7. Orthopedic Trauma
Educational materials and pathways regarding the evaluation and management of orthopedic injuries.
- Antibiotic Prophylaxis in Open Fractures
- Hand/Finger Reimplantation
- Isolated Hip Fracture Protocol
- Isolated Orthopedic Injury Admission Guidelines
- Orthopedic Trauma Discharge VTE Prophylaxis
- Management of Open Fractures
- Mangled Extremity Management
Antibiotic Prophylaxis in Open Fractures
BACKGROUND
Open fractures are high energy injuries with an increased risk of infection due to potential exposure of bone and deep tissue to a variety of environmental debris. Infection can lead to serious complications including nonunion of wounds and osteomyelitis.
DEFINITIONS
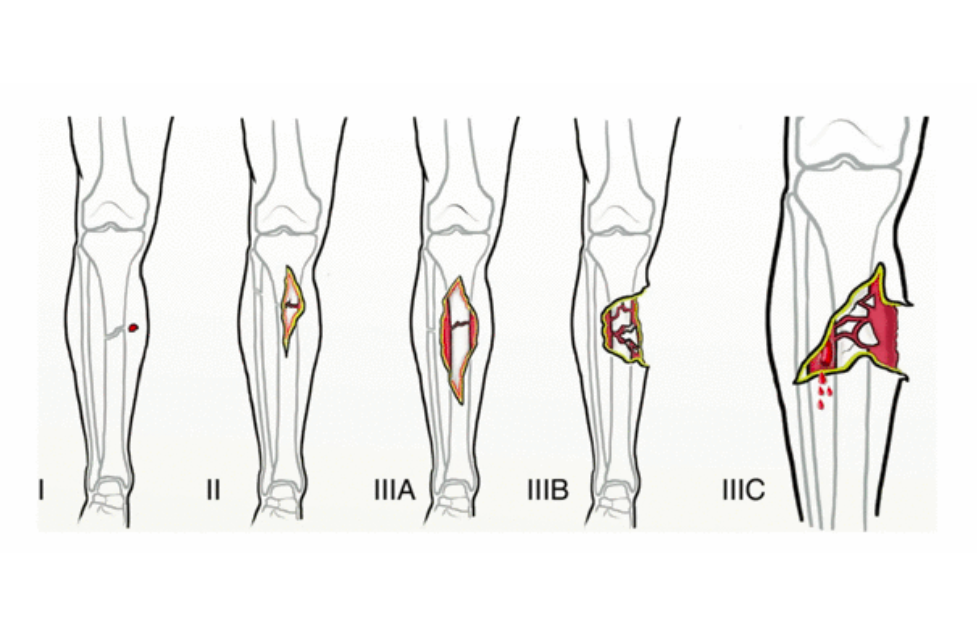
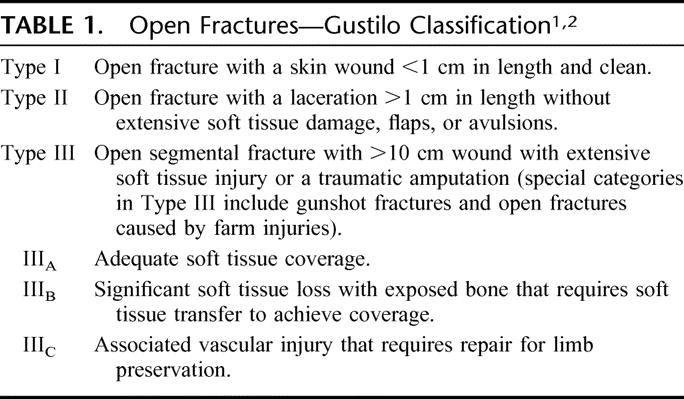
The Gustilo-Anderson classification system is the most commonly used grading system for open fractures. Fractures are designated as one of three types based on wound size, soft tissue involvement, contamination, and fracture pattern.
Table 1: Gustilo-Anderson Classification System
| Type I fracture | Open fracture with clean wound <1 cm long |
| Type II fracture | Open fracture with laceration >1 cm long without extensive soft tissue damage |
| Type III fracture | Open segmental fracture, open fracture with extensive soft tissue damage, or traumatic amputation |
BETA-LACTAM ALLERGY MANAGEMENT: Cefazolin is a safe option in patients with documented penicillin allergies due to its unique structural characteristics. Cross reactivity between PCN and advanced generation cephalosporins is also very rare. These agents (ceftriaxone) are generally considered safe for patients with distant (>10 years) or non-severe reactions to PCN. Patients who report a rash only or have previously tolerated cephalosporins of any kind may safely be given the agents listed in this guideline.
USE OF METRONIDAZOLE WITH ALCOHOL: The CDC no longer recommends avoiding alcohol when taking metronidazole. Current evidence doesn’t support that metronidazole use with alcohol results in vomiting (a disulfram-like reaction). It does not inhibit liver aldehyde dehydrogenase nor does its use with alcohol increase levels of acetaldehyde. Thus, metronidazole is considered safe to use in patients who have recently used alcohol or are intoxicated.
