# 6. Abdominal Trauma
Educational materials and pathways regarding the evaluation and management of abdominal injuries.
# Blunt Abdominal Trauma
[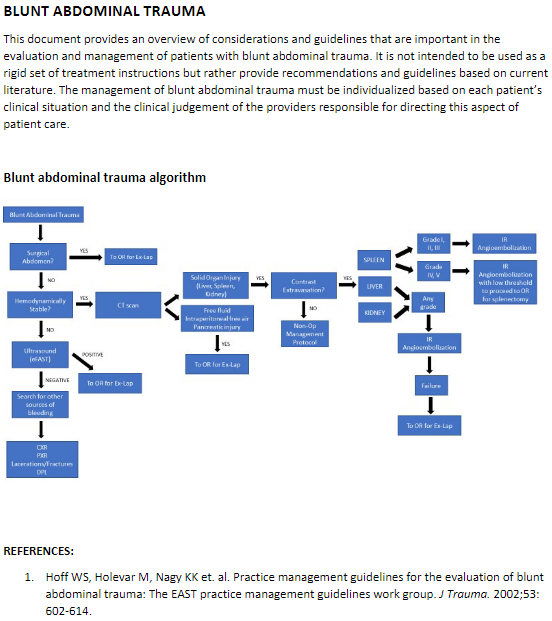](https://paths.trauma.ai/uploads/images/gallery/2023-01/OXYimage.png)
# Evaluation and Management of Blunt Splenic Injury
#### Purpose
Splenic injury is one of the most common injuries following blunt abdominal trauma and can result in significant bleeding given the vascular nature of this organ. Unrecognized injury can be a cause of preventable death following trauma. The following guidelines outline the approach that should be taken when evaluating and managing a trauma patient with splenic injury and the decision-making process between operative and non-operative management.
#### Background/Definitions
During the last century, management of blunt splenic injury has shifted from observation/expectant management in the early 1900s to operative intervention for all injuries, to the current practice of selective operative and non-operative management of splenic injury. The current non-operative paradigm in adults was stimulated by the success of non-operative management of solid-organ injuries in hemodynamically stable children. The potential advantages of non-operative management include lower hospital cost, earlier discharge, avoiding nontherapeutic laparotomies (as well as associated cost and morbidity), fewer intra-abdominal complications, and reduced transfusion rates associated with an overall mortality of these injuries. While the non-operative approach to blunt splenic injury has been proven to work well in hemodynamically stable patients with lower grade injuries, there is still a role for operative and/or endovascular intervention in those patients who are hemodynamically unstable or those with higher grade injuries.
