14. Care of the Trauma Patient
Information and miscellaneous things involved in caring for trauma patients throughout their acute hospitalization and beyond
- Advanced Care Planning and Palliative Care Consultation in Acute Care Surgery
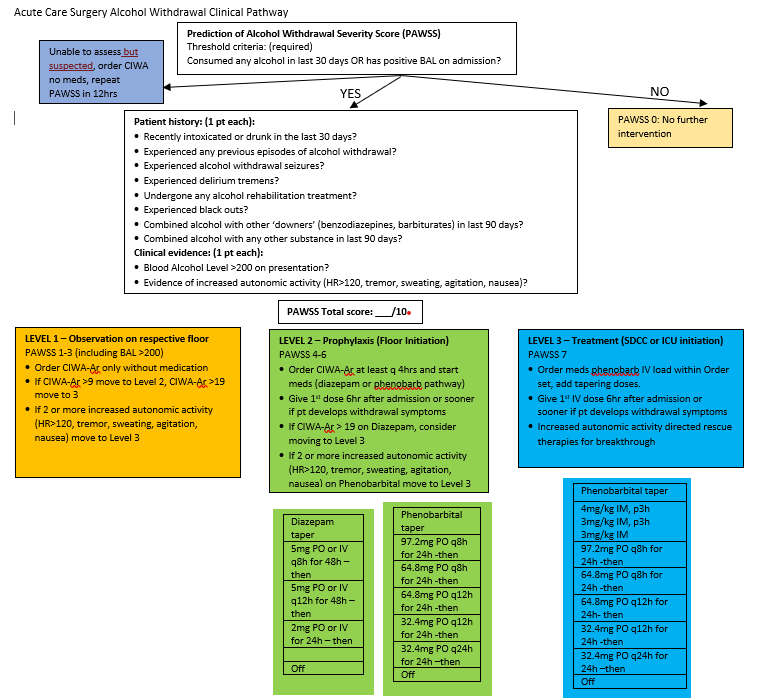
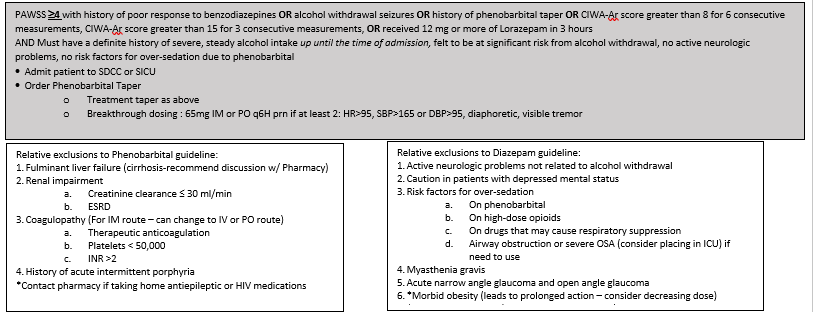
- Alcohol Withdrawal Pathway- PAWSS
- Assessing Capacity
- Evaluation and Management of Delirium
- Forensic Examiner Program Nebraska Medicine
- Summary – Law Enforcement Requests for Patient Information
Advanced Care Planning and Palliative Care Consultation in Acute Care Surgery
Purpose
· To engage injured or ill patient’s and/or families in discussions regarding goals of care and advanced care planning early and provide guidelines for Palliative Care consultation to assist in facilitating discussions surrounding goals of care and expectations of recovery following injury.
Background/Definitions
· Injury and illness is sudden, unpredictable and often life-altering. Patients and families display a variety of reactions after trauma and understanding the patient’s pre-existing psychosocial functioning is imperative to providing complete holistic care. Palliative care consultation can be a helpful service to patients by providing in depth discussion on goals of care related to prognosis and patient preferences, transitional planning, family support and symptom relief management.
Inclusion Criteria
- Age 55 years old or older
- ICU or SDCC admission (all ages)
- Multisystem injuries, specifically an upper and lower extremity injury
- >5 comorbidities
- Or provider discretion (consider things like homelessness, mental health, low social support, challenging injury)
- Should be done once in the inpatient setting- ie. Should not be done upon injury/in ER
Exclusion Criteria
- No absolutes
Diagnostic Evaluation
· Patients should be assessed per ATLS guidelines with labs, imaging, consults, and interventions as deemed necessary by trauma team to determine extent of injuries, co-morbid conditions, and general prognosis.
Similarly, emergency general surgery patients should be evaluated and managed as deemed appropriate for the current clinical status/diagnosis.