RECOMMENDATIONS
Type I and II Fractures
• Preferred: Cefazolin 2 g (3 g if > 120 kg) IV q8h
• Severe cephalosporin allergy: Clindamycin 900 mg IV q8h
• Known MRSA colonization: Add vancomycin 15 mg/kg IV q12h
• Duration of prophylaxis: 24 hours
Type III Fractures
• No gross contamination:
o Preferred: Ceftriaxone 2g IV q24h
o Severe cephalosporin allergy: levofloxacin 500 mg IV q24h
o Known MRSA colonization: Add vancomycin 15 mg/kg IV q12h
o Duration of prophylaxis: 48 hours or 24 hours after wound closure, whichever is shorter
• Contamination with soil or fecal material:
o Preferred: Ceftriaxone 2 g IV q24h + metronidazole 500 mg IV q8h
o Severe Cephalosporin allergy: Levofloxacin 500 mg IV q24h + metronidazole 500 mg IV q8h
o Known MRSA colonization: Add vancomycin 15 mg/kg IV q12h
o Duration: 48 hours after wound closure
o Consider orthopedic infectious diseases consult
• Contamination with standing water:
o Preferred: Piperacillin/tazobactam 4.5 g IV q8h over 4 hours
o Penicillin allergy: Levofloxacin 500 mg IV q24h + metronidazole 500 mg IV q8h
o Known MRSA colonization: Add vancomycin 15 mg/kg IV q12h
o Duration: 48 hours after wound closure
o Consider orthopedic infectious diseases consult
Guidance Summary
| Preferred therapy |
Severe cephalosporin allergy |
Duration |
|
| Type 1 and 2 Fracture |
Cefazolin 2g q8h | Clindamycin 900mg q8h | 24 hours |
| Type 3 Fracture |
Ceftriaxone 2g q24h | Levofloxacin 500mg IV q24h | 48 hours (or 24 hours after wound closure, whichever is shorter) |
| Type 3 Fracture contaminated with soil or fecal material |
Ceftriaxone 2g q24h PLUS Metronidazole 500mg IV q8h | Levofloxacin 500mg IV q24h PLUS Metronidazole 500mg IV q8h | 48 hours (or 24 hours after wound closure, whichever is shorter) |
| Type 3 Fracture with standing water exposure |
Piperacillin/tazobactam 4.5g q8h over 4hours | Penicillin Allergy: Levofloxacin 500mg IV q24h PLUS Metronidazole 500mg IV q8h | 48 hours (or 24 hours after wound closure, whichever is shorter) |
| Known MRSA colonization |
Add Vancomycin 15 mg/kg q12h |
Key Contributors
Kelley McGinnis, PharmD
REFERENCES
• Rodriguez L, Jung HS, Goulet JA, et al. Evidence-based protocol for prophylactic antibiotics in open fractures: improved antibiotic stewardship with no increase in infection rates. J Trauma Acute Care Surg. 2013;77(3):400-8.
• Hauser CJ, Adams CA Jr, Eachempati SR. Surgical infection society guideline: prophylactic antibiotic use in open fractures: an evidence-based guideline. Surg Infect (Larchmt). 2006;7(4):379-405.
• Dunkel N, Pittet D, Tovmirzaeva L, et al. Short duration of antibiotic prophylaxis in open fractures does not enhance risk of subsequent infection. Bone Joint J. 2013;95-B:831-7.
• Anderson A, Miller AD, Categoriestaver PB. Antimicrobial prophylaxis in open lower extremity fractures. Open Access Emergency Medicine. 2011:3:7-11.
• Hoff WS, Bonadies JA, Cachecho R, Dorlac WC. East Practice Management Guidelines Work Group: update to practice management guidelines for prophylactic antibiotic use in open fractures. J Trauma. 2011;70(3):751-4
• Mergenhagen KA, Wattengel BA, Skelly MK, et al. Fact versus Fiction: a Review of the Evidence behind Alcohol and Antibiotic Interactions. Antimicrob Agents Chemother. 2020;64:e02167-19.
• Visapaa JP, Tillonen JS, Kaihovaara PS, et al. Annals of Pharmacother. 2002;36:971-4.
• Workowski KA, Bachmann LH, Chan PA, et al. CDC Sexually Transmitted Infections Treatment Guidelines, 2021. https://www.cdc.gov/std/treatment-guidelines/bv.htm
Hand/Finger Reimplantation
Patients Requiring Hand/Finger Reimplantation
Decision to transfer/divert a patient needing revascularization/replantation will be made based upon:
· Patients with isolated, or near isolated, amputation or devascularization injuries should be transferred to nearest hand reimplantation center.
· Recovery of devascularized or amputated parts with mechanism of injury reasonable for replantation
· Determination of warm/cold limb ischemia time and ability to transport to appropriate replantation center prior to exceeding replantation time limits
o Digit
§ Warm Ischemia <12hrs
§ Cold Ischemia <24hrs
o Hand/Limb
§ Warm Ischemia <6hrs
§ Cold Ischemia <12hrs
· If patient is unable to reach a replant center prior to the ischemia limit, transfer to nearest regional trauma center for additional care.
***Important to note: Patients with multiple traumatic injuries, including hand/arm amputation/devascularization, may not be appropriate for transfer to nearest reimplantation center due to concomitant injuries. In these situations, it may be “life over limb” so transport to the nearest trauma center should take precedent.***
Never hesitate to contact your regional trauma center for guidance on patient transport appropriateness.