Splenic injuries are classified by a grading system established by the AAST (American Association for the Surgery of Trauma). In general, the higher the grade equals more severe injury and potential for associated morbidity and mortality.
AAST Splenic Injury Grading Scale
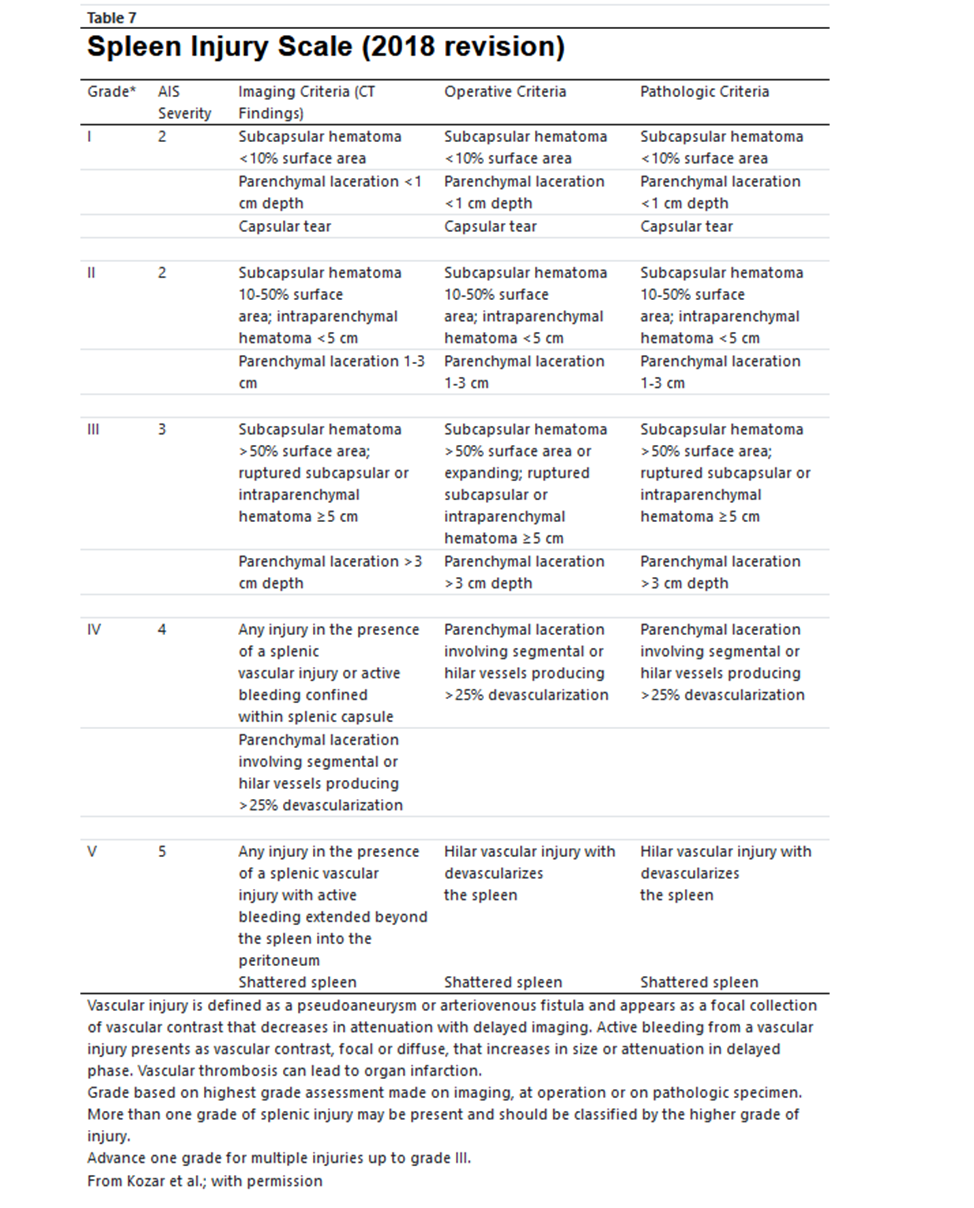
[ **https://www.aast.org/resources-detail/injury-scoring-scale#spleen** ](https://paths.trauma.ai/%20https:/www.aast.org/resources-detail/injury-scoring-scale#spleen)
#### Guideline Inclusion Criteria
- All trauma patients sustaining blunt abdominal trauma should be evaluated for potential splenic injury.
#### Guideline Exclusion Criteria
- Patients who no longer have a spleen.
- Pediatric patients <15 yrs age.
#### Diagnostic Evaluation
- All trauma patients should be initially evaluated per ATLS guidelines with work-up as mechanism and clinical presentation dictate.
- Resuscitative measures should be initiated as clinical status/presentation dictates.
- Labs, imaging and additional tests should be obtained as clinical status/presentation dictates.
- If a patient is hemodynamically UNSTABLE, minimal testing/imaging should occur prior to interventions for hemorrhage control.
#### Practice Recommendations for Management
- Once splenic injury is suspected and/or confirmed, management of that injury is dictated largely by the clinical status of the patient.
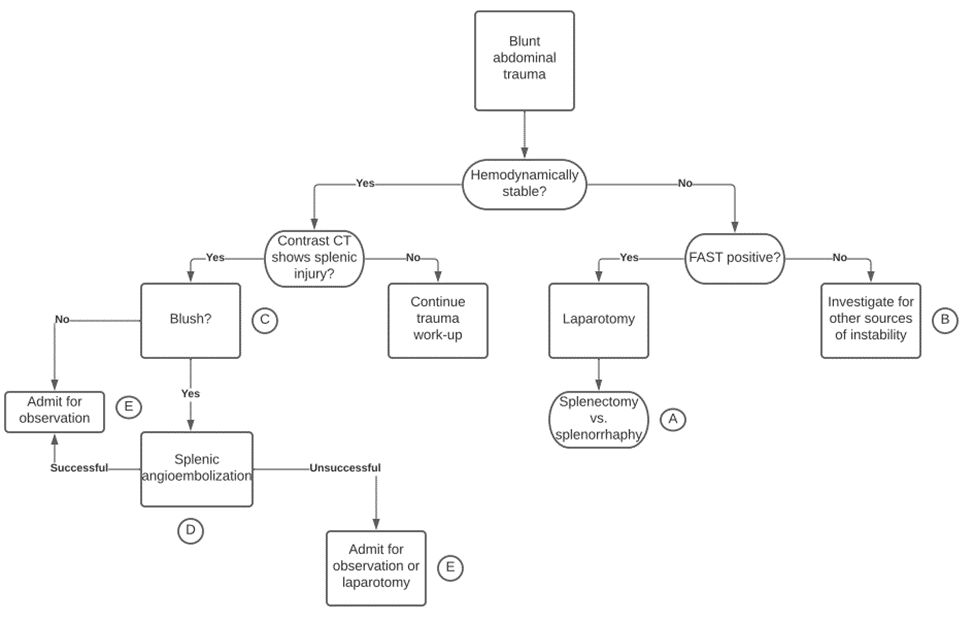
- - If a patient is hemodynamically **UNSTABLE**:
- - Initiate/continue resuscitative measures.
