9. Thermal Injury
Educational material and pathways regarding the management of thermal injury.
- Care of Trauma Patient with Accidental Hypothermia Practice Guidelines
- Guidelines for the Initial Management of Frostbite
- Initial Management of Burns
- Thrombolytic Therapy for the Management of Severe Frostbite
Care of Trauma Patient with Accidental Hypothermia Practice Guidelines
Purpose:
The purpose of this practice guideline is to provide guidance and standardize the approach to the management of trauma patients with accidental hypothermia.
Definition:
Hypothermia is defined as the involuntary drop of core temperature below 36°C (95°F). Symptoms vary based on severity of hypothermia (see section A. Clinical Signs).
A. Clinical Signs
|
Hypothermia |
Body temperature |
Clinical features |
|
|
Mild |
32.2°C to 36°C (90°F to 96.8°F) |
||
|
Hypertension |
|||
|
Shivering |
|||
|
Tachycardia |
|||
|
Tachypnea |
|||
|
Vasoconstriction |
|||
|
Apathy |
|||
|
Ataxia |
|||
|
Cold diuresis—kidneys lose concentrating ability |
|||
|
Hypovolemia |
|||
|
Impaired judgment |
|||
|
Moderate |
28°C (82.4°F) to 32.2°C (90°F) |
Atrial dysrhythmias |
|
|
Decreased heart rate |
|||
|
Decreased level of consciousness |
|||
|
Decreased respiratory rate |
|||
|
Dilated pupils |
|||
|
Diminished gag reflex |
|||
|
Extinction on shivering |
|||
|
Hyporeflexia |
|||
|
Hypotension |
|||
|
J wave |
|||
|
Severe |
< 28°C (82.4°F) |
||
|
Coma |
|||
|
Decreased or no activity on electroencephalography |
|||
|
Nonreactive pupils |
|||
|
Oliguria |
|||
|
Pulmonary edema |
|||
|
Ventricular dysrhythmias/asystole |
|||
B. General Principles
- Room temperature should be maintained at approximately 85ºC (29.4ºF). Use of overhead heating lamps should be considered in the trauma bay.
- Rewarming of the trunk should be undertaken BEFORE the extremities to minimize hypotension and acidemia due to arterial vasodilation and core temperature drop.
- Initiate or maintain CPR if required – Palpate pulse for full minute – An initial attempt at defibrillation can be made but if unsuccessful, further attempts at defibrillation and antiarrhythmic intravenous medications should be held until the patient is warmed to above 30°C.
- Gingerly handle patients to reduce risk of inducing malignant dysrhythmia.
C. Re-Warming
- Mild Hypothermia 32.2°C to 36°C (90°F to 96.8°F)
-
- Room temperature should be maintained at approximately 85ºC (29.4ºF).
-
- Remove all wet clothing.
- Obtain rectal temperature. If temperature will not register, insert a temperature sensing foley catheter or rectal probe thermometer.
-
- Rewarm patient using passive and active external rewarming:
-
- Heated blankets in neck, groin, axilla, torso
- Bair Hugger
-
- RT to place on warmed, humidified O2.
- Infuse Warm intravenous (IV) Fluids:
-
- Warmed isotonic crystalloids or
- Place IV fluids on rapid infuser to utilize warming mechanism. Adjust flow rate so fluids are not delivered at rapid rate unless there is an indication for rapid fluid resuscitation.
-
- Room temperature should be maintained at approximately 85ºC (29.4ºF).
-
- Moderate to Severe Hypothermia 28°C to 32.2°C (82.4°F - 90°F) to < 28°C (<82.4°F)
-
- Obtain temperature using either temperature sensing foley, esophageal temperature sensing probe or rectal temperature sensing probe (if utilizing gastric and/or bladder lavage, use the rectal temperature sensing probe).
- Employ all interventions listed under mild hypothermia.
- Consider use of Artic Sun device.
- Consider use of body bag to maintain the warm air around the patient.
- Per MD order, assist with active internal rewarming via:
-
- Gastric lavage
- Bladder lavage
- Peritoneal lavage
- Thoracic lavage
-
- Continuous Veno-Venous Hemodialysis (CVVHD) – Consider consulting nephrology for initiation of CVVHD.
- Extracorporeal Membrane Oxygenation (ECMO) – Consider consulting ECMO team and Cardiothoracic Surgery for initiation of ECMO.
-
D. Rate of Rewarming
- Slow rewarming - increases temperature by approximately 0.3-1.2°C/h.
-
- Warmed IV solutions.
- Heated, humidified oxygen by mask/endotracheal tube.
- Warmed blankets and/or Bair Hugger
-
- Moderate rewarming – increases temperature by approximately 3°C/h.
-
- Artic sun
- Warmed gastric lavage
- Warmed bladder lavage
- Warmed peritoneal lavage
-
- Rapid rewarming – increases temperature by approximately 6°C – 19°C/h.
