3. Neurological Trauma
Educational materials and pathways regarding the evaluation and management of neurological injuries.
- Cervical Spine Evaluation and Management
- Intracranial Hypertension Management Algorithm
- Management of Traumatic Brain Injury
- Modified Brain Injury Guidelines (mBIG)
- Pharmaceutical Management of Post-TBI Neuropsychiatric Symptoms
- Initial Assessment and Management of Spine Injury
- Transverse and Spinous Process Fractures
- Care of Patients with Spinal Cord Injuries Practice Guideline
Cervical Spine Evaluation and Management
Cervical Spine Evaluation and Management
Purpose: Although cervical spine injuries are relatively uncommon among all trauma patients presenting to emergency departments (approximately 1-3%), cervical spine fractures and associated spinal cord or blunt cerebrovascular injuries can be potentially devastating to an individual. These guidelines serve to provide our trauma patients with an efficient and thorough evaluation of the cervical spine with either clearance of c-spine precautions or appropriate intervention and treatment of injuries when identified.
C-spine Precautions:
I. Who needs C-spine precautions?
a. All blunt trauma patients should be placed in c-spine precautions until the cervical spine can be appropriately evaluated and cleared.
b. Penetrating trauma patients do not need to be placed in c-spine precautions unless there is other associated blunt trauma or they are unevaluable and blunt force trauma cannot be excluded.
II. “C-spine precautions” includes:
a. Bedrest (until remainder of spine can be cleared/evaluated)
b. Head flat (in a neutral position)
c. C-spine immobilization in a rigid cervical collar (Philadelphia collar or Miami-J) at all times
d. Transport flat or in reverse Trendelenburg on a gurney
III. In low risk patients, after T&L spines have been cleared, the Trauma Attending or Fellow may use his/her judgement and write the c-spine precautions order to include “HOB may be 30 degrees up.”
C-Spine Evaluation and Clearance of Cervical Collar:
I. Routine c-spine clearance includes imaging of the cervical spine COMBINED WITH a clinical exam of the cervical spine.
a. A CT c-spine is the preferred imaging modality for evaluation of the cervical spine if the patient is scheduled to undergo another type of CT examination.
b. If cervical spine x-rays are obtained, they must be considered adequate films which allow complete visualization of all cervical vertebra (from the skull base down to T1).
c. NEXUS CRITERIA--In patients that are a GCS 15, examinable and no further CT scans are planned, the c-collar can be cleared clinically using the National Emergency X-Radiography Utilization Study (NEXUS) criteria without additional c-spine imaging.
i. NEXUS low-risk criteria include:
1. No posterior midline cervical-spine tenderness
2. No evidence of intoxication
3. A normal level of alertness
4. No focal neurologic deficit
5. No painful distracting injuries
If ALL of these criteria are met, no additional imaging is required and the c-collar may be cleared with clinical exam alone. If any of these criteria are not met, one should proceed with CT c-spine to further evaluate for cervical spine injury.
d. Special populations:
i. Pediatric patients (15 and younger)
1. If the child is awake/alert and examinable, the cervical spine should be attempted to be cleared with NEXUS Criteria.
2. If the child is obtaining CT scans for work-up of other injuries, obtain a CT c-spine.
ii. Elderly patients (age 65 yrs and older)
1. Elderly patients are more likely to have cervical spine injury without associated mid-line tenderness. In patients 65 years or older, have a lower threshold to obtain CT c-spine depending on the mechanism of injury.
II. Patients with any spinal fracture should have a radiologic exam of the entire spine.
III. C-spine clearance after negative imaging tests
a. Clinically clearing the c-spine involves performing a physical examination to rule out midline pain or tenderness with palpation and range of motion (ROM).
i. First, palpate the cervical spine down the midline. If the patient denies midline pain and tenderness with palpation, the anterior half of the collar may then be removed.
ii. Next, the patient should then be given clear instructions to slowly move his/her head from side to side (without assistance) and then back to front and to stop at any time if he/she experiences any pain/discomfort. If no midline cervical spine pain is appreciated with ROM, then the c-collar may be removed.
b. Both an order and a progress note (documenting that the patient’s C-spine has been both radiographically and clinically cleared) must be written in order to clarify that the patient no longer requires c-spine precautions.
IV. Any patient with:
a. Midline cervical pain or tenderness
b. A distracting injury or competing pain
c. Intoxication (any intoxicating substance)
d. Any head injury or impaired level of consciousness
e. Focal neurologic deficit
SHOULD NOT undergo attempted clinical exam/clearance until sensorium is cleared.
V. Patients who are obtunded due to injury, intubated for a prolonged period of time or are unable/incapable of having his/her c-spine cleared clinically:
a. C-collar maybe cleared based on negative imaging (CT C-spine) alone at the discretion of the trauma attending
b. consider MRI of the c-spine within the first 72 hours of admission (if clinically stable to do so) to rule out ligamentous injury in patients sustaining poly trauma or injury secondary to high energy mechanisms. If the MRI does not demonstrate signs of ligamentous injury, the C-collar may be removed.
C-spine Injury Present or Unable to Clear C-collar:
I. Any patient with complaints of midline pain or tenderness of the c-spine should be kept in a cervical collar regardless of their radiographic exam results.
II. Negative CT c-spine but persistent pain on clinical exam.
a. A second attempt to clear the cervical collar with exam should be made 12-24 hours following the initial attempt.
b. If still unable to clear a patient’s c-spine:
i. The patient should be instructed to wear the collar for 2 weeks and follow-up in Spine clinic for repeat evaluation and clearance of precautions. This has been approved by Drs. Wilson (Neurosurgery) and Vincent (Ortho Spine).
ii. Consider MRI c-spine in special populations such as elderly where the presence of a c-collar may result in significant dysphagia or impair balance or mobility. This should be discussed with the trauma attending prior to obtaining.
III. Any patient with a c-spine injury noted on imaging or has neurologic deficits present on exam should be maintained in c-spine precautions and receive a formal spine surgery consult (either neurosurgery or orthopedic spine service).
a. If other spine injuries are present, the consulting spine team will be responsible for clearance of the cervical spine.
b. Patients with any cervical or > 3 thoracic/lumbar isolated transverse process or spinous process fractures should receive spine consultation.
IV. Some cervical spine fractures are associated with increased risk of blunt cerebrovascular injury (BCVI) and should be investigated with a CTA neck. Risk factors for BCVI are high energy transfer mechanisms associated with:
a. Displaced mid-face fracture (LeForte II or III)
b. Basilar skull fracture involving carotid canal
c. Closed head injury consistent with diffuse axonal injury and GCS <6
d. Cervical body fracture or transverse foramen fracture, subluxation or ligamentous injury at any level
e. Cervical fractures, at any level
f. Near hanging with cerebral anoxia
g. Clothesline type injury or seatbelt abrasion (sign) with significant swelling, pain or altered mental status.
V. Patients who require a c-collar for extended periods of time are at risk for skin breakdown and pressure wounds.
a. Mechanisms to prevent this include:
i. exchange the Philadelphia collar to a Miami-J collar
ii. ensure collar fits properly and has pads in appropriate locations
iii. consider consulting Hanger or Burton for custom fit cervical collars
iv. nursing is performing appropriate c-collar cares daily
1. cervical collar care performed q shift to assess skin for red/opened areas
2. pads should be changed daily and as needed if soiled
3. if patient is on flat bedrest, consider using ICU occipital back panel with Vista collar to reduce skin breakdown
REFERENCES:
1. Grossman MD, Reilly PM, Gillett T, Gillett D. National survey of the incidence of cervical spine injury and approach to cervical spine clearance in U.S. trauma centers. J Trauma. 1999; 47(4):684-90.
2. Hoffman JR, Mower WR, Wolfson AB, Todd KH, Zucker MI. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. National Emergency X-Radiography Utilization Group. N Engl J Med. 2000; 343(2):94-9.
3. Inaba K, Byerly S, Bush LD, Martin MJ, Martin DT, Peck KA, et al. Cervical Spinal Clearance: A Prospective Western Trauma Association Multi-Institutional Trial. J Trauma Acute Care Surg. 2016; 81(6):1122-30.
4. Ciesla DJ, Shatz DV, Moore EE, Sava J, Martin M, Brown CVR, Alam HB, Vercruysse G, Brasel K, Inaba K. Western Trauma Association critical decisions in trauma: cervical spine clearance in trauma patients. J Trauma Acute Care Surg. 2020;88(2):352-54.
5. Biffl WL, Cothren CC, Moore EE, Kozar R, Cocanour C, Davis JW, McIntyre RC, Jr., West MA, Moore FA. Western Trauma Association critical decisions in trauma: screening for and treatment of blunt cerebrovascular injuries. J Trauma.2009;67(6):1150-3.
6. Patel MB, Humble SS, Cullinane DC, Day MA, et al. Cervical spine collar clearance in the obtunded adult blunt trauma patient: a systematic review and practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg 2015; 78(2):430-441.
Intracranial Hypertension Management Algorithm
Management of Traumatic Brain Injury
Management of Traumatic Brain Injury
This document provides an overview of considerations and guidelines that are important in the evaluation and management of patients with traumatic brain injury (TBI). It is not intended to be used a rigid set of treatment instructions. Management of TBI must be individualized based on each patient’s clinical situation and the clinical judgment of the providers responsible for directing this aspect of patient care.