- Obtain an eFAST exam.
- If eFAST is positive, proceed to OR for surgical exploration.
- If a patient is hemodynamically **STABLE**:
- - May continue with evaluation and work-up as mechanism and presentation dictate.
- Obtain imaging as indicated, including a multi-phase CT abd/pelvis with IV contrast
- Determine appropriate management strategy based on grade of injury, presence of blush/extravasation on imaging, and clinical status and injury burden of patient.
[603730a847af494fa170694b778b703a.pdf (cvent.com)](https://custom.cvent.com/2A7C589629FA4A7181E1D1A892311435/files/603730a847af494fa170694b778b703a.pdf)
- Operative Management
- - Should be used in all patients who are hemodynamically unstable or those with peritonitis on exam.
- Should be considered in patients who are transient responders to resuscitation or in those with injury burden (head injury) in which hypotension secondary to hemorrhagic shock would be detrimental.
- Operative plan should be exploratory laparotomy for trauma with splenectomy vs splenorrhaphy.
- - Splenic salvage/splenorrhaphy may be considered in Grade I-II injuries depending on the clinical status of the patient.
- Splenectomy should be performed in Grade III-V injuries or in patients with ongoing bleeding.
- IR Angioembolization
- - Should be considered in patients who are transient responders to resuscitation, those with evidence of active extravasation/blush on CT abd/pelvis, those with high grade injuries (Grade III-V) or those with injury burden (e.g. head injury) in which hypotension secondary to hemorrhagic shock would be detrimental.
- Non-operative Management
- - Non-operative management of splenic injuries should ONLY be considered in hemodynamically stable patients.
- Patients undergoing non-operative management should be monitored closely for deterioration in clinical status suggestive of ongoing hemorrhage (i.e. failure of non-operative management) with vitals per unit protocol, serial labs, abdominal exams and repeat imaging as indicated.
- Bedrest is not routinely indicated for blunt splenic injuries that are managed non-operatively. In general, patients may be activity as tolerated unless bedrest is required for a concurrent injury or at trauma attending discretion.
- Admission level of care will be at the trauma attending’s discretion. In general, higher grade injuries (III, IV, V) should be initially monitored in the ICU or Step Down Unit and lower grade injuries (I, II) be initially monitored on the floor or Step Down Unit depending on clinical status and injury burden.
- Suggested non-operative management strategy is as follows:
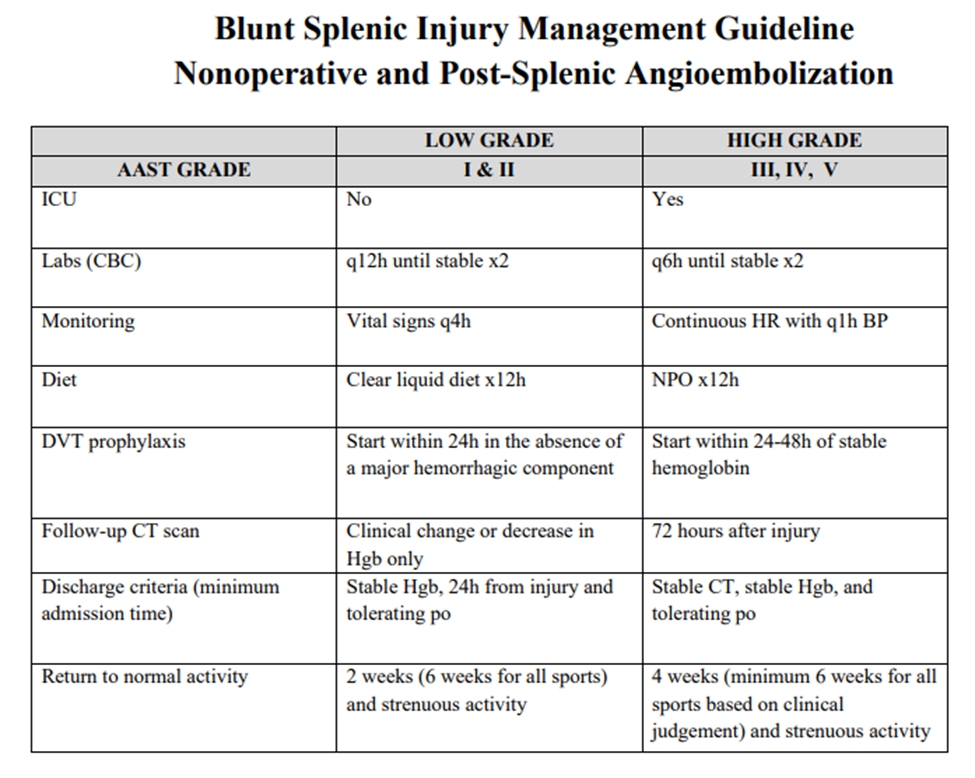
[603730a847af494fa170694b778b703a.pdf (cvent.com)](https://custom.cvent.com/2A7C589629FA4A7181E1D1A892311435/files/603730a847af494fa170694b778b703a.pdf)
- - - Repeat imaging for splenic injuries managed non-operatively
- - A repeat multi-phase CT abd/pelvis with IV contrast should be obtained for all Grade III or higher splenic injuries between 3-5 days post injury or prior to discharge to evaluate for development of post-traumatic pseudoaneurysms.
