Trauma
Trauma guidelines
- 1. Trauma Service Overview
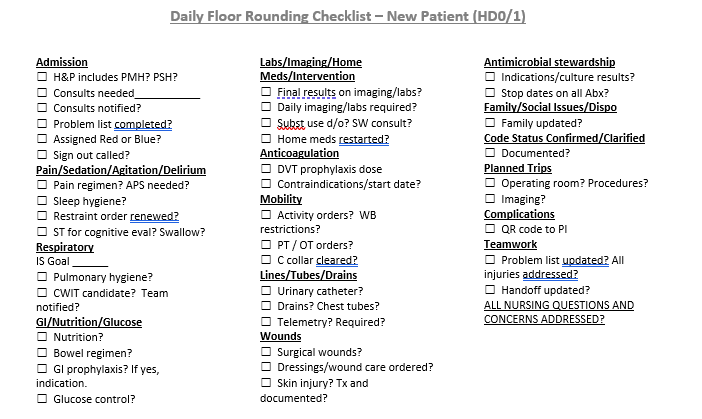
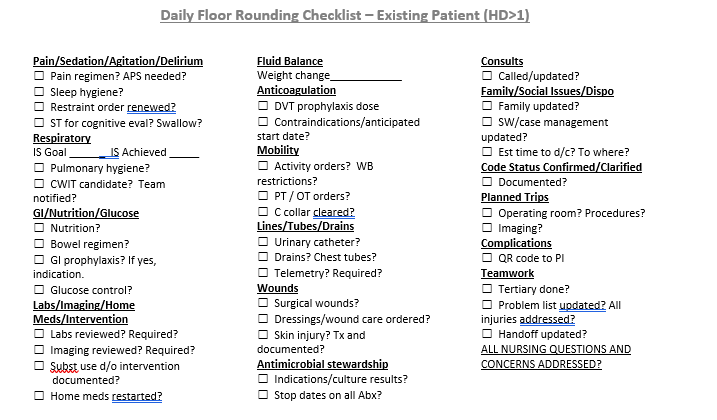
- Daily Floor Rounding Checklist for Trauma Patients
- Important Phone Numbers and Contact Information
- Isolated Orthopedic Transfers to Bellevue Medical Center Requiring Joint Replacement
- Reimplantation Triage and Transfer Pathway
- Trauma Patient Admission Criteria
- Trauma Team Activation (TTA) Criteria
- Trauma Tertiary Survey
- Trauma Quality Indicators
- 2. Initial Management and Resuscitation of the Trauma Patient
- Adult Traumatic Agonal Arrest and Resuscitation
- Drowning
- e-FAST for Trauma
- Early Femoral Arterial Line Placement for Trauma
- Hanging
- Management of the Pregnant Trauma Patient
- Massive Transfusion for Trauma Protocol
- REBOA Instructions
- Whole Blood Usage in Trauma
- Trauma Bay Adult Acute Agitation Management
- 3. Neurological Trauma
- Cervical Spine Evaluation and Management
- Intracranial Hypertension Management Algorithm
- Management of Traumatic Brain Injury
- Modified Brain Injury Guidelines (mBIG)
- Pharmaceutical Management of Post-TBI Neuropsychiatric Symptoms
- Initial Assessment and Management of Spine Injury
- Transverse and Spinous Process Fractures
- Care of Patients with Spinal Cord Injuries Practice Guideline
- 4. Head and Neck Trauma
- 5. Thoracic Trauma
- 6. Abdominal Trauma
- Blunt Abdominal Trauma
- Evaluation and Management of Blunt Splenic Injury
- Evaluation and Management of Hepatic Injury
- 7. Orthopedic Trauma
- Antibiotic Prophylaxis in Open Fractures
- Hand/Finger Reimplantation
- Isolated Hip Fracture Protocol
- Isolated Orthopedic Injury Admission Guidelines
- Orthopedic Trauma Discharge VTE Prophylaxis
- Management of Open Fractures
- Mangled Extremity Management
- 8. Vascular Trauma
- 9. Thermal Injury
- Care of Trauma Patient with Accidental Hypothermia Practice Guidelines
- Guidelines for the Initial Management of Frostbite
- Initial Management of Burns
- Thrombolytic Therapy for the Management of Severe Frostbite
- 10. Critical Care for Trauma
- Adult ICU Electrolyte Replacement
- Evaluation and Management of Atrial Fibrillation
- Nebraska Medicine Brain Death Criteria
- Percutaneous Tracheostomy Protocol
- 11. Geriatric Trauma
- Advanced Care Planning and Palliative Care Consultation in Acute Care Surgery
- Indications for Geriatric Consultation In Trauma Patients
- Isolated Hip Fracture Protocol
- 12. Pediatric Trauma
- Alcohol and Substance Misuse Screening, Brief Intervention and Referral for Treatment (SBIRT) Guidelines for Pediatric Trauma Patients at Nebraska Medicine
- Behavioral Consultation Team Contact Information
- Child Life in Trauma Resuscitations
- Discharging a Pediatric Trauma Patient Against Medical Advice (AMA)
- Evaluation and Management of Blunt Solid Organ Injuries in Pediatric Trauma Patients
- Evaluation and Management of Non-Accidental Trauma (NAT) in Children at Nebraska Medicine
- Guidelines for Imaging the Pediatric Trauma Patient
- Indications to Consult Pediatric Critical Care
- Indications to Consult Pediatric Co-Management Team for Pediatric Trauma Patients
- Managment of Open Pediatric Orthopedic Fractures
- Management of Pediatric Long Bone Fractures
- Management of Pediatric Pelvic Fractures
- Mental Health Screening and Intervention Guidelines for Pediatric Trauma Patients at Nebraska Medicine
- Non-Surgical Service Admissions of Pediatric Trauma Patients at Nebraska Medicine
- Pediatric Needle Cricothyroidotomy
- Pediatric Transport Contact Information
- Contact Information for Pediatric Trauma Patients
- Recommendations for Acute Pain Treatment and Procedural Pain and Sedation Management for Pediatric Patients
- Pediatric Presence at Pediatric Trauma Activations
- Transferring Pediatric Trauma Patients to Children's Nebraska Emergency Department
- 13. VTE Prophylaxis in Trauma
- 14. Care of the Trauma Patient
- Advanced Care Planning and Palliative Care Consultation in Acute Care Surgery
- Alcohol Withdrawal Pathway- PAWSS
- Assessing Capacity
- Evaluation and Management of Delirium
- Forensic Examiner Program Nebraska Medicine
- Summary – Law Enforcement Requests for Patient Information
- 15. Recovery of the Trauma Patient
- 17. Trauma Resident Resources
1. Trauma Service Overview
Orientation materials and additional information regarding work flow and requirements of the trauma service to help improve your experience and set expectations.
Daily Floor Rounding Checklist for Trauma Patients
Important Phone Numbers and Contact Information
Acute Care Surgery Attendings:
| Attending | Pager | Cell | Office |
| Zachary Bauman, DO | 402-888-1131 | 712-251-0895 | 402-559-4714 |
| Joseph Baus, MD | 402-888-1800 | 614-975-5466 | N/A |
| Christopher Barrett, MD | 402-888-6080 | 651-497-7846 | 402-559-3335 |
| Bennett Berning, MD | 402-888-5527 | 312-208-7465 | 402-559-4706 |
| Keely Buesing, MD | 402-888-0563 | 402-312-0984 | 402-559-8908 |
| Emily Cantrell, MD | 402-888-1201 | 336-775-8889 | 402-836-9142 |
| Mark Carlson, MD | 402-888-5161 | 402-650-4219 | 402-559-4581 |
| Samuel Cemaj, MD | 402-888-1203 | 402-305-5809 | 402-559-7166 |
| Charity Evans, MD | 402-888-0525 | 312-231-0897 | 402-559-2101 |
| Matthew Goede, MD | 402-888-3770 | 402-881-7345 | 402-559-8736 |
| Mark Hamill, MD | 402-888-5484 | 843-324-8252 | 402-559-3048 |
| Joshua Jaramillo, MD | 402-888-6059 | 720-363-1449 | N/A |
| Abigail Josef, MD | 402-888-5525 | 402-715-0029 | 402-559-4567 |
| Andrew Kamien, MD | 402-888-1453 | 716-228-0118 | 402-559-7399 |
| Kevin Kemp, MD | 402-888-2545 | 510-378-2215 | 402-559-8147 |
| Mike Matos, DO | 402-888-5655 | 304-482-2712 | 402-559-7051 |
| David Mercer, MD | 402-888-3758 | 402-889-3431 | 402-559-8272 |
| Olabisi Sheppard, MD | 402-888-5034 | 913-271-7241 | 402-559-2113 |
| John Tierney, MD | 402-888-6079 | 480-703-4556 | 402-559-1866 |
| William Terizian(Hillman), MD | 402-888-5526 | 703-505-1058 | 402-559-5970 |
| Jessica Veatch, MD | 402-888-6154 | 303-726-0736 | 402-559-8979 |
| Brett Waibel, MD | 402-888-0698 | 252-414-8586 | 402-559-6809 |
Acute Care Surgery APPs
| APPs 402-559-7901 / 402-559-9589 / 402-559-8142 | ||
| Tim Baack, NP | 402-888-5843 | 402-640-4084 |
| Jessica Bachmann, NP | 402-888-6252 | 402-660-4017 |
| Maggie Baumann, NP | 402-888-3839 | 402-813-4519 |
| Christina Boje, NP | 402-888-1871 | 402-578-7219 |
| Samantha Cunningham, NP | 402-888-5101 | 402-250-8711 |
| Sam Dellinger, PA | 402-888-6190 | 402-332-8474 |
| Esthefany Estrada, | 402-888-5155 | 308-325-8504 |
| Kelly Fenn, PA | 402-888-1440 | 563-299-5585 |
| Abby Hager, NP | 402-888-5582 | 402-680-9465 |
| Patrick Heavey, PA | 402-888-5675 | 402-699-9119 |
| Kristin Johnson, NP | 402-888-4584 | 308-530-5183 |
| Sophia Ketchmark, PA | 402-888-6189 | 402-926-6229 |
| Shannon Landry, PA | TBD | TBD |
| Ashley Lewis, NP | 402-888-4072 | 402-452-7660 |
| Sonia Malik, PA | 402-888-6008 | 703-994-2553 |
| Evan Meysenburg, NP | 402-888-6083 | 402-741-0970 |
| Erin Panowicz, NP | 402-888-5089 | 402-416-1274 |
| Whitney Petersen, NP | 402-888-0097 | 402-984-3744 |
| Meredith Reittinger, NP | 402-888-5865 | 336-549-2644 |
| Dom Samuel, NP | 402-888-1698 | 402-541-8998 |
| Amber Saltsgaver, NP | 402-888-5153 | 402-651-1250 |
| Megan Samland, NP | 402-888-5597 | 402-350-3564 |
| Emily Ulmer, PA | 402-888-6124 | 308-870-4515 |
| Theresa Vergara, NP | 402-888-2443 | 646-498-3829 |
| Makaela Waddell, NP | 402-888-0303 | 402-536-9460 |
| Becca Witt, PA | 402-888-5846 | 402-250-2134 |
| Cassey Younghans, NP | 402-888-6084 | 308-870-0791 |
Acute Care Surgery Administrators
| Administrative | |
| Jeannie Thomas | 402-559-9696 |
| Jessica Bruno | 402-559-8884 |
| Savannah Reyes | 402-559-5248 |
| Sue Cramer | 402-559-9225 |
| Karen Kroupa | 402-559-9960 |
| Copy Machine Code: | 10278 |
| Conf Room Code: | 51243 |
Acute Care Surgery Inpatient and Outpatient Team Contacts
| Inpatient Team Contacts | |||
| Molli Kies, Care Transition Nurse | 531-557-1135 | 402-559-6145 | 402-990-0874 |
| Angel Erwin, Care Transition Nurse | 531-557-0827 | 402-5522738 | 402-650-3038 |
| Ginny Rogers, Peds Care Transition Nurse | 531-5579166 | 402-552-2505 | 402-917-2593 |
| Barb Robertson, Nutritionist | 402-888-1848 | ||
| Dennis Brown, Care Transition nurse for EGS | 402-552-6588 | 402-981-9431 | 531-551-5031 |
| Social Worker | 402-888-1643 | 402-559-6145 | 531-557-3822 |