-
- Warmed thoracic lavage
- CVVHD
- ECMO
-
E. Traumatic hypothermic cardiac arrest
1. Continuation of resuscitation in traumatic hypothermic cardiac arrest will be at the discretion of the trauma surgeon and/or emergency medicine physician in accordance with previously established guidelines for traumatic cardiac arrest resuscitation (Reference 1,2,7).
References:
- American College of Surgeons. (2018). Advanced trauma life support: Student course manual.
- Burlew, C., Moore, E., Moore, F., Coimbra, R., McIntyre Jr., R., Davis, J, Sperry, J., & Biffl, W. (2012). Western Trauma Association critical decisions in trauma: Resuscitative thoracotomy. Journal of Trauma and Acute Care Surgery, 73(6),1359-1363.
- Duong H, Patel G. Hypothermia. [Updated 2021 Jan 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545239/
- Essentials of Emergency Medicine, Chapter 6, Temperature Related Disorders, 2006
- Paal, P., Brugger, H., & Strapazzon, G. (2018). Accidental hypothermia. In Romanovsky, A. (Ed), Thermoregulation: From basic neuroscience to clinical neurology (pp.547-561). Elsevier Science Inc. https://doi.org/10.1016/B978-0-444-64074-1.00033-1
- Paal, P., Gordon, L., Strapazzon, G., Brodman Maeder, M., Putzer, Walporth, B., Wansher, M., Brown, D., Holzer, M., Broessner., & Brugger, H. (2016). Accidental hypothermia-an update. Scandinavia Journal of Trauma, Resuscitation and Emergency Medicine, 24, 111. doi: 10.1186/s13049-016-0303-
- Seamon, M., Haut, E., Van Arendonk, K., Barbosa, R., Chiu, W., Dente, C., Fox, N., Jawa, R., Khwaja, K., Lee, J., Magnotti, L., Mayglothling, J., McDonald, A., Rowell, S., To, K., Falck-Ytter, Y., & Rhee, P. (2015). An evidence-based approach to patient selection for emergency department thoracotomy: A practice management guideline from the Eastern Association for the Surgery of Trauma. Journal of Trauma and Acute Care Surgery, 79(1), 159-173.
- StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan. Available fro
- Zafren, K., & Giesbrecht, G. (2014, July). State of Alaska: Cold injuries guidelines. http://dhss.alaska.gov/dph/emergency/documents/ems/documents/alaska%20dhss%20ems%20cold%20injuries%20guidelines%20june%202014.pdf
Developed by: Trauma Program Coordinator
Reviewed by: Trauma Operations Committee and Trauma Performance Improvement and Patient Safety (PIPS) Committee
Last Updated
February, 2022
Guidelines for the Initial Management of Frostbite
Purpose:
- Provide guidance on the initial evaluation and management of patients sustaining frostbite injuries as well as recommendations regarding wound care and soft tissue management.
Background/definitions:
- Frostbite is the tissue damage resulting from exposure to cold temperatures, usually from freezing of tissues, which results in cellular damage and tissue necrosis. The extent of frostbite depends on the temperature and duration of exposure.
Guideline Inclusion Criteria:
- Patients with history of recent cold exposure with evidence of soft tissue injury (frostbite) presenting to UNMC/NM emergency department
Guideline Exclusion Criteria:
- Patients without history of recent cold exposure
- Patients with history of cold exposure but without evidence of soft tissue injury 72 hrs after exposure.
- Referrals/transfers from outside hospitals—These patients should be referred to closest regional burn center.
Diagnostic Evaluation:
- Diagnosis of frostbite is based on history and clinical exam.
- History:
- Patients should have clinical history consistent with diagnosis of frostbite (i.e. exposure to cold or wet environment)
- Physical exam:
- Frostbite most commonly occurs on hands, feet, ears, and nose. However, can be present on any part of the body exposed to cold or wet conditions for a period of time.
- Findings consistent with frostbite include:
-
- Initially reddish (lighter skin), grayish (darker skin), pale/white or bluish/cyanotic discoloration in involved tissues.
- Tingling, stinging sensations or decreased/loss of sensation
- Involved tissues feel cold, stiff, or woody to palpation
- Blisters may or may not be present on initial examination but often develop over first 24-48 hours
-
- Additional labs and imaging should be obtained at physician discretion based on clinical status of patient, length of cold exposure, associated trauma, need for resuscitation, etc.
