2. Initial Management and Resuscitation of the Trauma Patient
Educational materials and pathways regarding the initial approach to the evaluation, management and resuscitation of the injured patient.
- Adult Traumatic Agonal Arrest and Resuscitation
- Drowning
- e-FAST for Trauma
- Early Femoral Arterial Line Placement for Trauma
- Hanging
- Management of the Pregnant Trauma Patient
- Massive Transfusion for Trauma Protocol
- REBOA Instructions
- Whole Blood Usage in Trauma
- Trauma Bay Adult Acute Agitation Management
Adult Traumatic Agonal Arrest and Resuscitation
Purpose
To outline the procedure for the treatment of the adult traumatic patient with a penetrating or blunt mechanism of injury who has no signs of life.
In patients without signs of life for >10 minutes in blunt trauma or >15 minutes in penetrating trauma, it is appropriate to terminate resuscitation efforts. Trauma surgeon discretion required as reported pre hospital CPR times may be inaccurate.
Definitions
- Blunt trauma –physical impact to the body by some force
- Penetrating trauma - occurs when a foreign object pierces the skin and enters the body creating a wound
- Adult trauma patient – any patient age fifteen (15) years or older who has sustained a blunt injury
- Agonal arrest - a severely injured patient in extremis, with no signs of life (absent pulse, absent respirations, absent pupil response, GCS 3)
Background
- Resuscitation of the adult trauma patient who is agonal or arrests as a result of a penetrating or blunt mechanism consist of a rapid assessment and treatment of the various measures of PEA (profound hypovolemia, airway compromise, tension pneumothorax and pericardial tamponade).
- Drowning, lightning strikes, medical causes of cardiac arrest, patients with profound hypothermia or if the patient’s age is 14 years and less are excluded from this guideline.
- The utilization of Advanced Cardiac Life Support (ACLS) and Basic Life Support (BLS) measures, including use of the Lucas device, in the setting of Advance Trauma Life Support (ATLS) resuscitation is of limited, if any, benefit in the setting of blunt traumatic patient arrest.
- Consider previous establishment of the patient’s DNR/DNI status, especially in patients who reside in a long term health care facility.
- Procedures (including airway assessment, chest tubes, etc.) take priority over chest compressions in the trauma patient in agonal or arrest states.
Resuscitation Algorithm
CONSIDER removal of Lucas device/mechanical chest compression device upon patient’s arrival in trauma bay.
- Airway:
-
- Non-intubated patient
-
- Obtain adequate airway (definitive ideal, however, if King, LMA or iGel is adequate, continue until pt stabilizes)
-
- Confirmation of Airway placement
-
- Visualization of ETT placement through vocal cords, if applicable
- Colorimetric CO2 detector (may not be reliable in arrest)
- Auscultation of bilateral breath sounds; absence of delivered breath sounds over epigastrium
- Appropriate O2 Saturation
-
- Intubated Patient
-
- Clear communication of assessment to trauma leader
- Confirmation of airway placement by ER faculty at head of bed
- Colorimetric CO2 detector (may not be reliable in arrest)
- Direct laryngoscopy may be considered in setting of any question of placement of ETT. Direct laryngoscopy in presence of ETT has a risk of dislodgement of appropriately placed ETT.
- Auscultation of bilateral breath sounds; absence of delivered breath sounds over epigastrium
- Appropriate O2 saturation
-
- Non-intubated patient
-
- Breathing:
-
- Bilateral Chest Tube Thoracostomy
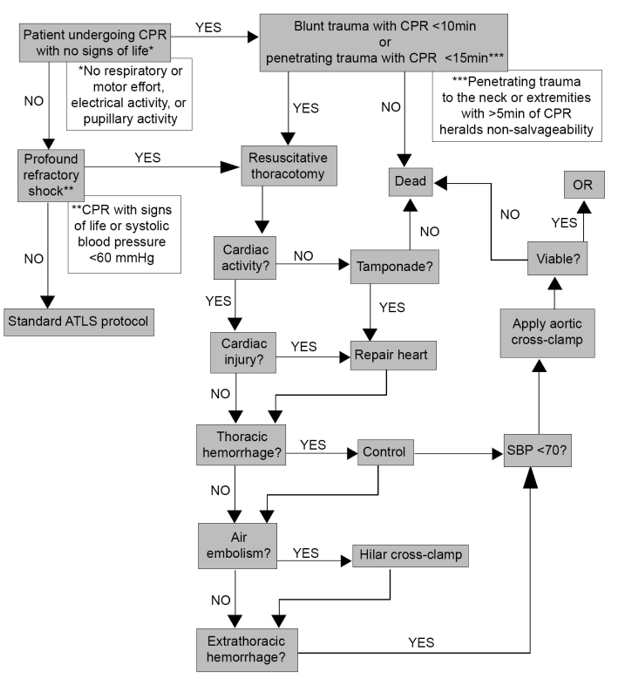
- Resuscitative Thoracotomy (see Western Trauma algorithm below)
-
- Circulation:
-
- Rapid assessment of central (femoral) and peripheral pulses (radial, pedal)
- Clear communication of assessment to trauma leader
- Control of life-threatening external hemorrhage (hold pressure, tourniquet, etc)
- Obtain manual blood pressure (will not be present if no pulse)
- Confirmation of in-place intravenous (IV) access
- If no IV access:
-
- Establish IV, Intraosseous (IO) or central access
- Rapid, early delivery of Whole blood or Packed Red Blood Cells/plasma
-
- Consider initiation of Massive Blood Transfusion (MBT) protocol
- Maintain 1:1:1 ratios
-
-
- Attach cardiac leads/monitor
- Check Cardiac window on Focused Assessment with Sonography in Trauma (FAST)
-
- Assess for pericardial effusion
- Assess cardiac kinetic activity
-
-
- Disability:
-
- Glasgow Coma Scale (GCS) measurement
- Pupillary response
-
- Exposure/Environment
-
- Rapid and complete patient exposure
- Rapidly cover the exposed patient with warmed blankets (allow above assessment and procedures)
- Ensure underbody Bair Hugger functional (or provide warmth by another means)
-
During ABCDEs in a blunt agonal arrest, determine length of time of CPR and quickly assess patient for signs of life (detectable blood pressure, respiratory or motor effort, cardiac electrical activity, or pupillary activity)
- If CPR<10 min in blunt trauma or <15 minutes in penetrating trauma, AND pt has signs of life, proceed with Resuscitative Thoracotomy (see Western Trauma Association algorithm below).
- If CPR>10 min in blunt trauma or <15 minutes in penetrating trauma, AND NO signs of life, pt should be pronounced dead.
FIGURE 1. Western Trauma Resuscitative Thoracotomy algorithm
https://www.westerntrauma.org/wp-content/uploads/2020/08/Resuscitative-Thoracotomy_FINAL.svg
{kind=link}
References
- Trauma patients receiving CPR: Predictors of Survival. J Trauma 2005 58:951-958. Pickens JJ, Copass MK, Bulger EM.
- Blunt Trauma Patients with Prehospital Pulseless Electrical Activity (PEA): Poor Ending Assured. J Trauma 2002 53:876-881. Martin SK, Shatney CH, Sherck JP, Ho C, Homan SJ, Neff J.
- Confusion Surrounding the Treatment of Traumatic Cardiac Arrest. Journal of the American College of Surgeons. Fulton RL, Voigt WJ, Hilakos AS.
- Role of External Cardiac Compression in Truncal Trauma. J Trauma 1982 Vol. 22 No.11. Mattox KL, Feliciano DV.
- Hemodynamic Effects of External Cardiac Massage in Trauma Shock. J Trauma 1989 Vol. 29 No. 10. Luna GK, Pavilin EG, Kirkman T, Copass MK, Rice CL.
- Guidelines for Withholding or Termination of Resuscitation In Prehospital Traumatic Cardiopulmonary Arrest: A Joint Position Paper From the National Association of EMS Physicians Standards and Clinical Practice Committee and the American College of Surgeons Committee on Trauma. Prehospital Emergency Care January / March 2003 Vol 7 / No. 1 141-146
- Withholding of Resuscitation for Adult Traumatic Cardiopulmonary Arrest: National Association of EMS Physicians and American College of Surgeons Committee on Trauma. Prehospital Emergency Care 2013 17:291
Authors
Charity Evans, MD | Division of Acute Care Surgery, Faculty | Principle Author
Last Updated
February, 2024
Drowning
Quick Guide:
Patients should be activated per their physiology and suspected injuries, which will most often be a full trauma given that the majority of suspected injuries include airway issues, level of consciousness/brain injury, and/or spinal cord injuries.