Resuscitation and Basic Physiological Goals
The following physiological parameters should be maintained as part of goal directed TBI treatment:
- Primary Parameters:
-
-
-
- Pulse Ox ≥ 90%
- PaO2 ≥ 100 mmHg
- PaCO2 35-40 mmHg
- SBP ≥ 110 mmHg and ≤ 160 mmHg
- pH 7.35-7.45
- ICP < 20 mmHg
- Temp 36.0-38.3⁰C
- Glucose ≤ 160 mg/dL
- INR ≤ 1.3
- Sodium goal
- Normonatremia (Na 135-145 mmol/L) vs permissive hypernatremia (Na 145-155 mmol/L)
-
-
-
- Secondary Parameters
-
-
- Cerebral Perfusion Pressure (CPP)
-
- Avoid aggressive use of pressors or fluids to maintain CPP > 70 mm Hg
- Avoid CPP < 60
- Pediatrics: CPP 40-50 mmHg
-
- Cerebral Perfusion Pressure (CPP)
- PbtO2 ≥ 15 mmHg
-
-
- Required monitoring/measurements in patients with severe TBI requiring mechanical ventilation
-
- Continuous SpO2 and EtCO2 monitors
- Indwelling urinary catheter to monitor UOP; may consider transition to external catheter after first 24 hrs
- Arterial catheter with continuous arterial pressure monitoring
- Hourly neurological exams
-
1. Airway Management
- Patients with a GCS < 8 should be intubated for airway protection
- Patients with a GCS < 10 should be considered for intubation.
- Intubation should be performed with in-line cervical spine immobilization.
- Rapid sequence intubation (RSI) is the preferred method.
- If clinical scenario allows, a baseline neurological exam should be obtained prior to intubation.
- Sedative and analgesic choices should favor short acting agents throughout the initial resuscitation, as temporal assessment of neurological status is critical. In general, the following agents are recommended:
- Etomidate – sedation for induction
- Succinylcholine – paralytic for induction
- Propofol – maintenance of sedation and prevention of agitation. Propofol should not be used as an induction agent in the case of trauma and is to be discontinued if its use results in persistent hypotension requiring vasopressor agents.
- Benzodiazepines – (i.e., midazolam or lorazepam) can be utilized as an initial or substitute sedative agent for propofol.
- Dexmedetomidine (Precedex)—maintenance sedation and analgesia; can also cause hypotension and bradycardia
- Fentanyl – can be used for PRN and maintenance analgesia as well as provide some sedation effects.
2. Oxygenation/Ventilation
- Avoidance of Hypoxia
- Efforts should be made to avoid hypoxia at all times as it has been shown in significantly worsen outcomes in TBI patients.
- Patients with TBI should have a pulse oximetry maintained at SpO2 ≥ 90% and an attempt for PaO2 ≥ 100 mmHg.
- Ventilation
- Hyperventilation should be intensively monitored during the initial resuscitation.
-
- Target PaCO2 is 35-40 mmHg.
- Prophylactic Hyperventilation is not recommended (PaCO2 < 25 mmHg)
- An ETCO2 monitor and serial ABGs should be used as needed to prevent profound hypocarbia or hypercarbia.
- Therapeutic hyperventilation may be necessary for brief periods when there is acute neurological deterioration that coincides with a cerebral herniation syndrome or for refractory elevations in ICP (see section on management of intracranial hypertension).
-
- Hyperventilation should be intensively monitored during the initial resuscitation.
3. Blood Pressure, Volume Resuscitation
- Blood Pressure
- Systolic blood pressure (SBP) and mean arterial pressure (MAP) readings should be recorded from a functioning arterial line, when present, or from non-invasive blood pressure (NIBP) cuff when arterial line is not present or presumed inaccurate.
- Strict blood pressure monitoring and control is required in all TBI patients with care taken to avoid hypotension and hypertension.
-
- Any patient with intra-cranial hypertension must have an arterial line.
- SBP should be kept between 110 mmHg and 160 mmHg for the first 7 days following injury or until discharge if patient discharged prior to 7 days.
-
- it should be noted that even one episode of hypotension (SBP<100mmHg) can significantly worsen outcomes in TBI patients.
-
- It should be recognized that lower blood pressures can represent a “relative” hypotensive state in TBI patients (especially with elevated ICP)
- Normal saline, PRBC, and FFP (when needed) should be used as the initial method of maintaining euvolemia to achieve the target blood pressure
- Use of vasopressors should be considered for treatment of refractory hypotension ONLY AFTER appropriate volume resuscitation has been given.
- Vasopressors and Inotropes including phenylephrine, norepinephrine, epinephrine, dobutamine, dopamine, and vasopressin should not be used to counteract the hemodynamic effects of propofol, Precedex or other sedating medications.
- Labetalol or hydralazine as needed should be administered to treat SBP > 160 mmHg during the initial resuscitation phases.
- If SBP > 160 mmHg is sustained, consider initiation of nicardipine gtt and/or scheduled beta blocker therapy and placement of arterial line, if not already present.
- Review home medication lists and consider resuming anti-hypertensive medications as clinically indicated.
-
- Euvolemia
- The primary target is euvolemia through resuscitation. In many cases, a bedside point of care ultrasound (POCUS) with evaluation of the IVC and cardiac function can give the clinician a reasonable assessment of volume status.
- Avoid use of hypotonic fluids for volume resuscitation and maintenance fluid support.
4. Anemia and Coagulopathy
- Hematologic and coagulation panels (CBC, PT/INR, PTT, TEG, fibrinogen, anti-Xa levels, platelet mapping) should be followed closely, particularly in patients on anti-coagulation medications or pre-existing bleeding dyscrasias.
- Patients on anti-coagulant or anti-platelet medications or those with bleeding disorders should be reversed/corrected as clinically indicated to correct coagulopathy regardless of need for surgical intervention. Potential interventions include the following: FFP, vitamin K, prothrombin complex concentrate (PCC)/KCentra, platelets, DDAVP, and NOAC specific reversal agents.
-
- For patients on antiplatelet medications (i.e. aspirin, Plavix, brilinta), 1 unit of platelets may be transfused if requested by Neurosurgery at the discretion of the trauma or surgical ICU attending. Decision to transfuse additional units of platelets should be based on results of TEG or platelet mapping.
-
- Target coagulation parameters:
-
- Hb > 7 g/dL
- Platelet count > 100 x 103/uL (if clinically feasible)
- INR ≤ 1.5
- Fibrinogen > 150 mg/dL
-
- INR and platelet count should be corrected in anticipation of operative intervention or bedside procedure such as placement of ICP monitor.
5. Imaging
- All patients with suspected or at high risk for possible TBI (i.e., LOC, significant mechanism, amnesia to event, use of anticoagulant/antiplatelet medications) must undergo urgent CT head (CTH) during the initial resuscitation barring need for emergent operative intervention for other life-threatening injuries.
- Repeat CT head will also be obtained at a specified time interval, per neurosurgery recommendations. (within 24 hours of presentation and/or with any significant deterioration in patient’s neurologic status). Additional CT scans will be obtained as needed based on patient clinical condition.
- MRI brain scans should be utilized for assessment of ischemic CVA, DAI, tumors/masses or per certain research protocols. MRI brain can also be used to help prognosticate/determine potential for neurologic viability, particularly in patients with persistent vegetative states. Discussion between Neurosurgery, Neurology, and Trauma can help determine timing and value of the MRI.
6. Sedation and Analgesia for intubated TBI patients
- Sedation and analgesia agents will be chose and titrated at the discretion of the surgical ICU attending’s discretion
-
- Propofol – maintenance of sedation and prevention of agitation. Propofol should not be used as an induction agent in the case of trauma and is to be discontinued if its use results in persistent hypotension requiring vasopressor agents.
- Benzodiazepines – (i.e., midazolam or lorazepam) can be utilized as an initial or substitute sedative agent for propofol.
- Dexmedetomidine (Precedex)—maintenance sedation and analgesia; can also cause hypotension and bradycardia
- Fentanyl/Dilaudid – can be used for PRN and maintenance analgesia as well as provide some sedation effects.
-
- Ideally, initial agents chosen should favor shorter acting agents so that serial neurologic exams can be obtained.
- In general, sedation will be titrated to RASS goal 0 to -2 unless deeper sedation deemed medically necessary by the surgical ICU attending. (i.e. intracranial hypertension, post-traumatic seizures, etc.)
-
- If ICP monitor in place, sedation should be titrated to maintain ICP < 20 mm Hg.
-
Intracranial Pressure (ICP) Monitoring
- Placement of ICP monitoring should be considered in the following:
-
- In patients with a salvageable traumatic brain injury (TBI) if the GCS is </= 8 following the initial resuscitation and the admission CT scan of the brain is abnormal (i.e., hematomas, contusions, edema, herniation or compressed basal cisterns).
- Patients undergoing emergent surgical procedures (orthopedic interventions, exploratory laparotomy, etc.) in whom a moderate to severe brain injury is suspected (GCS 3-12) to help guide appropriate intraoperative ICP management.