- If pseudoaneurysms are present, then IR should be consulted for consideration of splenic angioembolization.
- Follow-up Care:
- - Post splenectomy vaccines
- - Patients undergoing splenectomy as management of their splenic injury should obtain the following vaccines prior to discharge or at 14 days post-op (whichever date comes first)
- - Quadravalent meningococcus (Menactra or Menomune)
- Pneumococcus (Pneumovax 23)
- H.influenzae B (HIB, ActHIB)
- Viral influenza vaccine (depending on time of year)
- Patients undergoing splenic angioembolization do not routinely require vaccinations.
- All patients with splenic injury should follow-up in trauma clinic 1-2 weeks following discharge pending clinical status at time of discharge and hospital length of stay following injury.
#### Outcome Measures and Guideline Adherence
- Time to OR/IR and interventions for all hemodynamically unstable patients will be tracked through our performance improvement process/initiatives.
- Patients failing non-operative management (i.e. those requiring IR angioembolization or exploratory laparotomy in a delayed fashion) will be tracked through our performance improvement process/initiatives.
- Adherence to obtaining repeat imaging for Grade III or higher splenic injuries at post-injury day 3-5 and need for subsequent interventions will be assessed every 6 months.
#### Key Contributors
· Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
#### Last Updated
July, 2023
#### References
1. Stassen NA, Bhullar I, Cheng JD, et. al. Selective nonoperative management of blunt splenic injury: An Eastern Association for the Surgery of Trauma practice management guidelines. *J Trauma Acute Care Surg.* 2012;73(5): S294-300.
2. Rowell SE, Biffl WL, Brasel K, et. al. Western Trauma Association critical decisions in trauma: Management of adult blunt splenic trauma—2016 updates. *J Trauma Acute Care Surg.* 2016; 82(4): 787-93.
3. Wallen TE, Clark K, Baucom MR, et al. Delayed splenic pseudoaneurysm identification with surveillance imaging. *J Trauma Acute Care Surg.* 2022;93(1):113-117.
4. Freeman JJ, Yorkgitis BK, Haines K, et al. Vaccination after spleen embolization: A practice management guideline from the Eastern Association for the Surgery of Trauma. *Injury.* 2022;53(11):3569-3574.
# Evaluation and Management of Hepatic Injury
#### Purpose
The liver is the most frequently injured abdominal organ. Most injuries are minor and can heal spontaneously without operative management. Unrecognized injury can be a cause of preventable death following trauma. The following guidelines outline the approach that should be taken when evaluating and managing a trauma patient with hepatic injury and the decision-making process between operative and non-operative management.
#### Background/Definitions
During the last century, the management of blunt force trauma to the liver has changed dramatically. A shift away from operative management has resulted in a decline in mortality. The current nonoperative paradigm in adults was encouraged by the success of nonoperative management of solid organ injuries in hemodynamically stable children. As early as 1960, Shaftan advocated “observant and expectant treatment” rather than mandatory laparotomy in the management of penetrating abdominal injury. This was reinforced in 1969 by Nance and Cohn for the management of abdominal stab wounds. The advantages of nonoperative management include lower hospital cost, earlier discharge, avoiding nontherapeutic laparotomies, fewer intra-abdominal complications, and reduced transfusion rates. Gunshot wounds to the abdomen, however, are still commonly treated with mandatory exploration because of multiple reports emphasizing a high incidence of intra-abdominal injuries and the complications of a missed injury or an injury delayed in recognition and treatment. Multiple studies and review of National Trauma database have demonstrated that only 13.7% of hepatic injuries are now managed operatively. Complications develop in 2.5 to 41% of all trauma patients undergoing unnecessary laparotomy, and small bowel obstruction, pneumothorax, ileus, wound infection, myocardial infarction, visceral injury, and even death have been reported secondary to unnecessary laparotomy. It is important to recognize the importance of different mechanisms of penetrating injury (stab versus gunshot versus shotgun wounds), the velocity of the agent (low versus high) as well as the different regions of the abdomen (intraperitoneal, retroperitoneal, and thoracoabdominal areas).