Practice Recommendations for Management
All acute care surgery patients: WITHIN 24 HRS OF ADMISSION
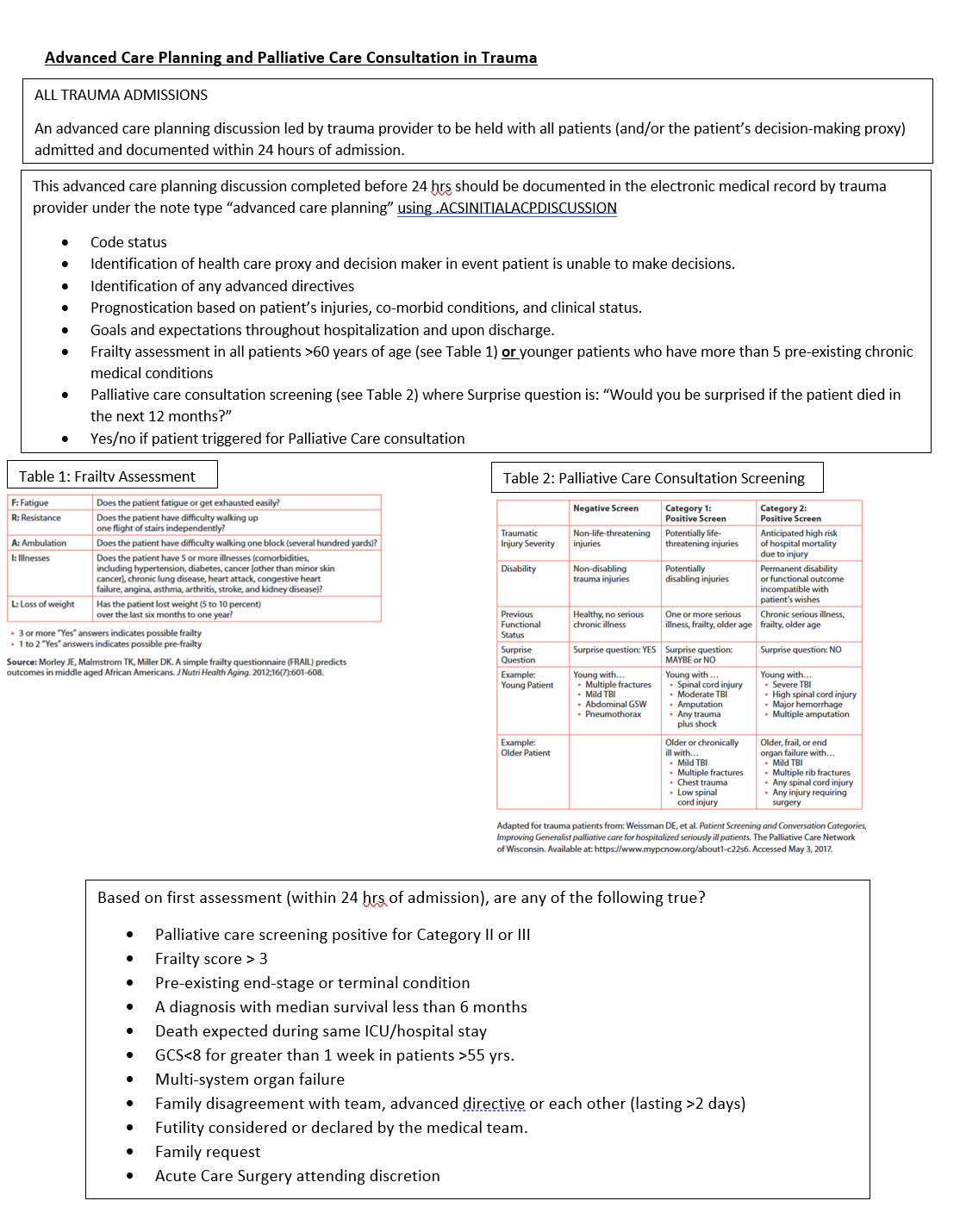
- An advanced care planning discussion should be held with patients (and/or the patient’s decision-making proxy) admitted to the trauma or emergency general surgery services within 24 hours of admission.
-
- For patient’s less than 19 years of age, discussions should occur with the patient’s legal guardian/parent.
-
- This initial advanced care planning discussion should be led by an acute care surgery service provider (physician or APP).
- The initial advanced care planning discussion should address the following:
-
- Code status
- Identification of health care proxy and decision maker in event patient is unable to make decisions.
- Identification of any advanced directives
- Prognostication based on patient’s injuries, co-morbid conditions, and clinical status.
- Goals and expectations throughout hospitalization and upon discharge.
- Frailty assessment in all patients >60 years of age (see Table 1) or in younger patients who have more than 5 pre-existing chronic medical conditions
-
Palliative care consultation screening (see Table 2)
- Palliative care consultation indicated/not indicated
-
- All advanced care planning discussions should be documented in the electronic medical record under the note type “advanced care planning”.
-
- Note template: .ACSACPINITIALACPDISCUSSION
-
-
Please use the ACP as an opportunity for a therapeutic discussion about the patient’s injuries and prognosis, and likely need for additional support. The goal should be to help explain the patient’s injuries, and guide expectations. If they are likely to need a facility, you can set the expectation that they may not go home, but give them encouragement to return home.
Triggers for Palliative Care Consultation based on initial advanced care planning discussion:
- Palliative care consultation should be considered if any of the following are present:
-
- Positive palliative care screen (Category 1 or 2)
- Frailty score greater than 3 (based on Frail Questionnaire, Table 1)
- Pre-existing end-stage or terminal condition
- A diagnosis with median survival less than 6 months
- Death expected during same ICU/hospital stay
- GCS<8 for greater than 1 week in patients >55 yrs.
- Multi-system organ failure
- Family disagreement with team, advanced directive or each other (lasting >2 days)
- Futility considered or declared by the medical team.