- Patients with a normal admission CT scan of the brain but have two or more of the following criteria,
-
-
- Age >40 y/o
- Unilateral or bilateral motor posturing
- Documented episode of hypotension (SBP<90mm Hg)
-
-
-
- ICP monitors may include an intraventricular catheter (EVD) and/or parenchymal monitor (Bolt).
-
- Patients with suspected increase in intracranial pressure and GCS ≤ 8 should receive an intraventricular catheter (EVD) or parenchymal monitor at the discretion of the treating Neurosurgeon as the clinical situation mandates.
-
- Ideally, ICP monitor should be placed within the first 12 hours following admission. ICP monitor placement may also occur later in the resuscitation if the patient’s clinical status declines/changes so that ICP monitoring is now warranted.
- Relative contraindications to ICP monitor placement:
-
- The brain injury is not felt to be salvageable/survivable.
- Coagulopathy (INR>1.3)
- Patient is awake/GCS ≥ 9
- Mass lesion with mass effect at the site of the ventriculostomy site
- Patient known to be post-ictal without obvious brain injury
- Metabolic causes of coma including intoxication without good evidence of head injury
-
- Removal of the ICP monitor will be at the discretion of the treating neurosurgeon but should be considered when:
-
- ICP within normal range
- 48 to 72 hours after interventions for elevated ICP.
-
- Target parameters:
-
- ICP < 20 mmHg
- Cerebral Perfusion Pressure (CCP) ≥ 60 mmHg.
-
Treatment of Intracranial Hypertension
- Intracranial hypertension is defined as sustained elevation in intracranial pressure (ICP) of more than 15 to 20 mmHg sustained for greater than 5 minutes and occurs when the three intracranial components—blood, brain, and cerebrospinal fluid (CSF)—are no longer able to compensate for volume changes occurring within the cranium.
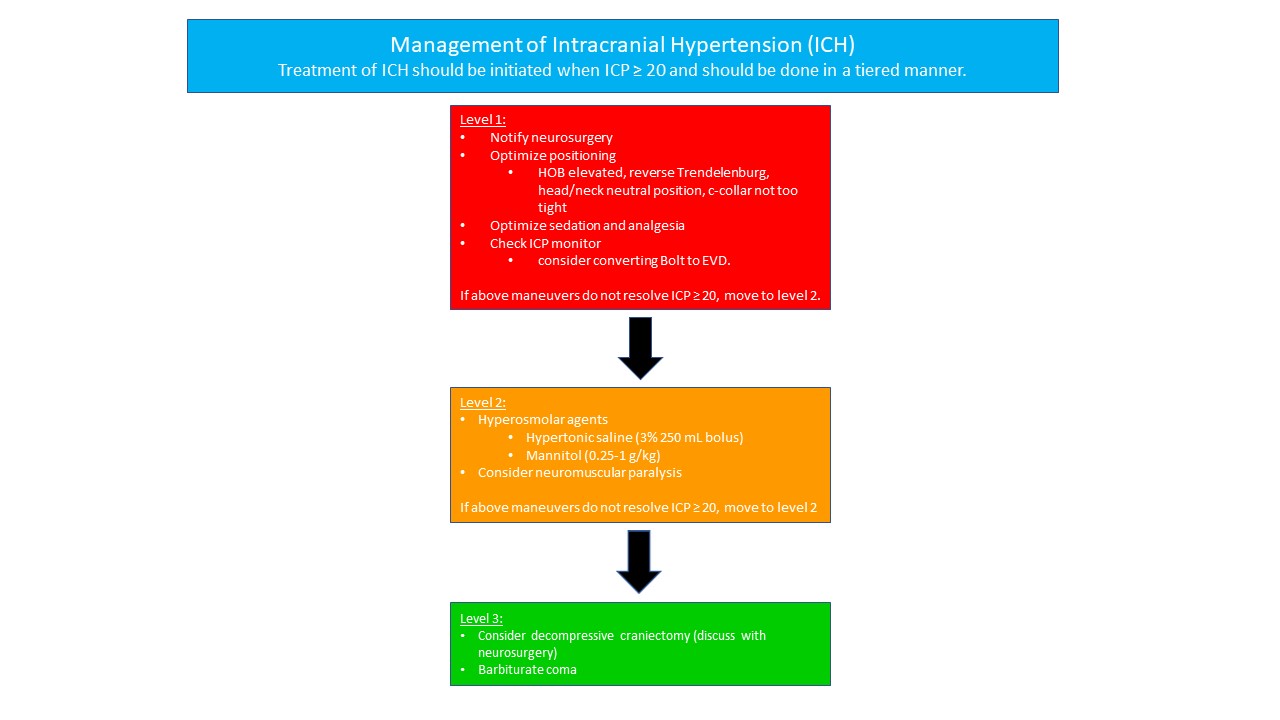
- Treatment for intracranial hypertension should be initiated when ICP ≥ 20 mmHg and is managed with a leveled algorithm with each level representing increasing levels of intensity. Patients should be initiated in Level 1, then staged through Level 3 as indicated. If the treatments in a given level have not sufficiently lowered the ICP within 20 minutes of implementation, then advancements to the next level should be promptly initiated.
-
- Level 1
- Notify Neurosurgery
- Positioning-- Elevate head of patient’s bed to ≥ 30 degrees or reverse Trendelenburg position if the T/L spine has not been cleared or there is a known fracture precluding the upright position. Maintain head and neck aligned in a midline neutral position and ensure cervical collar is not restrictively tight.
- Optimize sedation and analgesia using recommended agents (propofol, fentanyl and versed) in intubated patients.
- ICP monitor – ensure ICP monitor is functioning properly. If EVD in place, lower and/or open to drain CSF to assess patency. If parenchymal monitor in place, consider converting to EVD if situation allows.
- If the above maneuvers have not resolved the elevated ICP, move to Level 2.
- Level 2
- Hyperosmolar agents
-
- Hypertonic Saline – intermittent boluses of 3% saline (250 mL) may be given in the setting of increased ICP and is preferred if the patient has hypotension or is hypovolemic. Serum sodium and osmolality must be assessed every 6 hours and additional doses should be held if the serum sodium exceeds 160 mEq/L or serum osmolality > 360 mOsm/L
- Mannitol – intermittent boluses of mannitol (0.25-1gm/kg body weight) may also be administered Attention must be placed upon maintaining a euvolemic state as mannitol will induce an osmotic diuresis. The serum sodium and osmolality must also be assessed frequently (every 6 hrs) and additional doses should be held if the serum sodium exceeds 320 mOsm/L. Maintain a serum osm < 320 mOsm/L with a targeted serum Na of < 160 mEq/L.
-
- Neuromuscular paralysis: pharmacologic paralysis with a continuous infusion of a neuromuscular blocking agent should be considered if the above measures fail to adequately lower the ICP and restore CPP. The infusions should be titrated to maintain at least two twitches (out of a train of 4) using a peripheral nerve stimulator. Adequate sedation must be utilized if pharmacologic paralysis is employed and can be confirmed with BIS monitoring.
- If the above maneuvers have not resolved the elevated ICP, move to Level 3.
- Hyperosmolar agents
- Level 3
- CTV head should be considered to evaluate for cerebral sinus thrombosis
- Decompressive hemi-craniectomy or bilateral craniectomy should be discussed and performed at neurosurgery attending discretion.
- Barbiturate coma – an induced coma is an option for those patients who have failed to respond to aggressive measures to control malignant ICP including decompressive craniectomy. The use of BIS monitoring or equivalent is needed for assurance of adequate sedation and coma. Side effects include sudden hemodynamic collapse and a high incidence of pneumonia. Appropriate volume resuscitation and hemodynamic monitoring is mandatory. Utilizing vasopressor therapy may be warranted.
- Level 1
-
Adjunctive Medications and Prevention of Complications
- Antiseizure prophylaxis
-
- Keppra (levetiracetam) is the preferred anti-seizure medication given its lower side-effect profile, fewer drug interactions, and less need for tight monitoring of serum levels. Phenytoin/Fosphenytoin (Dilantin) also as efficacy in preventing early post-traumatic seizures in patients with TBI. Seizure prophylaxis should be considered for discontinuation after 7 days if no seizure activity occurs. However, a longer duration should be considered with certain injury patterns or in the presences of post-traumatic seizures.
-
- Stress Ulcer Prophylaxis
-
- Patients with significant TBI requiring mechanical ventilation as well as those with coagulopathies or a history of peptic ulcer disease should receive stress ulcer prophylaxis with either an H-2 block agent (famotidine) or proton pump inhibitor.
-
- Deep Venous Thrombosis (DVT) prophylaxis
-
- All patients with TBI should receive DVT prophylaxis in the form of sequential compression devices upon admission. Chemoprophylaxis (subcutaneous Lovenox or heparin) should be initiated 48 hours following injury/procedure for most intracranial hemorrhages and after craniotomy OR 24 hours following last stable CT head unless specifically requested by the neurosurgical attending. (see guidelines for VTE prophylaxis in trauma patients)
-
- Early Tracheostomy
-
- Tracheostomy within 7 days of admission is recommended in ventilator dependent patients to reduce total days of ET intubation. This is performed at the discretion of the trauma and neurosurgery services.