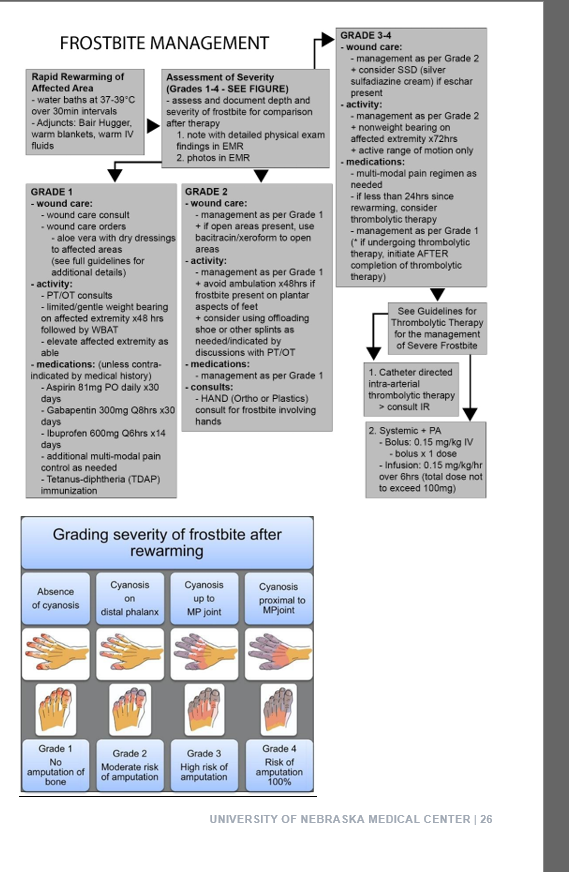
Practice Recommendations for Management:
- Initial frostbite management:
- Remove any wet clothing.
- Assess and resuscitate hypothermic patients as indicated (see hypothermia guidelines)
- Avoid re-freezing.
- Rapid re-warming of injured parts
-
- Water baths at temperatures of 37⁰-39⁰ C (98.6⁰-102.2⁰F) over 30 minute intervals is recommended.
- Other methods for active re-warming include: warm IV fluids, warm blankets, Bair hugger, etc.
- Clinical findings, such as the return of sensation, presence of flushing in involved tissues, and involved tissues are pliable or soft (i.e. not hard and frozen), will determine the length of time of rewarming.
-
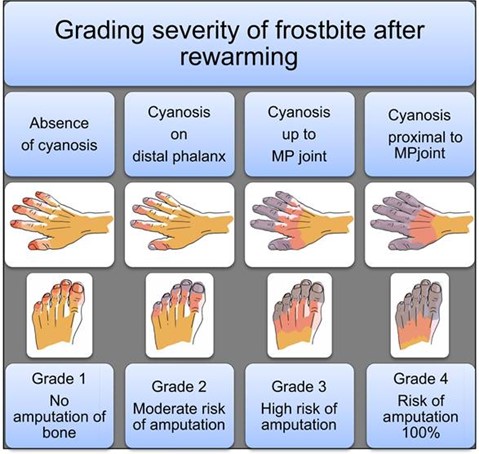
- Determine grade and depth of frostbite
-
-
-
-
- Depth
-
- Superficial – no blisters present
- Partial thickness – serous blisters present
- Full thickness – hemorrhagic blisters present
-
- Depth
-
-
-
-
-
-
-
- patients with grade 3 or 4 frostbite (cyanosis persisting proximal to the distal phalanx after rewarming) and/or demonstrated loss of perfusion at or proximal to the proximal interphalangeal joint of a finger or toe, or the interphalangeal joint of the great toe or thumb immediately after rewarming, consider thrombolytic therapy. (see Guidelines for Thrombolytic Therapy for Frostbite)
-
-
- Pain control:
-
- The re-warming process is often painful and analgesics (including narcotics) should be provided on an as needed basis.
-
- Tetanus prophylaxis should be provided if not up to date/given in the last 5 years.
- Patients should be kept NPO until initial evaluation is complete and need for thrombolytic therapy ruled out.
- Determine need for admission.
-
- If admission required, patients should be admitted to the trauma service.
-
-
- Photos:
- Photo documentation of wounds should be obtained on admission, 24 hours following admission and then serially every 2 days thereafter until discharge.
- Initial Wound care of frostbite
- Wound Care consult should be placed on admission.
- Wound care should be performed twice daily with nursing orders for wound care as indicated.
- Suggested soft tissue management:
-
- Recommendations regarding wound care and activity are based on depth of injury.
- Of note, frostbite may take up to 72 hrs before the depth of frostbite becomes apparent. (i.e. blisters form)
- Superficial thickness:
-
- No blisters present
- Wound care: consider aloe vera, place dry dressings, keep warm
- Activity: limited/gentle weight bearing of affected extremity for the first 48 hrs until soft tissue has fully declared. Following this, may weight bear as tolerated. Keep affected extremity elevated as able.
-
- Partial thickness:
-
- Serous blisters present
- Wound care:
- Activity: Avoid ambulation if on plantar aspects of feet. Otherwise, limited/gentle weight bearing and active range of motion of affected extremity for the first 48 hrs until soft tissue has fully declared. Following this, may weight bear as tolerated. Keep affected extremity elevated as able.
-
- Full thickness
-
- Hemorrhagic blisters present
- Wound care:
-
- blisters do not generally require debridement.
- Dress blisters and open areas in bacitracin followed by xeroform and gently secured with gauze. Avoid tight dressings.
