or an abnormal pericardial US.
- **Pediatric Abdominal Imaging**
- - Ultrasound
- - Routine use of eFAST in pediatric trauma patients is not supported by literature due to decreased sensitivity and specificity in pediatric patients when compared to adults.
- eFAST, however, may still be beneficial in decision making for certain clinical scenarios and IS RECOMMENDED for the assessment of pediatric trauma patients presenting in shock (i.e. hypotensive), when CT is not available or feasible or at the discretion of the trauma provider.
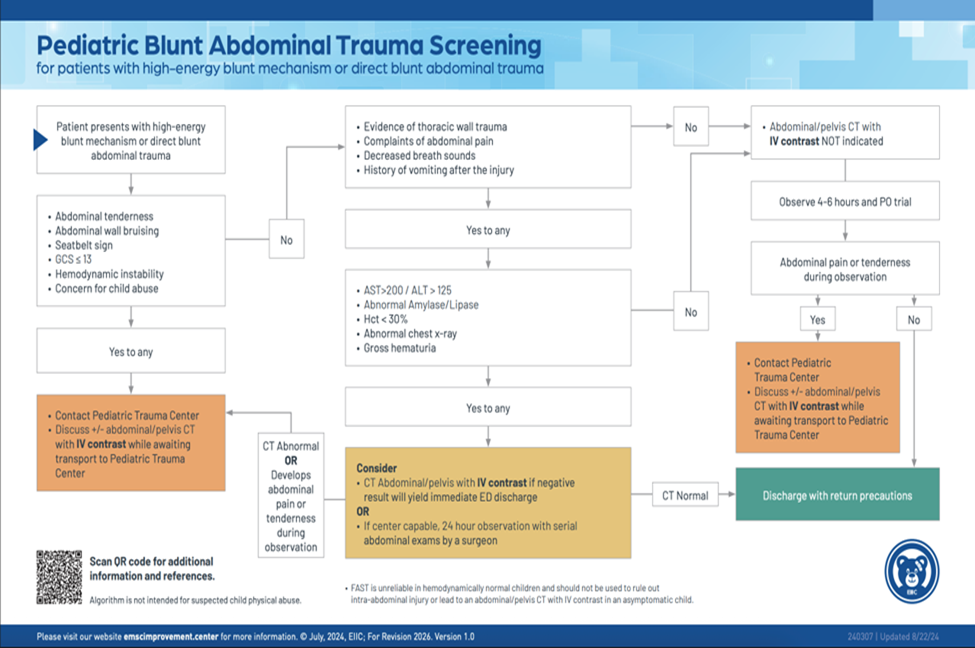
- CT scan
- - The PECARN Prediction Rule or the Streck Criteria should be applied to pediatric patients presenting after high-energy blunt mechanism or with blunt abdominal trauma to help determine when CT scans are indicated
- CT abdomen/pelvis should be used selectively in the evaluation of pediatric trauma patients to reduce unnecessary imaging.
- If indicated, a CT abdomen/pelvis should be obtained with IV contrast in at least 2 phases (typically arterial and venous) to help identify and distinguish active hemorrhage.
- - The portal venous phase is optimal for evaluation of visceral parenchyma.
- delayed excretory phase images are essential for the evaluation of genitourinary trauma (e.g. renal collecting system or bladder injuries) and should be considered in the setting of gross hematuria or microscopic hematuria with hypotension.
- oral contrast is typically not indicated unless there is concern for duodenal injury.
- **Pediatric Thoracic and Lumbar Spine imaging**
- - Routine imaging of the spine based on mechanism of injury alone is generally not recommended.
- AP and lateral x-rays are indicated for physical examination findings or symptoms.
- - Obesity/body habitus and other factors may affect the quality of the x-rays.
- If a patient is undergoing CT chest, abdomen or pelvis, obtain thoracic and lumbar spine reconstructions.
- If patient has a neurologic deficit/abnormality, consider obtaining MRI for evaluation of the spine.
- **Pediatric Orthopedic Injury Imaging**
- - Plain x-rays of the injured area are the standard for initial assessment of possible orthopedic injury.
- - Use “rule of twos” when ordering x-rays:
- - Two views – at least obtain an AP and lateral view of the injured limb/area
- Two joints—consider obtaining x-rays of the joints above and below the site of injury to rule out an potential associated fracture or dislocation.
- Two limbs—after consultation with orthopedic surgery, a request for x-rays of the injured and non-injured limb is made to aid in evaluation/diagnosis of certain injuries.
- Two times—pre- and post- reduction x-rays are needed to assess the adequacy of any fracture or dislocation manipulation or reduction.
- CT is not indicated for the routine evaluation of many orthopedic injuries and should only be ordered following consultation with orthopedic surgery when needed for pre-operative planning of complicated fractures.
- MRI of affected area can be helpful in identifying occult injuries or further evaluating certain injuries. MRI is rarely indicated in the acute setting and should be considered following consultation with orthopedic surgery.
- **Imaging for pediatric extremity vascular injury**
- - Extremity vascular imaging in the pediatric population is similar to that of adults.
- CTA of affected extremity remains the gold standard to evaluate for vascular injury in extremity trauma in the hemodynamically stable patient without hard signs of vascular injury.
- - Vasospasm cannot be reliably diagnosed by CTA and may require catheter angiography.
- Hard signs of vascular injury
- - Bruit/thrill
- Active/pulsatile hemorrhage
- Pulsatile/expanding hematoma
- Signs of limb ischemia and/or compartment syndrome including the 5 “P’s” (pallor, paresthesia, pulse deficit, paralysis, and pain on passive extension)
- Diminished or absent pulses
- Soft signs of vascular injury
- - Hypotension or shock
- Neurologic deficit
- Nonexpanding/nonpulsatile hematoma
- Proximity of wound to major vascular structures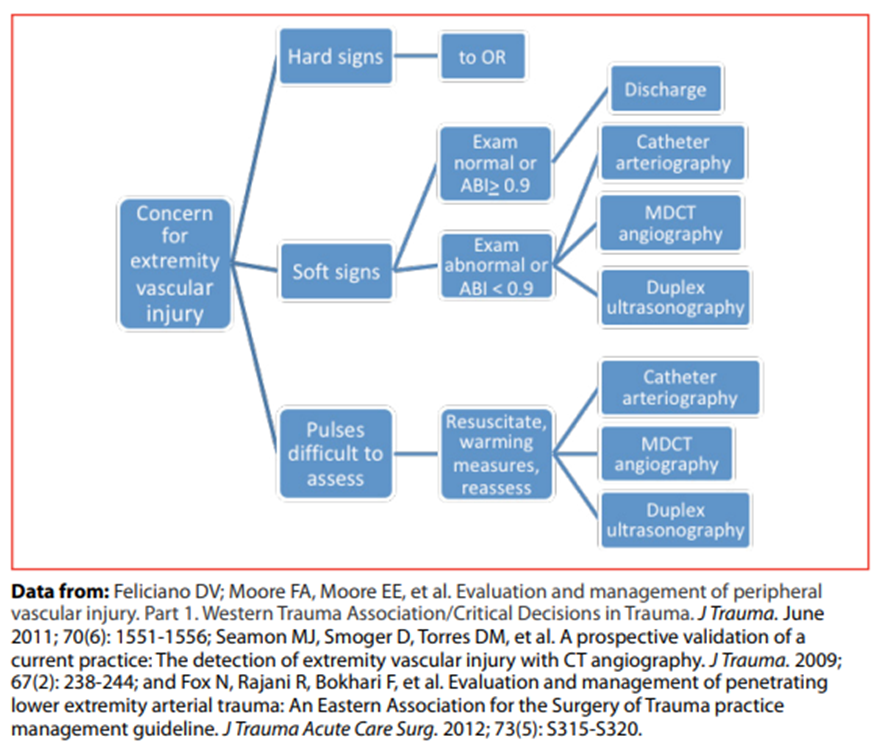
**Outcome Measures and Guideline Adherence:**
- All pediatric trauma patients will be reviewed for imaging obtained and adherence to above stated imaging guidelines. Deviations from guidelines will be investigated further for with intervention and education as needed when trends or opportunities for improvement are identified.
- Adherence to guidelines will be reported in the Pediatric Performance Improvement Process (PIPs) meeting.
**Key Contributors:**
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Abby Josef, MD | Division of Acute Care Surgery, Faculty | Reviewer
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Coordinator | Co-Author
- Megan Samland, DNP, APRN-NP, AGACNP-BC, FNP-BC | Division of Acute Care Surgery, APP | Co-Author
**Last updated:**
·February, 2026
**References:**
1. Brody, Frush, Huda, Brent, and the Section of Radiology, “Radiation Risk to Children from Computed Tomography,” Pediatrics 120: 677-682, 2007.