- Family request
- Acute Care Surgery attending discretion
-
- Palliative Care consultation ideally should occur early in patient's hospital course with a goal of assessing and managing the patient via "palliative care bundle" (see Table 3) within 72 hours of admission.
Triggers for Geriatrics Consultation for trauma patients based on initial advanced care planning discussion:
- All patients >75 years of age at admission
- Age 65-75, consider geriatric consultation if conditions listed below are present:
-
- dementia
- 10 or more home prescription medications
- 2 or more ED visits or inpatient admission in past 6 months
- not living independently or residents of nursing homes or assisted living facilities
- provider discretion
-
- in cases where patient's meet criteria for both Geriatrics and Palliative Care consultation:
-
- Request consultation of both services. Geriatrics will primarily assist with geriatric medical conditions, whereas Palliative Care will primarily assist with advance care planning/goals of care.
- This should occur with ongoing communication between Geriatric Medicine, Palliative Care and Trauma teams.
-
Triggers for Family Meeting WITHIN 72 HRS OF ADMISSION
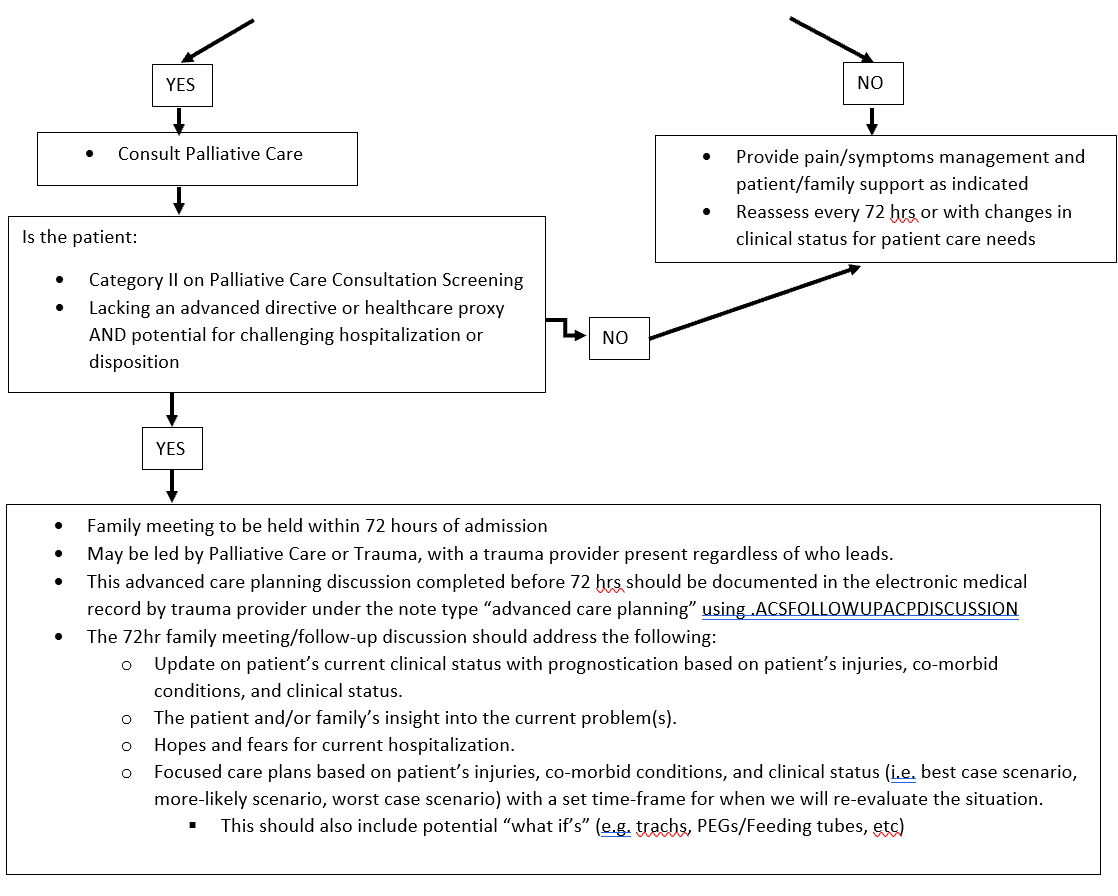
- All Category II patients require a family meeting within 72 hrs of admission.
- Any patient lacking an advanced directive or healthcare proxy AND potential for challenging hospitalization or disposition.
- Family meeting may be led by Palliative Care, Geriatric Medicine or Trauma.
-
- An acute care surgery provider should be present for this discussion regardless of who leads the meeting.
-
- This advanced care planning discussion should be documented in the electronic medical record under the note type “advanced care planning”.
-
- Note template: .ACSACPFOLLOWUP
-
- The 72hr family meeting/follow-up discussion should address the following:
-
- Update on patient’s current clinical status with prognostication based on patient’s injuries, co-morbid conditions, and clinical status.
- The patient and/or family’s insight into the current problem(s).
- Hopes and fears for current hospitalization.
- Focused care plans based on patient’s injuries, co-morbid conditions, and clinical status (i.e. best case scenario, more-likely scenario, worst case scenario) with a set time-frame for when we will re-evaluate the situation.