-
- Activity: No weight bearing on the affected extremity for 72 hours. Active range of motion only. Keep affected extremity elevated.
-
- Additional topical agents:
-
- Choice of topical agents may vary between providers and can include (but are not limited to) the following:
-
- Aloe vera – topical thromboxane inhibitor
- Bacitracin – topical antibiotic
- Silver sulfadiazine – topical antibiotic
-
- Choice of topical agents may vary between providers and can include (but are not limited to) the following:
-
-
-
-
-
- Cotton, web roll, or lambs wool should be placed between digits/toes for extra protection and warmth.
- Affected extremities should be elevated with splinting/padding (i.e. Rooke boots) as needed
- For those patient’s with frostbite of the feet, ambulation should occur in protective footwear (i.e. off-loading shoe)
- PT/OT consults should be placed on admission to assist in mobility, range of motion and splinting of the affected extremity as indicated.
- In general, similar to burns, frostbite injuries will evolve over the first 72 hours and can take an extended period of time to demarcate. Waiting until the full extent of necrosis is apparent is recommended prior to surgical amputation (if needed) to allow for as much tissue salvage as possible.
- For patients with Grade 2, 3, and 4 frostbite where amputations may be required, inpatient consultation of orthopedic or plastic surgery may be obtained as needed at the discretion of the trauma attending.
-
-
- Medications for frostbite injury:
- Anti-platelet plus analgesia therapies
-
- The following regimen should be initiated on admission for any frostbite patient NOT undergoing thrombolytic therapy or AFTER completion of thrombolytic therapy/therapeutic anticoagulation in grade 3 or 4 frostbite patients unless contraindicated by medical history (i.e. renal insufficiency, h/o PUD/GI bleed, recent intracranial hemorrhage, etc.)
-
- Aspirin 81mg PO daily x 30 days
- Gabapentin 300 mg q8 hrs x 30 days
- Ibuprofen 600 mg q6 hrs x 14 days
-
- The following regimen should be initiated on admission for any frostbite patient NOT undergoing thrombolytic therapy or AFTER completion of thrombolytic therapy/therapeutic anticoagulation in grade 3 or 4 frostbite patients unless contraindicated by medical history (i.e. renal insufficiency, h/o PUD/GI bleed, recent intracranial hemorrhage, etc.)
-
- Additional multi-modal pain control should be provided as needed.
- In general, prophylactic antibiotics are not indicated.
- Anti-platelet plus analgesia therapies
Admission Guidance:
- Acute frostbite (<72 hours since cold exposure):
- Admit to trauma
-
- Consult orthopedics for management and outpatient follow-up
- Consult hand for upper extremity frostbite and outpatient follow-up
-
- Admit to trauma
- Chronic wounds secondary to frostbite (>72 hours since cold exposure):
- If no other injuries or hypothermia, admit to primary home admitting service (Hospital Medicine, UNMC family medicine, or Clarkson Family Medicine
-
- Consult orthopedics for management and outpatient follow-up
- Consult hand for upper extremity frostbite and outpatient follow-up
-
- If no other injuries or hypothermia, admit to primary home admitting service (Hospital Medicine, UNMC family medicine, or Clarkson Family Medicine
- Frostbite re-admissions
- Admit to primary home admitting service (Hospital Medicine, UNMC family medicine, or Clarkson Family Medicine), NOT trauma
-
- Consult orthopedics for management and outpatient follow-up
- Consult hand for upper extremity frostbite and outpatient follow-up
-
- Admit to primary home admitting service (Hospital Medicine, UNMC family medicine, or Clarkson Family Medicine), NOT trauma
Follow-up Care:
- Patients with frostbite injuries will follow-up in trauma surgery clinic for ongoing wound care with referrals to orthopedic or plastic surgery clinics as needed.
Outcome Measures and Guideline Adherence:
- Track patients with Grade 2 and higher frostbite every 6 months for adherence to guidelines
- Measures: status of wounds, need for amputation, need for thrombolytic therapies, involvement of consulting services (orthopedics, plastic surgery, wound care clinic, etc)
Related Policies:
- Hypothermia Guidelines
- Thrombolytic Therapy for the Management of Severe Frostbite
Key Contributors:
· Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
· Abby Josef, MD | Division of Acute Care Surgery, Faculty | Author
· Zach Bauman, MD | Division of Acute Care Surgery, Faculty | Author
· Ashley Farrens | Division of Acute Care Surgery, Trauma Program Manager | Reviewer
· Meghan Blais, PharmD | Clinical Pharmacist, Nebraska Medicine | Reviewer
Last updated:
· 11/19/2025
References:
- Zaramo TZ, Green JK, Janis JE. Practical review of the current management of frostbite injuries. Plast Reconstr Surg Glob Open. 2022 Oct 24;10(10):e4618
- Murphy JV, Banwell PE, Roberts AH, McGrouther DA. Frostbite: Pathogenesis and treatment. J Trauma. 2000 Jan;48(1):171-8.