These issues were first addressed by the Eastern Association for the Surgery of Trauma (EAST) in the Practice Management Guidelines for Non-operative Management of Blunt Injury to the Liver and Spleen published online in 2003. The practice management guideline update was split into separate recommendations for the nonoperative management of blunt hepatic and splenic injuries in adult trauma patients, with the last set of guidelines being published in 2012 for blunt hepatic injuries and in 2010 for penetrating injuries.
Hepatic injuries are classified by a grading system established by the AAST (American Association for the Surgery of Trauma). In general, the higher the grade equals more severe injury and potential for associated morbidity and mortality.
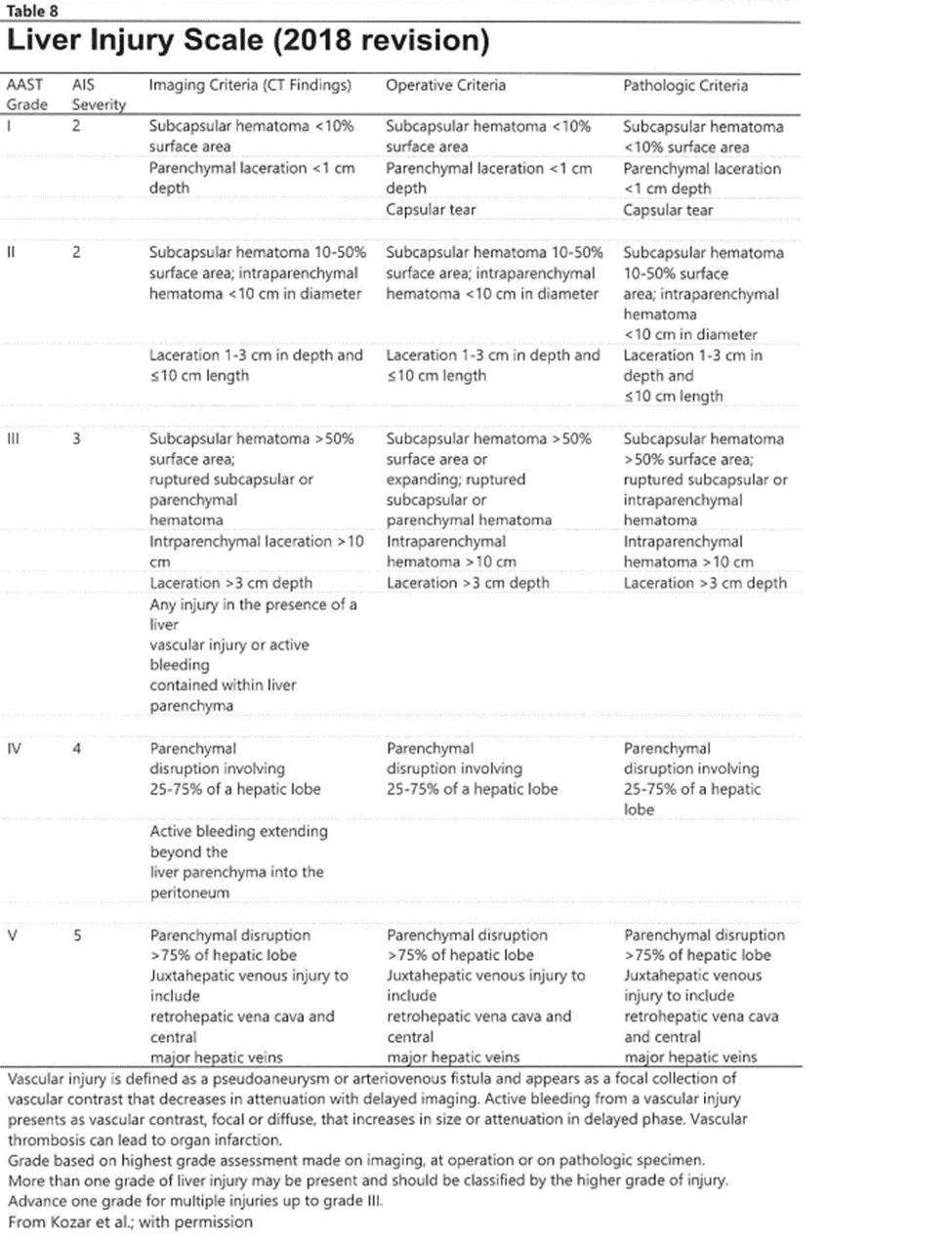
[https://www.aast.org/resources-detail/injury-scoring-scale#liver](https://www.aast.org/resources-detail/injury-scoring-scale#liver)
#### Guideline Inclusion Criteria
- All trauma patients sustaining abdominal trauma should be evaluated for potential hepatic injury.