-
- This should also include potential “what if’s” (e.g. trachs, PEGs/Feeding tubes, etc)
-
-
Follow-up Care
- Significant changes in a patient’s clinical status, should prompt additional advanced care planning discussions as needed.
- If consulted, palliative care will continue to follow the patient throughout his/her hospital course as indicated.
Outcome Measures and Guideline Adherence
- Timing and documentation of initial advanced care planning discussions will be monitored on 80% of all trauma patients
- Timing and utilization of palliative care services will be monitored on all trauma mortalities and hospice/CMO discharges.
- Pathway will be re-assessed following a 3 month pilot study.
Key Contributors
- Emily Cantrell, MD | Division of Acute Care Surgery | Author
- Charity Evans, MD | Division of Acute Care Surgery | Author
- Elizabeth Mahal, MD | Department of Emergency Medicine | Author
- Carrie Siedlik, APRN-NP | Palliative Care Medicine | Author
- Remy Kaslon, APRN-NP | Palliative Care Medicine | Author
- Katie Circo, RN | Nursing Professional Development Specialist MICU and SICU, Nebraska Medicine | Author
- Katherine Maliszewski, MD | Internal Medicine/Geriatric Medicine | Author
- Abby Josef, MD | Division of Acute Care Surgery | Updates Author
Last Updated
October, 2024
References
- American College of Surgeons. Trauma Quality Improvement Program Palliative Care Best Practice Guidelines. https://www.facs.org/media/g3rfegcn/palliative_guidelines.pdf
- American College of Surgeons. Trauma Quality Improvement Program Geriatric Trauma Management Guidelines. https://www.facs.org/media/314or1oq/geriatric_guidelines.pdf
- Fiorentino M, et al. Palliative care in trauma: Not just for the dying. J Trauma and Acute Care Surg. 2019:87(5):1156-1163.
Appendix and Supplemental Materials
Figure 1. Model for advanced care planning discussions and consultation of palliative care in trauma.

Table 1. 5 item FRAIL Questionnaire

Table 2. Palliative Care Screening in Trauma

*Surprise question example: “Would you be surprised if the patient died in the next 12 months?”
Table 3. Palliative Care Bundle

Guideline Algorithm
Alcohol Withdrawal Pathway- PAWSS

Date: January, 24, 2022
Key Contributor(s): Olabisi Sheppard, MD
Assessing Capacity
Why assess capacity? Informed consent promotes individual autonomy and fosters rational decision-making, and is founded on the right of self-determination and physician’s fiduciary responsibility to the patient. Informed consent requires disclosure of information, voluntary choice and capacity to decide. Therefore, determining a patient’s capacity is of utmost importance during a patient’s hospitalization.
Capacity refers to the ability to accept or refuse treatment recommendations. Capacity is determined by a clinician upon specific elements of a mental status exam. Capacity does not have to be a psychologist or psychiatrist.
Capacity differs from competency. Competency is defined as “the ability of an individual to participate in legal proceedings”. Legal competence is presumed - to disprove an individual's competence requires a hearing and presentation of evidence. Competence is determined by a judge. This legal determination is never determined by medical providers. Because this determination is not made by providers we will not use this term further in this pathway.
- Any patient who is observed to have functional deficits judged to be sufficiently great that the patient currently cannot meet the demands of a specific decision making situation and its inherent consequences SHOULD be assessed for capacity.
- Capacity is determined for individual decisions, and may vary by risk involved. For example, a patient may have capacity to refuse a bowel regimen but lack capacity to leave the hospital against medical advice.
- Capacity should be reassessed as decision-making abilities deteriorate or improve. Capacity also needs to be documented each time it is assessed.
- Speech therapy can provide the treatment team with additional information and expertise on cognition, to assist with the capacity assessment. However, cognition testing is not required for capacity assessment.
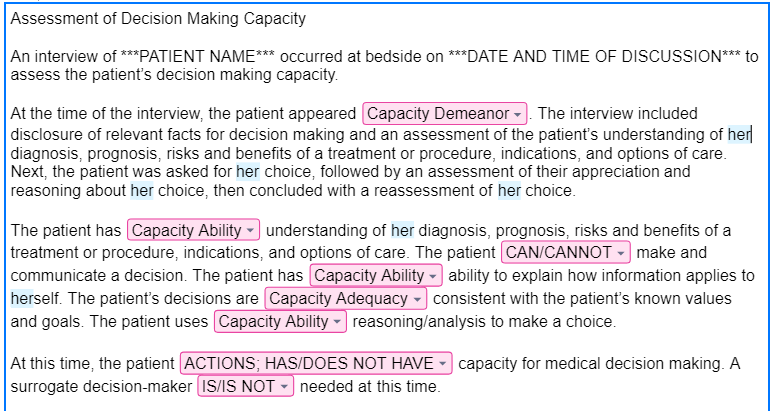
Discussions regarding a patient's capacity to make a decision should be documented in the electronic medical record in a short progress note using the assessing capacity note template.
The template can be found using the dot phrase = .acscapacityassessment
Example of note template in electronic medical record:
Evaluation and Management of Delirium
Purpose
Provide guidance on the evaluation, diagnosis, and management of hospitalized patients who develop delirium.