| Elizabeth Hawkins, Pharmacist | 531-557-7456 | 402-714-2787 | 402-552-3541 |
| Alli Gabriel, Pharmacist | 402-637-6454 | 402-552-3965 | 531-557-3983 |
| Ashley Farrens, Trauma Prog Manager | 402-612-7702 | 402-552-3997 | |
| Stacey Roode - PI Coordinator | 402-618-0375 | ||
| Liz McIntosh - PI Coordinator | 714-651-7733 | ||
| Kayla Petersen - PI Coordinator | 515-729-9289 | ||
| Lora Hofstetter - Peds PI Coordinator | 913-709-0923 | ||
| Brian Lake, 9N Manager | 402-552-3873 | ||
| Chad Himmelberg, SICU Manager | 402-552-7963 | ||
| Outpatient Team | |||
| Jenn Dickey, Case Manager | 402-888-3629 | 402-672-6081 | 402-559-6075 |
| Clinic Scheduling (# for pts) | 402-559-4075 | ||
| Clinic | 402-559-4737 | ||
| Clinic Workroom | 402-559-2028 | ||
| Trauma Clinic: Mon & Thurs @ 1-3pm | |||
| EGS Clinic: Wed @ 1-3pm | |||
| Elective EGS Clinic: Thurs @ 9am | |||
Service Pager and Consultant Contacts
| RED TRAUMA TEAM PAGER: | 402-888-1938 | GREEN SICU Pager: | 402-888-0282 | ||
| Blue APP TRAUMA TEAM PAGER: | 402-888-4774 | YELLOW CCS TEAM PAGER: | 402-888-3005 | ||
| EGS PAGER: | 402-888-0447 | General Surgery/Night Float Pager: | 402-888-0316 |
| Orthopedic Surgery Pager: | 402-888-0586 |
| Neurosurgery Pager: | 402-888-1866 |
| Pediatric Surgeons | Pager | Cell | Office |
| Angela Hanna, MD | N/A | 801-550-4482 | N/A |
| Abdalla Zarroug, MD | N/A | 507-271-5656 | N/A |
| ENCOMPASS TEAM | ||
| Ashley Raposo, Program Supervisor | 402-559-9154 | 402-980-1731 (cell) |
| Melissa Inzauro, Social Worker | N/A | 402-250-6336 (cell) |
| Allie Sothan, Social Worker | N/A | 531-375-8334 |
| Tia Manning, Mental Health Specialist | N/A | 402-250-9813 |
| Violence Intervention Specialists | ||
| Kam Wayne | N/A | 402-250-4324 (cell) |
| TiShara Wardlow | N/A | 402-830-7986 (cell) |
Departmental Contacts
| Department Contacts | |
| Handheld/Battery-Powered Bronch OR RT 402-559-1615 | 402-650-5748 |
| Anesthesia CD | 402-559-4078 / 402-552-3224 |
| OR | 402-889-0931 |
| OR Charge | 402-559-9900 / 402-552-3224 |
| Scheduling | 402-559-5257 |
| Preop | 402-559-9087 / 402-552-3288 (CCE) |
| PICU | 402-559-1420 |
| Anesthesia | 402-552-2090 |
| Micro | 402-559-5031 |
| Psychology | 402-559-1030 |
| Lab | 531-557-3980 |
| ICU Pharmacist | 531-557-7452 |
| SDCC Pharmacist | 402-559-7235 |
| Inpatient Pharmacy | 402-559-6502 |
| Trauma Bay | 402-559-4583 |
| ECHO | 402-559-6694 / 402-559-6637 |
| ER | 7-3600 |
| ED Charge Nurse | 402-559-1000 / 402-559-3216 |
| Radiology Dictation | 402-888-1898 |
| Radiology Resident | 402-559-8953/888-1314/888-1415(res) |
| IR | 402-559-8953 |
| Radiology Reading Rooms | |
| Body CT: | 402-559-1005 |
| Neuro: | 402-559-1008 |
| Bone: | 402-559-1006 |
| US: | 402-559-1023 |
| Nights: | 402-559-1233 |
Isolated Orthopedic Transfers to Bellevue Medical Center Requiring Joint Replacement
Purpose:
· To Identify which patients can appropriately be transferred to Bellevue Medical Center (BMC) who have sustained an isolated fractures requiring total or partial joint replacement
Background/definitions:
· Lack of OR availability at Nebraska Medicine main campus for partial or total joint replacement in trauma patients has put a strain on the system and delayed definitive surgical treatment for these patients.
Guideline Inclusion Criteria:
- Isolated traumatic fracture patients only needing partial or total joint replacement for their injury as opposed to ORIF of the hip fracture alone.
- Deemed appropriate for transfer to Bellevue Medical Center by the Trauma Service.
Guideline Exclusion Criteria:
- Poly-trauma patients with fractures requiring total or partial joint replacement.
- Deemed inappropriate for transfer to Bellevue Medical Center by the Trauma Team or Orthopedic Surgery Team.
Diagnostic Evaluation:
- Routine trauma lab work.
- Body region X-ray and/or CT scan
- Pan scan CT as indicated by mechanism or provider discretion
- Trauma Team consultation to make sure trauma work up is complete and no other injuries are present.
- Orthopedic Surgery consultation to make sure patient needs total or partial joint replacement (as opposed to non-operative management or routine ORIF of the fracture) and is appropriate for transfer to expidite surgical repair.
Practice Recommendations for Management:
- Patients transferred in from an outside institution will be directed to Nebraska Medicine ED (ER→ER). Trauma Team will do the initial trauma evaluation and work-up in the emergency department.
-
- If a fracture is identified along with other injuries, Orthopedic Surgery will be consulted as well as other consulting services as needed
-
- Patient will be admitted to Nebraska Medical Center (NMC) by the Trauma Service for further trauma management as deemed appropriate.
-
- If an isolated fracture is identified, Orthopedic Surgery will be consulted for their recommendations
- If a fracture is identified along with other injuries, Orthopedic Surgery will be consulted as well as other consulting services as needed
-
- If patient requires fixation via a partial or total joint replacement, is deemed appropriate for transfer to Bellevue Medical Center (BMC) by the Trauma Service, and has an accepting physician, the patient will then be transferred to BMC from the NMC ED for further isolated fracture management. BMC hospitalist is the accepting primary service for BMC transfer and ensures appropriate medical resources are in place for patient to be cared for at BMC. (Example- If patient has a hip fracture but is ESRD on dialysis, patient stays at NMC)
-
- Transfer to BMC will be arranged by the Orthopedic Surgery resident by contacting the PPU (aka BMC bed desk, 402-559-2337) and requesting transfer to the BMC hospitalist service.
- PPU informs Ortho resident of approximate inpatient BMC bed wait time.
- If there is an inpatient bed wait time at BMC, patient is sent to BMC Pre-Op as long as a same day BMC OR time can be assigned. If BMC OR time cannot be assigned the same day, patient is prioritized to BMC inpatient bed with all BMC ED admissions, the purpose of this prioritization is to transfer patient out of NMC ED expeditiously.
- No admission orders are placed to admit the patient to NMC. While the patient awaits transfer to BMC in the NMC ED, Trauma service continues to care for the patient.
-
- If Orthopedic Surgery resident determines patient would be more expeditiously cared for at main campus due to BMC bed wait
-
- Trauma service is contacted again and admits the patient.
- Trauma or Ortho provider contacts HM surgical co-mgmt service for pre-op evaluation and medical co-mgmt.
-
- If prolonged inpatient bed wait at both BMC and NMC campuses, On-Call Trauma attending and On-Call Orthopedic attending (& if needed BMC hospitalists for medical needs) determine whether it is best to transfer to BMC versus admit to NMC. PPU can help coordinate the conference call on the rare chance that all 3 physicians are needed to determine best location. Once location is determined, follow steps outlined above in A. to transfer to BMC or B. if admitting to NMC.
- The trauma tertiary survey will be completed by Orthopedic resident at BMC 24 hours after initial injury and documented as preferred by Trauma Service.
-
- If injuries discovered on tertiary appropriate consultations will be initiated by BMC Orthopedics team, including BMC service consults or remote NMC consultation.
-
- If the patient requires fracture fixation via routine ORIF, the patient will be admitted to the Trauma Service at Nebraska Medicine and follow the standard Nebraska Medicine Enhanced Recovery after Surgery (NERAS) pathway that has been established for isolated fracture patients.
-
- If the patient does not require fixation, the patient will be admitted to the Trauma Service at Nebraska Medicine and follow the standard NERAS pathway that has been established for isolated fracture patients.
-
- If patient primarily presents to Nebraska Medicine, patient will be activated based on criteria and both the Emergency Medicine and Trauma Team will respond appropriately and the trauma work-up will be conducted as per usual.
-
- If a fracture is identified along with other injuries, Orthopedic Surgery will be consulted as well as other consulting services as needed
-
- Patient will be admitted to Nebraska Medicine by the Trauma Service for further trauma management as deemed appropriate.