Regional Hand Reimplantation Centers:
Adults and Pediatrics
· Nebraska Medicine- consider for potential replantation/revascularization:
402-559-BEDS (9337)
· Denver Health Trauma:
1-855-602-5280 OR 303-628-1550
· University of Iowa
1-866-890-5969
· St. Louis (Barnes-Jewish: Adults/St. Louis Children’s: Pediatrics)
800-678-HELP (4357)
· Regions Hospital- St. Paul, MN:
888-588-9855
· Mayo Clinic
507-255-2910
Adults Only:
· Faith Regional Hospital in Norfolk- Dr. Hartzell
402-371-4880
· KU- Kansas City
913-588-1227
· University of Missouri
573-882-4141
Pediatric Only:
· Children’s Mercy Kansas City, MO
1-800-GO-MERCY
1-800-46-63729
Isolated Hip Fracture Protocol
Section One: Timing and Care Sequence:
1. Presentation to the Emergency Room
a. Assessment by the ED
b. Radiographs
i. Low AP pelvis, AP of affected hip, AP and lateral of affected femur
ii. MRI indicated if high suspicion but no clear fracture on x-ray, CT scan if MRI not available
2. Admission and Consultation
a. Patient admitted to Trauma
After tertiary survey
i. Trauma remains primary and SCM signs off
ii. Trauma signs off, Ortho takes primary, SCM remains on case
Trauma provider re-assigns primary treatment team so that all teams are aware of responsibilities.
b. Ortho consult (called by Trauma provider)
c. SCM consult (called by Trauma provider)
d. Pain consult - Ortho confirms with patient they consent to a block; then calls APS (@ 402-650-9676) for FIB to be done within 4 hours.
e. DEM consult (L. Armas will be contacted by Ortho)
f. consider palliative care consult- can be consulted by any service
g. SW consult (call not needed, just order)
h. PT/OT consult on admission but not to begin evaluation or treatment until the morning after surgery. If arthroplasty, pt will have posterior hip precautions in place
i. Foley only if clinically indicated
3. Orders
a. Preoperative labs drawn
i. CBC, CMP, PT/INR/PTT
ii. Type and Screen. If Hgb < 8 Type and Cross.
iii. Vitamin D: 25(OH)D level **Need to specify mass spect method
b. Chest radiograph if clinically indicated (hx of heart or lung problems or sx)
c. ECG if clinically indicated (hx of heart problems or new sxs)
d. Pain Control
i. Fascia Iliac block* see protocol below (The Ortho provider should call the Anesthesia Acute Pain Service 24/7 @ 402-650-9676 to notify them of the patient). Block should be placed within 4 hrs. of APS notification. (Catheter to be removed at end of OR case)
ii. Tylenol 1000mg TID scheduled; 650mg po TID if history of liver disease
iii. Celebrex 100mg BID scheduled
iv. If age>70, start Oxycodone 2.5mg po Q 3 hours prn, Dilaudid 0.4mg Q2hour prn severe pain
v. If age<70, start Oxycodone 5mg po Q 3 hours prn, Dilaudid 0.6 mg Q2 hours prn severe pain
vi. Weight-bearing Orders – toe touch weight-bearing
vii. Activity as tolerated
e. Warfarin
i. Hold warfarin
ii. If arthroplasty planned, give Vitamin K 2.5 mg IV x1 ASAP (Do not wait for labs)
f. For patients admitted in the evening, keep NPO in anticipation of OR next day, for patients admitted in the morning keep NPO for possibility of OR the same day. Allow Ensure Pre- Surgery CHO drink evening before; consume before midnight
g. Hold ACE-Is and ARBs at admission to decrease the risk of intraoperative hypotension, restart POD #1
Continue ACE-Is and ARBs if systolic BP > 160
Continue ACE-Is and ARBs if LVEF know to be < 30%
h. Continue beta-blockers/rate control medications
i. Order 2000 IU Vitamin D3 daily
4. Patient taken to OR: Goal is patient in the OR next day after admission (Goal: 24-48 hrs.)
5. Postoperative Course
a. Standard postoperative antibiotics x 1 dose (orthopedics orders)
b. Postop CBC, BMP, other labs as needed or based on medical comorbidities, not routine
c. Evaluate pre op anticoagulation medication. Consider Lovenox 30 mg subQ q 12 hours (pharmacy consult for dosing) for VTE prophylaxis x 4 weeks to start POD#1
d. Calcium carbonate 1000 mg (400 mg of elemental calcium) start once daily with food
e. If arthroplasty - nursing communication order for arthroplasty- input full order set for mobility
f. If present, remove Foley on POD #1, straight cath. if retention
g. Goal discharge to home or facility is < 48 hours
h. Mobility: Encourage Dangle within 6-8 hours of surgery with QID ambulation beginning on POD 1, activity as tolerated, WB as tolerated
i. Diet: Patient may resume normal diet post op day 0, protein supplements with each meal/snacks
j. Patient up in chair for all meals x 3
k. Multimodal pain regimen to include combination of Tylenol/NSAIDs
iii. Tylenol 1000mg TID scheduled; 650mg po TID if history of liver disease