- Hickey S, et. al. Guidelines for thrombolytic therapy for frostbite. J Burn Care Res. 2020 Jan 30;41(1):176-183.
- Lacey AM, et al. An institutional protocol for the treatment of severe frostbite injury—A 6-year retrospective analysis. J Burn Care Res. 2021 Aug 4;42(4):817-820.
Initial Management of Burns
Purpose:
Provide a brief overview of the classification of burns, initial resuscitation and management, as well as guidelines on triage.
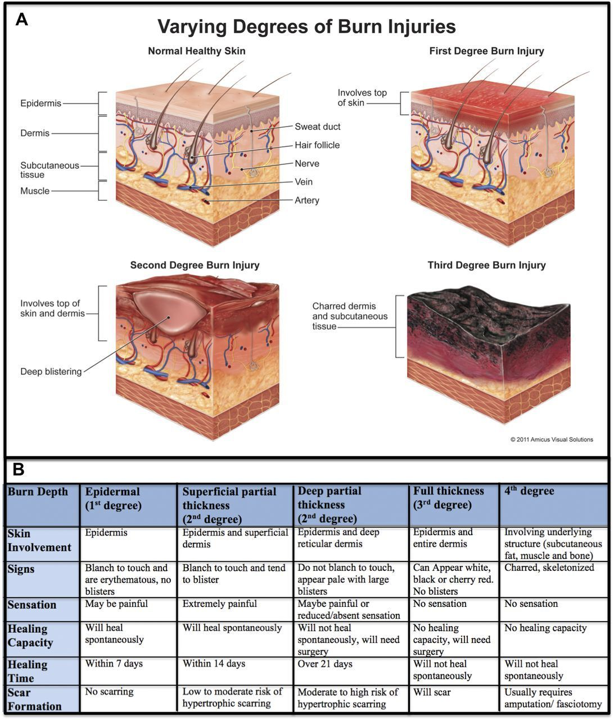
Classification of Burn Injuries:
- First Degree Burn (superficial)
- Involves only the epidermis (no penetration into the dermis)
- Skin appearance: warm, erythematous, no blistering or eschar present
- Painful
- Management: supportive cares (i.e. pain management, aloe vera or soothing lotions); these burns are typically self-limiting, do not scar and will heal without intervention.
- Second Degree Burns (partial thickness)
- Superficial Partial Thickness
-
- Involves the epidermis and papillary dermis
- Skin appearance: blistering, red or pink, moist, blanches with pressure
- Extremely painful
- Management: will usually heal with local wound care; low potential for scarring
-
- Deep Partial Thickness
-
- Involves epidermis, papillary dermis and reticular dermis
- Skin appearance: blistered, waxy, variable in color from red/pink to white, non-blanching
- Less painful
- Management: few smaller burns will heal with good wound care but most will require surgical excision and grafting; high risk for scarring and pigment changes
-
- Superficial Partial Thickness
- Third Degree Burn (full thickness)
- Penetration through epidermis/dermis and into subcutaneous tissues
- Skin appearance: dry, inelastic, waxy or leathery, non-blanching, white/yellow/brown in color with eschar.
- Insensate, not painful
- Management: will not heal without intervention, often requires surgical excision and grafting; high risk for scarring and contractures
- Fourth Degree Burn
- Extends down into the muscle, tendon, or bone
- Skin appearance: charred, black, skeletonized
- Insensate
- Management: will not heal without intervention; often requires surgery/amputation.
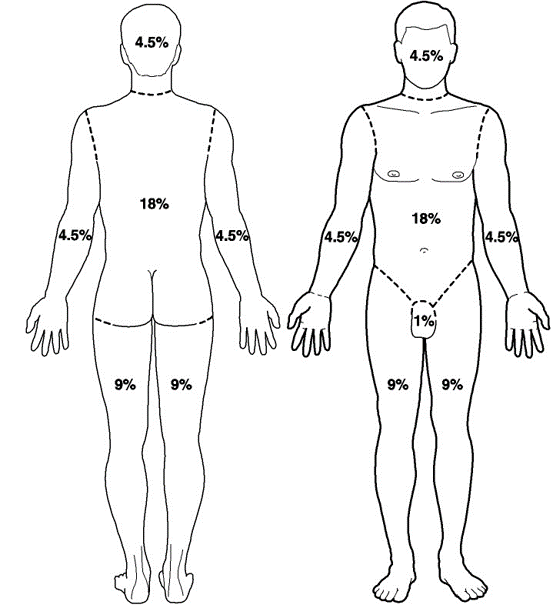
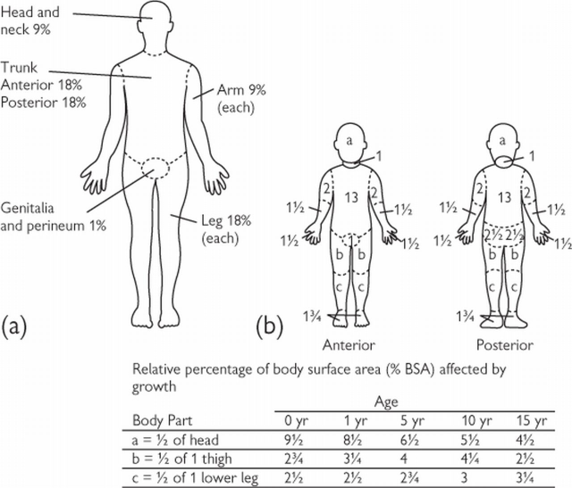
Extent of Burn Injuries
- Accurate determination of burn size ensures proper treatment and resuscitation
- The total body surface area (TBSA) of burns in adults can be estimated using the “Rule of Nines” or by using the patient’s open palm to equal approximately 1% TBSA.