-
- If an isolated fracture is identified, Orthopedic Surgery will be consulted for their recommendations
-
- If patient requires fixation via a partial or total joint replacement, is deemed appropriate for transfer to BMC by the Trauma Service, and has an accepting physician, the patient will then be transferred to BMC from the ED for further isolated hip fracture management.
-
- Transfer to BMC will be arranged by the Orthopedic resident.
- The trauma tertiary survey will be completed by Orthopedic resident at BMC 24 hours after initial injury.
-
- If injuries discovered on tertiary appropriate consultations will be initiated by BMC admitting team, including BMC service consults or remote NMC consultation.
-
-
- If the patient requires fracture fixation via routine ORIF, the patient will be admitted to the Trauma Service at Nebraska Medicine and follow the standard NERAS pathway that has been established for isolated fracture patients.
- If the patient does not require fracture fixation, the patient will be admitted to the Trauma Service at Nebraska Medicine and follow the standard NERAS pathway that has been established for isolated fracture patients.
- If patient requires fixation via a partial or total joint replacement, is deemed appropriate for transfer to BMC by the Trauma Service, and has an accepting physician, the patient will then be transferred to BMC from the ED for further isolated hip fracture management.
-
- If a fracture is identified along with other injuries, Orthopedic Surgery will be consulted as well as other consulting services as needed
-
- If the patient does not meet activation criteria, Emergency Medicine will perform the initial evaluation.
-
- ***If a fracture is identified, Trauma should be consulted for additional trauma evaluation***
- If a fracture is identified along with other injuries, Orthopedic Surgery will be consulted as well as other consulting services as needed
-
- Patient will be admitted to Nebraska Medicine by the Trauma Service for further trauma management as deemed appropriate.
-
- If an isolated fracture is identified, Orthopedic Surgery will be consulted for their recommendations
-
- If patient requires fracture fixation via a partial or total joint replacement, is deemed appropriate for transfer to BMC by the Trauma Service, and has an accepting physician, the patient will then be transferred to BMC from the ED for further isolated fracture management.
-
- Transfer to BMC will be arranged by the Orthopedic resident.
- The trauma tertiary survey will be completed by Orthopedic resident at BMC 24 hours after initial injury.
-
- If injuries discovered on tertiary appropriate consultations will be initiated by BMC admitting team, including BMC service consults or remote NMC consultation.
-
-
- If the patient requires fracture fixation via routine ORIF, the patient will be admitted to the Trauma Service at Nebraska Medicine and follow the standard NERAS pathway that has been established for isolated fracture patients.
- If the patient does not require fracture fixation, the patient will be admitted to the Trauma Service at Nebraska Medicine and follow the standard NERAS pathway that has been established for isolated fracture patients.
- If patient requires fracture fixation via a partial or total joint replacement, is deemed appropriate for transfer to BMC by the Trauma Service, and has an accepting physician, the patient will then be transferred to BMC from the ED for further isolated fracture management.
-
-
Follow-up Care:
- If the patient is a poly-trauma patient, discharge and follow-up recommendations will be provided by all consulting services as needed and PT/OT.
-
- All attempts will be made to discharge patient to appropriate location based on patient/family preferences, PT/OT recommendations, and discretion of the Trauma Service
-
- If the patient is an isolated fracture patient admitted to Nebraska Medicine, discharge and follow-up recommendations will be provided by Orthopedic Surgery and PT/OT.
-
- All attempts will be made to discharge patient to appropriate location based on patient/family preferences, Orthopedic Surgery and PT/OT recommendations, and discretion of the Trauma Service.
-
- If the patient is an isolated fracture patient transferred to BMC, discharge and follow-up recommendations will be at the discretion of the teams managing the patient at BMC
Outcome Measures and Guideline Adherence:
- All patients transferred to BMC will be reviewed by the PI team at Nebraska Medicine.
-
- If the patient is admitted to a non-surgical service @ BMC, and if there is no identified opportunity for improvement, the following may be closed in primary review:
-
- ISS<9
-
- As part of secondary review, the Trauma Medical Director must review any that meet any of the following criteria:
-
- ISS>9
- Cases with an opportunity for improvement identified at primary review
-
- Patients that get transferred to BMC and for some reason transferred back to Nebraska Medicine, will undergo a tertiary review by the Trauma PI team and by all providers involved.
- Emerging trends will signal a need to review this pathway and modify as necessary
- If the patient is admitted to a non-surgical service @ BMC, and if there is no identified opportunity for improvement, the following may be closed in primary review:
-
Key Contributors:
· Zachary Bauman, DO, MHA
Last updated:
· 1/16/2023
References:
· American College of Surgeons 2022 Trauma Standards
Reimplantation Triage and Transfer Pathway
Reimplantation Triage and Transfer Pathway
Purpose: As an American College of Surgeons, verified level I trauma center, we are responsible for thorough assessment of the traumatically injured patient. This document is to aid in the triage and transfer process of patient requiring reimplantation services.
Background: Nebraska Medicine has multidisciplinary coverage (orthopedics, plastics, vascular, and urology) for patients requiring reimplantation services for traumatic injury (ie: severed limb, digit, or other body part).
Please reference the three identified injury types for appropriate treatment plan:
Mangled Extremity
Treatment of a mangled extremity is a collaborative effort amongst the Trauma service, Orthopedic surgery, and Vascular surgery. When a patient is determined to have a mangled extremity or extremity requiring re-implantation, all three services are involved to determine the overall best course of action for the patient given other injuries, hemodynamic status, and the ability to salvage the extremity. We utilize a mangled extremity score (see table below) to help with this management decision. Once all three service lines have agreed to re-implantation and/or attempting to salvage the extremity, the patient is taken to the OR where Orthopedic surgery and Vascular surgery will re-attach/re-construct bones and vessels as needed. Both services are available and on-call 24/7.

Upper Extremity/Hand Re-implantation
Nebraska Medicine has three experienced hand surgeons that are willing and skilled to perform hand/digit reimplantation when they are on call. Unfortunately, between the three of them, they cannot cover the hand service 24/7.
When these surgeons are unavailable, calls should be made to transfer to our regional implantation centers. See list of resources with contact information.
Our usual workflow for this is when we get a call from an outside hospital wanting to transfer a patient to us who potentially needs a hand/digit re-implantation, we will do a conference call with our on-call hand surgeon to see if this is something they are able to care for at our institution. If they are, we will have the patient transferred. While the patient is in route, our hand surgeon will get the OR organized and ready to go when the patient arrives. If the patient is unable to be cared for at our institution, we will help the outside hospital coordinate care to the regional hand re-implantation center by providing phones numbers and contact information. The same process applies if the patient comes to our institution directly from the field. Our on-call hand surgeon will assess to see if this patient needs to be transferred or not (not all our hand surgeons do re-implantations).
University Hospital – University of Missouri Health Care
1 Hospital Drive, Columbia, MO 65212
1-573-882-6985 - line 1
1-573-771-7860 – line 2
University of Iowa
200 Hawkins Drive, Iowa City, IA 52242
1-319-384-5000
Option – 2 (adult)
Option – 1 (trauma) or Option 2 (ED to ED)
Mayo Clinic
200 First Street, Rochester, MN 55905
1-507-255-2910
Denver Health Medical Center
777 Bannock Street, Denver, CO 80204
1-303-602-5000
Hand Trauma Center Network | About Us | ASSH
We do recognize that in some trauma scenarios it is life over limb. Any poly-trauma patient with potential life-threatening injuries will come to or remain at our Level 1 trauma center where all these issues will be addressed. If a patient is too unstable to be transferred due to other injuries, we will address these life-threatening injuries first. Furthermore, if an outside hospital has a poly-trauma patient with a potential re-implantation, those patients will be directed to our facility given the amount of travel time to nearest re-implantation center. In these situation, we do have the ability to call our hand surgeons that do re-implantations when they are not on-call to inquire for urgent consultation.
Penile Re-implantation
For penile re-implantation, Urology will be consulted for reimplantation or re-creation. They will reestablish a urethra for urinary drainage. Time of reimplantation is determined by Urology and if assistance is required by Plastic surgery, they too will be involved. Both services are available and on-call 24/7.
Trauma Patient Admission Criteria
Trauma patients can be complex with multiple injuries requiring various management strategies, interventions, and care. As a result, determining the appropriate level of care for admission can be challenging. The following represents a list of criteria/conditions that may help guide level of care decision making for the trauma patient.
ICU ADMISSION
- Grade IV or greater solid organ injury or Grade III injury with blush/active extravasation
- Any hemodynamic instability
- Base deficit >6
- Pelvic fractures requiring blood transfusion or IR angiogram/embolization
- Any spine fracture with neurologic deficit
- Mandible fracture with edema or hematoma
- Traumatic brain injury with GCS<13
- Patient >55 yrs of age, on anticoagulation with abnormal CT head
- Risk of airway compromise
- High risk rib fracture patient with FRC<1000mL
- Presence of pulmonary co-morbidities
- Blunt myocardial injury with new
-
- arrythmia
- hemodynamic instability
- cardiac failure
-
- Unstable spine injury
- Frontal contusions >2cm
- Solid organ/pelvis/abdominal injuries with evidence of active extravasation on CT scan
- need for q1hr vital signs/neuro-vascular checks/interventions/etc.
- Trauma attending discretion
SDCC Admission
- Grade II/III solid organ injury without blush/active extravasation on CT
- presence of multiple injuries
- Rib fractures with FRC between 1000mL--1500mL
- Any patient on pre-injury anticoagulation therapy with an injury not requiring ICU
- Major soft tissue trauma in patients on anticoagulation therapy
- Need for q2hr vital signs/neuro-vascular checks/interventions/etc.