iv. Celebrex 100mg BID scheduled
v. Narcotic regimen per Arthroplasty Order Set
Oral Opioids - Moderate/Severe Pain (GFR 30 or less, age 79 yrs. or less)
oxycodone 5 mg, oral, every 2 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 12 hours PRN, moderate pain, severe pain
IV Opioids - Breakthrough Pain (GFR 30 or less, age 79 yrs. or less)
hydromorphone 0.5 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
Oral Opioids - Moderate/Severe Pain (GFR 30 or less, age 80 yrs. or more)
oxycodone 2.5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 12 hours PRN, moderate pain, severe pain
IV Opioids - Breakthrough Pain (GFR 30 or less, age 80 yrs. or more)
hydromorphone 0.2 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
Oral Opioids - Moderate/Severe Pain (GFR more than 30, age 79 yrs. or less)
oxycodone 5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
morphine 7.5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 6 hours PRN, moderate pain, severe pain
IV Opioids - Moderate/Severe Pain (GFR more than 30, age 79 yrs. or less)
morphine 2 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds OR
hydromorphone 0.5 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
Oral Opioids - Moderate/Severe Pain (GFR more than 30, age 80 yrs. or more)
oxycodone 2.5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 6 hours PRN, moderate pain, severe pain
IV Opioids - Moderate/Severe Pain (GFR more than 30, age 80 yrs. or more)
morphine 1 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds OR
hydromorphone 0.2 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
l. Vaccine reconciliation
m. Use of Recovery Milestone Checklist while in hospital
n. Develop Discharge Criteria
o. Gum chewing (sugar free) TID for 20 minutes
p. Utilize Static Meds Initiative (Early AM Meds to Beds delivery program)
6. Discharge: (3 appointments need to be made: bone health, orthopedics, primary care,
a. BONE HEALTH: with Dr. Armas
b. ORTHOPEDICS FOLLOW UP: Orthopedics team resident schedules Orthopedic Surgery
c. PRIMARY CARE: Primary team makes appointment with PCP within 2weeks
d. Primary service ensures detailed post-op instructions
i. Wound care/dressing
ii. PT/Activity
iii. Follow up anticipatory guidance
iv. Specific instructions on when to call the doctor (PCP vs Orthopedic Surgeon)
v. Updated medication list
vi. Continue calcium and vitamin D if they were on admission list or started inpatient.
Section Two: Specific Considerations for Anesthesia and Surgery
1. Anesthesia PreOp
a. Consider Neuraxial in all patients
b. Tranexemic Acid 1 gm IV at the beginning and end of the case
c. Any specific concerns for contraindications to surgery must be discussed between Attendings
2. Surgery
a. Arthroplasty: See pathway for anticoagulation
Case scheduled as Hip hemi-arthroplasty possible total hip.
b. CRPP/ORIF: See pathway for anticoagulation
Case scheduled as CRPP Hip, IMN Hip Fracture, Antegrade Femur Nail
c. Tranexemic Acid 1 gm IV at time of incision- same as spine
d. Standard preop antibiotics.
Section Three: Anticoagulation, Co-Morbidities and Specific Conditions
A. Anticoagulation
1. Anticoagulation for Arthroplasty (determined by Ortho upon eval in ED)
a. Antiplatelet agents
i. Continue Aspirin if history of CAD, stroke, TIA, or PAD. Irreversible antiplatelet effect persists for at least 5 days. If taking > 81 mg daily, reduce to 81 mg daily
ii. Discontinue P2Y12 inhibitors (clopidogrel, ticagrelor, or prasugrel) unless the patient is in the high risk window following coronary stent placement (policy MS54): Acute coronary syndrome within the past 12 months, bare metal stent in the past 1 month, or drug-eluting stent in the past 6 months
b. Warfarin (policy MP11)
i. If initial INR > 3, give additional Vitamin K 2.5 mg IV
ii. If initial INR > 1.5, type and cross for 2-4 units FFP
iii. Re-check INR 12 hours after vitamin K dose
iv. Goal INR for OR is 1.5 or less
v. Can proceed with surgery if INR 1.8 or less and patient can get FFP on the way to the OR (patient will receive GETA)
vi. Consider K Centra
d. DOACs (dibigatran, rivaroxaban, apixiban, edoxaban) (policy MS55)
i. Hold, clearly document time of last dose.
ii. Timing of surgery following last dose of DOAC
a. Factor Xa inhibitor (apixaban, edoxaban, rivaroxaban)
1. eGFR ≥ 30 = 24 hours
2. eGFR < 30 = 48 hours
b. Dabigatran
1. eGFR ≥ 80 = 24 hours
2. eGFR 30-80 = 48 hours
3. eGFR < 30 = 72 hours
c. Risks and benefits should be weighed by teams (ortho, medicine, geriatrics, and anesthesia) if delay > 24 hours is being considered.