-
- Nutritional Support
-
- Nutritional support should be initiated via enteral route within 48 hours post injury. Frequent assessment of residual volumes of gastric nutrition should be performed, as patients with TBI frequently do not tolerate intragastric feeding and are at risk for emesis and aspiration. Efforts should be made to obtain post-pyloric feeding access (i.e. Cortrak) when possible. Consider holding tube feeds if gastric residual volumes >500 ml.
-
Surgical Management of TBI
Surgical interventions for severe TBI will ultimately be performed at the discretion of the neurosurgery attending/service. However, there are certain criteria and situations where surgery should be considered.
- Epidural hematomas
-
- An epidural hematoma (EDH) of greater than 30 cm2 should be surgically removed regardless of GCS. Patients with an acute EDH, GCS <9 and anisocoria should undergo emergent EDH evacuation.
- Continued non-operative management should be considered in posterior EDH of venous origin.
- EDH of less than 5mm midline shift in patients with GCS >8 and no focal deficit can be closely monitored in an ICU with serial CT scans. Judicious use of narcotics and sedatives is important to minimize drug related alterations in the neurologic exam. Repeat CT head should be obtained within 6 hours if patients are to be managed non-operatively.
-
- Acute Subdural Hematomas
-
- Acute subdural hematomas (SDH) with a thickness of greater than 10 mm or 5mm of midline sift on CT scan should be considered for emergent evacuation regardless of GCS. (Clinical judgement should be used in patients with significant underlying atrophy)
- A SDH less than 10mm thickness and less than 5mm midline shift should be evacuated emergently if the patient has: GCS decrease by 2 points, asymmetric or fixed pupils, or ICP > 20 mmHg.
- Repeat CT head should be obtained within 24 hours or sooner if there is deterioration in patient’s neurologic status.
-
- Subarachnoid Hemorrhage
-
- In general, subarachnoid hemorrhage (SAH) is managed non-operatively. All patients with GCS ≤ 8 and SAH should have ICP monitoring with an EVD as the preferred monitoring of choice.
- Repeat CT head should be obtained within 24 hours or sooner if there is deterioration in patient’s neurologic status.
-
- Parenchymal lesions
-
- Intraparenchymal hemorrhage (IPH) causing progressive neurological deterioration, medically refractory ICP elevations, or significant mass effect should be considered for emergent evacuation.
- Frontal or temporal contusions with IPH > 3cm3 and >5 mm shift or cistern compression in patients with GCS < 8 should be considered for surgical evacuation.
- Normal ICP should not preclude operative.
- Repeat CT head should be obtained within 24 hours or sooner if there is deterioration in patient’s neurologic status.
-
- Diffuse Medically Refractory Cerebral Edema and Intracranial Hypertension
-
- Decompressive craniectomy (unilateral or bilateral) within 48 hours of injury should be considered for patients with elevated ICP (>20) refractory to medical management.
- Ultra-early decompressive craniectomy prior to ICP monitoring is not recommended unless surgery is performed for a mass occupying lesion (hematoma) and the bone flap is not replaced.
-
- Depressed Skull Fractures
-
- Open skull fractures depressed greater than the thickness of the inner and outer table should be considered for surgical management.
- Referable symptoms attributed to the fracture site are an indication for operative management.
- Open depressed fractures that are less than 1cm depressed and have no dural penetration, no significant intracranial hematomas, no frontal sinus involvement, no gross cosmetic deformity, no pneumocephalus, and/or no gross wound contamination may be non-operatively.
- All open skull fractures should be considered for treatment with prophylactic IV antibiotics with CSF penetration.
-
References
- Brain Trauma Foundation, Guidelines for the Management of Severe TBI, 4th ed. (braintrauma.org)
- Brain Trauma Foundation, Povlishock JT, Bullock MR. Cerebral perfusion thresholds. J Neurotrauma 2007; 24: S59-S64
- Brain Trauma Foundation, Povlishock JT, Bullock MR. Hyperventilation. J Neurotrauma. 2007; 24:S87-S90
Modified Brain Injury Guidelines (mBIG)
mBIG guidelines apply only to adult trauma patients (18 yrs and older). Pediatric trauma patients (less than 18 yrs of age) are excluded from these guidelines and neurosurgical consultation should be obtained for any intracranial hemorrhage.
Modified Brain Injury Guidelines (mBIG)

Treatment Plans:
mBIG 1:
- Place in observation (2OBS) if isolated head injury, otherwise admit to appropriate level of care
- Neuro checks q2 hours (if in 2OBS), otherwise neuro checks q4 hours
- If exam stable after 6 hours in 2OBS, discharge if GCS 15
- No Keppra, no BP goals, OK to start DVT prophylaxis if not being discharged after 6 hours
- Follow-up with neurocritical care outpatient**
mBIG 2:
- Admission to SDCC if isolated head injury, otherwise admit to appropriate level of care
- Neuro checks q2 hours
- Repeat CT-head at 6 hours, OK to start DVT prophylaxis after 24 hours from stable head CT
- Neuro checks q4 hours after 24 hours observation
- Keppra 7 days, no BP goals
- Follow-up with neurocritical care outpatient**
mBIG 3:
- Neurosurgery consultation
- Follow-up with neurosurgery outpatient

Pharmaceutical Management of Post-TBI Neuropsychiatric Symptoms
Definitions
1. Depression: TBI-associated depression is characterized by prolonged, persistent sadness associated with other symptoms such as anhedonia, lack of motivation, decreased self-care, variable sleep and/or appetite pattern, feelings of hopelessness, and/or suicidal thoughts. These symptoms may last for a couple of weeks to months (major depressive episode) or persist in a milder form for two or more years (dysthymia).
2. Mania/Agitation: Subtype of delirium unique to TBI which occurs during period of Post traumatic amnesia (PTA – period of time in which new memory formation is impaired), characterized by excess of behavior that includes some combination of aggression, disinhibition, akathisia, disinhibition, and emotional liability IN ABSENCE of other physical, medical or psychiatric causes.
3. Anxiety: A wide range of anxiety disorders may occur after TBI including generalized anxiety disorder, agoraphobia, social phobia, panic disorder, and obsessive-compulsive disorder.
4. PTSD: Symptoms may include nightmares or unwanted memories of the trauma, avoidance of situations that bring back memories of the trauma, heightened reactions, anxiety, or depressed mood.
5. Psychosis: There are predominantly 2 types of TBI-related psychosis: delusional disorders and schizophrenia-like psychosis.
6. Sleep disturbance: Sleep disturbances are common after TBI and can occur in isolation or as a symptom of a psychiatric disorder. Insomnia is the most common sleep disturbance, seen in about 50% of patients with TBI, although other disturbances such as hypersomnia, sleep apnea, and sleepwalking may also be present.
7. Executive function deficits: The constellation of cognitive impairments following TBI is variable and depends on the severity of the location of the injury on the brain. TBI can affect every cognitive domain, including attention, memory, visual-spatial processing, language, social cognition, and executive functioning.
Assessment and Diagnosis
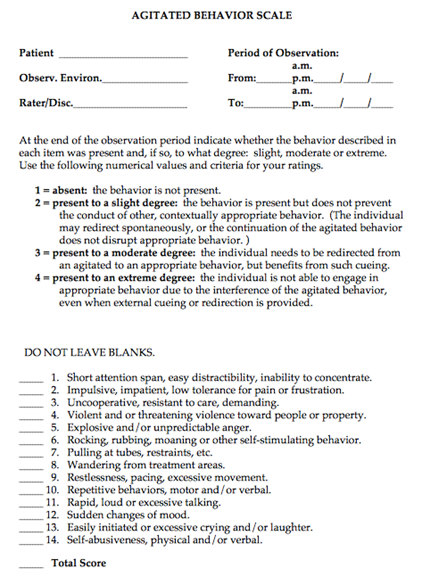
1. Mania/Agitation- Agitated Behavior Scale where 22-28 is mild agitation, 29-35 is moderate agitation, and 36-56 is severe agitation.