- Presence of multiple co-morbidities
- Age > 70
- C-spine fractures exclusive of spinous and transverse process fractures (without neurologic injury)
- History of sleep apnea who needs narcotics
- New CPAP/BiPAP requirements
- Trauma attending discretion
FLOOR Admission
- all other trauma patients who do not meet criteria for ICU or SDCC admission
Trauma Team Activation (TTA) Criteria
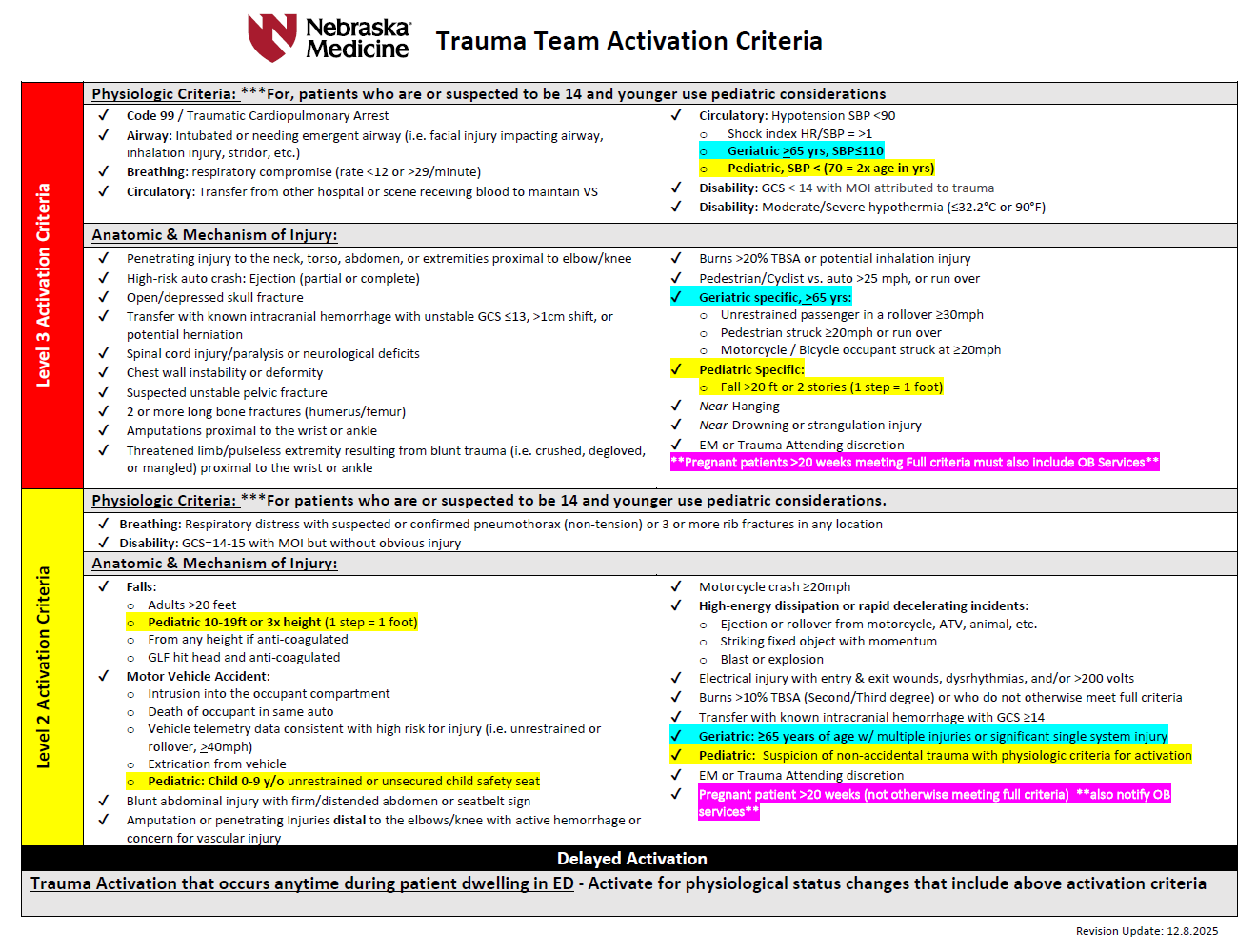
LEVEL 3 trauma team includes:
- Trauma attending
- Emergency medicine (EM) attending and resident
- PGY 4 or 5 surgical resident when available in house
- Junior surgical or EM residents on trauma service
- Trauma advanced practice providers (APP)
- Anesthesia resident (with immediate backup by anesthesia attending)
- Emergency department nurses and technicians
- Pharmacy
- Radiology technician
- Lab technician
- OR RN
- Blood bank (receives page to alert-do not respond in person)
- Spiritual care
- Respiratory therapy
LEVEL 2 trauma team includes:
- EM attending and resident
- General surgery resident(s)
- Trauma advanced practice provider(s) (APP)
- Emergency department nurses and technicians
- Pharmacy
- Radiology technician
- Lab technician
- OR RN (receives page to alert--do not respond in person)
- Spiritual care
- Respiratory therapy
- Trauma attending must respond if PGY4 or 5 surgical resident is not available and must evaluate the patient within 30 minutes of patient arrival.
- If the trauma attending is not in attendance, the EM attending has overall responsibility.
LEVEL 1 - Trauma CONSULTATION
These patients do not meet trauma activation criteria, but merit the expertise of trauma surgeon consultation and/or evaluation, i.e. isolated/single system injuries. A trauma service resident or APP will evaluate these patients within 30 minutes of consult being called and disposition of the patient will be determined within 60 minutes. If the patient requires admission, the trauma attending will evaluate these patients within 8 hours of consult regardless of patient location.
The EM physician or admitted physician will consult the trauma team for any patient requiring admission to the hospital for any traumatic injury that does not meet trauma activation criteria. This will include but is not limited to the following patients:
- Any patient with significant single system injury or multiple injuries
- Stable pelvic fractures (excludes isolated hip fractures)
- Stable chest injuries--rib fracture, sternal fracture, pneumothorax, seatbelt sign
- Minor brain injury (confirmed or suspected) with GCS 13-15
- Abdominal pain with significant mechanism of injury or seatbelt sign
- Spine fractures
- Pregnant patients who require admission to the OB floor for fetal monitoring
- Frostbite
- Any patient returning to the ED for care following treatment for a traumatic injury within the last 60 days
Patients who bypass the ED as a direct admit who are admitted for any injury meeting trauma criteria, will require a trauma consultation after notification of the admitting physician.
Trauma Tertiary Survey
A tertiary survey (exam) should be performed on all patients admitted to the trauma service approximately 24 hours following admission/initial evaluation.
The tertiary survey is a repeat head-to-toe examination of the trauma patient that is designed to identify injuries (usually more minor) that were not identified on the initial evaluation. Ideally the patient should be able to participate in the exam. EXCEPTION--intubated/sedated ICU patients should still receive a tertiary exam ~24 hrs following admission and also AGAIN, when his/her clinical status allows for them to participate in the exam.
The following is included in a trauma tertiary exam:
- complete physical exam
- review of any outstanding or follow-up imaging/labs/tests following initial examination/work-up
- review of previously diagnosed injuries and ensure injury is being addressed (i.e. consults called, treatment plans in progress, etc)
- review of patient's medical history
- ensure home medications have been reconciled and resumed as indicated
- review current status of patient (i.e. are existing lines/tubes still needed? VTE prophylaxis initiated? Activity restrictions? PT/OT/Speech consults? etc)
- update the patient's problems list in electronic medical records
How to complete a trauma tertiary survey at UNMC/Nebraska Medicine
Step 1: perform the tertiary survey
- thorough physical exam
- review all imaging, labs, etc.
- order additional imaging, labs, consults, etc. as indicated
- review injuries, treatment plans, etc and ensure plans are progressing appropriately
Step 2: document your tertiary survey
- New note
- Note type: Trauma Tertiary Survey

Step 3: complete tertiary survey template FULLY and ACCURATELY
- once trauma tertiary survey is selected as note type, a trauma tertiary template will autopopulate.
- fill in ALL values/categories based on your repeat assessment/examination at ~24 hours following admission
-
- this includes the Tertiary Trauma Quality Improvement (TQI) Section
-
- it appears in RED on the tertiary survey template
- this section includes certain pre-existing conditions that will be included in the trauma registry/TQIP database that help accurately capture the patient's status.
- to fill out this section, click on the TERTIARY TRUAMA QUALITY IMPROVEMENT (TQI) ADVANCED button at the top of the note template
- this will pull up a second screen/menu with a list of pre-existing conditions where conditions can be selected as appropriate (see pictures below)
-
- this includes the Tertiary Trauma Quality Improvement (TQI) Section
-


Trauma Quality Indicators
Background:
From the time a trauma patient is picked up by EMS on scene through the patient's initial assessment, hospital course, and discharge, our trauma program is carefully monitoring each patient and collecting data. Data collected includes demographic information, injury information, prehospital and hospital information, past medical history, traumatic injuries, in-hospital events and outcomes. Data is entered into our trauma registry and analyzed regularly through various performance improvement programs to ensure the trauma service is providing high quality care to each patient.
Much of the data collected for the registry is gathered by trauma registrars doing extensive chart reviews and depends greatly on complete and accurate documentation from our trauma providers. While we should be practicing complete and accurate documentation as part of being a good healthcare provider, it is also essential for our trauma program to able to monitor and analyze the care of our trauma patients to ensure that high quality care is provided and patient outcomes are optimized.
Pre-Existing Conditions
Several pre-existing conditions are captured in the trauma registry that help us risk stratify patients for observed and expected outcomes. These pre-existing conditions should be documented in the Trauma H&P and/or the Trauma Tertiary Survey as well as added to the patient's problem list in the electronic medical record.
The pre-existing conditions captured in the trauma registry are as follows:
- Advanced directive limiting care
-
- the patient has a written request to limit life-sustaining treatment that restricts the scope of care for the patient during this patient care event signed/dated by patient or designee prior to arrival.
-
- Alcohol use disorder
-
- can be actual diagnosis OR factors consistent with the diagnosis based on American Psychiatric Association, DSM 5 present prior to injury.
- only report on patients 15 yrs of age or older.
-
- Anticoagulant therapy
-
- administration of medication (including anticoagulants, antiplatelet agents, thrombin inhibitors, thrombolytic agents) that interferes with blood clotting. Exception: chronic aspirin.
-
- Attention deficit disorder/attention deficit hyperactivity disorder (ADD/ADHD)
-
- a disorder involving inattention, hyperactivity, or impulsivity requiring medication for treatment present prior to injury.
-
- Bipolar I/II disorder
-
- only report on patients 15 yrs of age or older.
-
- Bleeding disorder
-
- any condition that results in the blood not clotting properly (e.g. hemophilia, von Willenbrand disease, Factor V Leiden)
-
- Cerebral vascular accident (CVA)
-
- history prior to injury of stroke/CVA (embolic, ischemic, thrombotic, or hemorrhagic) with persistent residual motor, sensory or cognitive dysfunction (e.g., hemiplegia, hemiparesis, aphasia, sensory deficit, impaired memory).
-
- Chronic obstructive pulmonary disease (COPD)
-
- lung disease characterized by chronic obstruction of lung airflow that interferes with normal breathing and is not fully reversible. Includes more familiar terms such as "chronic bronchitis" and "emphysema".
- only report on patients 15 yrs of age or older.
-
- Chronic renal failure
-
- chronic renal failure prior to injury that requires periodic peritoneal dialysis, hemodialysis, hemofiltration, or hemodiafiltration.