2. Rice, Frush, Farmer, Waldhausen, and the APSA Education Committee, “Review of radiation risks from computed tomography: essential for the pediatric surgeon. J Pediatr Surg 42: 603-7, 2007.
3. Kupperman N, Holmes JF, Dayan PS, et al. Pediatric Emergency Care Applied Research Network (PECARN). Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet. 2009; 374(9696): 1160-70.
4. Pieretti-Vanmarcke R, Velmahos GC, Nance ML, et al Clinical clearance of the cervical spine in blunt trauma patients younger than 3 years: A multi-center study of the American Association for the Surgery of Trauma. *J Trauma* 2009; 67(3):543-550.
5. Markel, Kumar, Koontz, et al. The utility of computed tomography as a screening tool for the evaluation of pediatric blunt chest trauma. J Trauma 67:23-28, 2009.
6. Singh, Kalra, Moore, et al. Dose reduction and compliance with pediatric CT protocols adapted to patient size, clinical indication, and number of prior studies. Radiology 252: 200-208, 2009.
7. Chwals, Robinson, Sivit, et al. Computed tomography before transfer to a level I pediatric trauma center risks duplication with associated increased radiation exposure. J Pediatr Surg 43 2268-2272, 2008.
8. ACS Trauma Quality Programs Best Practice Guidelines in Imaging. [imaging\_guidelines.pdf (facs.org)](https://www.facs.org/media/oxdjw5zj/imaging_guidelines.pdf) October, 2018.
9. Holmes JF, Yen K, Ugaldge IT, et al. PECARN prediction rules for CT imaging of children presenting to the emergency department with blunt abdominal or minor head trauma: a multicentre prospective validation study. *Lancet Child Adolesc Health.* 2024 May; 8(5):339-347.
10. Leonard JC, Harding M, Cook LJ, et a.l PECARN prediction rule for cervical spine imaging of children presenting to the emergency department with blunt trauma: a multicentre prospective observational study. *Lancet Child Adolesc Health.* 2024 Jul; 8(7):482-490.
11. Chung S, Mikrogianakis A, Wales PW, et al. Trauma Association of Canada Pediatric Subcommittee National Pediatric Cervical Spine Evaluation Pathway: Consensus guidelines. *J Trauma*. 2011; 70(4):873-884.
12. Nigrovic LE, Rogers AJ, Adelgais KM, et al. Pediatric Emergency Care Applied Research Network (PECARN) Cervical Spine Study Group. Utility of plain radiographs in detecting traumatic injuries of the cervical spine in children. *Pediatr Emerg Care*. 2012; 28(5):426-432.
13. Herbert JP, Venkataraman SS, Turkmani AH, Zhu L, et al. Pediatric blunt cerebrovascular injury: The McGovern screening score. *J Neurosurg Pediatr.* 2018; 21(6):639-649.
14. Venkataraman SS, Herbert JP, Ravindra VM, et al. Multi-center validation of the McGovern Pediatric Blunt Cerebrovascular Injury Screening Score. *J Neurotrauma*. 2023; 40(13-14):1451-1458.
15. Emergency Medical Services for Children Innovation and Improvement Center (EIIC) (2025). *EIIC: Best Practices in Pediatric Trauma Imaging*.https://emscimprovement.center/education-and-resources/peak/multisystem-trauma/imaging/
# Indications to Consult Pediatric Critical Care
#### Purpose
The trauma service frequently encounters critically injured pediatric patients (aged 18 years or less) that require admission to the pediatric ICU for resuscitation and management of injuries. To optimize outcomes, assistance in resuscitation and care of these critically injured pediatric trauma patients is often enhanced by the involvement of pediatric critical care medicine (PCCM). As a result, collaboration between the trauma and pediatric critical care services is essential and the following guidelines are meant to outline when pediatric critical care should be consulted to assist in the management and care of injured children requiring admission to the pediatric ICU.
#### Indications to Consult Pediatric Critical Care Medicine (PCCM)
1. All injured children requiring ICU or progressive care level admission, age 12 years and younger.
2. Injured children with pre-existing or congenital conditions that would benefit from the expertise of a pediatric intensivist, age 18 and under.
3. At the admitting trauma attending’s discretion.
#### Consulting Pediatric Critical Care Medicine (PCCM)
1. The trauma service will contact the PCCM provider listed “on call” on PerfectServe for consultation/handoff if the patient is being admitted/transferred to the PICU.
2. The trauma service will need to place an “Inpatient consult to pediatric critical care” consult order. Reason for consultation can be “medical co-management.”
1. - Use the **PEDATRIC TRAUMA ADMISSION – 12 years old and younger** order set. Select **“Inpatient consult to Pediatric Critical Care Medicine”** order under Physician Consults-Academic section followed by also selecting the associated order **“Notify physician/provider—Please contact Pediatric Critical Care Medicine regarding invasive/non-invasive respiratory support, sedation, CRRT settings, and adjustment of existing pressors. For ALL OTHER CONCERNS, contact the TRAUMA TEAM”** located in the Vital Signs/Notify Physician section.
3. Direct verbal communication should occur between the trauma and PCCM providers caring for the patient on admission/transfer to the pediatric ICU and with any change in patient status/condition.
#### General Requirements
1. When consulted, PCCM will assist with management until the patient is transferred out “critical care” status. At which time, a pediatric co-management consult should be considered.
2. **The trauma service will serve as the patient’s PRIMARY team**. As a result, the trauma surgeon/team must be kept informed of and concur with all major therapeutic and management decisions when care is being provided by the PCCM team. 
1. 1. - A minimum of daily communication between the trauma and PCCM teams should occur to discuss patient care plans.
- The trauma and PCCM teams will round daily on patients and write daily progress notes.
- If it is determined that the trauma team should no longer be the primary team on a patient (i.e. transferring to another pediatric service), the trauma service will be responsible for finding an accepting primary service, placing the necessary orders for transfer, communicating plans for transfer with PCCM team, and documentation of transfer to include patient’s current status/injury management/follow-up/transfer details/etc. (“sign off” note)
3. If PCCM is consulted, adult critical care surgery (CCS) services will **not** be involved in the care of the pediatric trauma patient unless specifically requested by the trauma service.
#### Responsibilities of Pediatric Critical Care Medicine (PCCM) Team
1. Management of vasopressors and other continuous infusions (i.e. sedation, analgesia, etc.).
2. Management of ventilator.
3. Placement and management of central venous catheters, PICC line, and arterial lines (in collaboration with trauma team).
4. Medication management, review, and reconciliation.
- - Including guidance for dosing by weight and age (in collaboration with pediatric pharmacy).
- including electrolyte replacement, glucose management, seizure management, and antibiotics (in collaboration with the trauma team).
5. Ensuring adjunctive modalities are used for delirium prevention, pain control, and refusal of PO/medications by child or parent.
6. Discrepancies between orders (in collaboration with the trauma team).
7. Management of pre-existing/chronic medical conditions.
8. Responding to all acute decline and decompensation events.
- - In addition, will contact the trauma team to provide updates on significant events or status changes.
9. Screening and interventions for non-accidental trauma, as deemed necessary (in collaboration with the trauma team).
10. Counseling and guidance of injury prevention, including causative injury and other preventative measures, to patient and family.
11. Communication with primary pediatrician/PCP.
12. Facilitate pediatric specialist consults and follow-up (in collaboration with the trauma team).
13. Assist the trauma team with facilitating discharge to inpatient rehabilitation.
#### Responsibilities of the Trauma Service
1. Contacting all consult services based on patient injuries and clinical findings.
2. Coordinating and managing all procedural and operative interventions.
3. Admission and discharge orders and notes.
4. Diet/nutrition management and associated orders.
5. Activity orders.
6. Wound care management and associated orders.
7. Imaging and lab orders.
8. Determination of need, orders, and management of DVT prophylaxis (in collaboration with PCCM and pharmacy).
9. Blood product transfusions (in collaboration with PCCM).
10. Management of new medical issues (in collaboration with PCCM).
11. Chest tube placement and management (in collaboration with PCCM).
#### References
1. Rosen, N. G., Escobar Jr, M. A., Brown, C. V., Moore, E. E., Sava, J. A., Peck, K., ... & Martin, M. J. (2021). Child physical abuse trauma evaluation and management: a Western Trauma Association and Pediatric Trauma Society critical decisions algorithm. *Journal of Trauma and Acute Care Surgery*, *90*(4), 641-651.