Trauma should be the admitting service to the appropriate level of care. If ICU admission is warranted, the appropriate critical care team should also be consulted (i.e Critical Care Surgery (CCS) for patients >12 yrs of age and Pediatric Critical Care Medicine (PCCM) for patients ≤12 yrs of age).
**Patients who have an event where they are submerged in water but return to baseline at the scene without concern for traumatic injuries do not meet these criteria and do not need a trauma activation for the submersion event. They may be safely evaluated in the ER and observed by medical admitting services (most often pediatrics).
Terms
Drowning is the process of experiencing respiratory impairment from submersion or immersion in liquid.
There are no medically accepted conditions known as “near-drowning,” “dry drowning,” “secondary drowning” or delayed drowning wherein a person was submerged in the water at some point, had no immediate breathing difficulty and later developed delayed onset of respiratory symptoms after a period of being asymptomatic [3].
Epidemiology
Drowning is the leading cause of death for children ages 1-4, and the second leading cause of unintentional injury-related death for children 5-14 (second only to MVCs) [1]. There is another peak among children and young adults aged 15-30, most often due to recreational swimming in natural bodies of water [2]. Other risk factors include alcohol consumption, hypothermia, traumatic injury leading to unconsciousness, neurodevelopmental conditions, and seizure disorders.
Pathophysiology of Injuries
Airway:
Panic results in disruption of normal breathing patterns, subsequent aspiration of fluid leads to laryngospasm and hypoxemia.
Pulmonary:
There is no difference between salt and fresh water- both result in hypoxemia and surfactant destruction, predisposing patients to noncardiogenic pulmonary edema and acute respiratory distress syndrome (ARDS).
Cardiac:
Arrhythmias may occur secondary to hypoxemia and hypothermia.
Neurologic:
Cerebral edema and elevated intracranial pressure develop as consequences of cerebral hypoxia, which is the major contributor to morbidity and mortality.
Later findings:
Hypoxia and hypoperfusion can trigger systemic inflammatory response, causing isolated cardiac, renal, or hepatic dysfunction, sepsis, or multiorgan failure. Rarely, patients with normal initial chest x-rays (similar to pulmonary contusions) may develop fulminant pulmonary edema within 12 hours, potentially reflecting delayed ARDS, neurogenic edema, or airway hyperreactivity.
Death from drowning primarily results from hypoxemia caused by water aspiration, which disrupts alveolar gas exchange, destroys surfactant, and produces noncardiogenic pulmonary edema. If rescue does not occur, hypoxia rapidly leads to loss of consciousness, apnea, and hypoxic cardiac arrest, usually presenting with bradycardia or pulseless electrical activity. Later deaths mainly arise from neurologic injury due to prolonged cerebral hypoxia [5].
History & Physical Examination
-focus the history on duration of submersion, length of extraction/rescue time, whether pulses were lost and/or if CPR was required. The likelihood of diving related injuries associated with the entry into the water are also important.
-additional questions regarding nonaccidental trauma can be added depending on the individual patient’s circumstances.
-obtain labs for toxicology, ethanol, metabolic derangements (most commonly lactic acidosis)
-Physical examination for signs of traumatic injuries as per standard ATLS protocol
Early Management/Stabilization
-Patients should be activated per their physiology and suspected injuries, which will most often be a full trauma
-Evaluate ABCs as always (primary and secondary survey per ATLS protocol)
-Immobilization of the spine is recommended for patients who sustained a dive or present with an unknown history
- Noninvasive positive pressure ventilation or endotracheal intubation may be required to maintain oxygen saturation
-Hypothermia should be addressed by passive rewarming and removal of cold wet clothes
-Noncardiogenic pulmonary edema and ARDS may develop over the next 12-24 hours [6]
-Glucocorticoids, diuretics, and empiric antibiotics are not recommended for routine use. Antibiotic therapy should be initiated only if clinical evidence of infection emerges [7]
Imaging
- Chest x-ray
- Non-contrast CT Head
- CT C-spine
- CTA neck and Head
- Can consider additional CTs (i.e. Trauma “pan scan”) if patient is unconscious, physical exams warrants, or history is concerning for additional injuries or if history is uncertain
Disposition
Trauma should be the admitting service to the appropriate level of care:
-Admit critically ill patients to the ICU with either CCS or PCCM consultation
-Admit patients without ICU needs to the Trauma service
-Patients with mild or no symptoms may be observed in the ER for 4-8 hours.
-ECMO may be considered as salvage therapy for refractory hypoxemia or severe hypothermia. These patients would be admitted to the CVICU under CCA for ECMO therapy, with transfer back to trauma floor or ICU as appropriate when weaned from ECMO.
Author and last update
Abby Josef, MD, February 2026
References
- Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS). Accessed 19 January 2026.
- Gianfrancesco, H; Sternard, BT. Drowning: Clinical Management. https://www.ncbi.nlm.nih.gov/books/NBK430833/ . Accessed 9 February 2026.
- Spack L, Gedeit R, Splaingard M, Havens PL. Failure of aggressive therapy to alter outcomes in pediatric near-drowning. Pediatric Emergency Care 1997;13(2):98–102.
- Suominen PK, Vähätalo R. Neurologic long term outcome after drowning in children. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2012;20(55):1–7.
- Suominen PK, Sutinen N, Valle S, Olkkola KT, Lönnqvist T. Neurocognitive long term follow-up study on drowned children. Resuscitation 2014;85(8):1059–106.
- Szpilman D, Morgan PJ. Management for the Drowning Patient
- Berger S, Siekmeyer M, Petzold-Quinque S, Kiess W, Merkenschlager A. Drowning and Nonfatal Drowning in Children and Adolescents: A Subsequent Retrospective Data Analysis.
e-FAST for Trauma
Purpose
To standardize the application of e-FAST in the seriously injured patient, the technique employed, and the quality of standards by which they are retrospectively evaluated.
Background
e-FAST is a valuable diagnostic tool in the evaluation of traumatically injured patients that is able to detect life threatening inra-abdominal hemorrhage, pericardial effusion and hemo/pneumothoraces. An e-FAST exam is non-invasive, does not expose the patient to radiation, can rapidly be performed concurrently with other resuscitative measures, and is repeatable. e-FAST has a sensitivity between 73-88%, a specificity between 98-100%, and an accuracy of 96-98%.
Indications for an e-FAST Exam at UNMC/Nebraska Medicine
- Hemodynamically unstable patients as defined by a systolic blood pressure <90 mmHg for adults and <70mmHg + (2x age in years) for pediatric patients.
- At the discretion of the Emergency Medicine or Trauma attending.
Patients in whom e-FAST should strongly be considered
- Pregnant patients
In these special patient populations, if an e-FAST is performed:
- a repeat abdominal ultrasound should be performed 4 hours after the initial e-FAST or sooner if the patient becomes hypotensive.
- a repeat hemoglobin at the time of repeat ultrasound
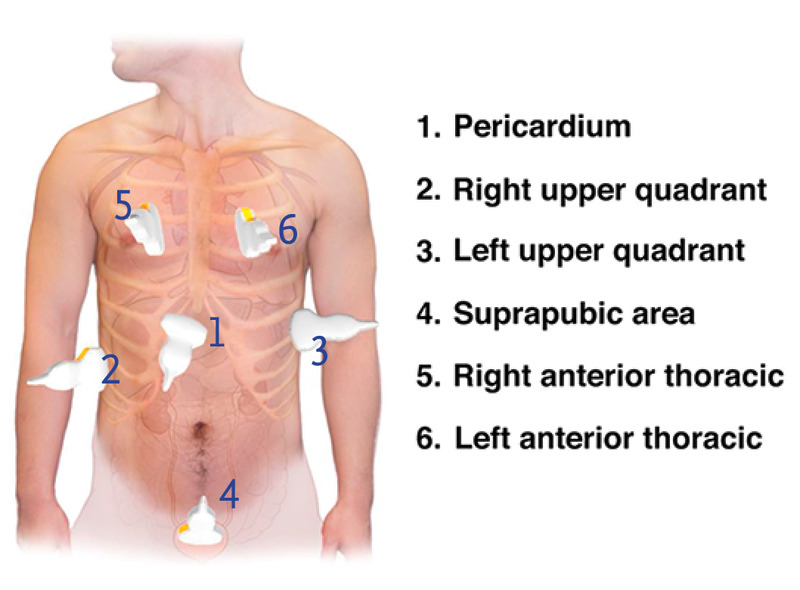
Six views of a complete e-FAST Exam
- pericardial or subxiphoid view
- Right upper quadrant: Lung base and hepatorenal recess
- Left upper quadrant: Lung base and splenorenal recess
- Pelvic: suprapubic view of bladder/Pouch of Douglass
- Right anterior thorax
- left anterior thorax
Ordering and Documentation of e-FAST exams
For all patients undergoing an e-FAST exam for trauma:
- Place an order in the electronic medical record (EPIC) for an e-FAST exam (POC ED US E-FAST, aka FAST)
- A procedure note will be documented by the provider performing the exam, including indication and interpretation of images.