-
- Cirrhosis
-
- replacement of normal liver tissue with non-living scar tissue related to other liver diseases often resulting in hepatic insufficiency/dysfunction and based on diagnostic imaging studies or laparotomy/laparoscopy. May also be referred to as end-stage liver disease.
-
- Congenital anomalies
-
- documentation of a pre-existing cardiac, pulmonary, body wall, CNS/Spinal, GI, renal, orthopedic, or metabolic anomaly.
- only report on patients less than 15 yrs of age
-
- Congestive heart failure (CHF)
-
- inability of the heart to pump a sufficient quantity of blood to meet the metabolic needs of the body or can do so only at an increased ventricular filling pressure.
- condition must be noted in medical record as CHF, congestive heart failure or pulmonary edema with onset of increasing symptoms within 30 days prior to injury.
-
- Current smoker
-
- includes patients who report smoking cigarettes every day or some days within the last 12 months.
- excludes patients who smoke cigars, pipes or smokeless tobacco.
-
- Currently receiving chemotherapy for cancer
-
- includes both oral and parenteral treatments
-
- Dementia
-
- includes, but not limited to, Alzheimer's, Lewy body dementia, frontotemporal dementia (Pick's disease), and vascular dementia.
-
- Diabetes mellitus
-
- diabetes mellitus that requires exogenous parenteral insulin or an oral hypoglycemic agent.
-
- Disseminated cancer
-
- cancer that has spread to one or more sites in addition to the primary site (i.e. metastatic or Stage IV cancer)
-
- Functionally dependent health status
-
- patients whom, prior to injury, and as a result of cognitive or physical limitations relating to a pre-existing medical condition, were partially or completely dependent upon equipment, devices or another person to complete some or all activities of daily living.
-
- Hypertension
-
- history of persistently elevated blood pressure requiring antihypertensive medication.
-
- Major depressive disorder
-
- only report on patients 15 yrs of age and older.
-
- Myocardial infarction (MI)
-
- history of MI in the 6 moths prior to injury
-
- Other mental/personality disorders
-
- a diagnosis of any of the following prior to injury: antisocial personality disorder, avoidant personality disorder, borderline personality disorder, dependent personality disorder, generalized anxiety disorder, histrionic personality disorder, narcissistic personality disorder, obsessive-compulsive disorder, obsessive-compulsive personality disorder, panic disorder, paranoid personality disorder, and schizotypal personality disorder.
- only report in patients 15 yrs of age and older
-
- Peripheral arterial disease (PAD)
-
- narrowing or blockage of vessels that carry blood from the heart to the legs. It is primarily caused by the buildup of fatty plaque in the arteries, which is called atherosclerosis. PAD can occur in any blood vessel but is most commonly found in the legs vs arms.
- only report in patients age 15 yrs of age or older.
-
- Post-traumatic stress disorder (PTSD)
-
- only report on patients 15 yrs of age or older.
-
- Pregnancy
-
- pregnancy confirmed by lab, ultrasound or other diagnostic tool OR diagnosis of pregnancy documented in the patient's medical record prior to arrival at your center.
-
- Prematurity
-
- babies born before 37 weeks of pregnancy are completed.
- only report in patients less than 15 years of age.
-
- Schizoaffective disorder
-
- only repot on patients 15 yrs of age or older
-
- Schizophrenia
-
- only report on patients 15 yr of age or older
-
- Steroid use
-
- regular administration of oral or parenteral corticosteroid medications within 30 days prior to injury for a chronic medical condition.
- excludes topical, inhaled, or rectally administered corticosteroids
-
- Substance use disorder
-
- diagnosis or symptoms/patient factors consistent with American Psychiatric Association, DSM 5 present prior to injury.
- only report on patients 15 yrs of age or older.
-
Hospital Events
Events reviewed through our performance improvement program include the following:
- Acute Kidney Injury (AKI)
- Acute Respiratory Distress Syndrome (ARDS)
- Alcohol withdrawal syndrome
- Cardiac arrest with CPR
- Catheter-associated urinary tract infection (CAUTI)
- Central line-associated blood stream infection (CLABSI)
- Deep surgical sight infection
- Deep vein thrombosis (DVT)
- Delirium
- Myocardial infarction (MI)
- Organ/space surgical site infection
- Osteomyelitis
- Pressure ulcer
- Pulmonary embolism (PE)
- Severe sepsis
- Stroke/CVA
- Superficial surgical site infection
- Unplanned admission to the ICU
- Unplanned intubation
- Unplanned visit to the operating room
- Ventilator-associated pneumonia (VAP)
If you are caring for a trauma patient that experiences one of the above stated hospital events, please notify our trauma program/performance improvement coordinators at traumapi@nebraskamed.com.
2. Initial Management and Resuscitation of the Trauma Patient
Educational materials and pathways regarding the initial approach to the evaluation, management and resuscitation of the injured patient.
Adult Traumatic Agonal Arrest and Resuscitation
Purpose
To outline the procedure for the treatment of the adult traumatic patient with a penetrating or blunt mechanism of injury who has no signs of life.
In patients without signs of life for >10 minutes in blunt trauma or >15 minutes in penetrating trauma, it is appropriate to terminate resuscitation efforts. Trauma surgeon discretion required as reported pre hospital CPR times may be inaccurate.
Definitions
- Blunt trauma –physical impact to the body by some force
- Penetrating trauma - occurs when a foreign object pierces the skin and enters the body creating a wound
- Adult trauma patient – any patient age fifteen (15) years or older who has sustained a blunt injury
- Agonal arrest - a severely injured patient in extremis, with no signs of life (absent pulse, absent respirations, absent pupil response, GCS 3)
Background
- Resuscitation of the adult trauma patient who is agonal or arrests as a result of a penetrating or blunt mechanism consist of a rapid assessment and treatment of the various measures of PEA (profound hypovolemia, airway compromise, tension pneumothorax and pericardial tamponade).
- Drowning, lightning strikes, medical causes of cardiac arrest, patients with profound hypothermia or if the patient’s age is 14 years and less are excluded from this guideline.
- The utilization of Advanced Cardiac Life Support (ACLS) and Basic Life Support (BLS) measures, including use of the Lucas device, in the setting of Advance Trauma Life Support (ATLS) resuscitation is of limited, if any, benefit in the setting of blunt traumatic patient arrest.
- Consider previous establishment of the patient’s DNR/DNI status, especially in patients who reside in a long term health care facility.
- Procedures (including airway assessment, chest tubes, etc.) take priority over chest compressions in the trauma patient in agonal or arrest states.
Resuscitation Algorithm
CONSIDER removal of Lucas device/mechanical chest compression device upon patient’s arrival in trauma bay.
- Airway:
-
- Non-intubated patient
-
- Obtain adequate airway (definitive ideal, however, if King, LMA or iGel is adequate, continue until pt stabilizes)
-
- Confirmation of Airway placement
-
- Visualization of ETT placement through vocal cords, if applicable
- Colorimetric CO2 detector (may not be reliable in arrest)
- Auscultation of bilateral breath sounds; absence of delivered breath sounds over epigastrium
- Appropriate O2 Saturation
-
- Intubated Patient
-
- Clear communication of assessment to trauma leader
- Confirmation of airway placement by ER faculty at head of bed
- Colorimetric CO2 detector (may not be reliable in arrest)
- Direct laryngoscopy may be considered in setting of any question of placement of ETT. Direct laryngoscopy in presence of ETT has a risk of dislodgement of appropriately placed ETT.
- Auscultation of bilateral breath sounds; absence of delivered breath sounds over epigastrium
- Appropriate O2 saturation
-
- Non-intubated patient
-
- Breathing:
-
- Bilateral Chest Tube Thoracostomy
- Resuscitative Thoracotomy (see Western Trauma algorithm below)
-
- Circulation:
-
- Rapid assessment of central (femoral) and peripheral pulses (radial, pedal)
- Clear communication of assessment to trauma leader
- Control of life-threatening external hemorrhage (hold pressure, tourniquet, etc)
- Obtain manual blood pressure (will not be present if no pulse)
- Confirmation of in-place intravenous (IV) access
- If no IV access:
-
- Establish IV, Intraosseous (IO) or central access
- Rapid, early delivery of Whole blood or Packed Red Blood Cells/plasma
-
- Consider initiation of Massive Blood Transfusion (MBT) protocol
- Maintain 1:1:1 ratios
-
-
- Attach cardiac leads/monitor
- Check Cardiac window on Focused Assessment with Sonography in Trauma (FAST)
-
- Assess for pericardial effusion
- Assess cardiac kinetic activity
-
-
- Disability:
-
- Glasgow Coma Scale (GCS) measurement
- Pupillary response
-
- Exposure/Environment
-
- Rapid and complete patient exposure
- Rapidly cover the exposed patient with warmed blankets (allow above assessment and procedures)
- Ensure underbody Bair Hugger functional (or provide warmth by another means)
-
During ABCDEs in a blunt agonal arrest, determine length of time of CPR and quickly assess patient for signs of life (detectable blood pressure, respiratory or motor effort, cardiac electrical activity, or pupillary activity)
- If CPR<10 min in blunt trauma or <15 minutes in penetrating trauma, AND pt has signs of life, proceed with Resuscitative Thoracotomy (see Western Trauma Association algorithm below).
- If CPR>10 min in blunt trauma or <15 minutes in penetrating trauma, AND NO signs of life, pt should be pronounced dead.
FIGURE 1. Western Trauma Resuscitative Thoracotomy algorithm
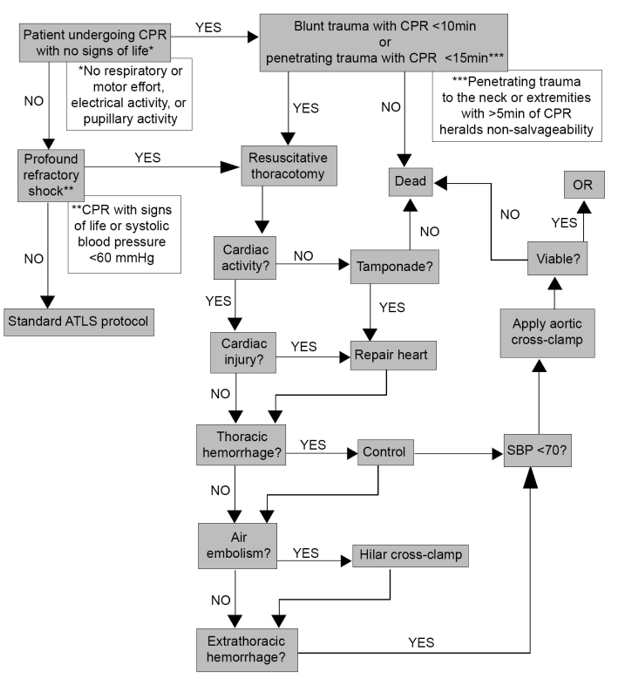
https://www.westerntrauma.org/wp-content/uploads/2020/08/Resuscitative-Thoracotomy_FINAL.svg
References
- Trauma patients receiving CPR: Predictors of Survival. J Trauma 2005 58:951-958. Pickens JJ, Copass MK, Bulger EM.