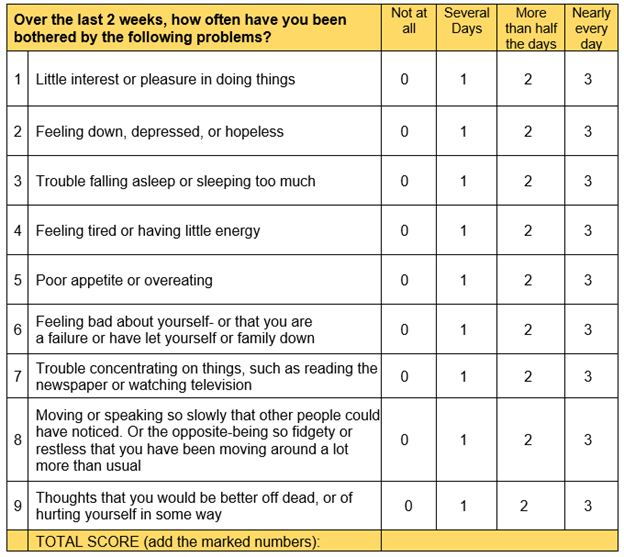
2. Depression- PHQ 9 where 1-4 is minimal depression, 5-9 is mild depression, 10-14 is moderate depression, 15-19 is moderately severe depression and 20-27 is severe depression
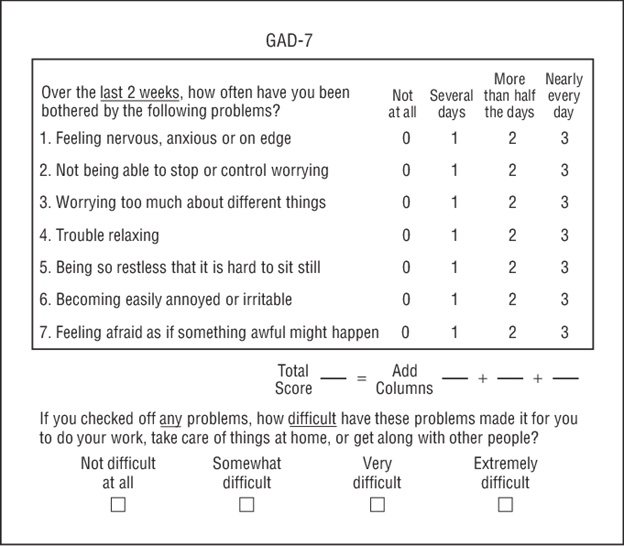
3. Anxiety: GAD-7 where 0-4 is minimal anxiety, 5-9 is mild anxiety, 10-14 is moderate anxiety, and 15-21 is severe anxiety
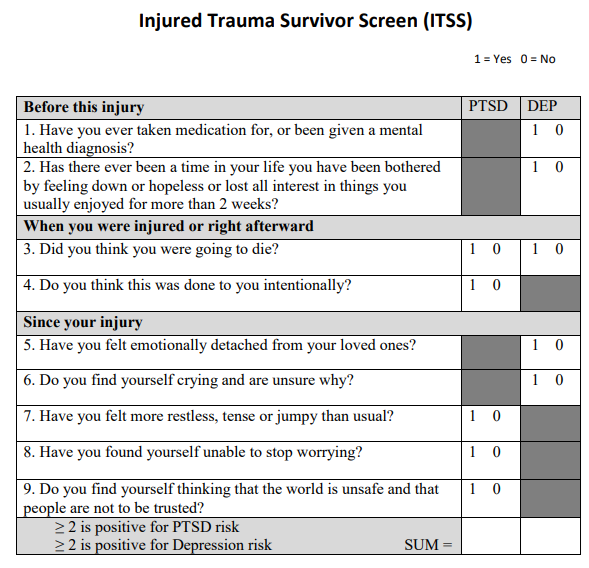
4. PTSD: ITSS where PTSD is evaluated in items 3, 4, 7, 8, 9 and Depression is evaluated in items 1, 2, 3, 5, 6. If the sum of questions 1, 2, 3, 5, and 6 is equal to or greater than 2, the screen is positive for PTSD risk. If the sum of questions 3, 4, 7, 8 and 9 is equal to or greater than 2, the screen is positive for depression risk.
5. Memory deficits, executive function deficits, and inattention: consult Speech Therapy for cognitive evaluation
Pharmacologic Management
General Considerations for all patients:
Propranolol - Patients with TBI by CT and GCS <12, hemodynamically stable at 24 hrs after admission (BP>100, not requiring vasopressor or blood transfusion) should be started on propranolol 20 mg po q12hrs . If patient develops bradycardia (HR<50 bpm) or hypotension (SBP <100mmHg), then propranolol should be stopped. Increase the dose from 20 mg BID to 40 mg BID based upon SBP>140s, and HRs> 110-120s. (Of note, if BP remains high, consider adding another agent). Propranolol should be stopped upon discharge or after 7 days, whichever is sooner.
In patients on home beta-blockers (for hypertension, heart failure, afib rate control), switch to propranolol temporarily and stop the home beta blocker (avoid ordering 2 beta blockers on the same patient). Propranolol dose can be titrated up if needed for BP or HR) or a second antihypertensive ordered.
Clonidine – has unclear role for use in TBI patients for agitation or storming. Its use as adjunct therapy in withdrawal syndromes is longstanding. It is explored for use as a transition-off agent in patients on dexmedetomidine and as an adjunct in treating PSH. Thus, practical uses for clonidine include: treating agitation in conjunction with withdrawal syndromes, treating agitation/delirium in a patient weaning off dexmedetomidine or whom dexmedetomidine was effective, 3-4th line in PSH (after gabapentin, opiates, benzos have been tried/considered). Initial dosing should be 0.1 mg PO TID. If patient is already on dexmedetomidine, the dose can be started at 0.2-0.3 mg TID and the dexmedetomidine can be decreased. Side effects include: hypotension, rebound hypertension, withdrawal.
Antipsychotics and stimulants– Generally for short-term use, should be tapered when symptoms resolve. Use assessment tools prior to initiation of pharmacologic agents to ensure you are treating the correct symptom.
All new antipsychotics and stimulants should be reviewed and weaned (if possible) at time of transfer from ICU to floor, and again, at time of discharge from hospital.
|
Assessment tool |
First line medications |
Standard dosage |
Common adverse effects |
|
|
Depression |
PHQ 9 |
Sertraline |
Start: 25 or 50 mg daily.
May double dose after 1 week, assess for effect in 4 weeks before further increasing. |
Nausea, diarrhea, sexual dysfunction |
|
Manic: acute |
Agitated Behavior Scale |
Quetiapine |
Start: 25-50 mg BID
Increase to effect to maximum of 400 mg/day |
Sedation, Parkinsonism, weight gain, QTc prolongation |
|
Mania: maintenance |
Agitated Behavior Scale |
Valproate |
Start: 250 mg TID
May load with 15 mg/kg for rapid symptom control
May increase every 2-3 days, checking level to ensure not above range |
Hepatotoxicity, hyperammonemia, thrombocytopenia, drug interaction with carbapenems
Safe therapeutic range: 50-125 mcg/mL |
|
Anxiety |
GAD-7 |
Sertraline |
Start: 25 mg daily
May double dose every 2 weeks until 100 mg daily reached. Assess in 4 weeks before further increasing. |
Nausea, diarrhea, sexual dysfunction
Low dosing to avoid worsening anxiety during initiation period |
|
PTSD |
ITSS |
Sertraline or paroxetine |
Sertraline Follow anxiety dosing
Paroxetine Start: 20 mg daily, may increase in 10 mg increments per week up to 60 mg daily. |
Nausea, diarrhea, sexual dysfunction
Paroxetine has higher sedating effect. |
|
Psychosis |
|
Risperidone or quetiapine |
Quetiapine Acute dose: 25 mg If scheduled dose indicated, same as above.
Risperidone Acute dose: 1-2 mg, up to 6 mg in 24 hours |
Parkinsonism, sedation |
|
Apathy |
|
Methylphenidate |
Start: 5 mg BID
|
Agitation, anxiety, insomnia, palpitations, tachycardia |
|
Sleep disturbance |
|
Melatonin
2nd line: Trazodone |
Melatonin 3-9 mg nightly
Trazadone 50 mg nightly |
Daytime drowsiness, sensory distortion, sleep walking |
|
Executive function deficits |
Consult Speech Therapy for cognitive evaluation |
Amantadine |
Start 100 mg BID
May increase in 50 mg increments weekly to max of 200 mg BID |
Headache, nausea, diarrhea, insomnia, orthostasis, psychosis at high doses |
|
Inattention |
Consult Speech Therapy for cognitive evaluation |
Methylphenidate |
Start: 5 mg BID, start >7-10 days post injury
|
Agitation, anxiety, insomnia, palpitations, tachycardia |
Appendix A: Agitated Behavior Scale where 22-28 is mild agitation, 29-35 is moderate agitation, and 36-56 is severe agitation.
Appendix B: PHQ 9 where 1-4 is minimal depression, 5-9 is mild depression, 10-14 is moderate depression, 15-19 is moderately severe depression and 20-27 is severe depression
Appendix C: GAD-7 where 0-4 is minimal anxiety, 5-9 is mild anxiety, 10-14 is moderate anxiety, and 15-21 is severe anxiety
Appendix D: ITSS where PTSD is evaluated in items 3, 4, 7, 8, 9 and Depression is evaluated in items 1, 2, 3, 5, 6. If the sum of questions 1, 2, 3, 5, and 6 is equal to or greater than 2, the screen is positive for PTSD risk. If the sum of questions 3, 4, 7, 8 and 9 is equal to or greater than 2, the screen is positive for depression risk.
Authors:
Charity Evans, Abby Josef Trauma and Acute Care Surgery
Becca Sedlak, Pharmacy
Last Updated: January 2024
Initial Assessment and Management of Spine Injury
Purpose
To provide an evidence-based, practical guide to the evaluation and management of an adult patient with a spinal injury, including both spinal column fracture (SCF) and spinal cord injury (SCI).
Background/Definitions
Although fractures of the spine represent a small proportion of all fractures from traumatic injury overall (incidence ranging from 4-23 percent), their impact on the individual and the healthcare system is significant due to the potential for long-term disability, associated health care consequences and costs. Additionally, the incidence of traumatic spinal injuries is expected to increase globally as the population ages. Optimal outcomes are closely related to rapid identification of injuries, early surgical intervention when necessary and early mobilization.
Guideline Inclusion Criteria
Adult Trauma patients (15 yrs and older) with spinal column fracture (SCF) and/or spinal cord injury (SCI).