2. Anticoagulation for ORIF/CRPP/IMN (Not arthroplasty)
a. Antiplatelet agents
i. Continue Aspirin if history of CAD, stroke, TIA, or PAD. Irreversible antiplatelet effect persists for at least 5 days. If taking > 81 mg daily, reduce to 81 mg daily
ii. Continue P2Y12 inhibitors (clopidogrel, ticagrelor, or prasugrel) if any of the following. Irreversible antiplatelet effect persists for at least 5 days. Acute coronary syndrome within the past 12 months, any cardiac stent, any peripheral artery stent, history of stroke or TIA
b. Warfarin
i. If initial INR > 3.0, administer Vitamin K 2.5 mg IV x 1
ii. If initial INR > 3.0, type and cross for 2-4 units FFP
iii. Goal INR for OR is 3.0 or less
iv. Can proceed with surgery if INR 3.0 or less
c. DOACs (dibigatran, rivaroxaban, apixiban, edoxaban)
i. Hold
ii. Do not delay surgery
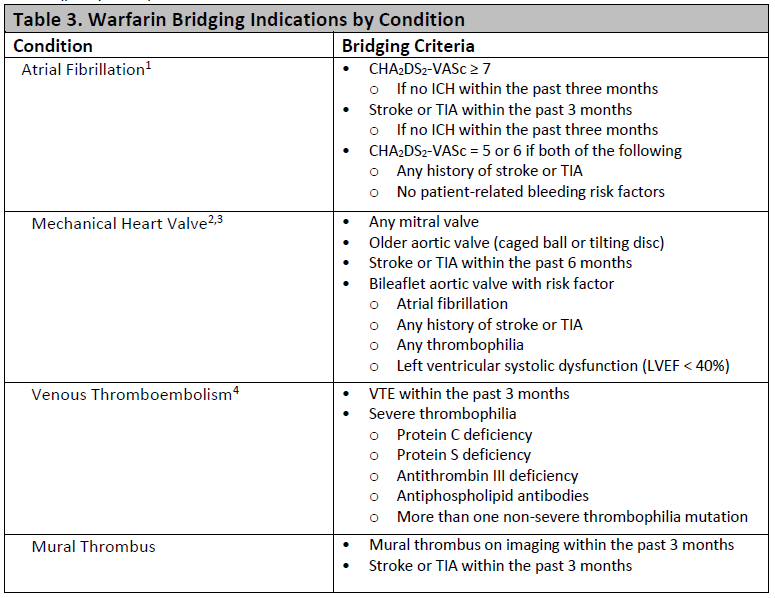
3. Bridging Anticoagulation
a. Bridging therapy applies only to patients taking warfarin
b. Bridging therapy with heparin indicated if any of the very high risk conditions below (policy MS55):
B. Comorbidity
Only unstable conditions should delay surgery. Evaluation of stable conditions must be completed within 24 hours of admission. If delay greater than 24 hours is anticipated, discussion between anesthesiology, Trauma, and hospital medicine is required within 8 hours of admission.
Statement of surgical readiness: One of these statements must be included in the SCM consultation report. If statement c is chosen, a discussion with anesthesiology, Trauma, and orthopedic surgery is required.
a. The patient is medically appropriate to proceed to surgery without further evaluation or management.
b. The patient will be medically appropriate to proceed to surgery when …
c. The patient is not medically appropriate to proceed to surgery. Delay or cancellation recommended.
Indications for surgical delay
a. Active Acute Coronary Syndrome (EKG changes or elevated troponin)
i. Cardiology consult
ii. Delay OR until optimized
b. Unstable Arrhythmia (hypotension or significantly uncontrolled)
i. Cardiology consult
ii. Delay OR until optimized
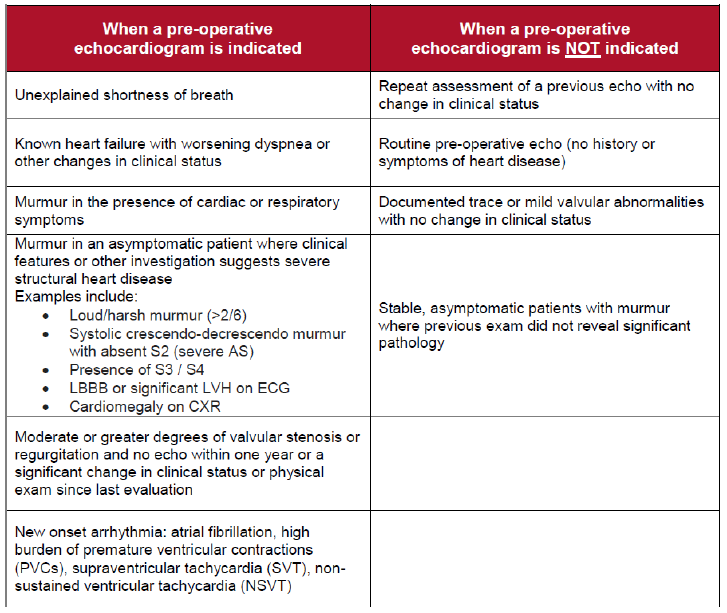
c. Decompensated CHF with new symptoms: see “Patients requiring an echo”
i. Obtain TTE,
ii. Cardiology consult
iii. delay OR until optimized
d. Acute respiratory failure
i. Obtain ABG for diagnosis of acute respiratory failure
a. SaO2 < 89
b. PO2 < 55
c. PCO2 > 55 with pH < 7.35
ii. Obtain pa/lat CXR, procalcitonin, b-natriuretic peptide
iii. Delay OR until optimized
e. Sepsis
i. Follow sepsis bundle for evaluation and treatment
ii. Delay OR until optimized
Other Comorbidity (not a reason to delay surgery)
a. Cardiac
i. Revised Cardiac Risk Index (RCRI) score: {NUMBERS 0 TO 6)
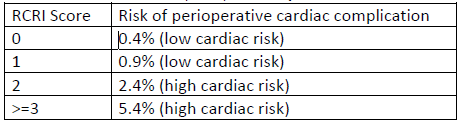
ii. Based on RCRI score and exercise tolerance:
a. Beta blockade indicated: continue if currently taking
b. Statin therapy indicated: continue if currently taking, start if indicated based on 10-year ASCVD risk
c. Inpatient telemetry monitoring recommendation: indicated if significant arrhythmia or RCRI score > 2
iii. Echocardiogram indications
b. Pulmonary
i. STOP-BANG score, OSA risk: (high risk if STOP-BANG > 5 or if known OSA not treated with CPAP)
ii. Management of high risk patients
a. Continuous oximetry
b. Continuous elevation of the head of the patient's bed
c. Complete avoidance of benzodiazepines and sedatives
iii. Management of home CPAP while inpatient
a. Begin CPAP therapy at home settings in the PACU and don't remove it for 48 hours unless the patient is eating or is out of bed.