- Blunt Trauma Patients with Prehospital Pulseless Electrical Activity (PEA): Poor Ending Assured. J Trauma 2002 53:876-881. Martin SK, Shatney CH, Sherck JP, Ho C, Homan SJ, Neff J.
- Confusion Surrounding the Treatment of Traumatic Cardiac Arrest. Journal of the American College of Surgeons. Fulton RL, Voigt WJ, Hilakos AS.
- Role of External Cardiac Compression in Truncal Trauma. J Trauma 1982 Vol. 22 No.11. Mattox KL, Feliciano DV.
- Hemodynamic Effects of External Cardiac Massage in Trauma Shock. J Trauma 1989 Vol. 29 No. 10. Luna GK, Pavilin EG, Kirkman T, Copass MK, Rice CL.
- Guidelines for Withholding or Termination of Resuscitation In Prehospital Traumatic Cardiopulmonary Arrest: A Joint Position Paper From the National Association of EMS Physicians Standards and Clinical Practice Committee and the American College of Surgeons Committee on Trauma. Prehospital Emergency Care January / March 2003 Vol 7 / No. 1 141-146
- Withholding of Resuscitation for Adult Traumatic Cardiopulmonary Arrest: National Association of EMS Physicians and American College of Surgeons Committee on Trauma. Prehospital Emergency Care 2013 17:291
Authors
Charity Evans, MD | Division of Acute Care Surgery, Faculty | Principle Author
Last Updated
February, 2024
Drowning
Quick Guide:
Patients should be activated per their physiology and suspected injuries, which will most often be a full trauma given that the majority of suspected injuries include airway issues, level of consciousness/brain injury, and/or spinal cord injuries.
Trauma should be the admitting service to the appropriate level of care. If ICU admission is warranted, the appropriate critical care team should also be consulted (i.e Critical Care Surgery (CCS) for patients >12 yrs of age and Pediatric Critical Care Medicine (PCCM) for patients ≤12 yrs of age).
**Patients who have an event where they are submerged in water but return to baseline at the scene without concern for traumatic injuries do not meet these criteria and do not need a trauma activation for the submersion event. They may be safely evaluated in the ER and observed by medical admitting services (most often pediatrics).
Terms
Drowning is the process of experiencing respiratory impairment from submersion or immersion in liquid.
There are no medically accepted conditions known as “near-drowning,” “dry drowning,” “secondary drowning” or delayed drowning wherein a person was submerged in the water at some point, had no immediate breathing difficulty and later developed delayed onset of respiratory symptoms after a period of being asymptomatic [3].
Epidemiology
Drowning is the leading cause of death for children ages 1-4, and the second leading cause of unintentional injury-related death for children 5-14 (second only to MVCs) [1]. There is another peak among children and young adults aged 15-30, most often due to recreational swimming in natural bodies of water [2]. Other risk factors include alcohol consumption, hypothermia, traumatic injury leading to unconsciousness, neurodevelopmental conditions, and seizure disorders.
Pathophysiology of Injuries
Airway:
Panic results in disruption of normal breathing patterns, subsequent aspiration of fluid leads to laryngospasm and hypoxemia.
Pulmonary:
There is no difference between salt and fresh water- both result in hypoxemia and surfactant destruction, predisposing patients to noncardiogenic pulmonary edema and acute respiratory distress syndrome (ARDS).
Cardiac:
Arrhythmias may occur secondary to hypoxemia and hypothermia.
Neurologic:
Cerebral edema and elevated intracranial pressure develop as consequences of cerebral hypoxia, which is the major contributor to morbidity and mortality.
Later findings:
Hypoxia and hypoperfusion can trigger systemic inflammatory response, causing isolated cardiac, renal, or hepatic dysfunction, sepsis, or multiorgan failure. Rarely, patients with normal initial chest x-rays (similar to pulmonary contusions) may develop fulminant pulmonary edema within 12 hours, potentially reflecting delayed ARDS, neurogenic edema, or airway hyperreactivity.
Death from drowning primarily results from hypoxemia caused by water aspiration, which disrupts alveolar gas exchange, destroys surfactant, and produces noncardiogenic pulmonary edema. If rescue does not occur, hypoxia rapidly leads to loss of consciousness, apnea, and hypoxic cardiac arrest, usually presenting with bradycardia or pulseless electrical activity. Later deaths mainly arise from neurologic injury due to prolonged cerebral hypoxia [5].
History & Physical Examination
-focus the history on duration of submersion, length of extraction/rescue time, whether pulses were lost and/or if CPR was required. The likelihood of diving related injuries associated with the entry into the water are also important.
-additional questions regarding nonaccidental trauma can be added depending on the individual patient’s circumstances.
-obtain labs for toxicology, ethanol, metabolic derangements (most commonly lactic acidosis)
-Physical examination for signs of traumatic injuries as per standard ATLS protocol
Early Management/Stabilization
-Patients should be activated per their physiology and suspected injuries, which will most often be a full trauma
-Evaluate ABCs as always (primary and secondary survey per ATLS protocol)
-Immobilization of the spine is recommended for patients who sustained a dive or present with an unknown history
- Noninvasive positive pressure ventilation or endotracheal intubation may be required to maintain oxygen saturation
-Hypothermia should be addressed by passive rewarming and removal of cold wet clothes
-Noncardiogenic pulmonary edema and ARDS may develop over the next 12-24 hours [6]
-Glucocorticoids, diuretics, and empiric antibiotics are not recommended for routine use. Antibiotic therapy should be initiated only if clinical evidence of infection emerges [7]
Imaging
- Chest x-ray
- Non-contrast CT Head
- CT C-spine
- CTA neck and Head
- Can consider additional CTs (i.e. Trauma “pan scan”) if patient is unconscious, physical exams warrants, or history is concerning for additional injuries or if history is uncertain
Disposition
Trauma should be the admitting service to the appropriate level of care:
-Admit critically ill patients to the ICU with either CCS or PCCM consultation
-Admit patients without ICU needs to the Trauma service
-Patients with mild or no symptoms may be observed in the ER for 4-8 hours.
-ECMO may be considered as salvage therapy for refractory hypoxemia or severe hypothermia. These patients would be admitted to the CVICU under CCA for ECMO therapy, with transfer back to trauma floor or ICU as appropriate when weaned from ECMO.
Author and last update
Abby Josef, MD, February 2026
References
- Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS). Accessed 19 January 2026.
- Gianfrancesco, H; Sternard, BT. Drowning: Clinical Management. https://www.ncbi.nlm.nih.gov/books/NBK430833/ . Accessed 9 February 2026.
- Spack L, Gedeit R, Splaingard M, Havens PL. Failure of aggressive therapy to alter outcomes in pediatric near-drowning. Pediatric Emergency Care 1997;13(2):98–102.
- Suominen PK, Vähätalo R. Neurologic long term outcome after drowning in children. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2012;20(55):1–7.
- Suominen PK, Sutinen N, Valle S, Olkkola KT, Lönnqvist T. Neurocognitive long term follow-up study on drowned children. Resuscitation 2014;85(8):1059–106.
- Szpilman D, Morgan PJ. Management for the Drowning Patient
- Berger S, Siekmeyer M, Petzold-Quinque S, Kiess W, Merkenschlager A. Drowning and Nonfatal Drowning in Children and Adolescents: A Subsequent Retrospective Data Analysis.
e-FAST for Trauma
Purpose
To standardize the application of e-FAST in the seriously injured patient, the technique employed, and the quality of standards by which they are retrospectively evaluated.
Background
e-FAST is a valuable diagnostic tool in the evaluation of traumatically injured patients that is able to detect life threatening inra-abdominal hemorrhage, pericardial effusion and hemo/pneumothoraces. An e-FAST exam is non-invasive, does not expose the patient to radiation, can rapidly be performed concurrently with other resuscitative measures, and is repeatable. e-FAST has a sensitivity between 73-88%, a specificity between 98-100%, and an accuracy of 96-98%.
Indications for an e-FAST Exam at UNMC/Nebraska Medicine
- Hemodynamically unstable patients as defined by a systolic blood pressure <90 mmHg for adults and <70mmHg + (2x age in years) for pediatric patients.
- At the discretion of the Emergency Medicine or Trauma attending.
Patients in whom e-FAST should strongly be considered
- Pregnant patients
In these special patient populations, if an e-FAST is performed:
- a repeat abdominal ultrasound should be performed 4 hours after the initial e-FAST or sooner if the patient becomes hypotensive.
- a repeat hemoglobin at the time of repeat ultrasound
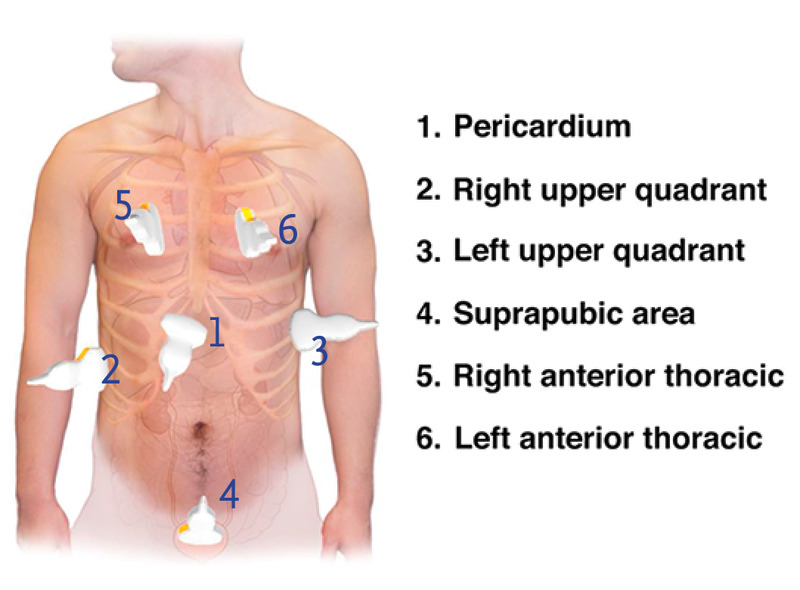
Six views of a complete e-FAST Exam
- pericardial or subxiphoid view
- Right upper quadrant: Lung base and hepatorenal recess
- Left upper quadrant: Lung base and splenorenal recess
- Pelvic: suprapubic view of bladder/Pouch of Douglass
- Right anterior thorax
- left anterior thorax
Ordering and Documentation of e-FAST exams
For all patients undergoing an e-FAST exam for trauma:
- Place an order in the electronic medical record (EPIC) for an e-FAST exam (POC ED US E-FAST, aka FAST)
- A procedure note will be documented by the provider performing the exam, including indication and interpretation of images.