 \
\ - Since body proportions in children differ with age, TBSA in children should be estimated using a Lund-Browder chart (see below) or by using the patient’s open palm to equal approximately 1% TBSA.
Burn Resuscitation
- The initial approach to a burn resuscitation is similar to standard ATLS
- Please see Special Considerations regarding Inhalational Injury and Escharotomies
- Volume Resuscitation is based upon the % TBSA, age, and weight of the patient
-
- TBSA > 20% require formal resuscitation in all ages
- TBSA > 10% require resuscitation in children and elderly patients
-
- American Burn Association Consensus Formula
-
- 2-4 ml/kg/% TBSA (using LR) in the first 24 hours
- Give 1/2 in the first 8 hours
- Give 1/2 in the subsequent 16 hours
-
- Adults: 2 mL/kg/% TBSA
- Children: 3 mL/kg/% TBSA
-
- Adjust fluid rate for goal urine output 1 cc/kg/hr if child < 14 yr
- If child is < 30 kg, add maintenance fluids that include dextrose (D5LR or D5 1/2 NS) in addition to the consensus formula
-
- Electrical: 4 mL/kg/% TBSA
- Initial Wound Care
-
- Wrap wounds with clean, dry gauze, wrapped in Kerlix
-
- Please note that any dressings or wound care performed will be quickly removed upon transfer to the referring hospital
-
- Wrap wounds with clean, dry gauze, wrapped in Kerlix
-
- Other caveats
-
- Pain Control
- Clarify time of burn and crystalloid received prior to arrival into calculations for initial burn resuscitation
- Update Tetanus
- Consider Cyanokit with appropriate mechanism/circumstances of burn and/or markedly high lactic acidosis
-
Special Considerations
- Inhalational Injury
-
- Significantly increases morbidity and mortality of burn patients
- Present in approximately 1/3 of burn patients
- Injury due to 1. direct injury, 2. edema leading to airway obstruction, and 3. massive inflammatory response
- Diagnosis is subjective and objective
-
- History: mechanism, duration of exposure, location
- Exam: facial burns, singed facial/nasal hair, carbonaceous sputum, soot in oropharynx, voice hoarseness, stridor, erythema and/or edema of the oropharynx
- Work-up: carboxyhemoglobin, chest x-ray, ABG, oxygen saturations
- Flexible bronchoscopy is the gold standard for diagnosis.
-
- Treatment
-
- Supplemental oxygen and pulmonary toilet
- Need for intubation/mechanical ventilation at discretion of the Trauma and ED providers
- Adjuncts: beta-agonists, nebulized acetylcysteine (NAC) and/or heparin, nebulized racemic epinephrine
-
-
- Electrical Burns
-
- Arc burn
-
- Generated by heat from an electrical arc
- Similar treatment to thermal burns
-
- Current burn
-
- Electrical current passes through the body
- Entrance and exit marks are common, as is history of tetany
- Risk for compartment syndrome; evaluation of compartments in an obtunded patient should be performed
-
- Arc burn
-
- Chemical Burn
-
- Identify the chemical, mechanism of exposure, and duration of exposure
- Remove contaminated clothing and follow decontamination protocol per hospital/facility policy
- Affected areas should be copiously irrigated with water
-
- Do not attempt to neutralize the solution as this can result in heat production and worsen injury
-
-
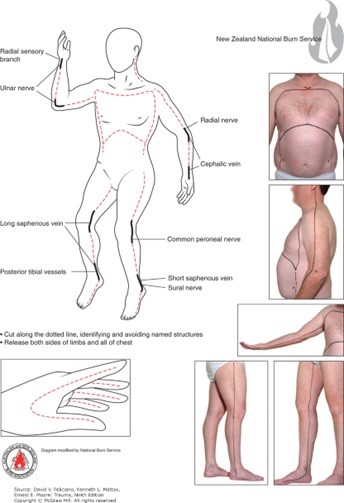
- Escharotomy
-
- Surgical division of nonviable eschar is sometimes required in deep partial and full thickness burns
- The inelastic tissue of the eschar can cause a tourniquet effect over inflamed extremities/compartments and body cavities
- Most commonly performed in extremities with circumferential deep partial or full thickness burns; but may also be required in the neck (airway compromise), chest (diminished chest wall compliance resulting in inadequate ventilation/oxygenation) and abdomen (abdominal compartment syndrome)
- Procedure:
- division through the epidermal and dermal layers (eschar) into the subcutaneous fat following the LAID pneumonic (Longitudinal incisions, axial planes, into normal skin, down into subcutaneous fat)
- usually performed at bedside with sterile drapping
- utilize electrocautery device
- have adequate analgesia and sedation available

-
- Non-Accidental Trauma
-
- Burns in children can be the result of child abuse or neglect
- Maintain a high index of suspicion for burns presenting with inconsistent stories for how burn occurred or those presenting in "stocking patterns" suggestive for water immersion burns that are uniform in nature and have a well demarcated line indicated depth of immersion
-
Burn Referral Criteria
- A burn center may treat adults, children, or both. Burn injuries that should be referred to a burn center include the following:
-
- Partial-thickness burns of > 10 % of the TBSA.