2. American College of Surgeons Trauma Quality Improvement Program (2019). ACS Trauma Quality Program Best Practices Guidelines for Trauma Center Recognition of Child Abuse, Elder Abuse, and Intimate Parner Violence. Release November 2019. Available at [https://www.facs.org/media/o0wdimys/abuse\_guidelines.pdf](https://www.facs.org/media/o0wdimys/abuse_guidelines.pdf). Accessed March 20, 2024.
#### Authors
1. Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principal Author
2. Megan Samland, DNP | Division of Acute Care Surgery, Advanced Practice Provider | Principal Author
3. Eleanor Gradidge, MD | Department of Pediatrics, Division of Pediatric Critical Care, Faculty | Principal Author
Last Updated: June, 2024
# Indications to Consult Pediatric Co-Management Team for Pediatric Trauma Patients
#### **Purpose:**
The trauma service frequently admits and cares for injured children (aged 18 years or less). To optimize outcomes and inpatient care, assistance in the management and care of these injured pediatric trauma patients is enhanced by involvement of the pediatric co-management team. As a result, collaboration between the trauma and pediatric co-management team is essential. These guidelines outline when pediatric co-management team should be consulted to assist in the management and care of pediatric trauma patients.
#### **Indications to Consult Pediatric Co-Management**
1. injured children age 18 and under upon admission or transfer to a pediatric floor
#### **Consulting Pediatric Co-Management**
1. The trauma service will contact the Pediatric Co-Management provider listed “on call” on PerfectServe under “General Pediatric and Neonatology Academic Service TNMC” (choose general pediatric inpatient) for consultation/handoff if the patient is being admitted/transferred to the pediatric floor.
2. The trauma service will need to place an “Inpatient consult to pediatrics academic” consult order in EPIC. Reason for consultation can be “medical co-management.”
3. Direct verbal communication should occur between the trauma and pediatric co-management providers caring for the patient on admission/transfer to the pediatric floor and with any change in patient status/condition. The pediatric resident may be reached at 402-619-9157.
#### **General requirements:**
1. When consulted, Pediatric Co-Management will assist with management of pediatric trauma patients once they are considered floor status.
2. **The trauma service will serve as the patient’s PRIMARY team**. As a result, the trauma surgeon/team must be kept informed of and concur with all major therapeutic and management recommendations by the pediatric co-management team. 
- - - A minimum of daily communication between the trauma and pediatric co-management teams should occur to discuss patient care plans.
- - - The pediatric co-management provider will contact the trauma team daily and as needed via PerfectServe (“Trauma Academic Service) with recommendations after seeing the patient.
- The trauma team will round daily on patients and write daily progress notes. Following the initial consultation and screenings, the pediatric co-management team will evaluate pediatric patients daily and write progress notes as needed to reflect any updates or changes in recommendations.
- If it is determined that the trauma team should no longer be the primary team on a patient (i.e. transferring to another pediatric service), the trauma service will be responsible for finding an accepting primary service, placing the necessary orders for transfer, communicating plans for transfer with the pediatric co-management team, and documentation of transfer to include patient’s current status/injury management/follow-up/transfer details/etc. (“sign off” note)
#### **Responsibilities of pediatric co-management team**
1. Medication management, review, and reconciliation.
- - Including guidance for dosing by weight and age (in collaboration with pediatric pharmacy).
2. management of pre-existing/chronic medical conditions
3. Responding to all acute decline and decompensation events.
1. - In addition, will contact the trauma team to provide updates on significant events or status changes.
4. discrepancies between orders (in collaboration with the trauma team)
5. communication with primary pediatrician/PCP
6. substance and alcohol misuse screening with interventions as needed
7. screening and interventions as determined necessary for non-accidental trauma (in conjunction with the trauma team)
8. Counseling and guidance of injury prevention, including causative injury and other preventative measures, to patient and family.
9. Facilitate pediatric specialist consults and follow-up (in collaboration with the trauma team).
10. Assist the trauma team with facilitating discharge to inpatient rehabilitation.
11. Mental health screening
#### **Responsibilities of Trauma Service**
1. Contacting all consult services based on patient injuries and clinical findings.
2. Coordinating and managing procedural/operative interventions
3. Admission and discharge orders and notes
4. Diet/nutrition management and associated orders
5. Blood product transfusions
6. Electrolyte replacement, glucose management, bowel regimen orders and other routine daily cares (in collaboration with pediatric co-management and pharmacy)
7. Activity orders
8. Pain Management (in collaboration with pediatric co-management)
9. Wound care management and associated orders.
10. Imaging and lab orders
11. Determination of need, orders, and management of DVT prophylaxis (in collaboration with Pediatric co-management and pharmacy)
12. Management of new medical issues (in collaboration with Pediatric co-management)
13. Line and tube placement and management (central lines, chest tubes, etc.)
**Authors:**
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principal Author
- Katherine MacKrell, MD | Department of Pediatrics, Division of Hospital Medicine, Faculty | Principal Author
**Last Revised**
July, 2024
# Managment of Open Pediatric Orthopedic Fractures
**Purpose:**
To provide guidance on the management of open orthopedic fractures in pediatric trauma patients.
**Background/definitions:**
An open fracture is a fracture in which there is an open wound or break in the skin near the site of the broken bone. Most often, this wound is caused by a fragment of bone breaking through the skin at the time of injury. The fractured bone is exposed to contamination from the external environment and is susceptible to infection.
**Guideline Inclusion Criteria:**
- Injured children and adolescents 18 years and younger with confirmed or suspected open fractures.
**Guideline Exclusion Criteria:**
- Injured patients >18 years old.
**Practice Recommendations for Management:**
1. Orthopedic surgery should be consulted on all open pediatric orthopedic fractures.
2. Classification is made according to the Gustillo classification of open fractures. This classification is made at the time of operative debridement.
- - Type I: open fracture with wound <1cm long; clean
- Type II: open fracture with wound >1cm long; soft tissue damage, avulsions, tissue flap, minimal to moderate contamination
- Type III: extensive soft tissue damage, open segmental fracture; significant contamination.
- - Type IIIA: soft tissue coverage is adequate (primary closure/delayed primary closure or skin graft)
- Type IIIB: periosteal stripping, bone exposure, massive contamination; will require either rotational flap or free flap for coverage
- Type IIIC: open fracture with arterial injury requiring repair to salvage limb
3. Antibiotics should be initiated within 60 minutes of patient arrival:
- - Type I and II:
- - Preferred: Cefazolin 30 mg/kg IV now and q8hr x 3 total doses (not to exceed 2000mg/dose)
- Severe cephalosporin allergy: Clindamycin 10mg/kg IV now and q8hr x 3 doses (not to exceed 900 mg/dose)
- Known MRSA colonization: add vancomycin 15mg/kg IV q12hr
- Duration of prophylaxis: 24 hours
- Type III
- - No gross contamination:
- - Preferred: Cefazolin 30 mg/kg IV now and q8hr x 3 total doses (not to exceed 2000mg/dose)
- Severe cephalosporin allergy: Clindamycin 10mg/kg IV now and q8hr x 3 doses (not to exceed 900 mg/dose)
- Known MRSA colonization: add vancomycin 15mg/kg IV q12hr
- Duration of prophylaxis: 48 hours or 24 hours after wound closure, whichever is shorter
- Contamination with soil or fecal material
- - Preferred: ceftriaxone 75mg/kg IV now and q24hr (not to exceed 2000mg/dose) **AND** metronidazole 15mg/kg IV now and q8hr (not to exceed 500 mg/dose)
- Severe cephalosporin allergy: Clindamycin 10mg/kg IV now and q8hr (not to exceed 900 mg/dose)
- Known MRSA colonization: add vancomycin 15mg/kg IV q12hr
- Duration of prophylaxis: 48 hours after wound closure
- Consider orthopedic infectious disease consult
- Contamination with standing water:
- - a.Preferred: Piperacillin/tazobactam 100mg/kg IV q8hr over 4 hours (not to exceed 4.5g IV)
- b.Penicillin allergy: Clindamycin 10mg/kg IV now and q8hr (not to exceed 900 mg/dose)**AND** metronidazole 15mg/kg IV now and q8hr (not to exceed 500 mg/dose)
- c.Known MRSA colonization: add vancomycin 15mg/kg IV q12hr
- d.Duration of prophylaxis: 48 hours after wound closure
- e.Consider orthopedic infectious disease consult
- Variances in dosing within 5mg/kg are acceptable based upon dosage rounding in Pharmacy.