-
- the performance of an e-FAST, the indication for exam and results of the exam should also be documented in the trauma H&P.
-
- Images will be saved with the patient's MRN.
Internal review of e-FAST exams:
The patients in whom e-FAST exams are indicated will be queried and the percentage of those receiving e-FAST exams reported. The documentation, image views and quality, and interpretation of images will be reviewed. Findings will be compared with CT or operative findings. Data will be presented at the monthly Performance Improvement Patient Safety (PIPS) meeting.
References
- AIUM Practice Parameter for the Performance of the Focused Assessment with Sonography for Trauma (FAST) Examination. American Institute of Ultrasound Medicine in collaboration with the American College of Emergency Physicians. http://www.aium.org/resources/guidelines/fast.pdf.
- Branney SW, Moore EE, Cantrill SV, et al. Ultrasound based key clinical pathway reduces the use of hospital resources for the evaluation of blunt abdominal trauma. J Trauma 42:1086-1090, 1997.
- Healey MA, Simons RK, WInchell RJ, et al. A prospective evaluation of abdominal ultrasound in blunt trauma: Is it useful? J Trauma 40:875-883, 1996.
- Glaser K, Tschmelitsch J, Klingler P, et al. Ultrasonography in the management of blunt and thoracic trauma. Arch Surg 129:743-747, 1994.
- Liu M, Lee CH, P'eng FK. Prospective comparison of diagnostic peritoneal lavage, computed tomographic scanning and ultrasonography for the diagnosis of blunt abdominal trauma. J Trauma. 35:267-270 1993.
- Boulanger BR, McLellan BA, Brenneman FD, et al. Emergent abdominal sonography as a screening test in a new diagnostic algorithm for blunt trauma. J Trauma. 40;867-874, 1996.
- Boulanger BR, Brenneman FD, McLellan BA, et al. A prospective study of emergent abdominal sonography after blunt trauma. J Trauma. 39;325-330, 1995.
- Ma OJ, Kefer MP, Mateer JR, et al. Evaluation of hemoperitoneum using single vs multiple ultrasonographic examination. Acad Emerg Med. 2:581-586, 1995.
- Rozycki GS, Oshsner MG, Jaffin JH, et al. Prospective evaluation of surgeons' use of ultrasound in the evaluation of trauma patients. J Trauma. 34:516-527, 1993.
- Smith SR, Kern SJ, Fry WR, et al: Institutional learning curve of surgeon-performed trauma ultrasound. Arch Surg. 133:530-536, 1998.
- McKenney MG, Martin L, Lentz K, et al. 1000 consecutive ultrasounds for blunt abdominal trauma. J Trauma. 40:607-612, 1996.
- Kem SJ, Smith RS, Fry WR, et. al. Sonographic examination of abdominal trauma by senior surgical residents. Am Surg. 63:669-674, 1997.
- Rozycki GS, Ochsner MG, Schmidt JA, et al. A prospective study of surgeon-performed ultrasound as the primary adjuvant modality for injured patient assessment. J Trauma. 39;492-500, 1995.
- Ong A, McKenney MG, McKenney KA, et al. Predicting the need for laparotomy in pediatric trauma patietns on the basis of ultrasound score. J Trauma. 2003;54:503-508.
- Soudack M, Epelman M, Maor R, et al. Experience with focused abdominal sonography for trauma (FAST) in 313 pediatric patietns. J Clin Ultrasound. 2004;32(2):53-61.
- McPartland SJ, Jackson C-CA, Gilchrist BF. "Pediatric Blunt Trauma". Trauma, Critical Care and Surgical Emergencies. Eds. Rabinovici R, Frankel HL, Kirton O. London:Informa, 2010203-226. Print.
UNMC/NM Policy last updated
August, 2019
May, 2025
Early Femoral Arterial Line Placement for Trauma
Purpose
Identify patients who would benefit from early femoral arterial access and describe the process facilitating early femoral arterial access.
Background
Hemorrhage is the leading cause of preventable death in trauma patients. Decision making regarding optimal therapy for the patient experiencing life threatening hemorrhage can be challenging. Early femoral arterial access provides additional information by way of continuous blood pressure monitoring. In addition to improved monitoring, common femoral artery (CFA) access is an essential and rate-limiting step in performing hemorrhage control interventions such as resuscitative endovascular balloon occlusion of the aorta (REBOA) or angioembolization. As the hemorrhaging patient progresses further into hemorrhagic shock, CFA access becomes more challenging to obtain.
Inclusion Criteria
- Trauma patients with blunt or penetrating mechanism
- Concern for life threatening hemorrhage as evidenced by any of the following
-
- Shock index greater than 1
- Assessment of Blood Consumption (ABC) score greater than 2
- Revised Assessment of Bleeding and Transfusion (RABT) score greater than 2
- Systolic blood pressure less than 90 mmHg
- Transient or non-responder to initial resuscitation
-
- Difficulty obtaining non-invasive blood pressure management
- REBOA deployment is considered as an adjunct for hemorrhage control
Exclusion Criteria
- Concern for pericardial tamponade
- Concern for supradiaphragmatic hemorrhage
- Patient not a candidate for REBOA
Trauma Bay Workflow
- For full trauma activations, ensure that a functioning ultrasound machine is present in the trauma bay, is powered up and otherwise ready to be used
- Ensure either femoral arterial line kit or 5 French micropuncture kit is immediately available
- Ensure that sterile probe cover, Chloraprep and ultrasound gel are immediately available
- Communicate with nursing staff that early CFA access may be pursued giving them time to set up pressure transducer
- Using the criteria above at the discretion of the trauma surgeon or their surrogate, decision to pursue early CFA access is made
- The groin is prepped and draped sterilely
- The linear array ultrasound probe is draped in the usual fashion
- Using real time ultrasound guidance, the CFA is accessed and the catheter placed in the usual fashion. A detailed description of this technique is beyond the scope of this document. Ultrasound guidance should be standard of care, however access by landmarks can be considered on a case by case basis
- Once the catheter has been inserted into the CFA, it is connected to the pressure transducer set up
- The catheter is secured and a sterile dressing is applied
- Depending on the patient’s hemodynamics, their response to resuscitation and their injury pattern, this femoral catheter can remain for hemodynamic monitoring or can be upsized to a 7 French sheath to facilitate placement of REBOA
Key Contributors
Kevin Kemp, MD
Last Updated
April, 2023
References
- Manning JE, Moore EE, Morrison JJ, Lyon RF, DuBose JJ, Ross JD. Femoral vascular access for endovascular resuscitation. J Trauma Acute Care Surg. 2021 Oct 1;91(4):e104-e113. doi: 10.1097/TA.0000000000003339. PMID: 34238862.
- Romagnoli A, Teeter W, Pasley J, Hu P, Hoehn M, Stein D, Scalea T, Brenner M. Time to aortic occlusion: It's all about access. J Trauma Acute Care Surg. 2017 Dec;83(6):1161-1164. doi: 10.1097/TA.0000000000001665. PMID: 29190256.
- Hadley, Jamie B. MD; Coleman, Julia R. MD, MPH; Moore, Ernest E. MD; Lawless, Ryan MD; Burlew, Clay C. MD; Platnick, Barry MD; Pieracci, Fredric M. MD; Hoehn, Melanie R. MD; Coleman, Jamie J. MD; Campion, Eric M. MD; Cohen, Mitchell J. MD; Cralley, Alexis MD; Eitel, Andrew P. MD; Bartley, Matthew MD, MS; Vigneshwar, Navin MD, MPH; Sauaia, Angela MD, PhD; Fox, Charles J. MD. Strategies for successful implementation of resuscitative endovascular balloon occlusion of the aorta in an urban Level I trauma center. Journal of Trauma and Acute Care Surgery 91(2):p 295-301, August 2021. | DOI: 10.1097/TA.0000000000003198
- Romagnoli, A and Brenner, M. “Principles of REBOA.” Chapter 6, p 81-96. Horer, T et al (eds.). Endovascular Resuscitation and Trauma Management, Hot Topics in Trauma and Acute Care Surgery. Springer Nature 2020.
Hanging
Quick Guide:
Patients should be activated per their physiology and suspected injuries, which will most often be a full trauma given that the majority of suspected injuries include airway issues, level of consciousness/brain injury, and/or spinal cord injuries.
Trauma should be the admitting service to the appropriate level of care. If ICU admission is warranted, the appropriate critical care team should also be consulted (i.e Critical Care Surgery (CCS) for patients >12 yrs of age and Pediatric Critical Care Medicine (PCCM) for patients ≤12 yrs of age).
Terms/Classification [1]
-“Near-hanging” is a term for patients who have survived an attempted hanging (or at least long enough to reach the hospital).
-“Complete hanging” defines when a patient’s legs are fully suspended off the ground and the patient's bodyweight is fully suspended by the neck.
-“Incomplete hanging” defines when some part of the patient’s body is still on the ground and the body's full weight is not suspended off the ground.
-“Judicial hanging” classically refers to victims who fell at least the height of their body.
Epidemiology
-Hanging is the 2nd most common form of successful suicide in the US after firearms. In many areas without access to firearms, hanging is the most common form of successful suicide (England, Australia, New Zealand, also more relevant- in the US jail system)
-Highly lethal (around 70%) but also high survival in those who are rescued and reach the hospital alive (80-90% survival)
-Risk Factors: male, aged 15-44 years, history of drug or alcohol abuse, history of psychiatric illness
Pathophysiology of Injuries
Spine/Spinal Cord:
-In a judicial hanging, there will almost always be cervical spine injury. The head hyperextends, leading to fracture of the upper cervical spine ("hangman's fracture” of C2) and transection of the spinal cord.
-Cervical injuries in non-judicial hangings are rare. [2] One retrospective case review of near-hangings over a 10-year period found the incidence of cervical spine fracture to be as low as 5%. [3]
Vascular:
The major pathologic mechanism of death in hanging/strangulation is neck vessel occlusion, not airway obstruction. [1,4] Death ultimately results from cerebral hypoxia and global ischemia. The most implicated cause of death is venous obstruction. Obstruction of venous outflow from the brain leads to stagnant hypoxia and loss of consciousness in as little as 15 seconds. The risk of damage to the major arterial blood flow to the brain (such as carotid artery dissection) is rare, but should evaluated in patients. [4]
Cardiac:
Carotid body reflex-mediated cardiac dysrhythmias are reported and may account for a minor mechanism of death.