#### Guideline Exclusion Criteria
- Pediatric patients <15 yrs of age.
#### Diagnostic Evaluation
- All trauma patients should be initially evaluated per ATLS guidelines with work-up as mechanism and clinical presentation dictate.
- Resuscitative measures should be initiated as clinical status/presentation dictates.
- Labs, imaging and additional tests should be obtained as clinical status/presentation dictates.
- If a patient is hemodynamically UNSTABLE, minimal testing/imaging should occur prior to interventions for hemorrhage control.
#### Practice Recommendations for Management
- Once hepatic injury is suspected and/or confirmed, management of that injury is dictated largely by the clinical status of the patient.
- - - If a patient is hemodynamically **UNSTABLE**:
- - Initiate/continue resuscitative measures.
- Obtain an eFAST exam.
- If eFAST is positive, proceed to OR for surgical exploration.
- If a patient is hemodynamically **STABLE**:
- - May continue with evaluation and work-up as mechanism and presentation dictate.
- Obtain imaging as indicated, including a multi-phase CT abd/pelvis with IV contrast.
- Determine appropriate management strategy based on grade of injury, presence of blush/extravasation on imaging, and clinical status and injury burden of patient.
- Operative Management
- - - Should be used in all patients who are hemodynamically unstable or those with peritonitis on exam.
- Should be considered in patients who are transient responders to resuscitation or in those with injury burden in which hypotension secondary to hemorrhagic shock would be detrimental.
- Operative plan should be exploratory laparotomy for trauma with consideration of cauterization, topical hemostatic agents, hepatorrhaphy or packing +/- endovascular procedures.
- Diagnostic laparoscopy may be considered as a tool to evaluate diaphragmatic lacerations as well as peritoneal penetration.
- In severe/high grade liver injuries, interventional radiology for angioembolization may also be considered for hemorrhage control in conjunction with operative interventions.
- IR Angioembolization
- - Should be considered in patients who are transient responders to resuscitation, those with evidence of active extravasation/blush on CT abd/pelvis, those with high grade injuries (Grade III-V) or those with injury burden (e.g. head injury) in which hypotension secondary to hemorrhagic shock would be detrimental.
- Non-operative Management
- - Non-operative management of hepatic injuries should ONLY be considered in hemodynamically stable patients.
- Patients with penetrating injury isolated to the right upper quadrant of the abdomen may be managed without laparotomy in the presence of stable vital signs, reliable examination and minimal to no abdominal tenderness.
- The severity of hepatic injury (as suggested by CT grade or degree of hemoperitoneum), neurologic status, age of more than 55 years, and/or the presence of associated injuries are not absolute contraindications to a trial of nonoperative management in a hemodynamically stable patient.
- Patients undergoing non-operative management should be monitored closely for deterioration in clinical status suggestive of ongoing hemorrhage (i.e. failure of non-operative management) with vitals per unit protocol, serial labs, abdominal exams and repeat imaging as indicated.
- Interventional modalities including endoscopic retrograde cholangiopancreatography (ERCP), angiography, laparoscopy, or percutaneous drainage may be required to manage complications (bile leak, biloma, bile peritonitis, bilious ascities, and hemobilia)
- Bedrest is not routinely indicated for blunt hepatic injuries that are managed non-operatively. In general, patients may be activity as tolerated unless bedrest is required for a concurrent injury or at trauma attending's discretion.
- Admission level of care will be at the trauma attending's discretion. In general, higher grade injuries (III, IV, V) should initially be monitored in the ICU or Step Down Unit and lower grade injuries (I, II) be initially monitored on the floor or Step Down Unit depending on the clinical status and injury burden of the patient.