-
- the performance of an e-FAST, the indication for exam and results of the exam should also be documented in the trauma H&P.
-
- Images will be saved with the patient's MRN.
Internal review of e-FAST exams:
The patients in whom e-FAST exams are indicated will be queried and the percentage of those receiving e-FAST exams reported. The documentation, image views and quality, and interpretation of images will be reviewed. Findings will be compared with CT or operative findings. Data will be presented at the monthly Performance Improvement Patient Safety (PIPS) meeting.
References
- AIUM Practice Parameter for the Performance of the Focused Assessment with Sonography for Trauma (FAST) Examination. American Institute of Ultrasound Medicine in collaboration with the American College of Emergency Physicians. http://www.aium.org/resources/guidelines/fast.pdf.
- Branney SW, Moore EE, Cantrill SV, et al. Ultrasound based key clinical pathway reduces the use of hospital resources for the evaluation of blunt abdominal trauma. J Trauma 42:1086-1090, 1997.
- Healey MA, Simons RK, WInchell RJ, et al. A prospective evaluation of abdominal ultrasound in blunt trauma: Is it useful? J Trauma 40:875-883, 1996.
- Glaser K, Tschmelitsch J, Klingler P, et al. Ultrasonography in the management of blunt and thoracic trauma. Arch Surg 129:743-747, 1994.
- Liu M, Lee CH, P'eng FK. Prospective comparison of diagnostic peritoneal lavage, computed tomographic scanning and ultrasonography for the diagnosis of blunt abdominal trauma. J Trauma. 35:267-270 1993.
- Boulanger BR, McLellan BA, Brenneman FD, et al. Emergent abdominal sonography as a screening test in a new diagnostic algorithm for blunt trauma. J Trauma. 40;867-874, 1996.
- Boulanger BR, Brenneman FD, McLellan BA, et al. A prospective study of emergent abdominal sonography after blunt trauma. J Trauma. 39;325-330, 1995.
- Ma OJ, Kefer MP, Mateer JR, et al. Evaluation of hemoperitoneum using single vs multiple ultrasonographic examination. Acad Emerg Med. 2:581-586, 1995.
- Rozycki GS, Oshsner MG, Jaffin JH, et al. Prospective evaluation of surgeons' use of ultrasound in the evaluation of trauma patients. J Trauma. 34:516-527, 1993.
- Smith SR, Kern SJ, Fry WR, et al: Institutional learning curve of surgeon-performed trauma ultrasound. Arch Surg. 133:530-536, 1998.
- McKenney MG, Martin L, Lentz K, et al. 1000 consecutive ultrasounds for blunt abdominal trauma. J Trauma. 40:607-612, 1996.
- Kem SJ, Smith RS, Fry WR, et. al. Sonographic examination of abdominal trauma by senior surgical residents. Am Surg. 63:669-674, 1997.
- Rozycki GS, Ochsner MG, Schmidt JA, et al. A prospective study of surgeon-performed ultrasound as the primary adjuvant modality for injured patient assessment. J Trauma. 39;492-500, 1995.
- Ong A, McKenney MG, McKenney KA, et al. Predicting the need for laparotomy in pediatric trauma patietns on the basis of ultrasound score. J Trauma. 2003;54:503-508.
- Soudack M, Epelman M, Maor R, et al. Experience with focused abdominal sonography for trauma (FAST) in 313 pediatric patietns. J Clin Ultrasound. 2004;32(2):53-61.
- McPartland SJ, Jackson C-CA, Gilchrist BF. "Pediatric Blunt Trauma". Trauma, Critical Care and Surgical Emergencies. Eds. Rabinovici R, Frankel HL, Kirton O. London:Informa, 2010203-226. Print.
UNMC/NM Policy last updated
August, 2019
May, 2025
Early Femoral Arterial Line Placement for Trauma
Purpose
Identify patients who would benefit from early femoral arterial access and describe the process facilitating early femoral arterial access.
Background
Hemorrhage is the leading cause of preventable death in trauma patients. Decision making regarding optimal therapy for the patient experiencing life threatening hemorrhage can be challenging. Early femoral arterial access provides additional information by way of continuous blood pressure monitoring. In addition to improved monitoring, common femoral artery (CFA) access is an essential and rate-limiting step in performing hemorrhage control interventions such as resuscitative endovascular balloon occlusion of the aorta (REBOA) or angioembolization. As the hemorrhaging patient progresses further into hemorrhagic shock, CFA access becomes more challenging to obtain.
Inclusion Criteria
- Trauma patients with blunt or penetrating mechanism
- Concern for life threatening hemorrhage as evidenced by any of the following
-
- Shock index greater than 1
- Assessment of Blood Consumption (ABC) score greater than 2
- Revised Assessment of Bleeding and Transfusion (RABT) score greater than 2
- Systolic blood pressure less than 90 mmHg
- Transient or non-responder to initial resuscitation
-
- Difficulty obtaining non-invasive blood pressure management
- REBOA deployment is considered as an adjunct for hemorrhage control
Exclusion Criteria
- Concern for pericardial tamponade
- Concern for supradiaphragmatic hemorrhage
- Patient not a candidate for REBOA
Trauma Bay Workflow
- For full trauma activations, ensure that a functioning ultrasound machine is present in the trauma bay, is powered up and otherwise ready to be used
- Ensure either femoral arterial line kit or 5 French micropuncture kit is immediately available
- Ensure that sterile probe cover, Chloraprep and ultrasound gel are immediately available
- Communicate with nursing staff that early CFA access may be pursued giving them time to set up pressure transducer
- Using the criteria above at the discretion of the trauma surgeon or their surrogate, decision to pursue early CFA access is made
- The groin is prepped and draped sterilely
- The linear array ultrasound probe is draped in the usual fashion
- Using real time ultrasound guidance, the CFA is accessed and the catheter placed in the usual fashion. A detailed description of this technique is beyond the scope of this document. Ultrasound guidance should be standard of care, however access by landmarks can be considered on a case by case basis
- Once the catheter has been inserted into the CFA, it is connected to the pressure transducer set up
- The catheter is secured and a sterile dressing is applied
- Depending on the patient’s hemodynamics, their response to resuscitation and their injury pattern, this femoral catheter can remain for hemodynamic monitoring or can be upsized to a 7 French sheath to facilitate placement of REBOA
Key Contributors
Kevin Kemp, MD
Last Updated
April, 2023
References
- Manning JE, Moore EE, Morrison JJ, Lyon RF, DuBose JJ, Ross JD. Femoral vascular access for endovascular resuscitation. J Trauma Acute Care Surg. 2021 Oct 1;91(4):e104-e113. doi: 10.1097/TA.0000000000003339. PMID: 34238862.
- Romagnoli A, Teeter W, Pasley J, Hu P, Hoehn M, Stein D, Scalea T, Brenner M. Time to aortic occlusion: It's all about access. J Trauma Acute Care Surg. 2017 Dec;83(6):1161-1164. doi: 10.1097/TA.0000000000001665. PMID: 29190256.