Background/Definitions
Delirium is a neuropsychiatric disorder that is characterized by a disturbance in attention, consciousness and cognition with a reduced ability to focus, sustain or shift attention. It can develop over a short period of time, is a change from baseline, and fluctuates in severity. The clinical presentation varies but usually presents with psychomotor behavioral disturbances such as hyperactivity or hypoactivity and with impairment in sleep duration and quality.
Delirium is caused by an underlying medical condition that is not better explained by another preexisting, evolving, or established neurocognitive disorder. The underlying cause of delirium can vary widely and involve anything that stresses the baseline homeostasis of a vulnerable patient. Examples include: substance abuse intoxication and withdrawal, medication side effects, infection, surgery, metabolic derangements, pain, constipation, and urinary retention.
There are 3 subtypes of delirium:
- Hyperactive: patients present with restlessness, purposeless and uncontrollable movements, agitation, hallucinations, and behaviors
- Hypoactive: patients appear calm, lethargic, and have slowed mentation and slow/decreased movements.
- Mixed: fluctuation between hyperactive and hypoactive states.
Delirium has consistently shown to be associated with higher mortality rates, longer ICU and hospital lengths of stay, increased morbidity, and cognitive and psychiatric sequelae that can persist weeks to months following hospital discharge.
The elderly, polytrauma patients and those critically ill in the ICU are all groups that have been identified as particularly susceptible to developing delirium. The incidence of delirium in trauma patients admitted to the ICU has been reported as up to 67%, with increased risk for elderly and those requiring mechanical ventilation.
In light of this, it is critical for trauma and critical care providers to be well versed in screening for and identifying delirium as well as implementing preventative strategies against delirium in order to optimize patient outcomes and reduce healthcare costs.
Guideline Inclusion Criteria
All admitted trauma patients
Guideline Exclusion Criteria
none
Diagnostic Evaluation
· Risk factors for delirium development:
Each trauma patient should be assessed for nonmodifiable and modifiable risk factors that may contribute to the development of delirium.
|
Nonmodifiable Risk Factors |
Modifiable Risk Factors |
|
Increased age |
Restraints |
|
Depressed GCS on arrival |
Ventilator days |
|
Increased blood product transfusion |
Increased sedation |
|
Multisystem organ failure |
Infection/sepsis |
|
Traumatic brain injury (TBI) |
Indwelling urinary catheters/lines |
|
History of substance abuse |
Medications |
|
Frailty |
|
|
Comorbidities (hypertension, dementia) |
|
|
Nutritional impairment |
|
|
Medications known to be associated with increased delirium can include: |
||||||||||||||||
|
· Patient care should be centered around optimizing modifiable risk factors as able in hopes of minimizing the risk of delirium development.
· Delirium Detection and monitoring:
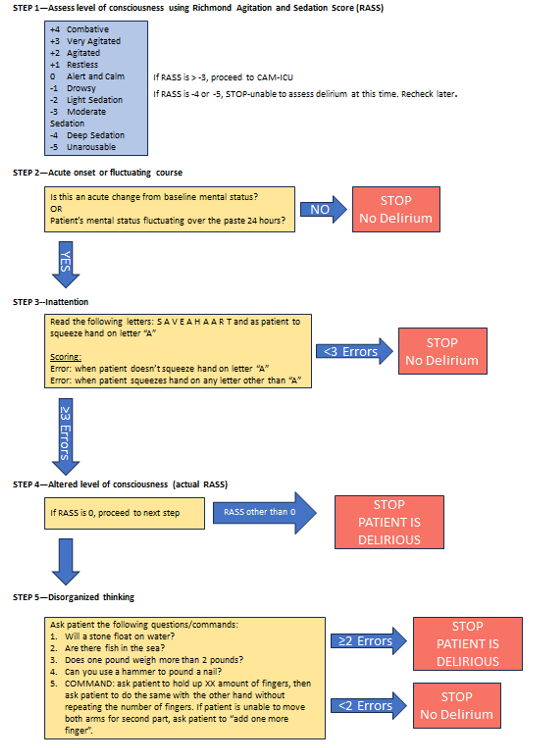
The most reliable method for detecting delirium is with the use of externally validated screening tools. One of the more widely used screening tool is the Confusion Assessment Method for ICU (CAM-ICU) which is applied primarily to patients in the ICU. Alternatively, a Brief Confusion Assessment Method (bCAM) is primarily used for delirium screening on floor patients. (see Figure 1)
Practice Recommendations for Management
- All trauma patients should be assessed for delirium risk and development daily and as needed when a change in clinical status occurs and delirium is suspected. This includes optimizing modifiable risk factors and medication regimens as able and implementing delirium prevention strategies. (see Figure 2)
- If delirium is suspected, diagnosis should be confirmed by using the CAM-ICU or bCAM screening tools.
- Once delirium is confirmed, provider should examine/evaluate the patient for possible causes and contributing factors to delirium (i.e. infection, electrolyte abnormalities, medication side effects, substance intoxication/withdrawal, etc) and treat/correct as indicated by work-up (See FIGURE 3).