- If there are any drug-related questions (drug choice, dosing, allergies, alternative options), discuss with pharmacy.
4. Tetanus toxoid should be administered if the patient had an incomplete immunization, if it has been >1- years since the last booster, or if immunization history is unknown or unclear. Tetanus immunoglobulin should be administered if patient has never been immunized and present with wound that is felt to be tetanus prone.
5. Patients with open fractures should be taken to the operating room for irrigation and debridement within 24 hours of initial presentation whenever possible. Patients with severe fractures associated with gross wound contamination should be brought to the operating room as soon as clinically feasible based on the patient’s condition and resources available. All patients will receive an initial bedside irrigation with removal of obvious foreign contamination and application of clean dressings to wounds in the emergency department.
6. Whenever possible, skin defects overlying open fractures should be closed at the time of in initial debridement in the operating room.
7. Soft tissue coverage should be completed within seven days of injury whenever possible for open fractures associated with wounds requiring skin grafting or soft tissue transfers.
8. Skeletally mature patients between 14 and 18 years of age may follow the adult open fracture protocol (PRO 12 Management of Open Fractures).
**Outcome Measures and Guideline Adherence:**
- Orthopedic response times for urgent consults, time to antibiotic administration, time to OR for debridement and time to wound coverage for open fractures will be monitored through the pediatric trauma performance improvement process.
**Related Policies:**
- PRO 12 Management of Open Fractures
- Antibiotic Prophylaxis in Open Fractures
**Key Contributors:**
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Manager | Co-Author
- Sara Putnam, MD, ABOS MD| Department of Orthopedic Surgery, Faculty | Reviewer
**Last updated:**
·July, 2024
**References:**
1. Davis M, Della Rocca G, Brenner M, et al. (2022) ACS TQIP Best Practices in the Management of Orthopedic Trauma. [Best Practices in the Management of Orthopedic Trauma | ACS TQIP (facs.org)](https://www.facs.org/media/mkbnhqtw/ortho_guidelines.pdf)
# Management of Pediatric Long Bone Fractures
**Purpose:**
To provide guidance on the management of long bone fractures in pediatric trauma patients.
**Background/definitions:**
A long bone is defined as any bone of the extremity that has a length greater than the width to include:
- Femur
- Tibia/fibula
- Humerus
- Radius/Ulna
Management of pediatric long-bone injuries is highly dependent upon skeletal maturity. In general, the pediatric orthopedic surgery attendings manage long bone injuries in patients with immature skeletons (i.e. open growth plates), while adult orthopedic surgery attendings manage injuries in patients with mature skeletons (i.e. closed growth plates). The general cutoff is 16 years of age, although the final decision for management of an individual patient is at the discretion of the orthopedic surgery attending on-call, and can involve a discussion between the on-call attending surgeons for pediatric and adult orthopedic surgery. Discretion of casting versus operative care of these injuries is at the discretion of the orthopedic attending on call.
**Guideline Inclusion Criteria:**
- Injured children and adolescents 18 years and younger with a long bone fracture
**Guideline Exclusion Criteria:**
- Injured patients >18 years old.
**Practice Recommendations for Management:**
1. Long bone fractures should be stabilized as early as possible.
2. Orthopedic surgery will be consulted on all pediatric long bone fractures.
3. In the absence of polytrauma, definitive long bone stabilization of femoral shaft fractures should occur within 24 hours of arrival.
- - Other long bone fractures should undergo early fixation as deemed appropriate by the orthopedic team.
4. For the polytrauma patient, medical stability and concomitant injuries should be assessed prior to internal fixation. A damage control approach should be taken and the internal fixation of long bone fractures should be delayed until the patient is adequately resuscitated.
1. - Internal fixation should occur within 48 hours of arrival in the polytrauma patient and after initial stabilization.
- External fixation devices should be utilized until internal fixation is appropriate.
5. Children younger than thirty-six months with a diaphyseal femur fracture should be evaluated for child abuse.
1. - For children younger than one year of age, the Child Advocacy Team (CAT) should be consulted for evaluation.
- For children above one year of age, consultation of the Child Advocacy Team (CAT) will be at the discretion of the pediatric orthopedic and trauma surgery attendings on call.
6. Management of pediatric diaphyseal femur fractures will be at the discretion of the pediatric orthopedic attending on call, with reference to the 2020 AAOS Clinical Practice Guideline ([pdffcpg.pdf (aaos.org)](https://www.aaos.org/globalassets/quality-and-practice-resources/pdff/pdffcpg.pdf)) on this injury.
7. Transfer of pediatric long bone fractures to Children’s Nebraska for definitive management may be considered in the absence of polytrauma and requires approval from the trauma surgery attending on call.
**Outcome Measures and Guideline Adherence:**
1. Orthopedic response times for urgent consults as well as time to OR for definitive management of long bone fractures will be monitored through the pediatric trauma performance improvement process.
2. All transfers to Children’s Nebraska will be reviewed through the pediatric trauma performance improvement process.
**Key Contributors:**
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Manager | Co-Author
- Sara Putnam, MD, ABOS MD| Department of Orthopedic Surgery, Faculty | Reviewer
**Last updated:**
·July, 2024
**References:**
1. Davis M, Della Rocca G, Brenner M, et al. (2022) ACS TQIP Best Practices in the Management of Orthopedic Trauma. [Best Practices in the Management of Orthopedic Trauma | ACS TQIP (facs.org)](https://www.facs.org/media/mkbnhqtw/ortho_guidelines.pdf)
2. American Academy of Orthopedic Surgeons. (2022). Treatment of Pediatric Diaphyseal Femur Fractures. [https://www.aaos.org/globalassets/quality-and-practice-resources/pdff/pdffcpg.pdf](https://www.aaos.org/globalassets/quality-and-practice-resources/pdff/pdffcpg.pdf)
# Management of Pediatric Pelvic Fractures
**Purpose:**
Provide guidance on the initial evaluation and management of pediatric trauma patients with pelvic fractures.
**Background:**
Injures to the pelvis range from benign to life threatening. They include pelvic ring fractures, acetabular fractures, avulsion, and iliac wing fractures. The pelvis in children consists of high cartilaginous volume with greater elasticity at the sacroiliac joints and symphysis. Therefore, the pediatric pelvis is less prone to fracture and more able to dissipate a relatively large amount of energy. Most pediatric pelvic injuries are due to high-energy blunt trauma, which increases the likelihood of concomitant injuries to the head, chest, abdomen, and extremities.
**Guideline Inclusion Criteria:**
- Pediatric trauma patients age 18 years and younger with confirmed or suspected pelvic fractures
**Guideline Exclusion Criteria:**
- Trauma patients >18 years of age
**Practice Management Guidelines:**
1. Orthopedic surgery will evaluate the patient within 30 minutes of consultation request; interventional radiology (IR) should be notified if there is any consideration for embolization.
2. Initial evaluation
- - Patient should be assessed and managed per ATLS guidelines. Physical examination should be performed by the trauma team in conjunction with the orthopedic team to specifically include:
- - Urologic/vaginal exam
- Perineum exam
- Rectal exam
- An AP pelvis x-ray will be obtained in the trauma bay. The decision to forego AP pelvis x-ray and proceed directly to CT imaging is at the discretion of the trauma surgery attending.
- Pediatric trauma patients that require pelvic stabilization via binder or sheet are limited to: unstable pelvic fracture and hemodynamically unstable patient
- - This includes patients who arrived hemodynamically unstable and have since stabilized.
- The pelvic binder or sheet should be placed at the level of the greater trochanters
- Patients who arrive to the trauma bay with a pelvic binder or stabilization sheet already in place should not have it removed until either AP pelvis x-ray is obtained to determine necessity, or unless directed by Orthopedic Surgery.
- - It is acceptable to briefly remove the binder or stabilization sheet for adequate patient assessment.
- CT scan of the pelvis, including reconstructions, are obtained to evaluate for associated injuries.
- Initial evaluation should include determination if a urinary catheter is necessary.
- - The Orthopedic Surgery team will include any recommendations for urinary catheterization in the consult note, and either Orthopedic Surgery or Trauma Surgery will place the order for urinary catheter in the electronic medical record.
- Timely urinary catheter insertion is essential. Any barriers to insertion should be promptly escalated to Orthopedic Surgery or Trauma Surgery.
- Questions related to permissible patient positioning during urinary catheter insertion should be directed to Orthopedic Surgery. If there are difficulties in obtaining proper positioning or if there is concern related to fractures as it relates to positioning, Orthopedic Surgery may be contacted for bedside assistance.