- Burns that involve the face, hands, feet, genitalia, perineum, or major joints.
- Third-degree burns in any age group.
- Electrical burns, including lightning injury.
- Chemical burns.
- Inhalation injury.
- Burn injury in patients with preexisting medical disorders that could complicate management, prolong recovery, or affect mortality.
- Burns and concomitant trauma (such as fractures) when the burn injury poses the greatest risk of morbidity or mortality. If the trauma poses the greater immediate risk, the patient’s condition may be stabilized initially in a trauma center before transfer to a burn center. Physician judgment will be necessary in such situations and should be in concert with the regional medical control plan and triage protocols.
- Burns in children; children with burns should be transferred to a burn center verified to treat children. In the absence of a regional pediatric burn center, an adult burn center may serve as a second option for the management of pediatric burns.
- Burn injury in patients who will require special social, emotional, or rehabilitative intervention.
- Trauma Surgeon Discretion
-
Regional Burn Centers Contact Information
- Isolated Burn
- St. Elizabeth’s Burn Center, Lincoln, NE
-
- Transfer Line 1st: (800) 877-2876
- Burn RN Station: (402) 219-7680
- Fax: (402) 219-8773
- Outpatient Burn Clinic: (402) 219-8770
-
- St. Elizabeth’s Burn Center, Lincoln, NE
- Burn with Traumatic Injuries
-
- University of Kansas (KU) Medical Center, Kansas City, KS: 1-877-738-7286
- University of Iowa Medical Center, Iowa City, IA: 1-866-890-5969
-
Note: Requests for photographic evidence of burns sent over SMS/Text are not HIPAA protected and therefore not permitted
Contributors
Last Updated: Feb 14, 2023
References:
1. Levi, Benjamin; Vercruysse, Gary. 2021. Chapter 51: Burns and Radiation. Trauma, 9e. Feliciano DV, Mattox KL, Moore EE. McGraw Hill.
2. Resources for Optimal Care of the Injured Patient. Guidelines for Trauma Centers Caring for Burn Patients. American College of Surgeons, Committee on Trauma, Chicago, Ill. 2014
3. Chapter 9: Thermal Injuries. Advanced Trauma Life Support (ATLS®): The Tenth Edition. 2018. ATLS Subcommittee. American College of Surgeons’ Committee on Trauma; International ATLS working group. Chicago, IL. American College of Surgeons
Thrombolytic Therapy for the Management of Severe Frostbite
Purpose
- Provide guidance on the administration of thrombolytic therapy (t-PA) for the purpose of improving tissue perfusion in the management of severe frostbite injuries.
Background/Definitions
- Frostbite is the tissue damage resulting from exposure to cold temperatures, usually from the freezing of tissues, which results in cellular damage and tissue necrosis. The extent of frostbite depends on the temperature and duration of exposure.
- In more severe forms, frostbite can impair perfusion to digits and extremities.
Inclusion Criteria
- Patients with severe frostbite (grades 3 or 4) in the distal limbs and digits with:
- Absent or weak doppler signals in limbs and/or digits, and no improvement after rewarming OR no perfusion on bone scan.
- Less than 24 hrs of warm ischemia time (defined as time from passive or active rewarming)
Exclusion Criteria
- Contraindications to thrombolytic agents in frostbite include:
-
- Repeated freeze-thaw cycles
- Concurrent or recent (within 30 days) intracranial hemorrhage or traumatic injury with active bleeding
- Recent (within 3 months) intracranial or intraspinal surgery
- Recent (within 3 months) serious head trauma or stroke
- History of gastrointestinal bleeding
- Current severe and uncontrolled hypertension (SBP>180 mm Hg and/or DBP>105 mm Hg)
- Pregnancy
- Uncorrected coagulopathies (INR>1.7, PT>50, PTT>40)
- Thrombocytopenia (Platelets <50)
- Recent hemorrhage or bleeding diasthesis
- Drug or alcohol intoxication
-
(Healthcare provider discretion may override some contraindications as patient's condition warrants)
Diagnostic Evaluation
- The healthcare provider should follow the "Guidelines for the Initial Management of Frostbite".