- Hadley, Jamie B. MD; Coleman, Julia R. MD, MPH; Moore, Ernest E. MD; Lawless, Ryan MD; Burlew, Clay C. MD; Platnick, Barry MD; Pieracci, Fredric M. MD; Hoehn, Melanie R. MD; Coleman, Jamie J. MD; Campion, Eric M. MD; Cohen, Mitchell J. MD; Cralley, Alexis MD; Eitel, Andrew P. MD; Bartley, Matthew MD, MS; Vigneshwar, Navin MD, MPH; Sauaia, Angela MD, PhD; Fox, Charles J. MD. Strategies for successful implementation of resuscitative endovascular balloon occlusion of the aorta in an urban Level I trauma center. Journal of Trauma and Acute Care Surgery 91(2):p 295-301, August 2021. | DOI: 10.1097/TA.0000000000003198
- Romagnoli, A and Brenner, M. “Principles of REBOA.” Chapter 6, p 81-96. Horer, T et al (eds.). Endovascular Resuscitation and Trauma Management, Hot Topics in Trauma and Acute Care Surgery. Springer Nature 2020.
Hanging
Quick Guide:
Patients should be activated per their physiology and suspected injuries, which will most often be a full trauma given that the majority of suspected injuries include airway issues, level of consciousness/brain injury, and/or spinal cord injuries.
Trauma should be the admitting service to the appropriate level of care. If ICU admission is warranted, the appropriate critical care team should also be consulted (i.e Critical Care Surgery (CCS) for patients >12 yrs of age and Pediatric Critical Care Medicine (PCCM) for patients ≤12 yrs of age).
Terms/Classification [1]
-“Near-hanging” is a term for patients who have survived an attempted hanging (or at least long enough to reach the hospital).
-“Complete hanging” defines when a patient’s legs are fully suspended off the ground and the patient's bodyweight is fully suspended by the neck.
-“Incomplete hanging” defines when some part of the patient’s body is still on the ground and the body's full weight is not suspended off the ground.
-“Judicial hanging” classically refers to victims who fell at least the height of their body.
Epidemiology
-Hanging is the 2nd most common form of successful suicide in the US after firearms. In many areas without access to firearms, hanging is the most common form of successful suicide (England, Australia, New Zealand, also more relevant- in the US jail system)
-Highly lethal (around 70%) but also high survival in those who are rescued and reach the hospital alive (80-90% survival)
-Risk Factors: male, aged 15-44 years, history of drug or alcohol abuse, history of psychiatric illness
Pathophysiology of Injuries
Spine/Spinal Cord:
-In a judicial hanging, there will almost always be cervical spine injury. The head hyperextends, leading to fracture of the upper cervical spine ("hangman's fracture” of C2) and transection of the spinal cord.
-Cervical injuries in non-judicial hangings are rare. [2] One retrospective case review of near-hangings over a 10-year period found the incidence of cervical spine fracture to be as low as 5%. [3]
Vascular:
The major pathologic mechanism of death in hanging/strangulation is neck vessel occlusion, not airway obstruction. [1,4] Death ultimately results from cerebral hypoxia and global ischemia. The most implicated cause of death is venous obstruction. Obstruction of venous outflow from the brain leads to stagnant hypoxia and loss of consciousness in as little as 15 seconds. The risk of damage to the major arterial blood flow to the brain (such as carotid artery dissection) is rare, but should evaluated in patients. [4]
Cardiac:
Carotid body reflex-mediated cardiac dysrhythmias are reported and may account for a minor mechanism of death.
Pulmonary:
-Airway compromise plays less of a role in the immediate death of complete hanging/strangulation. However, it is a major cause of delayed mortality in near-hanging victims. [1,4] Airway edema can occur from mechanical trauma to the airway, which can make intubation difficult. Tracheal stenosis can develop later in the hospital course. The hyoid bone can fracture, and injuries to the cricoid or thyroid cartilage can also occur. [5]
-Significant pulmonary edema occurs through two mechanisms:
1) Neurogenic: centrally mediated, massive sympathetic discharge; often in association with serious brain injury.
2) Post-obstructive: strangulation causes marked negative intrapleural pressure, generated by forceful inspiratory effort against extra-thoracic obstruction; when the obstruction is removed, there is a rapid onset pulmonary edema leading to ARDS.
-Aspiration pneumonitis/pneumonia can cause later sequela of near-hanging injury.
Physical Examination
-"Ligature marks" or abrasions, lacerations, contusions, bruising, edema of the neck
-Tardieu spots (petechiae/ecchymoses) of skin or eyes
-Severe pain on gentle palpation of the larynx (laryngeal fracture)
-Respiratory signs: cough, stridor, dysphonia/muffled voice, aphonia
-Varying levels of respiratory distress
-Hypoxemia
-Mental status changes
Early Management/Stabilization
-Patients should be activated per their physiology and suspected injuries, which will most often be a full trauma
-Evaluate ABCs as always (primary and secondary survey per ATLS protocol)
-Routine immobilization of the cervical spine is recommended
-Patients who have symptoms such as odynophagia, hoarseness, neurologic changes, or dyspnea may require sudden emergent intubation
-Judicious and cautious fluid resuscitation - avoid large fluid volume resuscitation and consider early pressors, as fluids increase the risk/severity of ARDS and cerebral edema
-Monitor for cardiac arrhythmias
-Comatose patients should be assumed to have cerebral edema with elevated ICP and medically managed as such
-Non-intubated patients with pulmonary edema may benefit from noninvasive positive end-expiratory pressure ventilation
-Patients with symptoms of laryngeal or tracheal injury (e.g. dyspnea, dysphonia, aphonia, or odynophagia), should undergo laryngobronchoscopy with ENT [4,6]
Imaging
- Chest x-ray
- Non-contrast CT Head
- CT C-spine
- CTA neck and Head
- Can consider additional CTs (i.e. Trauma “pan scan”) if patient is unconscious, physical exams warrants, or history is concerning for additional injuries or if history is uncertain
Disposition
Trauma should be the admitting service to the appropriate level of care:
-Admit critically ill patients to the ICU with either CCS or PCCM consultation
-Admit patients without ICU needs to the Trauma service
-Even if the initial presentation is clinically benign, all near-hanging victims should be observed for 24 hours, given the potential risk of delayed neurologic, airway, and pulmonary complications [7, 8]
-Psychiatry consult on all suspected intentional cases
-Emphasize strict return precautions as well as education about possible delayed respiratory and neurologic dysfunction when discharging patients
Author and last update
Abby Josef, MD, February 2026
References
1. Walls RM, Hockberger RS, Gausche-Hill M. Rosen's emergency medicine: concepts and clinical practice. Ninth edition. ed. Philadelphia, PA: Elsevier; 2018.
2. Aufderheide TP, Aprahamian C, Mateer JR, et al. Emergency airway management in hanging victims. Ann Emerg Med. 1994;24(5):879-884.
3. Salim A, Martin M, Sangthong B, Brown C, Rhee P, Demetriades D. Near-hanging injuries: a 10-year experience. Injury. 2006;37(5):435-439.
4. Tintinalli JE, Stapczynski JS, Ma OJ, Yealy DM, Meckler GD, Cline DM. Tintinalli's emergency medicine: a comprehensive study guide. 9th. ed. New York: McGraw-Hill Education; 2019.
5. Tugaleva E, Gorassini DR, Shkrum MJ. Retrospective Analysis of Hanging Deaths in Ontario. J Forensic Sci. 2016;61(6):1498-1507.
6. Hackett AM, Kitsko DJ. Evaluation and management of pediatric near-hanging injury. Int J Pediatr Otorhinolaryngol. 2013;77(11):1899-1901.
7. McHugh TP, Stout M. Near-hanging injury. Ann Emerg Med. 1983;12(12):774-776.
8. Balaji Kannamani, Neeru Sahni, Anjishnujit Bandyopadhyay, Vikas Saini, Laxmi Narayana Yaddanapudi. Insights into pathophysiology, management, and outcomes of near-hanging patients: A narrative review. J Anaesthesiol Clin Pharmacol. 2024 Oct-Dec;40(4):582-587.
Management of the Pregnant Trauma Patient
Purpose:
Pregnancy alters baseline physiology and anatomy. These changes can influence the evaluation of a traumatically injured pregnant patient. The signs and symptoms of injury can be confusing. The pregnant patient has abnormal baseline laboratory values. There are special considerations in the approach and response to resuscitation. While there are two patients – mother and fetus, the initial treatment priorities are the same, focusing on the optimal treatment of the mother. To provide safe care to the pregnant trauma patient, a collaborative effort between Emergency Medicine, the Trauma Service and the Department of Maternal Fetal Medicine should occur.
Policy Statement:
This guideline is a supplement to and is to be used in conjunction with the policy Trauma Team Activations (TTA01).