Guideline Exclusion Criteria
Pediatric trauma patients (Less than 15 yrs of age)
Diagnostic Evaluation
- All trauma patients should be initially evaluated per ATLS guidelines, independent of whether an SCF or SCI is suspected or confirmed.
- Cervical and thoracolumbar spinal motion restriction (SMR) should be maintained throughout this evaluation.
-
- DO NOT use force to move the patient’s neck or thoracolumbar spine into a position that elicits pain.
- Perform examinations of the spine by log rolling the patient when necessary.
-
- Examination of the cervical, thoracic, lumbar and sacral spine should include the following:
-
- Gross inspection for abrasions, contusions, hematomas, open wounds, and obvious spinal deformities.
- Systematically palpate the entire spine to evaluate for pain, tenderness, step offs, gaps or any other deformities.
- When a SCI is suspected, perform a digital rectal exam (DRE) before rolling the patient back to the supine position.
- NOTE: physical examination of the spine has low sensitivity for injury. Level of pain and/or tenderness often do not correlate with level of injury on imaging. A normal exam has low sensitivity in ruling out spinal injuries.
-
- Imaging of the spine should be obtained in any patient that has new/acute pain on examination or new neurologic deficit following a traumatic event.
- Imaging of the spine should be considered in trauma patients who present with severe injuries at high risk for associated spinal trauma including traumatic brain injury (TBI), complex maxillofacial trauma, pelvic fractures, thoracic trauma, calcaneal fractures resulting from fall from height, and presence of seat-belt sign. Imaging the spine should also be considered with certain mechanisms of injury including high speed motor vehicle collisions (especially when associated with ejection or roll over), motorcycle/bicycle/ATV or UTV collisions, crush injuries, falls from height, or injuries leading to an axial load on the head (e.g. diving and peds vs auto).
- Age by itself, is considered a high-risk factor for spinal trauma and spinal imaging should be taken into consideration even after low-energy mechanisms such as ground level falls.
- Computed tomography (CT) of the cervical, thoracic, and lumbar spine is the preferred initial imaging modality.
Practice Recommendations for Management
- Once spine fracture is identified on imaging or if acute neurologic deficit present/SCI suspected, consult the appropriate spine surgery service (Orthopedic Spine or Neurosurgery Spine) based on call schedule.
-
- EXCEPTION: 3 or fewer isolated and unilateral transverse or spinous process fractures located in the thoracolumbar spine DO NOT require a spine consult
-
- Spine service will evaluate patient and address the following issues (if able) in consultation note:
-
- Fractures present
-
- Stable vs unstable
-
- Spinal cord injury present
-
- Level/ASIA grade
- Blood pressure goals and length of goals
- Other specific concerns (i.e. presence of epidural hematoma, etc)
-
- Frequency of neurological exams
- Additional imaging
- Injury operative or non-operative
- Need for brace/what type of brace
- Activity restrictions (i.e. maintain full spine precautions, OK for HOB 30 deg, OK for activity in brace, etc)
- Recommendations regarding initiation of DVT prophylaxis
- Attending surgeon staffing consult
- Fractures present
-
- Operative vs non-operative management of SCF will be at the discretion of the consulting spine service and based on patient exam and fracture pattern/stability.
- On admission:
-
- Patient should be initiated on a multi-modality pain regimen to include the following (if not contraindicated):
-
- Acetaminophen 1000 mg q 8 hrs
- Calcitonin 200 IU per day intranasally
- Lidocaine 5% patch to affected area for 12 hrs
- Cyclobenzaprine 10 mg q 8 hrs (avoid in elderly)
- Oxycodone (avoid in elderly)
- Ibuprofen 800 mg q 8 hrs
- Gabapentin 300 mg q 8 hrs
-
- Activity orders
- Appropriate bracing should be ordered.
- Additional consults: physical therapy (PT), occupational therapy (OT)
-
- Consider speech consult in patients with cervical fractures and complaints of dysphonia or dysphagia
- PM&R consult for patients with SCI
-
- Patient should be initiated on a multi-modality pain regimen to include the following (if not contraindicated):
-
- Non-operative spine fractures:
-
- Within 24 hrs of admission:
-
- Appropriate brace delivered to bedside
- Ambulate with nursing staff and/or physical therapy (if not on full spine precautions or limited by concomitant injuries)
- Upright X-rays or additional imaging ordered and obtained.
-
- Once upright X-rays obtained, contact the appropriate spine service for interpretation and additional recommendations.
- Spine service will provide interpretation and additional recommendations within 6hrs of being notified x-rays are complete.
- If upright x-rays are unable to be obtained within 48 hrs of admission, notify spine service and discuss alternatives.
-
-
- 24-48 hrs of admission:
-
- PT/OT evaluations completed with disposition recommendations.
- Social work and case management engaged in disposition and discharge planning.
-
- Within 24 hrs of admission:
-
- Operative spine fractures:
-
- Surgical decompression or stabilization of SCF will ideally be performed within 72 hrs of admission in attempt to optimize outcomes and minimize morbidity related to delayed operative intervention.
-
- If patient unable to undergo recommended operative intervention within 72 hours, document why (i.e. patient factors, OR availability, surgeon availability).
-
- Within 24 hrs post-operatively:
-
- Appropriate brace delivered to bedside (if required)
- Ambulate with nursing staff and/or physical therapy
- Upright X-rays or additional imaging ordered and obtained.
-
- Once upright X-rays obtained, contact the appropriate spine service for interpretation and additional recommendations.
- Spine service will provide interpretation and additional recommendations within 6hrs of being notified x-rays are complete.
-
-
- 24-48 hrs post-operatively:
-
- PT/OT evaluations completed with disposition recommendations.
- Social work and case management engaged in disposition and discharge planning.
-
- Surgical decompression or stabilization of SCF will ideally be performed within 72 hrs of admission in attempt to optimize outcomes and minimize morbidity related to delayed operative intervention.
-
Follow-up Care
· Patients with SCF and/or SCI will follow-up at the discretion of the consulting spine service in the post-hospital setting.
Outcome Measures and Guideline Adherence
- All trauma patients with SCF and/or SCI experiencing a complication will be reviewed by our Trauma PI team for compliance with spinal injury guidelines.
- 6 months following implementation of guidelines, timing to OR for operative spinal injuries and length of stay will be reviewed for compliance and opportunities for improvement.
Related Policies
Cervical spine clearance
Key Contributors
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty
- Charity Evans, MD | Division of Acute Care Surgery, Faculty
- Daniel Surdell, MD | Department of Neurosurgery, Faculty
- Miki Katzir, MD | Department of Neurosurgery, Faculty
- Jamie Wilson, MD | Department of Neurosurgery, Faculty
- Scott Vincent, MD | Department of Orthopedic Surgery, Faculty
Last Updated
March, 2024
References
1. American College of Surgeons. Trauma Quality Improvement Program Spine Injury Best Practice Guidelines. spine_injury_guidelines.pdf (facs.org)
Transverse and Spinous Process Fractures
Background:
The majority of transverse process (TP) and spinous process (SP) fractures are structurally and neurologically stable injuries, which do not require spine service intervention. However there are some features which can be more worrisome for associated spinal cord and/or ligamentous involvement. Transverse process fractures are defined as those involving the transverse process only, without extension into the pedicle, lamina, or facet complex. The spinous process serves to attach muscles and ligaments, which are therefore at risk for injury in the presence of an SP fracture. We sought to create inclusion criteria to ensure that consistent spine consultation is obtained for the most high risk of these generally low-risk, stable fractures.
Guidelines for medical decision-making:
Trauma patients will receive imaging per usual protocol at the discretion of the treating team. TP and/or SP fractures may be identified on CT scan. If present, the following are indications for a spine consult:
· 4 or more contiguous TP fractures / SP fractures
· Bilateral TP fractures / SP fractures (regardless of the # of fractures)
· All C-spine TP fractures / SP fractures
Additionally, Spine consultation is required for ANY fracture (including TP and SP) when a concern for ligamentous injury exists.
Key contributors:
Abby Josef, Trauma
Reviewed by: Jamie Wilson, Neurosurgery and Scott Vincent, Ortho Spine
Version Date:
January 2024
References:
A. Homnick et al. Isolated thoracolumbar transverse process fractures: call physical therapy, not spine. J Trauma. (2007)
L.H. Bradley et al. Isolated transverse process fractures: spine service management not needed. J Trauma (2008)
J. H. Boulter et al. Implications of isolated Transverse Process fractures: Is spine service consultation necessary? World Neurosurgery (2016)
Care of Patients with Spinal Cord Injuries Practice Guideline
Purpose: To optimize the care of the spinal cord injured patient and prevent secondary complications.
Admission: All traumatic SCI patients will be admitted to ICU level of care with either Neurosurgery or Ortho Spine consult.
Spine Stabilization:
1. Patients with SCI should have unstable spinal injuries stabilized as early as possible, goal is within 24-48 hours post injury.