- Consider urology consult if there are concerns related to urethral injury or if urinary catheterization attempts are unsuccessful.
- External catheters, such as Pure Wick, are not an acceptable substitution and should not be utilized in acute pelvic fracture management.
- Mobile patients without activity restrictions may utilize a bedpan.
3. Management is based upon hemodynamic stability
1. - Ultimate decision for fracture treatment is determined by the Orthopedic Surgeon
- Volume resuscitation with appropriate blood products and maintenance of core temperature must be continued during all phases of resuscitation. Activation of Massive Transfusion Protocol (MTP) will be utilized as indicated per policy (PRO 09- Massive Transfusion in Trauma Guidelines). Blood products will be administered via rapid transfuser.
- For patients in a pelvic binder:
- - Repeat AP pelvic x-ray should be obtained to assess reduction
- Binder should not remain in placed for longer than 48 hours unless there are extenuating circumstances that prevent operative intervention.
- Skin checks should be performed by the orthopedic surgery service ever 12 hours while the binder is in place, with removal of the binder ever 24 hours for more thorough skin check (maintaining precautions to prevent movement of the pelvis).
- Skeletal traction may be placed at the discretion of the orthopedic surgery attending.
- For hemodynamically unstable patients despite adequate resuscitation and/or patients with evidence of contrast extravasation on CT imaging related to pelvic fractures, consider consultation of IR for possible angioembolization.
**Pediatric Pelvic Fracture Pathway**
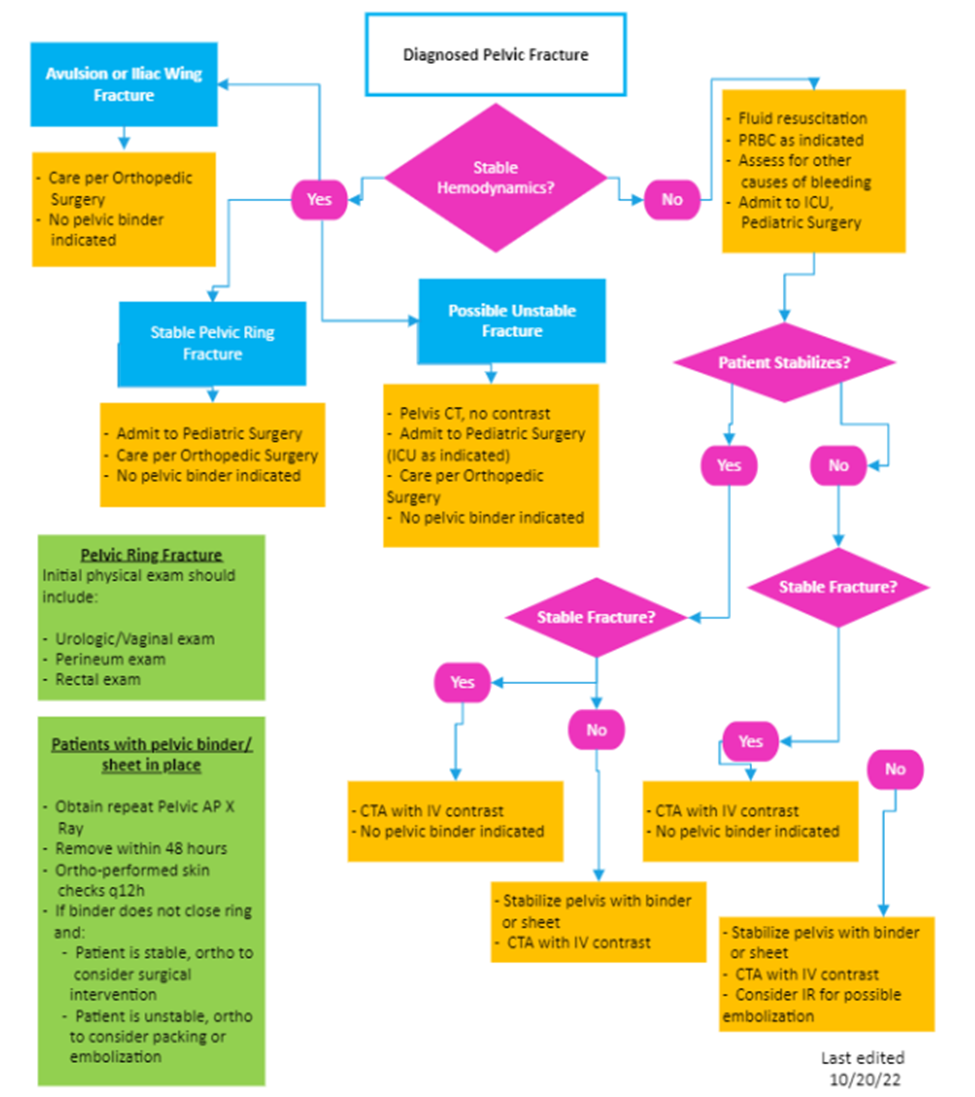
**Key Contributors:**
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Manager | Co-Author
- Sara Putnam, MD, ABOS MD| Department of Orthopedic Surgery, Faculty | Reviewer
**Last updated:**
·July, 2024
**References:**
1. Coccolini, F. (2017) Pelvic Trauma: WSES classification and guidelines, *World Journal of Emergency Surgery*, 12(5), 1-18.
2. DeFrancesco CJ, Sankar, WN. (2017). Traumatic pelvic fractures in children and adolescents. *Seminars in Pediatric Surgery*, 26(1), 27-35.
3. Hermans E, Cornelisse ST, Biert J, et al. (2017) Paediatric pelvic fractures, how do they differ from adults? *Journal of Children’s Orthopeadics,* 11, 49-56.
4. Swaid F, Peleg K, Alfici R, et al. (2017). A comparison study of pelvic fractures and associated abdominal injuries between pediatric and adult trauma patients. *Journal of Pediatric Surgery*, 52, 386-389.
5. Swenson SJ, Otsuka NY. (2022) *Pelvic Fractures*. Pediatric Orthopedic Society of North America. [Pelvic Fractures | Pediatric Orthopaedic Society of North America (POSNA)](https://posna.org/physician-education/study-guide/pelvic-fractures).
6. Tosounidis TH, Sheikh H, Giannoudis PV. (2015). Pelvic fractures in paediatric polytrauma patients: Classification, concomitant injuries and early mortality. *The Open Orthopedics Journal*. 9(1), 303-312. **
# Mental Health Screening and Intervention Guidelines for Pediatric Trauma Patients at Nebraska Medicine
Childhood traumatic stress happens when unexpected, violent, life-threatening, or devastating events overwhelm the ability to cope. The ACS reports that 20-30% of pediatric trauma patients report mental health symptoms and/or decreased quality of life following a traumatic event.
The purpose of this guideline is to identify pediatric trauma patients at high risk for post-trauma mental health adjustment disorder post-injury and facilitate brief interventions and appropriate referrals for longer term management and care.
1.A HEADSS assessment will be performed on all admitted pediatric trauma patients age 11 years and older by the pediatric co-management team once the patient reaches floor status.
2.Patients with a positive HEADSS assessment in the mental health categories AND/OR any pediatric patient experiencing the following traumatic events:
a.Neglect and psychological, physical, or sexual abuse.
b.Victim of community and school violence.
c.Victim of gun-related violence (intentional self-inflicted GSW or suicidal attempt will prompt child psychiatry consult)
d.Serious traumatic event causing life-threatening and devastating injuries (traumatic brain injury, spinal cord injury, loss of limb, mutilating/deforming injuries, etc)
e.Prolonged hospital stay (longer than 1 week)
f.Death of friend/family member in traumatic event
g.Care provider discretion.
These patients are identified as high risk for post-injury mental health disorder(s) will undergo additional screening using the ASC6/ASC3 screening tool derived from the Acute Stress Checklist (ASC-Kids) or consultation with behavioral health/child psychiatry.
[https://www.healthcaretoolbox.org/sites/default/files/2021-03/ASC-Kids%20English%20and%20Spanish%20with%20scoring%20info%20-%20all%20versions%20SAMPLE.pdf](https://www.healthcaretoolbox.org/sites/default/files/2021-03/ASC-Kids%20English%20and%20Spanish%20with%20scoring%20info%20-%20all%20versions%20SAMPLE.pdf)
3.Patients admitted following self-inflicted injury or suicide attempt as well as patients with suicidal or homicidal ideation will receive inpatient consultation with child psychiatry.