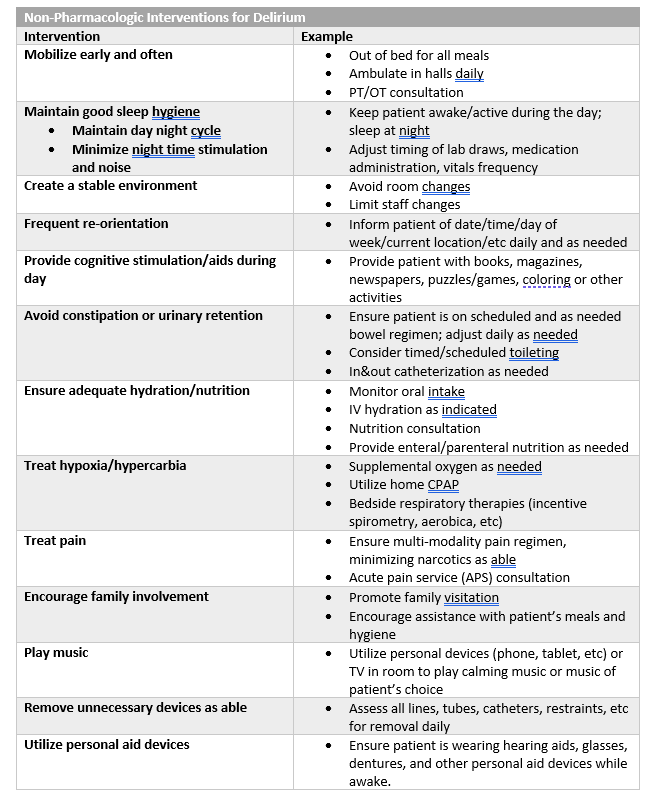
- In addition to correcting/treating contributing factors, provider should also implement delirium treatment interventions beginning with non-pharmacologic interventions first and escalating to pharmacologic interventions as needed. (see FIGURE 4)
-
-
- There are currently no pharmacologic agents shown to prevent the development of delirium or shorten the course of delirium. Pharmacologic agents should be used as needed to treat symptoms of delirium and prevent harm to patient and/or staff.
- If pharmacologic interventions are required, they should be preferentially used on an as needed basis with the minimal dose required to achieve the desired effect (i.e. not agitated or at risk to harm self/staff).
- If scheduled pharmacologic interventions are used, medications should be assessed daily for need and weaned/discontinued once delirium has resolved.
-
-
Follow-up Care
- All patients diagnosed with delirium during his/her hospital stay should be assessed daily and as needed for ongoing signs and symptoms of delirium and potential opportunities to optimize delirium prevention and treatment.
- Diagnosis of delirium should be well documented in the patient’s hospital discharge summary so that post-discharge cognitive and psychiatric sequelae may be assessed at follow-up visits with either trauma providers or patient’s primary care providers.
Outcome Measure and Guideline Adherence
- Diagnosis of delirium is actively tracked through our trauma performance improvement initiatives.
-
-
- Each case will be reviewed by our PI coordinators and TMD/aTMD at a primary and/or secondary review level to confirm diagnosis and assess for opportunities for improvement.
- If opportunities for improvement or trends identified, cases will be further examined at a secondary and/or tertiary review level in our weekly trauma performance improvement conference or monthly multi-disciplinary trauma meetings.
-
-
Related Policies
- Pharmaceutical Management of Post-TBI Neuropsychiatric Symptoms, Acute Care Surgery Patient Pathway, Nebraska Medicine.
Key Contributors
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Erin Panowicz, APRN | Division of Acute Care Surgery | Author
- Rebecca Sedlak, PharmD, BCCCP | Critical Care Pharmacy, Nebraska Medicine | Author
Last Updated
February, 2024
References
- Williams EC, Estime S, Kuza CM. Delirium in trauma ICUs: a review of incidence, risk factors, outcomes, and management. Curr Opin Anesthesiol. 2023 Apr;36(2):137-146.
- Devlin JW, Skrobik Y, Gelinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018 Sep;46(9):e825-e873.
- Shoulders BR, Elsabagh S, Tam DJ, et al. Risk factors for delirium and association of antipsychotic use with delirium progression in critically ill trauma patients. Am Surg. 2023 May;89(5):1610-1615.
- Ely EW, et al. Confusion Assessment Method for the Intensive Care Unit. JAMA. 2001; 286:2703-2710.
- Inouye SK, et al. Confusion Assessment Method. Ann Intern Med. 1990; 113:941-948.