b. After 48 hours, CPAP with sleep only
c. Diabetes or hyperglycemia (glucose > 180)
i. Avoid dextrose-containing IV fluid
ii. Hold oral diabetes medications while inpatient
iii. Institute basal-bolus insulin therapy
iv. Goal glucose 100-180
d. Hypertension
i. See above for ACEI and ARB management
ii. Continue other antihypertensive medication without interruption
iii. Goal BP < 180/105
e. Delirium
i. High risk for delirium if any of the following
a. Diagnosis of dementia or mild cognitive impairment
b. History of delirium
c. Age ≥ 80 years
e. Transfer from a facility
ii. Prevention of delirium in high risk patients
a. Avoid sedatives (including benzodiazepines and sleep aids) and anticholinergics (including scopolamine patch)
b. Minimize opioids as able.
c. Frequent re-orientation and opening of window shades during the day recommended.
d. Allow sleep
f. Stress dose steroids
i. Continue the patient's home oral steroid regimen without interruption perioperatively
ii. If the patient takes > 7.5 mg prednisone (or equivalent dose of another steroid) daily, administer stress dose steroids. Hydrocortisone 100 mg IV in pre-op followed by 50 mg IV every 8 hours for 3 total doses.
g. Alcohol Use- see CIWA and Phenobarbital protocols
Key Contributors
Zach Bauman,
UNMC Division of Acute Care Surgery, 2024
Isolated Orthopedic Injury Admission Guidelines
Purpose
· To identify which isolated traumatically injured patients can appropriately be admitted to the Orthopedic Service
Background/Definitions
Quality of care and length of stay continue to be areas for improvement at Nebraska Medicine. Given Orthopedic Surgery’s expertise and current workflow/resources, certain trauma patients with isolated Orthopedic issues, may be better served on the Orthopedic Service to improve quality of care and expedite disposition.
Guideline Inclusion Criteria
- Isolated traumatic fracture patients.
- Minimal medical problems or past medical issues which are currently stable and not exacerbated by the injury
- Deemed appropriate for admission to the Orthopedic Service by both the Trauma and Orthopedic Service.
- “Full” or “Limited” activations with isolated injuries.
Guideline Exclusion Criteria
- Poly-trauma patients with fractures.
- Deemed inappropriate for admission to the Orthopedic Service based on medical complexity. If the patient has minimal medical problems or past medical issues which are currently stable and not exacerbated by the injury, then the patient should be admitted to the Orthopedic service. It is highly encouraged for a Trauma/Orthopedic staff conversation in these situations
Diagnostic Evaluation
- Standard trauma work-up per ATLS standards.
- Routine trauma lab work.
- Body region X-ray and/or CT scan
- Pan scan CT as indicated by mechanism or provider discretion
- Trauma Team consultation to make sure trauma work up is complete and no other injuries are present. Also to evaluate appropriateness of Orthopedic Surgery admission.
- Orthopedic Surgery consultation to evaluate patient’s isolated traumatic injury and determine disposition (admission to hospital versus outpatient follow-up) as well as to evaluate appropriateness of Orthopedic Surgery admission.
Practice Recommendations for Management
Patient Entrance into Nebraska Medical Center
- Patients transferred in from an outside institution will be directed to Nebraska Medicine ED (ER→ER). Trauma Team will do the initial trauma evaluation and work-up in the emergency department.
- Patient primarily presents to NMC and meets criteria for an activation (Full or Limited), both the Emergency Medicine and Trauma Team will respond appropriately and the trauma work-up will be conducted as per usual.
- If the patient does not meet activation criteria, Emergency Medicine will perform the initial evaluation.
**If a fracture is identified, Trauma Surgery should be consulted for additional trauma evaluation to make sure the trauma work-up is complete. In all instances, they will be responsible for completion of the tertiary exam.**
Admitting Service and Consultant Involvement
- If a fracture is identified along with other injuries, Orthopedic Surgery will be consulted as well as other consulting services as needed
-
-
- Patient will be admitted to Nebraska Medical Center (NMC) by the Trauma Service for further trauma management as deemed appropriate.
-
-
- If an isolated fracture is identified, Orthopedic Surgery will be consulted for their recommendations.
-
-
- If the decision to admit the patient is made in order to repair the isolated fracture, Orthopedic Surgery will admit the patient to their service based on ACS requirements that trauma patients need to be admitted by a surgeon.
-
-
- If there is concern from the Trauma Service or Orthopedic Service that Orthopedics should not admit the patient, a staff-to-staff conversation should be held between the two services to decide which service the patient should be admitted to.
- Whether the patient needs surgery or not, the standard Nebraska Medicine Enhanced Recovery after Surgery (NERAS) pathway that has been established for isolated fracture patients will be followed.
-
-
- If the decision to admit the patient is made in order to repair the isolated fracture, Orthopedic Surgery will admit the patient to their service based on ACS requirements that trauma patients need to be admitted by a surgeon.
-
-
-
-
- If the decision to discharge the patient is made, the discharge paperwork should be completed by the accepting/managing team with outpatient follow-up orders to be placed by the Orthopedic Surgery service.
-
** Regardless of the admitting service, the Surgical Co-Management Service should be consulted for all fragility fractures (e.g. resulting from ground level fall) and in any other cases for which preoperative risk stratification is desired. **
Follow-up Care
- If the patient is a poly-trauma patient and admitted to NMC per the Trauma Service, discharge and follow-up recommendations will be provided by all consulting services as needed and PT/OT.