Non-trauma activated/minor trauma patients > 20 weeks seen in the Emergency Department (ED) by Emergency Medicine should have an OB consult within 1 hour of presentation to the ED even for minor trauma.
All pregnant trauma patients will be evaluated in an organized fashion whether they be evaluated in the ED, on the floor, or in Labor and Delivery. Obstetrics, including Maternal Fetal Medicine, is available to consult on any pregnant patient <20 weeks at any time to discuss medication risks or risk of surgery in pregnancy. Additionally, if a pregnant trauma patient at any gestational age cannot be bedded on the trauma floor, contact Labor and Delivery.

References
-
1. American College of Surgeons Committee on Trauma. (2025). ATLS, Advanced Trauma Life Support: Student Course Manual. 11th ed. American College of Surgeons.
Author(s)
- Acute Care Surgery/Trauma Leadership
- Emergency Medicine Leadership
- Maternal Fetal Medicine Division Leadership
Last Updated
February, 2026
Massive Transfusion for Trauma Protocol
Purpose
Hemorrhage is the leading cause of early death following traumatic injury. Protocol-driven transfusion strategies that approach a 1:1:1 ratio in patients who require massive transfusion improve patient survival, reduce hospital and ICU length of stay, decrease ventilator days, and ultimately reduce patient care costs.
These guidelines are meant to standardize the approach to resuscitation of an injured patient in hemorrhagic shock utilizing massive transfusion.
This guideline is a supplement to and is to be used in conjunction with Nebraska Medicine’s organizational policies “Massive Transfusion/Severe Coagulopathy” (TX-36) and “Guidelines for Management in Patients Receiving Anticoagulation” (MP 11).
Background/Definitions
Massive transfusion may be defined as transfusion in response to massive and uncontrolled hemorrhage resulting in any of the following:
- Replacement of half of a patient’s total blood volume in a 4 hour period
- Replacement of a patient’s total blood volume within 24 hours
- Transfusion of >10 units of PRBCs in 24 hours
- Specific pediatric parameters are more challenging to define and include transfusion of >40mL/kg PRBCs in a short period of time.
Hemorrhage is the most common cause of death within the first hour of arrival to a trauma center. Blood product resuscitation, specifically massive transfusions, are often unplanned and require the processing and delivery of large amounts of blood products rapidly for a sustained period of time, significant preplanning and coordination between the blood bank, resuscitating unit (i.e. emergency department, operating room, intensive care unit) and pharmacy is required. The initiation of a massive transfusion protocol (MTP) outlines a standard process for the safe, rapid preparation and delivery of blood products and coagulation factors for the pediatric patient experiencing massive hemorrhage. Additionally, implementation of a standardized guideline may prevent the anticipated complications of massive transfusion including thrombocytopenia, coagulopathies, electrolyte and acid/base disturbances, hypothermia and transfusion reactions as well as utilize valuable blood components in a resourceful manner.
At Nebraska Medicine, the massive transfusion protocol is divided into 3 categories based on the patient’s weight with each pack within that category containing the following blood product components.
|
MTP type |
Packed Red Blood Cells (PRBC) |
Thawed Plasma (FFP) |
Apheresis Platelets |
Pre-pooled cryoprecipitate (cryo) |
|
Adult (> 40 kg) |
6 (O pos) |
6 (A) |
1 |
On pack #3 and every pack thereafter |
|
Pediatric (10-40kg) |
6 (O pos) |
6 (a) |
1 |
On pack #3 and every pack thereafter |
|
Neonate/Infant (<10 kg) |
1 (O neg, irradiated) |
|
1 (irradiated) |
|
Guideline Inclusion Criteria
Injured patients with concern for massive or uncontrolled hemorrhage.
Guideline Exclusion Criteria
This is a guideline only. Individual circumstances need to be considered, as there may be times when it is appropriate to deviate from this guideline.
Diagnostic Evaluation
Injured patients should be assessed per ATLS guidelines paying close attention to circulation. Presence or history of hemodynamic instability, poor perfusion and external blood loss are red flags for hemorrhage. Signs of hemodynamic instability or poor perfusion may include altered mental status, pallor, delayed capillary refill, tachycardia, and hypotension. Hypotension is often a late sign of hypovolemic/hemorrhagic shock.
Practice Recommendations for Management
Initiation and Activation
- The decision to activate MTP is a clinical decision made by the trauma or emergency medicine attending physician and should be strongly considered with one or more of the following criteria:
-
- Persistent hemodynamic instability
- Shock Index >1 (SI = HR/SBP)
- Active bleeding requiring operation or angioembolization
- Blood transfusion in the Trauma Bay
- Adult patients (>40 kg)--Anticipated of transfusion of >10 units PRBC in 24 hrs or >4 units in 1 hr.
- Pediatric patients (≤40kg) -- Anticipated or actual use of ≥ 40 mL/kg PRBCs in 2 hours or replacement of total blood volume (approximately ≥ 80 mL/kg) in 24 hrs
- Assessment of blood consumption (ABC) score is ≥2 (adults only):
-
- Penetrating mechanism of injury (1pt)
- Systolic blood pressure less than or equal to 90 mm Hg (1pt)
- Heart rate greater than or equal to 120 (1pt)
- Positive FAST exam (1pt)
-
-
- Initiation of MTP should not be delayed for lab results.
-
- Universally compatible RBC (O Rh-negative) and thawed plasma may be given.
-
- Emergency release blood should be utilized as indicated until MTP blood products are available.
-
- Whole blood is preferred in the initial resuscitation of hemorrhagic shock in patients age 6 and older.
-
- 4 units of whole blood (O positive) are available for trauma resuscitations in the emergency department (ED) and can be found in the ED trauma bay kiosk refrigerator pending inventory availability.
- Use of whole blood in pediatric patients age 6-12 years of age should be limited to 1 unit due to potential risk of hemolysis.
-
- Emergency release blood is located in the following locations:
-
- Emergency Department (ED) trauma bay kiosk refrigerators (2 kiosks located in T1 and T4) each containing 2 units O positive whole blood, 2 units O negative PRBC, 6 units O positive PRBCs, and 3 units A plasma
- Blood bank keeps 4 units O negative PRBC, 12 units O positive PRBC, 12 units A plasma, 8 units platelets, and 25 units pre-pooled cryoglobulin (frozen).
-
- Whole blood is preferred in the initial resuscitation of hemorrhagic shock in patients age 6 and older.
-
- To activate the MTP, the attending physician (or designee) will notify the Blood Bank via telephone (402-559-3639) that MTP is being activated and provide the following information:
-
- Caller name and title
- Caller location
- Caller contact number
- Ordering provider’s name
- Patient’s name (may be the trauma name or real name)
- Patient’s MRN
- Category of MTP being activated (adult, pediatric, neonate/infant)
- Patient’s weight (kg)
-
Blood Product Administration and Transfusion Goals
- Minimize crystalloid or colloid resuscitation to prevent dilutional coagulopathy.
- Utilize emergency release blood products until MTP products are available.
- Blood products are released in 1:1 ratios of whole units but will be administered based on the clinical status of the patient and at the discretion of the attending physician.
-
- Maintaining a 1:1:1 transfusion ration of PRBC to FFP to Platelets is recommended. (Platelets are pooled-packs thus one apheresis platelets should be transfused for every 6 units of PRBC/FFP with the exception of neonatal/infant MTP resuscitations where apheresis platelets serves as FFP and platelet components). These rations help to avoid dilutional coagulopathy and thrombocytopenia and have been associated with decreased mortality.
-
- Pediatric Patients (≤40 kg), recommended volumes include:
-
- Whole blood -- 20 mL/kg
-
- if using whole blood during pediatric MTP, utilize entire unit of whole blood with repeated boluses of 20mL/kg before moving on to blood components.
-
- PRBC – 20 mL/kg
- FFP – 20 mL/kg
- Apheresis Platelets – 5 mL/kg
- Cryoprecipitate – 0.1 unit/kg
-
- Consider cryoprecipitate if serum fibrinogen levels remain less than 150 mg/dL following FFP.
-
- Whole blood -- 20 mL/kg
-
- Massive transfusion products should be administered rapidly and warmed via a rapid infuser with the exception of platelets
-
- For pediatric patients requiring smaller volumes, a “push-pull” system with 60mL syringe, stop-cock, and tubing may be utilized.
-
- Initial rate of transfusion should restore perfusion but allow permissive hypotension until bleeding has been controlled in the operating room or interventional radiology.