2. Optimize other injuries in multisystem injured patients with SCI to facilitate early spinal surgical stabilization.
3. Patients with SCI should be on bedrest until cleared by Neurosurgery/Ortho Spine. Once spinal injury is stabilized, activity should be liberated.
|
|
Phase 1: ICU |
Phase 2: Step-down or Floor |
|
Neurological |
· Neuro assessments per unit protocol. · Additionally, a neuro assessment should be performed and documented by nursing after any transfer (to new bed, new room, any procedure, etc). · Provider should be immediately notified of any changes in neuro exam. |
· Follow phase 1. |
|
Pain/Spasticity
|
· Assess pain per unit protocol. · Initiate multimodal pain regimen. Neuropathic Pain: · Pregabalin 75mg po q12h (can increase to 150 mg q12h at one week if needed) (reduce dosage if creatinine clearance is < 60mL/min) OR · Gabapentin 300 mg po q8h; > 65 years, 100 mg q8h (max 3600mg/day) · Consult pharmacy for titration. Should be weaned off over 1-2 weeks before discontinuing. · Initiate medication soon after injury. Spasticity: · Baclofen 10mg PO TID (max 120mg/day). · If minimal response to Baclofen, start Dantrolene 25mg PO Q 24 hrs; may titrate every 7 days to max of 400mg/day. Monitor LFTs weekly while actively titrating Dantrolene. Muscle Spasms: · Carisoprodol 350 mg po q6h PRN OR · Cyclobenzaprine 10 mg po q8h PRN |
|
|
Respiratory
|
All Patients: · Monitoring: Continuous pulse oximetry & EtCO2 for 7-10 days in patients with high cord injury and/or risk of respiratory compromise. Assess neurological level of injury daily. · For high cervical spine injuries (C6 and above): Consider daily ABG for 1-2 weeks post injury, with indications for escalation of respiratory support (including intubation) if PaO2 < 50 or PaCO2 > 50 on room air. · Consider monitoring with serial determination of the vital capacity, FEV1, the peak expiratory flow rate, the negative inspiratory force (NIF). If declining trend, order CXR and ABG with considerations as above. · Pts with weak cough, initiate manually assisted coughing (quad cough) Q 4 hrs. · Implement strict oral cares routine: every 2-4hrs and prn for intubated or unconscious patients; all other patients at minimum once per shift. Non-Intubated: · Incentive spirometry (IS) Q 1hr while awake. Nursing to document volume achieved. · If achieved IS volume < 50% predicted, consult Respiratory Therapy (RT) for lung volume expansion. RT Consult in all C spine and upper thoracic injuries- Pulmonary function test + possible addition of oscillatory positive expiratory pressure (OPEP), chest percussion therapy (CPT). Assisted Cough, IPV
Intubated: · In adults: Implement adult ventilator management EPIC order set which includes VAP bundle and ventilator weaning protocol. · Assess need for respiratory suctioning frequently to avoid mucous plugging. · Consider higher tidal volumes (TV) of 10-15 cc/kg to resolve or prevent atelectasis, if no contraindications. · Consider early tracheostomy who are likely to remain ventilator dependent or to wean slowly from mechanical ventilation. (<7 days) · Consult Speech Therapy (ST) to start Passy Muir Valve (PMV) trials · If not unable to tolerate or inappropriate for PMV, consult ST for alternate communication methods. · Consider downsizing trach as early as possible. Secretions: · Consider bronchoscopy. · 3% saline nebulized Q 8 hrs. · Add Guaifenesin · Consult RT for possible addition of oscillatory positive expiratory pressure (OPEP), chest percussion therapy (CPT), cough assist, IPV |
· Follow phase 1 non-intubated patient. Trach: · Consider larger TV (see phase 1 for parameters). · If remains on ventilator, continue weaning per protocol. · If not completed in phase 1, consult ST for PMV and/or alternate communication methods. Secretions: · Same as phase 1. · Discontinue therapies when secretions become thin. |
|
Cardiac |
· Vital signs per unit protocol. · Prevent and treat hypotension. Hypotension: · MAP Goal ≥ 80 x minimum 3-7 days (per Spine consult recommendations) from injury for ASIA A-D injuries. · Utilize Norepinephrine as first line agent. · Place arterial line for accurate hemodynamic monitoring. · Obtain central access if utilizing vasopressors. · If persistent vasopressor requirement > 3 days: Consider Midodrine 5 mg po q8h, titrate up to 40 mg/day. · Apply TED hose and /or ACE wraps to bilateral extremities when getting out of bed to chair, remove once back in bed. Bradycardia: · Assess for presence of mucus plugs (most common cause of acute bradycardia). · Order Atropine 0.5mg IV q1h prn for HR < 40 and have available at bedside. If persistent symptoms of bradycardia: · Start Robinul 0.1-0.2 mg IV or 1-2 mg po q8h to q12h. · Consider external or temporary pacemaker to maintain HR > 60. · If pacing required, consult cardiology. |
Hypotension: · Must be weaned off vasopressors prior to transfer out of ICU. · Continue or initiate Midodrine doses from phase 1 if needed. · Monitor for need or wean dose as tolerates. · Continue TED hose and/or ACE wraps from phase 1 when out of bed. Bradycardia: · Follow phase 1. |
|
Gastrointestinal |
· Gastrointestinal assessment per unit protocol. Monitor for nausea, vomiting, signs and symptoms of an ileus. Monitor for incontinence. · Initiate bowel regimen on admission. · Nursing to notify provider if patient goes more than a day without BM Stress Ulcer Prophylaxis: · Initiate and continue while patient remains ventilated. · Discontinue once patient off ventilator and tolerating goal tube feeds or regular diet x 48 hrs. Bowel Care (Prevent and Treat Constipation): · Initial upper motor neuron (UMN) regimen: Colace 100 mg po tid, Senna 17.6 mg 8-12 hours prior to digital simulation (typically given at lunch for nighttime digital stimulation) and Dulcolax 10 mg per rectum given along with digital stimulation. · Lower motor neuron (LMN) and mixed UMN/LMN injury regimen: Metamucil and manual stool evacuation. · No large volume enemas scheduled or routine. · Once enteral feedings have begun, bowel care should be done consistently at the same time each day, regardless of involuntary stooling between scheduled bowel care. · Schedule Bowel Routine: Dulcolax suppository at the same time daily with digital/manual stimulation. Discontinue only if excessive diarrhea. · Digital/Manual stimulation: Position patient left side down. Always use lubricant for comfort and to prevent autonomic dysreflexia. Should be done with scheduled Dulcolax suppository. · No BM by 72 hrs of admission: Check for impaction by positioning left side down. No impaction then increase Dulcolax to Q 12 hrs and start Lactulose 20grams PO Q 12 hrs until first BM. Diarrhea (liquid >500cc every Q 8 hrs or > 3 stools/day for 2 days): · Hold bowel regimen. · Start Metamucil 1 packet PO Q 12 hrs · Start Nutrisource Fiber 1 packet TID PO prn. · Consider checking stool for C.Difficile Toxin. |
· Follow phase 1. · Cervical level SCI requires 4 weeks of GI ppx |
|
Nutrition
|
· Consult Speech Therapy for swallow evaluation prior to initiating any oral intake in any SCI patient with cervical spinal cord injury, prolonged intubation, tracheostomy, halo fixation, or after any cervical spine surgery. · Obtain feeding access and initiate enteral support within 48 hrs of injury if no evidence of ongoing shock or hypoperfusion and off IV vasopressors. · Nutrition consult for assessment of calorie and protein needs. Also to provide nutrition support recommendations. · Once full estimated needs are being consistently provided consider ordering indirect calorimetry and/or 24 hour urine urea nitrogen to determine adequacy of nutrition. · Order calorie count when transitioning patient off enteral nutrition to oral intake to assist with titration. · Obtain prealbumin, CBC, CMP, folate and vitamin B12 every Sunday. · Maintain normoglycemia. |
· Follow phase 1 - continue current diet orders. · Nutrition to continue to monitor/intervene as per consult. · Transition to oral diet, if not on one, once patient passes ST swallow evaluation. |
|
Genitourinary |
· Genitourinary assessment per unit protocol. · Place indwelling catheter unless contraindicated, catheter cares per policy. · Remove indwelling catheter once patient is hemodynamically stable and no longer needs strict I&Os – then assess for volitional bladder control.
For patients without volitional bladder control: · Once Foley is removed: STRICT q4h straight cath & 2L fluid restriction. · If volumes are consistently less than 400 mL, can stop fluid restriction and go to q6h straight cath schedule. · Nursing or OT to teach self-cath technique. · Once patient is on the floor, closely follow ins/outs to ensure cath schedule is followed.
For patients with some volitional bladder control: · Check PVR after emptying bladder to assess need for above regimen.