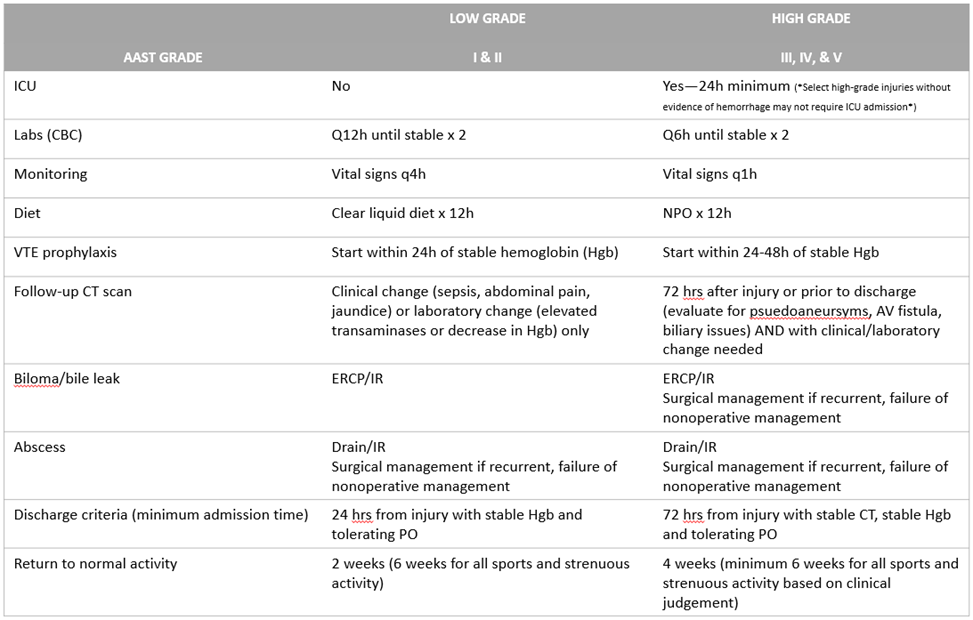
- Suggested non-operative management strategy is as follows (Table 1):
Table1. Blunt Hepatic Injury Guidelines for Nonoperative and Postintervention Management
- Repeat imaging for hepatic injuries managed non-operatively
- Clinical factors such as a persistent systemic inflammatory response, increasing persistent abdominal pain, jaundice, or an otherwise unexplained drop in hemoglobin should prompt reevaluation by CT scan.
- A repeat multi-phase CT abd/pelvis with IV contrast should be obtained for all Grade III or higher blunt hepatic injuries between 3-5 days post injury or prior to discharge to evaluate for development of post-traumatic pseudoaneurysms, AV fistulas or biliary issues.
Figure 1. Western Trauma Association algorithm for the diagnosis and management of blunt hepatic injury in adults. Circled letters correspond to lettered section in the articles text. OR, operating room; IR, interventional radiology. (Keric N, Shatz DV, Schellenberg M, et al. Adult blunt hepatic injury: A Western Trauma Association critical decisions algorithm. *J Trauma Acute Care Surg.* 2024 Jan 1;96(1):123-128. Doi:10.1097/TA.0000000000004141. Epub 2023 Sep 25. PMID: 37747241)
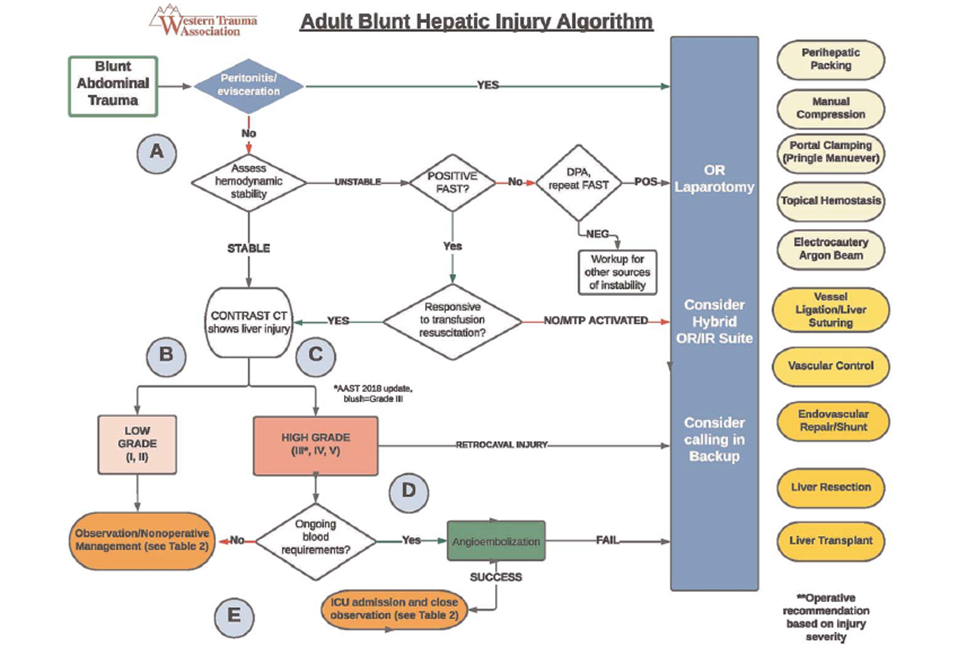
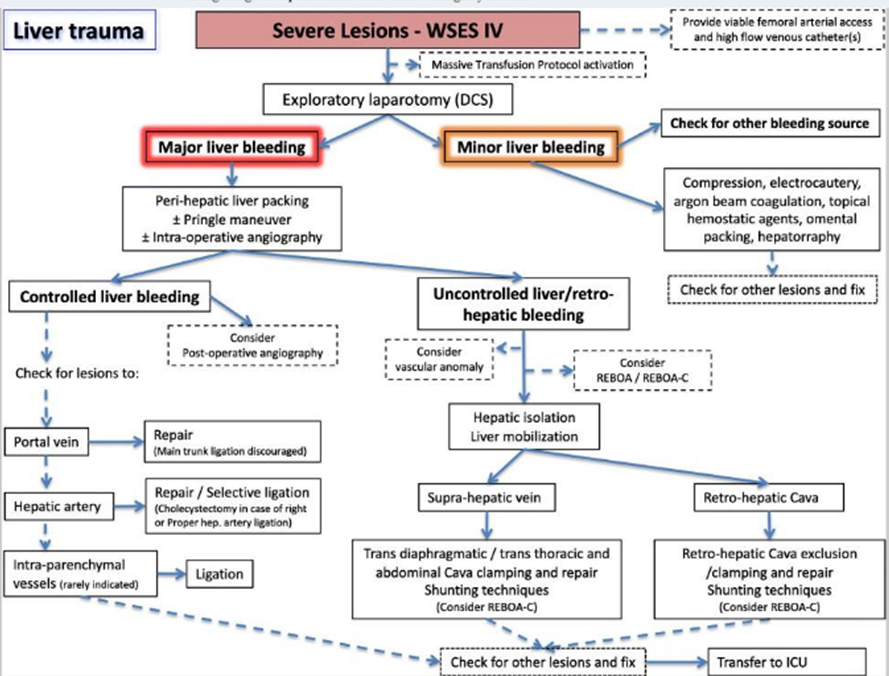
Figure 2. Operative management of blunt hepatic injury in adults.
- Follow-up Care
- - All patients with hepatic injury should follow-up in trauma clinic 1-2 weeks following discharge pending clinical status at time of discharge and hospital length of stay following injury.
#### Outcome Measures and Guideline Adhearance
- Time to OR/IR and interventions for all hemodynamically unstable patients will be tracked through our performance improvement process/initiatives.