Appendix/Supplemental Materials
FIGURE 1--Delirium Screening Tools
(a) Confusion Assessment Method for ICU (CAM-ICU)
(b) Brief Confusion Assessment Method (bCAM) Flow Sheet
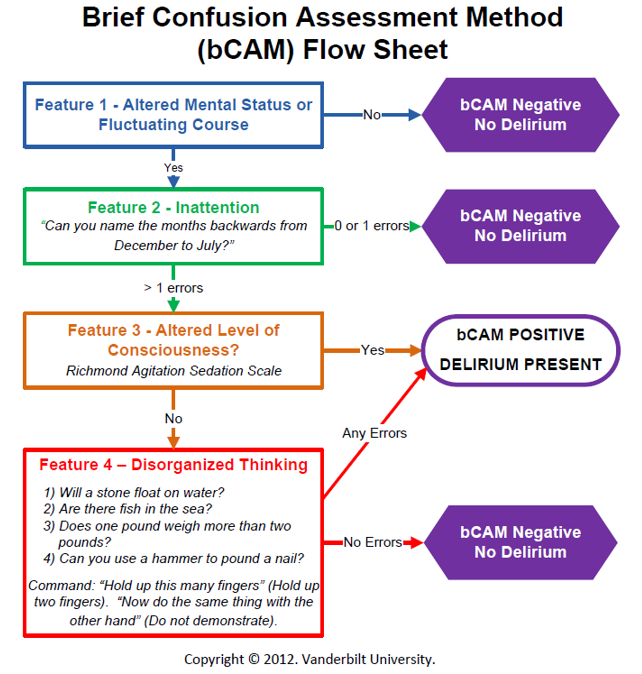
FIGURE 2-- Delirium Prevention Strategies
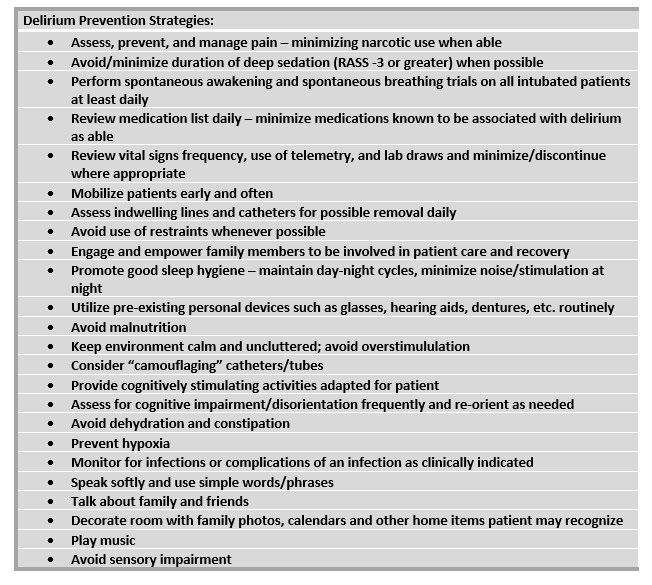
FIGURE 3--Suggested algorithm for management of delirium
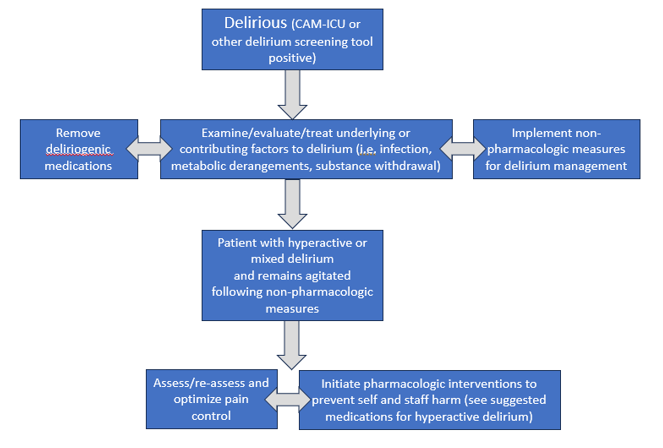
FIGURE 4--Non-pharmacologic and pharmacologic interventions for delirium
|
Pharmacologic Interventions for Delirium
|
|||
|
Class/Drug |
Suggested Use |
Dosing |
Adverse Effects |
|
Typical Antipsychotic: Haloperidol (Haldol)
|
Controlling acute severe agitation |
2.5-10 mg (usual dose 5 mg) IV/IM. May repeat Q15min (up to 20 mg) until calm achieved |
Oversedation, QT prolongation, arrythmia, extrapyramidal symptoms, dopaminergic antagonism (avoid in Parkinsons), may lower seizure threshold |
|
Controlling intermittent (or breakthrough) agitation |
2.5- 5 mg Q4H PRN agitation |
||
|
Atypical Antipsychotics: |
|
||
|
Quetiapine (Seroquel) |
Maintaining control of agitation associated with hyperactive/ mixed delirium
|
Typical start: 50 mg PO/perFT Q8-12hr. If effect not achieved at 24 hours, may increase dose (max 400 mg/day). |
Oversedation, QT prolongation (less than IV haloperidol), extrapyramidal symptoms (less than haloperidol) |
|
Olanzapine (Zyprexa) |
Typical start: 5 mg PO/perFT daily. If effect not achieved at 24 hours, may increase dose (max of 20 mg/day). |
||
|
Risperidone (Risperdal) |
Controlling acute agitation |
1-2 mg PO/per FT. May repeat dose in 1-2 hours, up to 6mg in 24 hours.
|
|
|
Central Alpha-2 Agonist: Dexmedetomidine (Precedex) |
Maintaining control of agitation associated with delirium |
If intubated: 0.2-1.5 mcg/kg/hour continuous infusion
If extubated: 0.2-0.7 mcg/kg/hour continuous infusion, order expires at 24-hours, must reassess and reorder if still indicated. |
Restricted to ICU and SDCC. No bolus dosing allowed.