4.Patients who screen positive on the ASC6/ASC3 will receive one or more of the following intervention(s):
a.Consultation of child psychiatry for inpatient assessment of mental health concernsb.Referral to child psychiatry or psychology for outpatient assessment and management of mental health concerns
c.Notification of primary pediatrician of mental health concerns for assistance in longer term follow-up and/or outpatient mental health referrals as indicated
5.For patients who do not screen positive but have experienced one of the above traumatic events, the patient’s primary pediatrician should be notified with the recommendation to perform a repeat assessment of the patient’s mental health in 4-6 weeks time.
Documentation
The HEADDS, ASC6/ASC3 assessment (if performed), and interventions provided will be documented in a progress note by the pediatric co-management teams in the patient’s electronic medical record when consulted. For those patients remaining in the ICU for entire hospital course, mental health screening will be performed as indicated by the trauma service.
References:
1.American College of Surgeons. (2022, December). Best Practices Guidelines: Screening and Intervention for mental health disorders and substance use and misuse. [**https://www.facs.org/media/nrcj31ku/mental-health-guidelines.pdf**](https://www.facs.org/media/nrcj31ku/mental-health-guidelines.pdf)2.The Acute Stress Checklist (ASC-kids) (2016), [**https://www.healthcaretoolbox.org/acute-stress-checklist**](https://www.healthcaretoolbox.org/acute-stress-checklist)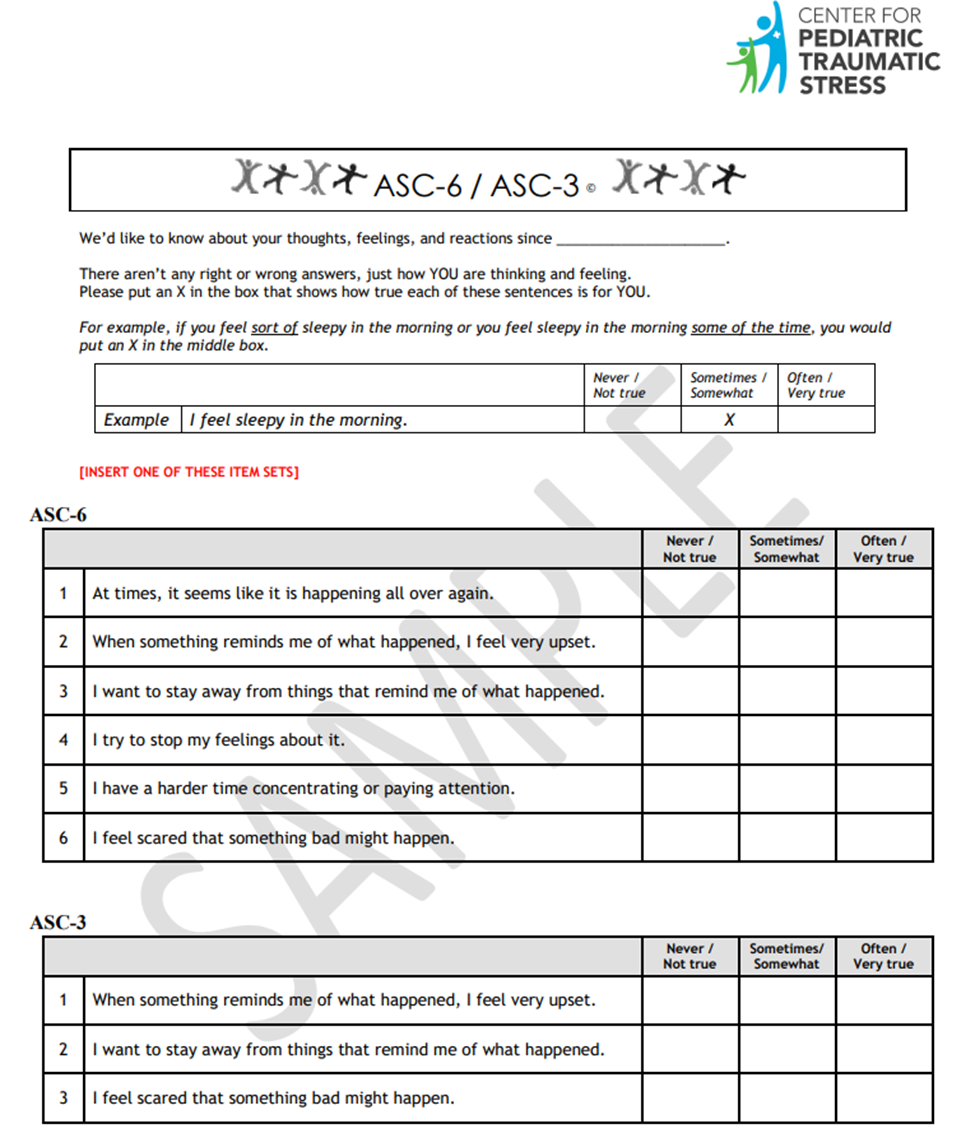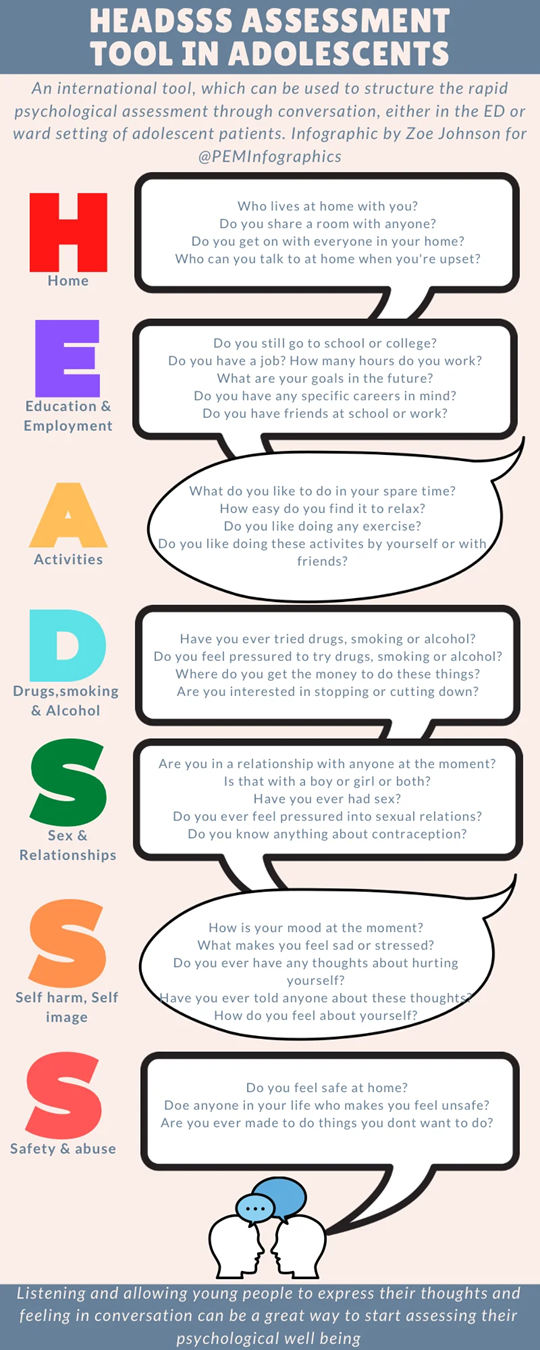
# Non-Surgical Service Admissions of Pediatric Trauma Patients at Nebraska Medicine
**SCOPE AND PURPOSE**
The document is applicable to pediatric patients (age <19) assessed and cared for at Nebraska Medicine.
**POLICY AND PROCEDURE STATEMENTS**
The pediatric trauma accreditation standards, as set forth by the American College of Surgeons, encourage all injured patients to be admitted to a surgical service. Children may be admitted to a pediatric general or subspecialty service when a medical diagnosis was initially made based on history and physical exam or for care of a pre-existing medical condition. In those rare instances, the following policy has been formulated to guide the management of an injured patient admitted to a non-surgical service.
1. When it is known that a physical injury has occurred, a Trauma Surgery consult must be obtained. Assessment and recommendations for care will be documented in the electronic medical record.
2. In conjunction with the admitting pediatrician, the trauma surgery attending will determine a plan of care that includes transfer to a surgical service when injury is the primary reason for admission. Concurrent care with pediatric critical care medicine (PCCM), pediatric co-management team or other pediatric specialists will continue during the child’s hospitalization. (See “Indications to consult Pediatric Critical Care Medicine for pediatric trauma patients” and “Indications to consult Pediatric Co-Management for pediatric trauma patients”)
3. All patients who are found to have physical injuries must be evaluated for rehabilitative and social work needs.
4. If suspicion of child abuse or neglect is identified, a referral to the Child Advocacy Team (CAT) and social work must occur promptly with subsequent additional work-up as indicated. (See “Evaluation and Management of Non-Accidental Trauma (NAT) in Children at Nebraska Medicine”)
5. All non-surgical service admissions (NSA) of injured patients will be reviewed through the pediatric trauma performance improvement process.