- Patients failing non-operative management (i.e. those requiring IR angioembolization or exploratory laparotomy in a delayed fashion) will be tracked through our performance improvement process/initiatives.
#### Key Contributors
· Gina Lamb, MD | Division of Acute Care Surgery, Faculty | Principle Author
Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Author
#### Last Updated
February, 2024
#### References
1. Tinkoff G, Esposito T, Reed J, et al. American Association for the Surgery of Trauma Organ Injury Scale I: spleen, liver, and kidney, validation based on the National Trauma Data Bank. J Am Coll Surg. 2008;207:646–655
2. Como J, Bokhari F, et al. Practice Management Guidelines for Selective Nonoperative Management of Penetrating Abdominal Trauma. J Trauma. 2010;68: 721–733
3. Stassen, N, Bhullar, I, et al. Nonoperative management of blunt hepatic injury. An Eastern Association for the Surgery of Trauma practice management guideline. *Journal of Trauma and Acute Care Surgery *[73(5):p S288-S293, November 2012.](https://journals.lww.com/jtrauma/toc/2012/11004)
4. Wagner ML, Streit S, Makley AT, Pritts TA, Goodman MD. Hepatic Pseudoaneurysm Incidence After Liver Trauma, Journal of Surgical Research, Volume 256, 2020, Pages 623-628
5. Keric N, Shatz DV, Schellenberg M, et al. Adult blunt hepatic injury: A Western Trauma Association critical decisions algorithm. *J Trauma Acute Care Surg.* 2024 Jan 1;96(1):123-128. Doi:10.1097/TA.0000000000004141. Epub 2023 Sep 25. PMID: 37747241
6. Coccolini F, Coimbra R, Ordonez C, Kluger Y, et al. WSES expert panel. Liver trauma: WSES 2020 guidelines. World J Emerg Surg. 2020 Mar 30;15(1):24. doi: 10.1186/s13017-020-00302-7. PMID: 32228707; PMCID: PMC7106618
####