-
- All attempts will be made to discharge patient to appropriate location based on patient/family preferences, PT/OT recommendations, and discretion of the Trauma Service
-
- If the patient is an isolated fracture patient admitted to NMC per the Orthopedic Service, discharge and follow-up recommendations will be provided by Orthopedic Surgery and PT/OT.
-
- All attempts will be made to discharge patient to appropriate location based on patient/family preferences, PT/OT recommendations, and discretion of the Orthopedic Service.
-
Outcome Measures and Guideline Adherence
- All traumatically injured patients, whether poly-trauma or isolated Orthopedic injured patients, will be tracked and entered into the NMC and National Trauma Database.
- Performance improvement opportunities will be review by the appropriate service when needed based on the ACS pre-defined hospital complications (see ACS 2022 Trauma Standards Grey Category).
- Non-surgeon admissions of trauma patients will be tracked and updated monthly to the individual services as well as at the monthly PIPS meeting. Each non-surgeon admission will be reviewed per the PI process based on ACS Trauma Standards to determine appropriateness.
Key Contributors
- Zachary Bauman, DO, MHA
- Justin Siebler, MD
- Sara Putnam, MD
- Jason Schiffermiller, MD
Last Updated
February, 2024
References
- American College of Surgeons 2022 Trauma Standards
Orthopedic Trauma Discharge VTE Prophylaxis
Not Indicated:
- In general, VTE prophylaxis at discharge is not indicated for the following injuries:
-
- isolated upper extremity fractures (i.e. clavicle, humerus, elbow, forearm)
- non-operative isolated pelvic fractures (i.e. pubic rami, sacral ala)
-
Indicated:
- In general, if a patient has a lower extremity fracture and is NWB or TTWB for 6 weeks or greater, he/she will require VTE prophylaxis on discharge.
-
- Length of recommended VTE prophylaxis begins from the time of surgery for that particular orthopedic injury.
- If the patient has multiple orthopedic injuries undergoing operative fixation and requiring post-op VTE prophylaxis, pick the longest of the recommended therapies.
-
- While inpatient, a patient should remain on standard VTE prophylaxis for the trauma patient (typically Lovenox BID) and be continued on VTE prophylaxis upon discharge with the recommended therapy and remaining length of treatment as noted for each specific injury.
Recommendations:
- Operative Pelvis Fracture (i.e. pelvic ring, SI joint, pubic symphysis, acetabulum)
-
- VTE Prophylaxis: Lovenox 40 mg subcutaneous daily x 3 weeks followed by Aspirin 81mg PO BID x 3 weeks.
-
- Hip or Femur Fracture
-
- VTE prophylaxis: Lovenox 40mg subcutaneous daily x 3 weeks followed by Aspirin 81mg PO BID x 3 weeks
-
- Patella Fracture
-
- VTE prophylaxis: Aspirin 81 mg BID x 6 weeks
-
- Tibial Fracture
-
- VTE prophylaxis: Lovenox 40 mg subcutaneous daily x 3 weeks, followed by Aspirin 81 mg BID x 3 weeks.
- ***Unless stated otherwise in Dr. Putnam op-note: Aspirin 81 mg BID x 6 weeks
-
- Ankle Fracture
-
- Typical VTE prophylaxis: Aspirin 81 mg BID x 6 weeks
- Pilon fracture/Ex-fixed ankle: Lovenox 40 mg subcutaneous daily x 3 weeks followed by Aspirin 81 mg PO BID x 3 weeks.
- Low risk (no-comorbidities): Aspirin 81 mg BID x 30 days.
-
- Operative food fracture (i.e. calcaneous/tallus/navicular/cuboid)
-
- VTE prophylaxis: Aspirin 81 mg BID x 30 days
-
- Operative Lisfranc injuries (typically ex-fixed initially)
-
- VTE prophylaxis: Lovenox 40 mg subcutaneous daily x 3 weeks followed by Aspirin 81mg PO BID x 3 weeks.
-
- Lower extremity amputation
-
- VTE prophylaxis: none unless considered high risk (co-morbidities, other fractures, etc)
-
- Toe amputation
-
- Antibiotics: oral antibiotics until 1st follow-up appointment
- VTE prophylaxis: none
-
Management of Open Fractures
Purpose
Open fractures are high energy injuries that have increased risk of infection due to potential exposure of bone and deep tissue to a variety of environmental debris. Infection can lead to serious complications including nonunion of wounds and osteomyelitis.
Definitions
Gustilo-Anderson Classifications for open fractures
| Type I fracture |
open fracture with clean wound <1cm long |
| Type II fracture | open fracture with laceration >1cm long without extensive soft tissue damage |
| Type III (A-D) fracture | open segmental fracture, open fracture with extensive soft tissue damage, or traumatic amputation. |
Antibiotic Prophylaxis:
- Intravenous antibiotic prophylaxis should be given to patients with open fractures within 60 minutes of presentation to reduce the risk of infection.
- Antibiotic prophylaxis and duration is based upon the risk of infection utilizing the Gustilo-Anderson Classification System (listed above), with increasing rates of infection associated with higher grades.