- Blood product resuscitation should be based on clinical evidence of ongoing bleeding in addition to quantitative data, such as ROTEM when available.
- Utilization of the patient’s own blood when safe (i.e. cell saver, autotransfusion from chest tube, etc) also provides readily available warm, matched blood.
Therapeutic Adjuncts in MTP
Tranexamic Acid (TXA)
- TXA is an antifibrinolytic used to treat coagulopathy. TXA should be initiated early in the coagulopathic cascade – within the first 3 hours of bleeding, in order to be effective.
- TXA should be administered based on the evidence of shutdown of fibrinolysis or hyper-fibrinolysis on ROTEM and/or provider discretion.
- Recommended dosing:
-
- <12 years:
-
- Loading dose of 15 mg/kg (max dose 1000mg) intravenous administered over 10 minutes
- Maintenance infusion of 2mg/kg/hr intravenous for 8 hours (max dose 1000mg)
-
- ≥12 years/Adult Dosing:
-
- Loading dose of 1000 mg intravenous administered over 10 minutes
- Maintenance infusion of 1000 mg intravenous over 8 hours
-
- <12 years:
-
Calcium
- The rapid rate of transfusion during MTP often exceeds the liver’s capacity to metabolize citrate, leading to severe hypocalcemia. Calcium is also required by several clotting factors for activation, stabilization of thrombus formation and contractility of myocardial and smooth muscle cells. Hypocalcemia can lead to coagulopathy, myocardial depression and vasodilation—all physiologic changes that complicate the management of hemorrhagic shock. Thus, adequate calcium repletion is an important component of MTP.
- Adults (>40 kg): 3g IV calcium chloride should be administered following completion of each MTP cooler.
- Pediatric patients (≤40 kg): 20 mg/kg IV calcium chloride should be administered after every 2 rounds of PRBC/FFP
Anticoagulant Reversal
- Injured patients in hemorrhagic shock with pre-existing anticoagulant use should be reversed with the appropriate reversal agent. See “Guidelines for Management of Bleeding in Patients Receiving Anticoagulation” (MP 11) for additional details.
***Please utilize Pharmacy for any questions regarding dosage and use of therapeutic adjuncts.***
Assessment of Coagulopathy and Transfusion Targets
- Coagulopathy
-
- Recommended initial lab testing at initiation of MTP include:
-
- CBC, PT/PTT, INR, fibrinogen, ROTEM
-
- Ongoing lab testing during MTP include:
-
- CBC, PT/PTT, INR, fibrinogen, and ROTEM every 4 hrs or as clinical situation indicates.
-
- ROTEM parameters
-
- A5EXTEM <35 mm OR ML ≥ 5% (within 60 min) à give TXA
- A5EXTEM <35 mm AND A5FIBTEM <9 mm à give cryoprecipitate
- A5EXTEM <35 mm AND A5FIBTEM ≥9 mm à give platelets
- CTEXTEM >80 s AND A5FIBTEM ≥9 mm à Give PCC or plasma
- CTINTEM > 240 s AND ( CTINTEM/CTHEPTEM) > 1.25 à give protamine, if suspected heparin activity or heparin like effects
- CTINTEM > 240 s AND ( CTINTEM/CTHEPTEM) < 1.25 à give plasma
-
- Recommended initial lab testing at initiation of MTP include:
-
- Acidosis
-
- Goal: Lactic Acid < 2
- Goal: Base Deficit <4
- Ongoing lab testing: Lactic acid and arterial blood gas (ABG) to assess acid-base status every 6 hrs during MTP or as clinical situation indicates.
-
- Hypothermia
-
- Goal: 36 degrees Celsius or warmer
- All trauma patients should undergo passive external rewarming including warmed blankets and increased ambient room temperature
- Administer warm blood products
- Continuously monitor utilizing core temperature probe.
-
- Hypocalcemia
-
- Goal: ionized calcium (iCa) >1.0 mmol/L
- Ongoing testing: iCa should be monitored at initiation of MTP and after completion of each MTP cooler.
-
- Hyperkalemia
-
- Goal: potassium <5
- Ongoing lab testing: Potassium every 6 hours or as clinical situation indicates.
-
Discontinuation and Transition to Goal Directed Therapy
- Ratio-driven massive transfusion may be discontinued and transitioned to goal-directed transfusion based on laboratory findings if surgical bleeding has been controlled or there is radiographic and physiologic evidence of bleeding control after embolization.
- MTP may also be discontinued when there is recognition that further resuscitation is futile.
- Suggested values for Goal Directed Therapy:
-
- Hemoglobin ≥ 10g/dL
- Platelets >150,000/mcL
- PT <18 seconds
- PTT < 35 seconds
- INR <1.5
- Fibrinogen >180
- ROTEM
-
- Clotting time (CT) – CTIN<215 and CTEX<75
- Amplitude 5 min after CT (A5)—A5IN,EX>33
- Amplitude 10 min after CT (A10)—A10IN,EX>45
- Maximum clot firmness (MCF)—MCFIN,EX>56 and MCFFIB>5
- Maximum Lysis (ML)—MLIN,EX,FIB<7%
-
-
Outcome Measures and Guideline Adherance
All trauma massive transfusion activations will be monitored through the trauma performance improvement (PI) process. Specific indicators that will be monitored/assessed include:
- Time from initiation of MTP to infusion of the first unit PRBCs
- Time from initiation of MTP to infusion of the first unit of plasma
- Overall ration of blood product transfusion and at 2 hours
- Total blood products used from MTP activation to 24 hours
- Notifying blood bank within 1 hour of MTP termination
- Use of therapeutic adjuncts
- Complications
Related Policies:
- TX36 Massive Transfusion/Severe Coagulopathy
- MP 11 Guidelines for Management of Bleeding in Patients Receiving Anticoagulation
Key Contributors
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Abby Josef, MD | Division of Acute Care Surgery, Faculty | Author
References
- American College of Surgeons Trauma Quality Improvement Program. (2015) ACS TQIP Massive Transfusion in Trauma Guidelines. Retrieved from transfusion_guildelines.pdf (facs.org)
- American College of Surgeons Advanced Trauma Life Support, 10th Ed. 2018.
- Callcut RA, Cotton B, Mskat P, Fox EE, Wade CE, Holcomb JB, Robinson RH. (2013) Defining when to initiate massive transfusion (MT): A validation study of individual massive transfusion triggers in PROMMTT patients. J Trauma Acute Care Surg.74(1), 59-67.
- Schroll R, Swift D, Tatum D, Courch S, Heaney JB, Llado-Farulla M, Zucker S, Gill F, Brown G, Buffin N, Duchesne J. Accuracy of shock index versus ABC score to predict need for massive transfusion in trauma patients. Injury. 49(1), 15-19.
- Napolitano LM, Cohen MJ, Cotton BA, Schreiber MA, Moore EE (2013). Tranexamic acid in trauma: How we should us it? J Trauma Acute Care Surg. 74(6), 1575-1586.
- Nunez TC, Voskrensensky IV, Dossett LA, Shinal R, Dutton WD, Cotton BA. (2009) Early prediction of massive transfusion in trauma: Simple as ABC (assessment of blood consumption)? J Trauma: Injury, Infection, and Critical Care. 66, 346-352.
- Panteli M, Pountos I, Giannoudis PV. (2016) Pharmacological adjuncts to stop bleeding: Options and effectiveness. Eur J Trauma and Em Surg. 42, 303-310.
- Stettler GR, Moore EE, Nunns GR, Chandler J, Peltz E, Silliman CC, Banerjee A, Sauaia A. (2018) Rotational thromboelastometry thresholds for patients at risk for massive transfusion. J Surg Res. 228: 154-159.
- Chidester SJ, Williams N, Wang W, Groner JI. (2012) A pediatric massive transfusion protocol. J Trauma Acute Care Surg. 73(5), 1273-1277.
- Eckert MJ, Wertin TM, Tyner SD, Nelson DW, Martin MJ. (2014) Tranexamic acid administration to pediatric trauma patients in a combat setting: The pediatric trauma and tranexamic acid study (PED-TRAX). J Trauma Acute Care Surg. 77(6), 852-858.
- Neff LP, Cannon JW, Morrison JJ, Edwards MJ, Spinella PC, Borgman MA. (2015) clearly defining pediatric massive transfusion: Cutting through the fog and friction with combat data. J Trauma Acute Care Surg. 78(1), 22-29.