For all patients: · Outpatient urodynamic evaluation with Urology to be scheduled 3 months following injury. |
· Follow phase 1. Work towards schedule for time straight caths. · Encourage moderate fluid intake spaced out throughout day to facilitate timed straight caths.
|
|
Integumentary
|
· Skin checks Q shift, pay close attention to bony prominences and under medical devices. · Give extra caution when assessing darker skin complexions as early signs of pressure injuries can go unnoticed. · If wound or skin concern identified, notify primary team and consult wound care per protocol. · Reposition pt at least every Q 2 hrs while maintaining spinal precautions (this includes all SCI pts –pre & post spine fixation, halo traction). · Position wedges above & below bony prominences to offload pressure. · Order and utilize TAPS turning system. · Patient with c-spine injury must be turned WITH wedges, not pillows to at 30+ degrees. Side lying preferred. · Sand beds for c-spine patients. Consider for high T-spine injury or patients with BUE weight bearing restrictions and consult with PT/OT. · Place on low air loss mattress. · Avoid friction, shearing, moisture and heat. Keep areas under patient clean and dry. · Implement pressure injury prevention skin bundle. · Consider placing Mepilex sacral dressing to coccyx/sacrum. · Order PRAFO and Prevalon boots. Alternating between the two Q 2 hrs. · Incision and drain wound care per orders. · Maintain normothermia. |
· Follow phase 1. · Consider specialty bed for floor · Order ROHO or GeoMatt cushion for wheelchair, utilize any time pt out of bed in chair. |
|
Mobility & Rehab |
· Consult physical therapy (PT) and occupational therapy (OT) for evaluate and treat. (should be seen within the first week, even if sedated/intubated) · Consult PM&R. · For cervical spine injuries, continue c-collar at all times. · Utilize brace, if ordered, when HOB > 30° and out of bed (confirm with neurosurgery). · Splinting should be considered for all patients at risk of contracture. · Let fingers flex passively and DO NOT overextend. This can cause loss stretch-induced paresis. · Sip and puff call light if pancake call light isn’t sufficient. Can consult OT for assistance with hydration system. · Consult SLP for communication needs (eye gaze system, etc.) · Early and aggressive mobilization. Head of Bed: · A gradual increase in HOB elevation, beginning at 15–30 degrees and advancing to 45 degrees or higher as tolerated, to promote upright tolerance and reduce the risk of orthostatic hypotension. · Unstable spinal injury requiring surgical fixation: Do not elevate HOB. Keep patient in reverse Trendelenburg unless contraindicated. · Stable fractures or post spinal fixation: HOB should remain elevated to at least 30° unless contraindicated. Activity: · Unstable spinal injury requiring surgical fixation, bedrest until fixation occurs. · Once spinal stabilization has occurred, discontinue bedrest order and place activity order. · Passive ROM should be performed daily for all major joints to prevent contractures. Active ROM when able. · Assess patient with the Bedside Mobility Assessment Tool before initiation of out of bed mobility. · Goal: Out of bed to chair or wheelchair Q 12 hrs once medical and spinal stability has been achieved. · For best practice, while in chair recline pt every 30 mins for 2 minutes or every 15 mins for 1 minute to achieve pressure relief then return to full upright position. · Consider utilizing ROHO or GeoMatt cushion when in chair or wheelchair. |
· Follow phase 1, continue to increase activity as tolerates. · PT/OT to assess need for orthotics of UE/LE. |
|
VTE Prophylaxis
|
· Pneumatic compression +/- Graduated compression stockings- ASAP when no LE injury C/I. Order SCDs, to be worn while in bed or sitting. (Including children of all ages) · No routine DVT screening. · Consider IVC filter if delay in starting chemical prophylaxis; otherwise no routine IVC filter placement. Chemical VTE prophylaxis · First line acute phase – Lovenox 30 mg BID. Recommendation against Heparin unless LMWH not available or contraindicated Timing of initiation · Stable spinal injury requiring no surgical fixation: Initiate Lovenox 30mg BID 24 hr. after admission. · Unstable spinal injury requiring surgical fixation: Start DVT PPX 24 hrs. post injury, if no other C/I and there is delay in OR for spine fixation. Hold morning dose on the day of surgery. · Unstable spinal injury post spinal fixation: <48 hrs. (as early as 24 hrs. post is safe) after surgery initiate Lovenox 40mg Q daily for 5 or 7 days then can transition to Lovenox 30mg BID dosing. (Check with Surgeon) · For patients with renal dysfunction, utilize Heparin 8000u SQ Q 8hrs. · Continue chemical prophylaxis for at least 8 weeks post injury in patients with limited mobility. Consider longer duration in motor complete injuries, lower-extremity fractures, older age, previous VTE, cancer, and obesity · Rehab phase – LMWH preferred, other options warfarin (INR 2-3) or DOAC. · Chemical VTE prophylaxis should be held prior to drain removal post-surgical fixation. Neurosurgery or Ortho spine to place this hold order. |
· Continue SCDs and chemical DVT prophylaxis. |
|
Psychosocial |
· Consult psychology. · Assess for depression. · Foster effective coping strategies. · Utilize assistive devices including specialty call lights and communication boards. · Identify, educate, and support family/caregivers. · For pediatric patients or patients with children or younger siblings consult child life. |
· Follow phase 1. |
|
Discharge Planning |
· Communicate early with care transitions to determine disposition options. · Consult social work to facilitate placement. |
· Continue discharge planning. |
|
Education |
· Begin teaching family and/or family/caregiver cares early on in stay once patient medically stable. Respiratory: How to manually assist coughing. Trach – suctioning and trach cares.
Cardiac: How to apply TED hose or ACE wraps prior to getting patient out of bed.
GI: Importance of bowel care schedule and how to manually stimulate.
GU: How to preform clean straight caths and catheter cares.
Integumentary: Importance of maintaining skin integrity and frequent assessments of skin.
Autonomic Dysreflexia (typically develops a few months post-SCI): Signs and symptoms, causes, prevention and treatment. |
· Continue to follow phase 1. Reinforce education and practice. |
Keely Buesing, MD, Trauma & Acute Care Surgery
Dan Pierce, MD, Physical Medicine & Rehabilitation
January 2026
References:
1. Beom, J., & Seo, H. (2018). The need for early tracheostomy in patients with traumatic cervical cord injury. Clinics in Orthopedic Surgery, 10(2), 191-196. doi: 10.4055/cios.2018.10.2.191
2. Cabahug, P., Pickard, C., Edmiston, T., & Lieberman, J. A. (2020). A Primary Care Provider's Guide to Spasticity Management in Spinal Cord Injury. Topics in spinal cord injury rehabilitation, 26(3), 157–165. https://doi.org/10.46292/sci2603-157
3. Consortium for Spinal Cord Medicine. (2008). Early acute management in adults with spinal cord injury: a clinical practice guideline for health-care professionals. Journal of Spinal Cord Medicine, 31(4), 403-479. doi: 10.1043/1079-0268-31.4.408
4. Dhall, S, Hadley, M., Aarabi, B., Gelb, D., Hurlbert, J., Rozzelle, C., Ryken, T., Theodore, N. & Walters, B. (2013). Deep venous thrombosis and thromboembolism in patients with cervical spinal cord injuries. Neurosurgery, 72, 244-254. doi: 10.1227/NEU.0b013e31827728c0
5. Fehlings, M., Tetreault, L., Wilson, J., Aarabi, B., Anderson, P., Arnold, P., Brodke, D., Burns, A., Chiba, K., Dettori, J., Furlan, J., Hawryluk, G., Holly, L., Howley, S., Jeji, T., Kalsi-Ryan, S., Kotter, M., Kurpad, S., Marino, R., …Harrop, J. (2017). A clinical practice guideline for the management of patients with acute spinal cord injury and central cord syndrome: Recommendations on the time (≤ 24 hours versus > 24 hours) of decompressive surgery. Global Spine Journal, 7, 195S-202S. doi: 10.1177/2192568217706367.
6. Groah, S., Schladen, M., Pineda, C., & Hsieh, C. (2015). Prevention of pressure ulcers among people with spinal cord injury: A systematic review. PM&R: The Journal of injury, function, and rehabilitation, 7(6), 613-636. doi: 10.1016/j.pmrj.2014.11.014
7. Liu, Y., Xu, H., Liu, F., Lv, Z., Kan, S., Ning, G., & Feng, S. (2017). Meta-analysis of heparin therapy for preventing venous thromboembolism in acute spinal cord injury. International Journal of Surgery, 43, 94-100. doi: 10.1016/j.ijsu.2017.05.066
8. Saadeh, Y., Smith, B., Joseph, J., Jaffer, S., Buckingham, M., Oppenlander, M., Szerlip, N., & Park, P. (2017). The impact of blood pressure management after spinal cord injury: a systematic review of the literature. Journal of Neurosurgery, 43(5), 1-7. https://doi.org/10.3171/2017.8.FOCUS17428
9. Sabit, B., Zeiler, F., & Berrington, N. (2018). The impact of mean arterial pressure on functional outcome post trauma-related acute spinal cord injury: A scoping systematic review of human literature. Journal of Intensive Care Medicine, 33(1), 3-15. doi: 10.1177/0885066616672643.
10. Stein, D., & Knight, W. (2017). Emergency neurological life support: Traumatic spine injury. Neurocritical Care, 27, 170-180. doi: 10.1007/s12028-017-0462-z.
11. Walters, B., Hadely, M., Hurlbert, R., Aarabi, B., Dhall, S., Gelb, D., Harrigan, M., Rozelle, C., Ryken, T., & Theodore, N. (2013). Guidelines for the management of acute cervical spine and spinal cord injuries: 2013 update. Neurosurgery, 60, 82-91. doi: 10.1227/01.neu.0000430319.32247.7f.
12. Zakrasek, E., Nielson, J., Kosarchuk, J., Crew, J., Ferguson, A. & McKenna, S. (2017). Pulmonary outcomes following specialized respiratory management for acute cervical spinal cord injury: a retrospective analysis. Spinal Cord, 55(6), 559-565. doi: 10.1038/sc.2017.10