- In addition to those guidelines, the healthcare provider should also obtain the following:
-
- a thorough history to identify indications and contraindications to t-PA use
- a thorough physical exam should also be performed to include:
-
- an extended neurologic examination
- a detailed description of frostbite, grade of frostbite injury and vascular exam of the involved digit(s) or extremity, and photos of the involved areas.
-
-
- Order baseline labs: CBC, BMP + Mg/Phos, PT/INR, PTT, CK, TEG, and type and screen
- Obtain baseline vital signs
- Obtain CT head if there is any history of associated trauma or if patient is altered and unable to provide a reliable history.
- Obtain Tech-99 bone scan, if possible, to document perfusion status of involved extremity.
Practice Recommendations for Management
- Based on history, physical exam findings, and additional imaging/lab results--the TRAUMA ATTENDING will make the decision to initiate t-PA for frostbite.
- if t-PA is indicated,
-
- Insert 2-3 large bore peripheral IVs (if not already present) with one line dedicated to t-PA administration.
- Ensure blood pressure is controlled prior to initiation of t-PA (SBP<180 and DBP<105)
- Insert/perform any invasive tubes, lines or procedures (if possible) prior to initiating t-PA. Otherwise, wait until t-PA infusion is complete.
- Order TDAP vaccination, if indicated, to be given prior to initiation of t-PA.
- Admit patient to the surgical ICU.
- Notify the ICU charge nurse and pharmacist that thrombolytic therapy is being ordered.
-
- The decision for systemic vs catheter directed intra-arterial thrombolytic therapy will be made at the discretion of the trauma attending.
-
- Catheter directed intra-arterial thrombolytic therapy
-
- Consult interventional radiology
- Orders and infusion rates of thrombolytics to be placed by interventional radiology
-
- Systemic t-PA
-
- Order using the "t-PA for frostbite" order set in EPIC (***currently awaiting build, so in meantime discuss with pharmacy for assistance in ordering***)
- t-PA dose:
-
- Bolus: 0.15 mg/kg IV bolus x 1
- Infusion: 0.15 mg/kg/hr over 6 hours (total dose not to exceed 100mg)
-
-
- Catheter directed intra-arterial thrombolytic therapy
-
- Patient care considerations during thrombolytic therapy:
-
- Patients must undergo q1hr vitals and neurologic checks during infusion of t-PA and or 24 hours following completion of infusion.
- Blood pressure should remain less than 180 mm Hg systolic and 105 mm Hg diastolic during t-PA infusion
- Neurovascular checks of the affected extremity should occur q1hr while t-PA is infusion followed by q4-24 hr checks after infusion is completed.
- CBC, PT/INR, and TEG should be performed q6 hrs while thrombolytics are infusing and for 24 hrs following completion of infusion.
- Limit invasive procedures or punctures while thrombolytics infusing.
- Patients should remain on bedrest while thrombolytics are infusion but should be encouraged to continue with active and functional range of motion while in bed to improve circulation.
-
- Once thrombolytic therapy is complete, the patient should be initiated on therapeutic anticoagulation with either Lovenox or Heparin infusion for 7 days. (If patient is to be discharged prior to 7 days, can consider DOAC for completion of therapy.)
- Additional frostbite wound care and management should follow those listed in the Guidelines for the Initial Management of Frostbite.
Follow-up Care
- Patients with frostbite injuries will follow-up in trauma surgery clinic for ongoing wound care as needed with referrals to orthopedic and plastic surgery clinic as indicated.
Outcome Measure and Guideline Adherence
- All frostbite patients receiving thrombolytic therapy will be reviewed yearly for adherance to guidelines, bleeding complications, status of wounds, need for amputations, and involvement of consulting services.
Related Policies:
- Guidelines for the Initial Management of Frostbite
Key Contributors
Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
Meghan Blais, PharmD | Clinical Pharmacist, Nebraska Medicine | Author
Last Updated
February, 2023
References
- Hickey S, et. al. Guidelines for thrombolytic therapy for frostbite. J Burn Care Res. 2020 Jan 30;41(1):176-183.
- Lacey AM, et al. An institutional protocol for the treatment of severe frostbite injury—A 6-year retrospective analysis. J Burn Care Res. 2021 Aug 4;42(4):817-820.
- Drinane J, Kotamarti VS, O'Connor C, et al. Thrombolytic salvage of threatened frostbitten extremeties and digits: A systematic review. J Burn Care Res. 2019; 40 (5): 541-549.
- Jones LM, Coffey RA, Natwa MP, et al. The use of intravenous tPA for the treatment of severe frostbite. Burns. 2017; 43(5): 1088-1096.