1. - NSA with trauma or other surgical consultations, with ISS≤9, or without other identified opportunities for improvement may be closed in primary review.
- NSA without trauma or other surgical consultation, with ISS>9, or with identified opportunities for improvement must at a minimum be reviewed by the Pediatric Trauma Medical Director in secondary review.**APPROVALS:**
Authorized:
Emily Cantrell, MD
Pediatric Trauma Program Medical Director
Approved:
Lora Hofstetter, MSN, RN, CCRN, C-NPTPediatric Trauma Program Manager
**DATE OF ORIGIN AND REVIEWS**
Date of Origin: 8/2024
Date of Reviews:
**CONTENT REVIEWERS AND CONTRIBUTORS**
Pediatric Trauma Program Liaisons, Pediatrics
# Pediatric Needle Cricothyroidotomy
**Pediatric Needle Cricothyroidotomy**
**Supplies**
- (Kit located in 2nd Drawer of Pediatric Grey Trauma Cart—Trauma Bay 2)
- 16G Angiocath (IV catheter)
- Macrobore IV Extension Tubing
- End of a 3.0 ETT
- 10 ml Syringe with 5ml saline (for air placement confirmation)
**Process for Cannot Intubate and Cannot Ventilate (CICV) Emergency**
Video available here: [https://youtu.be/EEqXqiOyKr4?si=iF8VRp-n3FwuVeIB](https://youtu.be/EEqXqiOyKr4?si=iF8VRp-n3FwuVeIB)
1. Identify landmarks and stabilize the larynx with non-dominant hand
2. Access the cricothyroidotomy membrane with a 16G angiocath, aim in the caudad direction
3. Connect syringe with saline and pull-back to confirm placement by air aspiration
4. If placement is confirmed, connect macrobore tubing to catheter and then place 3.0 ETT end on tubing (See picture).
5. Connect to a pressure limiting bag or a jet ventilation device
6. Breaths should be delivered over 1 second and allowing for 2 second exhalation
7. Observe for complications such as: subcutaneous emphysema, hemorrhage, hypoventilation, equipment failure, catheter kink, & false placement.

**Additional Resources:**
- [https://www.paediatricemergencies.com/intubationcourse/course-manual/cricothyroidotomy/](https://www.paediatricemergencies.com/intubationcourse/course-manual/cricothyroidotomy/)
- [https://medicine.uiowa.edu/iowaprotocols/needle-cricothyroidotomy](https://medicine.uiowa.edu/iowaprotocols/needle-cricothyroidotomy)
*Please contact Dr. Emily Cantrell, Pediatric Trauma Medical Director, or Lora Hofstetter, Pediatric Trauma Program Coordinator for questions and additional training.*
# Pediatric Transport Contact Information
#### Critical Pediatric Trauma Patient Transfer Requests
##### **Please be prepared with the following information:**
- Provider's name requesting transport and call back number
- Patient's name, age, DOB, and weight
- Chief complaint/diagnosis and present conditions
- Medical history and allergies, if known
- Current vitals and ABCs
- Treatment, medications started, and IV access
**If requesting transport to Children’s Nebraska:**
·*Children’s Nebraska Transport **855-850-5437***
oAsk for assistance in coordinating a transport to Children’s Nebraska for (state the need) i.e. Trauma, PICU, Orthopedics, Neurology, etc.**If Children’s Nebraska Transport team is unavailable:**·*LifeNet or StarCare (AirMethods programs)**844-359-9111***
oAsk for assistance in coordinating transport of a patient to Children’s NebraskaoThis will get you to an AirMethods Team that is closest.
**If requesting transport of a patient to outside Omaha:**
·*Children’s Nebraska Transport **855-850-5437***
oAsk for assistance in coordinating transport of a patient from Nebraska Medicine to \[Destination\]oYou will be connected to a team member to triage call.·*Children’s Mercy**800-466-3729***
oAsk for assistance in coordinating transport of a patient from Nebraska Medicine to \[Destination\]oCommunication specialists will connect you to the appropriate physician or team to coordinate transport.
**If Specialized Pediatric Transport teams are unavailable:**
·*LifeNet or StarCare (AirMethods)**844-359-9111***
oAsk for assistance in coordinating transport of a patient from Nebraska Medicine to \[Destination\]oThis will get you to an AirMethods Team that is closet with the appropriate asset.
**Alternate Resource:**
·*MercyOne (Sioux City, IA)**800-247-1911***
oSame process as LifeNet\*\*Air/Ground transport may be dependent on program regulations, weather, & team availability. For the safety of the team & patient, never pressure a team to change a decision based on decline for weather or comfort.
# Contact Information for Pediatric Trauma Patients
**Common Consults for Traumatic Injuries: **
- Cardiothoracic Surgery
- - - - PerfectServe: Cardiac Surgery Academic Service TNMC
- FACE (ENT, OMFS, Plastics)
- - - - PerfectServe: Facial Trauma Unassigned TNMC
- HAND (Plastics, Ortho)
- - - - PerfectServe: Hand—TNMC (Hand Trauma and Consults – Ortho, Plastics)
- Neurosurgery
- - - - PerfectServe: Neurosurgery Academic Service TNMC
- OB-GYN
- - - - PerfectServe: Obstetrics and Gynecology Academic Service TNMC
- Ophthalmology
- - - - PerfectServe: Ophthalmology Academic Service TNMC
- Orthopedic surgery
- - - - PerfectServe: Orthopedic Academic Service TNMC
- Pediatric Surgery
- - - - Call Children’s Nebraska Access Center at 1-855-850-KIDS (5437) and request to be put in contact with provider on call for specific service.
- Please utilize as first to call in pediatric trauma patients <15 years of age for assistance in general surgical injuries with the exception of emergent complex hepatobiliary injuries.
- Transplant/Hepatobiliary Surgery
- - - - PerfectServe: Transplant – Liver & Bowel TNMC
- Spine (Ortho, NSGY)
- - - - M/W/F/Sun—
- - PerfectServe: Neurosurgery Academic Service TNMC
- T/Th/Sat—Orthopedic Spine Service
- - PerfectServe: Orthopedic Academic Service TNMC
- Urology
- - - - PerfectServe: Urology Academic Service (Genitourinary-GU)
- Vascular Surgery
- - - - PerfectServe: Vascular Surgery Academic Service TNMC
\*\*\*In general, pediatric specialists will manage injuries in pediatric trauma patients <15 years of age with some variability between service lines and attendings. Pediatric surgery should be utilized for patients <15 years of age for general traumatic injuries. In patients 15 years and older, adult general surgery subspecialties (MIS, CRS, surgical oncology) may be consulted for second opinions/area expertise if needed but may defer consultation to pediatric surgery in certain circumstances (i.e. congenital issues, complex/prior pediatric surgery history, etc). Transplant/Hepatobiliary Surgery should be considered for the first call in the setting of emergent complex traumatic hepatobiliary injuries.\*\*\*
\*\*\*Pediatric attendings will be contacted by his/her respective resident. If there are questions or uncertainty involving the case, the trauma attending should reach out and discuss case with the on-call attending for that specific specialty\*\*\*
\*\*\*Decision to engage pediatric orthopedic specialists will be based on injury, skeletal maturity and discretion of orthopedic attending on call. If orthopedic injury is isolated and transfer to Children’s hospital for management is requested, the trauma attending should be notified and agree to transfer. The pediatric TMD should also be notified of the plan to transfer a patient\*\*\*
**General Pediatric and Pediatric Subspecialties:**
- Pediatric Floor and ICU (main desk): 402-559-7400
- PICU/Pediatric Lead Nurse (Volte): 531-557-3201
- Melanie Anderson (nurse manager, PICU/general pediatrics): 402-885-0156
- Pediatric Anesthesia
- - - - Call anesthesia attending phone at (402)-650-5748 to discuss specific needs.
- - In house anesthesia (preferentially pediatric anesthesia when available) will handle emergent issues (intubations, starting emergent cases, etc.).
- Overnight, pediatric anesthesia is on home call and can be mobilized if needs arise.