Last updated:
May, 2024
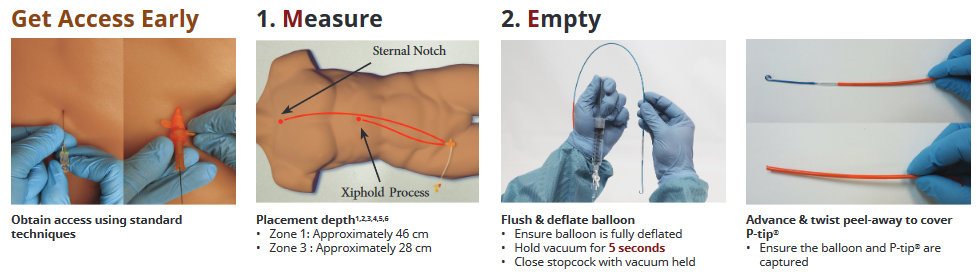
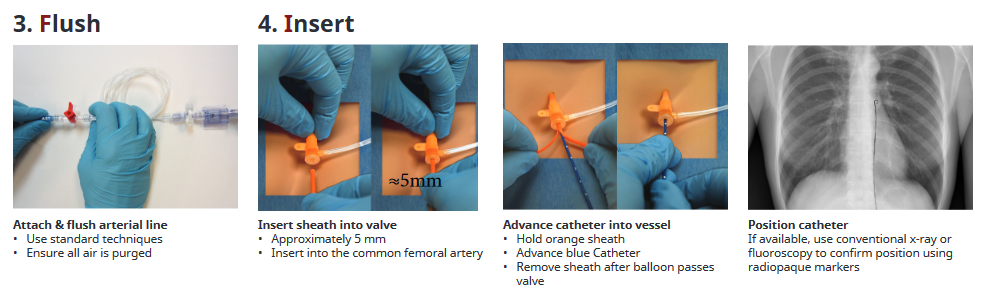
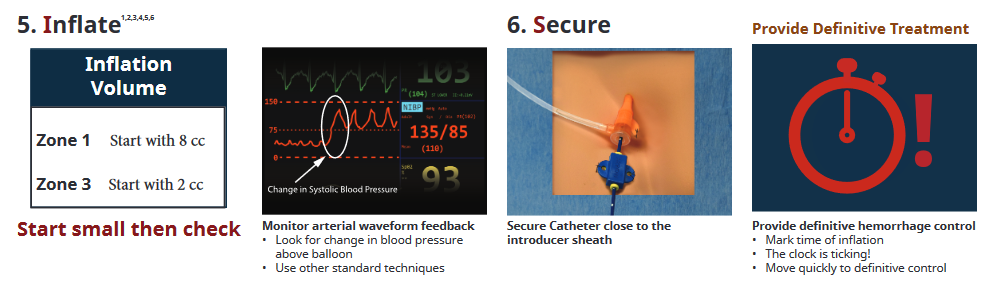
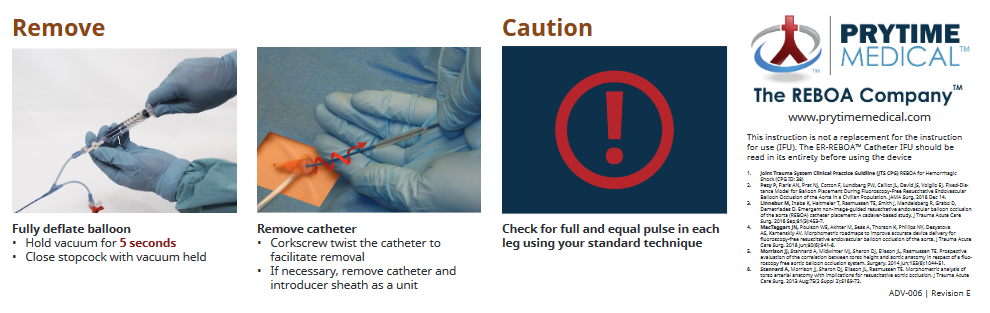
REBOA Instructions
This page is intended to serve as a quick reference for easy access to the REBOA kit instructions. The information and images are directly from the insertion instructions, and were obtained from http://prytimemedical.com/wp-content/uploads/2017/08/ER-REBOA-Catheter-Quick-Reference-Guide-wall-poster.pdf

Whole Blood Usage in Trauma
Purpose:
The implementation of a whole blood program at Nebraska Medicine is designed to optimize our resuscitation practices for the hemorrhaging trauma patient. Whole blood, specifically Low Titer O Whole Blood (LTOWB) immediately delivers a balanced product with less preservative than individual components. It also has the advantage of being more convenient by giving one product instead of three to achieve a balanced transfusion ratio. The goal of this document is to standardize the management of resuscitation with LTOWB for hemorrhagic shock from a traumatic mechanism.
Definitions:
Low Titer O Whole Blood (LTOWB): a complete blood product that contains Type O red blood cells, plasma and platelets. It contains low levels of antibodies making it safe to transfuse to a patient with any blood type. Additionally, LTOWB contains less preservative than its respective components.
Protocol:
1. This protocol may be initiated in the Trauma Bay in the Emergency Department of Nebraska Medicine for trauma patients only
2. Whole Blood transfusion can only be activated by the attending physician or their surrogate
3. Patients who meet the following criteria are eligible to receive LTOWB
a. Patient is a male or female 6 years of age or older
b. Patient has significant and potentially life-threatening bleeding
c. Anticipated need for massive transfusion protocol (MTP)
4. Once a patient has been deemed eligible and the decision to transfuse LTOWB has been made, the attending physician or their surrogate will direct the ED nurse to begin the transfusion process in accordance with the established MTP/Severe Coagulopathy/Emergency Release Blood Administration Policy (TX 36)
5. After having been deemed eligible to receive LTOWB, a patient may receive a maximum of two units
6. Once a patient receives two units of LTOWB, the MTP should proceed in the usual manner, if indicated
7. Whole blood transfusion initiated in the Trauma Bay may be continued in other patient care areas such as the operating room, interventional radiology, or the intensive care unit
8. All other aspects of transfusion should proceed per established protocols
9. No additional testing is required following administration of LTOWB as the risk of transfusion reaction and hemolysis is thought to be similar to risks associated with uncrossmatched transfusions
FAQ:
Can LTOWB be used for non-traumatic patients?
- No, not at this time. Trauma pilot will run from Nov 2021 to April 2022, then will review for utilization and cost effectiveness.
2. How do I report blood transfused?
- Report LTOWB units separately. For example: 2 u LTOWB, 5 pRBCs, 5 FFP, 1 plts
3. Turn around time after utilization of the 2 u LTOWB in the trauma bay fridge?
- About 2 weeks
4. Do I need additional labs or studies before or after giving LTOWB?
- No, just a T & S within 10 min of accessing the product
5. When does LTOWB expire?
- 3 week topic life after collection, so will be stored in fridge for 2 weeks, then reprocessed
6. Can I give more than 2 units LTOWB?
- No, the 2 units are a bridge to MTP.
Trauma Bay Adult Acute Agitation Management
Purpose:
Traumatically injured patients presenting to the emergency department (ED) experiencing acute agitation have the potential to harm themselves, hospital staff, and others. Safe and expeditious management of agitation is imperative to prevent potential further harm. However, treatment of acute agitation is challenging due to the heterogenicity of the patient population, cause or source of agitation, and the available therapeutic treatment options.
There are two critical factors that are essential to the management of agitation – early recognition and targeted intervention to the etiology driving the patient’s acutely agitated state. This treatment protocol is designed to help streamline the care of this difficult patient population.
Background/Definitions:
Acutely agitated and/or violent behaviors displayed by trauma patients interfere with the required medical care of the patient. Acute agitation is a medical emergency. Determining the cause or causes of agitation will allow for a more informed management strategy for the patient. However, because of constraints on time, limited information, and lack of patient engagement, one must assess and identify the underlying cause(s) expeditiously. The goal of acute agitation treatment is to calm the patient in the least invasive way, without causing oversedation.
Per policy TX-1, the philosophy of Nebraska Medicine is to reduce/limit the use of physical and chemical restraint while maintaining the safety and preserving dignity, rights, and wellbeing of patients. Nebraska Medicine respects the patient’s right to be free of restraints of any form that are not medically necessary. If a patient’s condition necessitates the use of restraints, the safety and wellbeing of the patient and medical staff caring for the patient is the primary focus of the medical team.