Hypotension, bradycardia, withdrawal (if use prolonged) |
|
Benzodiazepine: Lorazepam (Ativan) |
Controlling severe acute agitation—not typically used as 1st line
|
0.5-1 mg IV/PO/perFT, may repeat in 15 min |
AVOID if able as BZDs causes/exacerbate delirium.
Oversedation |
|
Acceptable option for alcohol withdrawal, agitation in patient with chronic benzo use, agitation in Parkinson’s |
0.25-1 mg IV/PO/perFT Q4-6H PRN agitation |
||
|
Anticonvulsant: Valproic Acid (Depakote) |
For agitation refractory to other agents (ie adequate analgesia/ sedation, antipsychotics). May be especially useful when associated with substance withdrawal or untreated mood (ie bipolar) disorder
|
Typical start: 250 mg IV/PO/perFT Q8H. If effect not achieved at 24 hours, may increase by 250 mg increments.
May use loading dose for acute control: 15 mg/kg (~ 1000 mg)
|
Hepatotoxicity, hyperammonemia, thrombocytopenia, drug interaction with carbapenems
Safe therapeutic range: 50-125 mcg/mL |
|
Endogenous Hormone: Melatonin |
Consider if insomnia is contributing to delirium |
3 mg PO/perFT QHS, may increase to 9 mg |
Daytime drowsiness, limited side effects |
|
SSRI: Trazodone
|
Potentially useful if insomnia is contributing to delirium (2nd line) |
25-50 mg PO/perFT QHS |
Daytime drowsiness, antihistamine effects, sensory distortion, sleep walking |
|
For all added medications for delirium/agitation: · Start at lowest (or a 50% reduced dose) in elderly (ie >65 yoa). · These medications are not for long-term use, reassess daily. Delirium often resolves/improves over several days and the agents should be weaned/discontinued if no longer indicated. |
|||
Forensic Examiner Program Nebraska Medicine

Summary – Law Enforcement Requests for Patient Information
| Law Enforcement Request | NM Staff Response | |
| 1 |
Staff safety/security concerns |
Staff may always request law enforcement’s presence when concerned for their safety/security. |
| 2 |
Requests for patient information, general rule | Ok to disclose patient information as permitted in this chart, by our policies (see policy IM12), or with written patient authorization (form CON MR 0074) |
| 3 |
Patient condition | Ok to disclose one-word condition status without patient authorization: undetermined, good, fair, serious, or critical |
| 4 |
Date of birth (DOB) |
Ok to disclose if:
|
| 5 |
Blood or urine test specimen/results |
Do not provide test specimen or test results to law enforcement UNLESS:
|
| 6 |
Notify law enforcement when patient is discharged | Ok if provided court order that requires such notification or patient is in police custody. Otherwise, decline to provide this notification. See policy LD-12. |
| 7 |
Forms • Court order • Subpoena • Warrant |
Ok to provide information specifically referenced in any of these documents. Forward document to HIM for processing. If urgent request that can’t wait for HIM, Nebraska Medicine staff may contact Risk (consult Web On Call or hospital operator to reach on-call Risk staff) or Legal with any questions. |
| 8 |
Victims of Crime |
If patient is victim of crime and unable to authorize disclosure because incapacitated or there are other emergency circumstances, NM staff may disclose patient info to law enforcement if law enforcement: • states information is needed to determine whether someone other than patient violated law, |
| 9 |
Identification of: • suspect • fugitive • material witness • missing person |
Ok to disclose only the following information if requested by law enforcement to identify suspect, fugitive, material witness, or • name and address |
| 10 |
Interviews Patient is in police custody |
Ok for law enforcement officer to be present/ask patient questions UNLESS presence would impede staff’s ability to provide patient care or compromise sterilization/infection control procedures |
| 11 |
Interviews Patient is not in police custody |
Ok for law enforcement officer to be present/ask patient questions IF patient agrees and presence would not impede staff’s ability to provide patient care or compromise sterilization/infection control |
| 12 |
Visitation restrictions Patient is in police custody |
Ok to restrict visitor access per law enforcement officer’s direction. |
| 13 |
Visitation restrictions Patient is not in police custody |
Ok to grant law enforcement officer’s request to speak with patient before visitors are allowed to visit patient in two situations: 1. patient agrees to request and honoring request does not impede patient care or compromise sterilization/infection control |
| 14 |
Wounds of Violence (excluding sexual assault) |
If NM staff suspect patient injury caused by crime (excluding sexual assault), must report to law enforcement: victim’s name, description of victim’s physical injury, and, if ascertainable, victim’s residential address and location of offense. See policy PE 03. |
| 15 |
Sexual assault | If patient was 18+ years at time of sexual assault and provides written consent or patient is suffering from serious bodily injury or any bodily injury caused by deadly weapon, which appears to have been received in connection with or as a result of sexual assault, must report following to law enforcement: victim’s name, description of victim’s physical injury, and, if ascertainable, victim’s residential address and location of the offense. |
| 16 |
Child Abuse or Neglect | For suspected child abuse or neglect, see the following policies for related reporting obligations and permitted disclosures: • PE 03 (Reporting of Abuse, Neglect or Injury) • SH21 (Infant Drug Testing Guidelines for Providers) • AD48 (Drug Testing Guidelines for Providers: Pregnant and Postpartum Patients) |