- Pediatric Cardiology
- - - - PerfectServe: Children’s Hospital Cardiology
- PREFERRED: Call Children’s Nebraska Access Center at 1-855-850-KIDS (5437) and specify if you need consult, echo, EP, etc.
- Pediatric Co-Management
- - - - PerfectServe: General Pediatric and Neonatology Academic Service TNMC OR Pediatrics Nebraska Medicine à General Pediatric Inpatient
- Pediatric resident pager: 402-619-9157
- Pediatric Critical Care Medicine
- - - - PerfectServe: Pediatric Critical Care Medicine Academic Service TNMC
- PICU APP pager number: 402-888-7226; office located in pediatric unit
- Pediatric Endocrine
- - - - Not currently available. Hired new staff and working to find out when they will provide consult support again.
- Pediatric Gastroenterology
- - - - PerfectServe: Pediatric Gastroenterology Academic Service TNMC (Pedi GI)
- Physically present on the pediatric unit daily, M-F at 10:30am and Sat-Sun at 9am.
- Pediatric Hematology-Oncology
- - - - PerfectServe: Pediatric Hematology Oncology Academic Service TNMC
- Pediatric Infectious Disease
- - - - PerfectServe: Pediatric Infectious Disease Academic Service TNMC (Pedi ID)
- Pediatric Nephrology
- - - - PerfectServe: Pediatric Nephrology Academic Service TNMC
- Pediatric Neurology
- - - - PerfectServe: Pediatric Neurology Academic Service TNMC
- Pediatric Palliative Care
- - - - Call Children’s Nebraska Access Center at 1-855-850-KIDS (5437) and request to be put in contact with provider on call for specific service.
- Pediatric PM&R
- - - - PerfectServe: PM&R – Physical Medicine and Rehabilitation TNMC
- Dr. Pierce and Dr. D’Angelo staff the pediatric patients at NM.
- Pediatric Pulmonology
- - - - Call Children's Nebraska Access Center at 1-855-850-KIDS (5437) and request to be put in contact with provider on call for specific service.
- Pediatric Psychiatry
- - - - PerfectServe: Psychiatry Academic Service TNMC à Is this regarding a child? à Inpatient Child Psychiatry
- Pediatric Surgery
- - - - Call Children’s Nebraska Access Center at 1-855-850-KIDS (5437) and request to be put in contact with provider on call for specific service.
\*\*\*\*\*If there is difficulty in contacting specific pediatric subspecialties or find that any of these numbers are incorrect/out of date, please contact Dr. Emily Cantrell (pediatric TMD) of Lora Hofstetter (pediatric trauma program coordinator) for additional assistance\*\*\*\*\*
Last updated: March, 2025
# Recommendations for Acute Pain Treatment and Procedural Pain and Sedation Management for Pediatric Patients
Common medical procedures used to assess and treat children can cause significant pain and distress. Before initiating any non-emergent procedure in pediatric trauma patients, please take a moment to try and optimize pain and sedation management. Below are two links with recommendations and suggestions on how to approach pain and sedation management in pediatric patients before procedures. Of note, NM does not have all of the recommended drugs/products available on formulary. Please discuss with pharmacy if there are any questions regarding drug choice and dosage prior to use.
1. [Pediatric Education and Advocacy (PEAK): Bottom Line Recommendations: Pain Treatment](https://media.emscimprovement.center/documents/EMS230601_PainBLRUpdate_230621v2.pdf)
2. [Pediatric Education and Advocacy Kit (PEAK): Bottom Line Recommendations: Procedural Pain ](https://emscimprovement.center/education-and-resources/peak/peak-pediatric-pain/bottom-line-recommendations-pediatric-procedural-pain/)
3. [Pediatric Education and Advocacy Kit (PEAK): Bottom Line Recommendations: Procedural Sedation](https://emscimprovement.center/education-and-resources/peak/procedural-sedation/sedation-recommendations/)
Date Created: March, 2025
# Pediatric Presence at Pediatric Trauma Activations
##### **Purpose:**
The trauma service frequently encounters critically injured pediatric patients that require pediatric specific resuscitation measures. To optimize patient outcomes and experiences, assistance in the initial resuscitation and care of these critically injured pediatric trauma patients is often enhanced by the presence and involvement of pediatric nursing and/or pediatric critical care provider. The following guidelines outline when pediatric nursing and providers will be present at pediatric trauma activations.
##### **Criteria for Pediatric Presence at Pediatric Trauma Activations:**
- When available, the pediatric critical care provider (APP and/or attending)will present to all FULL trauma activations in patients age 12 years and younger.
- For LIMITED activations or other pediatric trauma encounters in the ED, the presence of the pediatric critical care provider (APP and/or attending) may be requested on an as needed basis.
- - - - The pediatric ICU APP may be contacted via PerfectServe (Pediatric Critical Care Medicine Academic Service TNMC) or by paging 402-888-7226.
- The presence of the pediatric ICU (PICU)/pediatric lead nurse (or designee) may be requested for any pediatric trauma activation/encounter in the ED when pediatric specific skill set felt to be beneficial to case.
- - - - The PICU/Pediatric Lead Nurse may be contacted via Volte phone at 531-557-3201.
**\*\*\*Due to staffing and responsibilities in the pediatric ICU, the pediatric critical care provider and pediatric ICU lead nurse (or designee) may not always be immediately available to respond in person to activations. If the pediatric critical care provider and/or nurse are not present at a pediatric trauma activation and presence is needed, please contact at above listed numbers.\*\*\***
##### **Responsibilities:**
Responsibilities and involvement of pediatric nursing and pediatric critical care provider during the initial trauma resuscitation will be in collaboration with the trauma team and at the discretion of the trauma attending. Responsibilities include, but are not limited to, the following:
- Pediatric Nurse:
- - - - Assist in obtaining IV access
- Assist in nursing procedures (NG, OG, foley placement, etc)
- Assist in administration and titration of medications or IV fluids
- Assist in transfusion of blood products
- Pediatric Critical Care Provider:
- - - - Assistance with procedures (central lines, arterial lines, chest tubes, etc)
- Assistance with medication selection and dosage (in collaboration with pharmacy)
- Coordination and assistance with fluid and blood product resuscitation (in conjunction with trauma team)
- Assistance with ventilator management
- assistance in consultation of pediatric subspecialties
# Transferring Pediatric Trauma Patients to Children's Nebraska Emergency Department
**Process for Transferring Pediatric Trauma Patients to Children’s Nebraska Emergency Department**
As a level II pediatric trauma center, every effort should be made to care for pediatric trauma patients at Nebraska Medicine (NM). However, based on allocation of resources and specialty services, certain pediatric traumatic injuries may benefit from transfer to Children’s Nebraska. In general, these injuries include but are not limited to the following:
- Isolated orthopedic injury in skeletally immature children
- Orthopedic injury in skeletally immature children with minor additional injuries that do not require admission/monitoring
- Need for cardiopulmonary bypass or ECMO in children <15 yrs of age
Patients with multiple injuries, particularly those requiring active monitoring for risk of hemodynamic decompensation or need for rapid intervention, should stay at NM and be primarily admitted and managed by the trauma service with appropriate consulting services as indicated by injury/clinical status.
If transfer to Children’s Nebraska is deemed necessary, the following steps should be taken:
[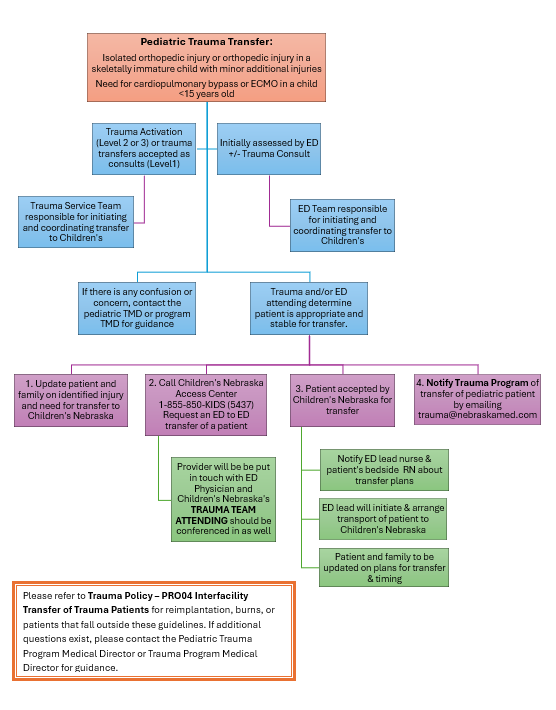](https://paths.trauma.ai/uploads/images/gallery/2026-02/image.png)