· Severe Agitation:
o Currently violent or aggressive, attacking people and/or objects.
· Moderate Agitation:
o Physically or verbally threatening, difficult to redirect, extremely active, however, not violent.
· Mild Agitation:
o Signs of overt physical or verbal activity but redirectable.
· De-escalation:
o A combination of both verbal and nonverbal strategies intended to calm the patient down to cooperate with their care.
· Sedation and Analgesia:
o Use of pharmacologic agents to create a drug-induced state to reduce physiologic and psychological stress to a patient undergoing medical, surgical, or diagnostic procedures.
Common Medical Causes of Acute Agitation
|
Type |
Examples |
|
Neurological |
Traumatic brain injury, intracranial hemorrhage, seizure/post-ictal, stroke, encephalopathy |
|
Infectious |
Meningitis, sepsis, urinary tract infection (elderly) |
|
Metabolic |
Electrolyte disturbance, hypoglycemia |
|
Respiratory |
Hypoxia |
|
Toxicological |
Environmental toxin, medication reaction, illicit drug use |
|
Endocrine |
Thyrotoxicosis, myxedema coma |
|
Other |
Hyper- or hypothermia, acute pain |
Practice Recommendations for Medical Management:
· De-escalation should always be attempted prior to medication management and physical restraint.
· Restraint may only be imposed to ensure the immediate physical safety of the patient, staff or others and must be discontinued as soon as safely possible, regardless of the scheduled expiration of the order.
· TX_01 will be followed if/when restraint use is required.
· Follow the management considerations, listed in the table below, using the preferred agent(s) as listed in Attachment A. Preferred agents show better clinical properties, including onset of action, efficacy, and lower incidence of adverse effects.
Management Considerations for Agitation
|
Severity of Agitation |
Preferred Route of Administration |
Dosing Considerations |
Special Populations |
|
Severe |
IV, when able IM, if IV not available |
Maximize dose of first agent used, allowing for the onset and effects of the previous dose prior to administering second dose |
Dosing adjustments may be required for elderly, renally/hepatically impaired, and/or when given medication(s) prior to arrival. Lower doses may be required when using concomitant sedating medications. |
|
Moderate |
IV, when able IM, if IV not available |
Smaller doses may be sufficient (as compared to what is required for severe agitation) If able/known, use a patient’s home regimen when patients can tolerate oral therapy. |
|
|
Mild |
PO |
If able/known, use a patient’s home regimen when patients can tolerate oral therapy. |
Attachment A – Preferred Treatment Options for Acute Agitation (Trauma Bay)
Preferred Treatment Options: *
|
Preferred Options |
Medication |
Dose |
Soft Max (Single Dose) |
Onset |
Time to Peak |
Duration |
Patient Considerations |
|
Midazolam |
2-5 mg IV |
5 mg IV |
IV: 1-5 min |
IV: 3-5 min |
IV: 1-2 hours |
Hypotension with larger doses (IV). Delayed onset of action (IM). |
|
|
5-10 mg IM |
10 mg IM |
IM: 15 min |
IM: 30-60 min |
IM: 1-2 hours |
|||
|
Olanzapine |
2.5-5 mg IV |
5 mg IV |
IV: 5-10 min |
15-45 min |
2 hours |
Possible hypotension and respiratory depression with IV use. Caution when used with benzodiazepines due to risk of over-sedation. MAX 30 mg/24 hrs (Cumulative for all routes of administration) |
|
|
10 mg IM |
10 mg IM |
IM: 15 min |
|||||
|
Haloperidol |
5 mg IV/IM |
5 mg |
IV: 3-20 min |
IV: 30 min |
2-4 hours |
Risk of EKG changes Can lower seizure threshold |
|
|
IM: 15 min |
IM: 20-30 min |
||||||
|
Dexmedetomidine |
0.1-0.7 mcg/kg/hr IV, titrate to response |
MAX rate 0.7 mcg/kg/hr IV |
5-15 min |
60 min |
60-240 min (Dose dependent, after drip stopped) |
Restricted for Use in Non-Intubated Patients. Only approved indication is refractory agitated delirium unresponsive to other pharmacologic agents or with contraindications to other pharmacologic agents. Only available with IV access. Can cause bradycardia. Bolus dosing not allowed outside of OR. Restricted to ED, ICU, and OR use only. |
*Subject to drug availability/restrictions secondary to national drug shortage
Management Considerations for Ketamine:
At Nebraska Medicine, ketamine is restricted to the following indications:
· Induction for rapid sequence intubation
· Ventilator management
· Procedural sedation
· Subanesthetic analgesia (restricted ordering to anesthesiology, pain management, emergency medicine, and pediatric critical care medicine)
If ketamine is required for the use of acute agitation, the institutional policy, MS_15 for procedural sedation or MP_33 for subanesthetic ketamine for pain management, will need to be followed. A provider must remain at bedside.
Dosing recommendations:
· Sub-Anesthetic Ketamine for Pain
o Must be ordered by emergency medicine provider (while patient is in the ED).
o Use dosing recommendations per MP_33
· Procedural Sedation
|
Dose |
Soft Max (Single Dose) |
Onset |
Time to Peak |
Duration |
|
0.5 mg/kg IV |
1 mg/kg |
30-60 sec |
5-10 min |
1-2 hours (recovery) |
|
2 mg/kg IM |
3 mg/kg IM |
3-4 min |
5-30 min |
3-4 hours (recovery) |
· (MS_15) Medical Staff: Procedural Sedation and Analgesia Administration Guidelines (Non-Anesthesiology Providers)
· (TX_01) Care of Patients: Restraint Use
o Attachment A: Alternative Interventions to Restraints
· (TX_24) Admission, Transfer and Discharge for Define Levels of Care
· (MP_33) Medication Policy and Guidelines: Low-Dose (Sub-anesthetic) Ketamine for Pain in Non-Intubated Patients
Key Contributors:
· Krysta Baack, PharmD | Department of Pharmacy, Emergency Medicine | Principal Author
· Nathan Sutera, PharmD | Department of Pharmacy, Psychiatric Emergency Services | Author
· Zach Bauman, DO | Division of Acute Care Surgery, Faculty | Author
Last Updated:
July 2024
References:
1. Roppolo LP, Morris DW, Khan F, et al. Improving the management of acutely agitated patients in the emergency department through implementation of Project BETA (Best Practices in the Evaluation and Treatment of Agitation). JACEP Open 2020; 1:898-907.
2. Zareifopoulos N and Panayiotakopoulos G. Treatment options for acute agitation in psychiatric patients: theoretical and empirical evidence. Cureus 2019; 11(11): e6152.
3. Curry A, Malas N, Mroczkowski M, et al. Updates in the assessment and management of agitation. Focus (Am Psychiatr Publ) 2023; 21(1): 35-45.
4. Lexicomp. (2024). Midazolam: dosage & administration. In Lexi-Drugs Online. Retrieved [June 27, 2024.] from https://online.lexi.com.
5. Lexicomp. (2024). Olanzapine: dosage & administration. In Lexi-Drugs Online. Retrieved [June 27, 2024.] from https://online.lexi.com.
6. Lexicomp. (2024). Haloperidol: dosage & administration. In Lexi-Drugs Online. Retrieved [June 27, 2024.] from https://online.lexi.com.
7. Lexicomp. (2024). Dexmedetomidine: dosage & administration. In Lexi-Drugs Online. Retrieved [June 27, 2024.] from https://online.lexi.com.
8. Lexicomp. (2024). Droperidol: dosage & administration. In Lexi-Drugs Online. Retrieved [June 27, 2024.] from https://online.lexi.com.
9. Lexicomp. (2024). Lorazepam: dosage & administration. In Lexi-Drugs Online. Retrieved [June 27, 2024.] from https://online.lexi.com.
10. Lexicomp. (2024). Ketamine: dosage & administration. In Lexi-Drugs Online. Retrieved [June 27, 2024.] from https://online.lexi.com.
11. Li M, Martinelli AN, Oliver WD, et al. Evaluation of ketamine for excited delirium syndrome in the adult emergency department. J Emerg Med. 2019; S0736-S4679(19)30802-9.
12. O'Brien ME, Fuh L, Raja AS, et al. Reduced-dose intramuscular ketamine for severe agitation in an academic emergency department. Clin Toxicol (Phila). 2020;58(4):294-298.