- Please refer to: Antimicrobial Stewardship Program Open Fracture Prophylaxis Protocol on the Nebraska Medicine intranet (https://www.unmc.edu/intmed/divisions/id/asp/surgical-prophylaxis/index.html), or the EPIC order set entitled Antibiotic Prophylaxis for Open Fractures (304010005108) for specific antibiotics, dosing, and frequency.
Operative Treatment:
- Open fractures should be taken to the operating room on an urgent basis for irrigation and debridement within 24 hours of initial presentation or sooner whenever possible.
- When possible, skin defects overlying open fractures should be closed at the time of initial debridement.
Performance Improvement:
- All long bone open fractures will be monitored through the Trauma Performance Improvement Process. Specific indicators include:
-
- Time from arrival to first antibiotic dose.
- Time from arrival to initial irrigation and debridement.
-
References
- American College of Surgeons Trauma Quality Improvement Program. ACS TQIP Best Practices in the Management of Orthopedic Trauma. 2015. Retrieved from https://www.facs.org/~/media/files/quality-programs/trauma/tquip/ortho_guidelines.ashx.
- Anderson A, Miller AD, Bookstaver PB. Antimicrobial prophylaxis in open lower extremity fractures. Open Access Emergency Medicine. 2011;3:7-11. doi:10.2147/OAEM.S11862.
- Drunkel N, Pittet D, Tovmirzaeva L, Suva D, Bernard L, Lew D, Hoffmeyer P, Uckay I. Short duration of antibiotic prophylaxis in open fractures does not enhance risk of subsequent infection. The Bone and Joint Journal. 2013;95-B(6):831-837.
- Hauser CJ, Adams CA Jr., Eachempati SE. Surgical infection society guideline: Prophylactic antibiotic use in open fractures: An evidence-based guideline. Surgical Infections. 2006:74(4)379-405.
- Hoff WS, Bonadies JA, Cachecho R, Dorlac WC. EAST practice management guidelines work group: Update to practice management guidelines for prophylactic antibiotic use in open fractures. J Trauma Acute Care Surg. 2011;70(3):751-754.
- Rodriguez L, Jung HS, Goulet JA, Cicalo A, Machado-Aranda DA, Napalitano LM. Evidence-based protocol for prophylactic antibiotics in open fractures: Improved antibiotic stewardship with no increase in infection rates. J Trauma Acute Care Surg. 2014;77(3):400-408.
Author(s)
Justin Siebler, MD, Chief of Orthopedic Trauma
Last Updated
May, 2021
Mangled Extremity Management
Purpose: To aid in the rapid evaluation of a trauma patient presenting with a severely injured limb, providing a decision-making tool for limb salvage vs. amputation in a multidisciplinary fashion.
Background: Patients with a mangled extremity, defined as an extremity with an injury to at least three out of four systems (soft tissue, bone, nerves, and vessels) represent a high-risk patient population requiring expedient care to salvage life and limb. These patients frequently have multi-system and life-threatening injuries and balancing these issues is extremely important. Prompt re-establishment of vascular integrity and fracture stabilization is imperative for limb salvage, when possible. The coordination of multiple surgical services (Trauma, Orthopedics, Vascular, and Plastics) is essential.
Limb salvage versus amputation
Current injury severity scoring systems, specifically the Predictive Salvage Index (PSI) and Mangled Extremity Severity Score (MESS), for mangled extremities do not predict functional recovery of patients who undergo successful limb reconstruction. Limb salvage should be attempted if the other injuries are minimal, the patient is hemodynamically stable and the extremity injuries are amendable to salvage. The involved faculty should have a brief but focused discussion in the OR regarding priorities of care.
Questions for the teams involved:
Orthopedics: can the bone ultimately be saved/reconstructed and/or temporarily stabilized?
Vascular: can the acute arterial injury (if present) be repaired or bypassed in a timely fashion?
Trauma surgery: is the patient stable enough hemodynamically and metabolically to undergo acute revascularization and a prolonged reconstruction?
Plastic surgery: can the wound ultimately be covered or managed? (may be difficult to tell at initial presentation, but should weigh in)
If there is consensus among the involved teams, i.e. all the answers are affirmative to the above questions, then proceed with limb salvage (revascularization/reconstruction procedures). If one or many of the answers to the above questions are are in the negative then proceed with acute amputation.
All services must document their agreement of findings accordingly.
Indications for early amputation:
· Hemodynamic and physiologic instability secondary to complex injured extremity as determined by Trauma surgery faculty, i.e. “life over limb”
· unreconstructible osseous injuries as determined by Orthopedic surgery faculty
· unreconstructible soft tissue injuries as determined by Plastic Surgery faculty
· irreparable vascular injuries as determined by Vascular or Trauma Surgery faculty
· severe loss of soft tissue
Indications for limb salvage:
· all other patients not meeting above criteria
Updated:
· September 2023
Authors
Abby Josef, MD
References:
Ly TV, Travison TG, Castillo RC, Bosse MJ, MacKenzie EJ, LEAP Study Group. Ability of lower-extremity injury severity scores to predict functional outcome after limb salvage. J Bone Joint Surg Am. 2008;90: 1738-1743.
Prasarn ML, Helfet DL, Kloen P. Management of the mangled extremity. Strat Traum Limb Recon. 2012;7: 57-66.
Bonanni F, Rhodes M, Lucke JF. The futility of predictive scoring of mangled lower extremities. J Trauma.1993;34:99-104.
Potter BK, Bosse MJ. American Academny of Orthopaedic Surgeons Clinical Practice Guideline Summary for Limb Salvage or Early Amputation. J Am Acad