Pulmonary:
-Airway compromise plays less of a role in the immediate death of complete hanging/strangulation. However, it is a major cause of delayed mortality in near-hanging victims. [1,4] Airway edema can occur from mechanical trauma to the airway, which can make intubation difficult. Tracheal stenosis can develop later in the hospital course. The hyoid bone can fracture, and injuries to the cricoid or thyroid cartilage can also occur. [5]
-Significant pulmonary edema occurs through two mechanisms:
1) Neurogenic: centrally mediated, massive sympathetic discharge; often in association with serious brain injury.
2) Post-obstructive: strangulation causes marked negative intrapleural pressure, generated by forceful inspiratory effort against extra-thoracic obstruction; when the obstruction is removed, there is a rapid onset pulmonary edema leading to ARDS.
-Aspiration pneumonitis/pneumonia can cause later sequela of near-hanging injury.
Physical Examination
-"Ligature marks" or abrasions, lacerations, contusions, bruising, edema of the neck
-Tardieu spots (petechiae/ecchymoses) of skin or eyes
-Severe pain on gentle palpation of the larynx (laryngeal fracture)
-Respiratory signs: cough, stridor, dysphonia/muffled voice, aphonia
-Varying levels of respiratory distress
-Hypoxemia
-Mental status changes
Early Management/Stabilization
-Patients should be activated per their physiology and suspected injuries, which will most often be a full trauma
-Evaluate ABCs as always (primary and secondary survey per ATLS protocol)
-Routine immobilization of the cervical spine is recommended
-Patients who have symptoms such as odynophagia, hoarseness, neurologic changes, or dyspnea may require sudden emergent intubation
-Judicious and cautious fluid resuscitation - avoid large fluid volume resuscitation and consider early pressors, as fluids increase the risk/severity of ARDS and cerebral edema
-Monitor for cardiac arrhythmias
-Comatose patients should be assumed to have cerebral edema with elevated ICP and medically managed as such
-Non-intubated patients with pulmonary edema may benefit from noninvasive positive end-expiratory pressure ventilation
-Patients with symptoms of laryngeal or tracheal injury (e.g. dyspnea, dysphonia, aphonia, or odynophagia), should undergo laryngobronchoscopy with ENT [4,6]
Imaging
- Chest x-ray
- Non-contrast CT Head
- CT C-spine
- CTA neck and Head
- Can consider additional CTs (i.e. Trauma “pan scan”) if patient is unconscious, physical exams warrants, or history is concerning for additional injuries or if history is uncertain
Disposition
Trauma should be the admitting service to the appropriate level of care:
-Admit critically ill patients to the ICU with either CCS or PCCM consultation
-Admit patients without ICU needs to the Trauma service
-Even if the initial presentation is clinically benign, all near-hanging victims should be observed for 24 hours, given the potential risk of delayed neurologic, airway, and pulmonary complications [7, 8]
-Psychiatry consult on all suspected intentional cases
-Emphasize strict return precautions as well as education about possible delayed respiratory and neurologic dysfunction when discharging patients
Author and last update
Abby Josef, MD, February 2026
References
1. Walls RM, Hockberger RS, Gausche-Hill M. Rosen's emergency medicine: concepts and clinical practice. Ninth edition. ed. Philadelphia, PA: Elsevier; 2018.
2. Aufderheide TP, Aprahamian C, Mateer JR, et al. Emergency airway management in hanging victims. Ann Emerg Med. 1994;24(5):879-884.
3. Salim A, Martin M, Sangthong B, Brown C, Rhee P, Demetriades D. Near-hanging injuries: a 10-year experience. Injury. 2006;37(5):435-439.
4. Tintinalli JE, Stapczynski JS, Ma OJ, Yealy DM, Meckler GD, Cline DM. Tintinalli's emergency medicine: a comprehensive study guide. 9th. ed. New York: McGraw-Hill Education; 2019.
5. Tugaleva E, Gorassini DR, Shkrum MJ. Retrospective Analysis of Hanging Deaths in Ontario. J Forensic Sci. 2016;61(6):1498-1507.
6. Hackett AM, Kitsko DJ. Evaluation and management of pediatric near-hanging injury. Int J Pediatr Otorhinolaryngol. 2013;77(11):1899-1901.
7. McHugh TP, Stout M. Near-hanging injury. Ann Emerg Med. 1983;12(12):774-776.
8. Balaji Kannamani, Neeru Sahni, Anjishnujit Bandyopadhyay, Vikas Saini, Laxmi Narayana Yaddanapudi. Insights into pathophysiology, management, and outcomes of near-hanging patients: A narrative review. J Anaesthesiol Clin Pharmacol. 2024 Oct-Dec;40(4):582-587.
Management of the Pregnant Trauma Patient
Purpose:
Pregnancy alters baseline physiology and anatomy. These changes can influence the evaluation of a traumatically injured pregnant patient. The signs and symptoms of injury can be confusing. The pregnant patient has abnormal baseline laboratory values. There are special considerations in the approach and response to resuscitation. While there are two patients – mother and fetus, the initial treatment priorities are the same, focusing on the optimal treatment of the mother. To provide safe care to the pregnant trauma patient, a collaborative effort between Emergency Medicine, the Trauma Service and the Department of Maternal Fetal Medicine should occur.
Policy Statement:
This guideline is a supplement to and is to be used in conjunction with the policy Trauma Team Activations (TTA01).
Non-trauma activated/minor trauma patients > 20 weeks seen in the Emergency Department (ED) by Emergency Medicine should have an OB consult within 1 hour of presentation to the ED even for minor trauma.
All pregnant trauma patients will be evaluated in an organized fashion whether they be evaluated in the ED, on the floor, or in Labor and Delivery. Obstetrics, including Maternal Fetal Medicine, is available to consult on any pregnant patient <20 weeks at any time to discuss medication risks or risk of surgery in pregnancy. Additionally, if a pregnant trauma patient at any gestational age cannot be bedded on the trauma floor, contact Labor and Delivery.

References
-
1. American College of Surgeons Committee on Trauma. (2025). ATLS, Advanced Trauma Life Support: Student Course Manual. 11th ed. American College of Surgeons.
Author(s)
- Acute Care Surgery/Trauma Leadership
- Emergency Medicine Leadership
- Maternal Fetal Medicine Division Leadership
Last Updated
February, 2026
Massive Transfusion for Trauma Protocol
Purpose
Hemorrhage is the leading cause of early death following traumatic injury. Protocol-driven transfusion strategies that approach a 1:1:1 ratio in patients who require massive transfusion improve patient survival, reduce hospital and ICU length of stay, decrease ventilator days, and ultimately reduce patient care costs.
These guidelines are meant to standardize the approach to resuscitation of an injured patient in hemorrhagic shock utilizing massive transfusion.
This guideline is a supplement to and is to be used in conjunction with Nebraska Medicine’s organizational policies “Massive Transfusion/Severe Coagulopathy” (TX-36) and “Guidelines for Management in Patients Receiving Anticoagulation” (MP 11).
Background/Definitions
Massive transfusion may be defined as transfusion in response to massive and uncontrolled hemorrhage resulting in any of the following:
- Replacement of half of a patient’s total blood volume in a 4 hour period
- Replacement of a patient’s total blood volume within 24 hours
- Transfusion of >10 units of PRBCs in 24 hours
- Specific pediatric parameters are more challenging to define and include transfusion of >40mL/kg PRBCs in a short period of time.
Hemorrhage is the most common cause of death within the first hour of arrival to a trauma center. Blood product resuscitation, specifically massive transfusions, are often unplanned and require the processing and delivery of large amounts of blood products rapidly for a sustained period of time, significant preplanning and coordination between the blood bank, resuscitating unit (i.e. emergency department, operating room, intensive care unit) and pharmacy is required. The initiation of a massive transfusion protocol (MTP) outlines a standard process for the safe, rapid preparation and delivery of blood products and coagulation factors for the pediatric patient experiencing massive hemorrhage. Additionally, implementation of a standardized guideline may prevent the anticipated complications of massive transfusion including thrombocytopenia, coagulopathies, electrolyte and acid/base disturbances, hypothermia and transfusion reactions as well as utilize valuable blood components in a resourceful manner.
At Nebraska Medicine, the massive transfusion protocol is divided into 3 categories based on the patient’s weight with each pack within that category containing the following blood product components.
|
MTP type |
Packed Red Blood Cells (PRBC) |
Thawed Plasma (FFP) |
Apheresis Platelets |
Pre-pooled cryoprecipitate (cryo) |
|
Adult (> 40 kg) |
6 (O pos) |
6 (A) |
1 |
On pack #3 and every pack thereafter |
|
Pediatric (10-40kg) |
6 (O pos) |
6 (a) |
1 |
On pack #3 and every pack thereafter |
|
Neonate/Infant (<10 kg) |
1 (O neg, irradiated) |
|
1 (irradiated) |
|
Guideline Inclusion Criteria
Injured patients with concern for massive or uncontrolled hemorrhage.
Guideline Exclusion Criteria
This is a guideline only. Individual circumstances need to be considered, as there may be times when it is appropriate to deviate from this guideline.
Diagnostic Evaluation
Injured patients should be assessed per ATLS guidelines paying close attention to circulation. Presence or history of hemodynamic instability, poor perfusion and external blood loss are red flags for hemorrhage. Signs of hemodynamic instability or poor perfusion may include altered mental status, pallor, delayed capillary refill, tachycardia, and hypotension. Hypotension is often a late sign of hypovolemic/hemorrhagic shock.
Practice Recommendations for Management
Initiation and Activation
- The decision to activate MTP is a clinical decision made by the trauma or emergency medicine attending physician and should be strongly considered with one or more of the following criteria:
-
- Persistent hemodynamic instability
- Shock Index >1 (SI = HR/SBP)
- Active bleeding requiring operation or angioembolization
- Blood transfusion in the Trauma Bay
- Adult patients (>40 kg)--Anticipated of transfusion of >10 units PRBC in 24 hrs or >4 units in 1 hr.
- Pediatric patients (≤40kg) -- Anticipated or actual use of ≥ 40 mL/kg PRBCs in 2 hours or replacement of total blood volume (approximately ≥ 80 mL/kg) in 24 hrs
- Assessment of blood consumption (ABC) score is ≥2 (adults only):
-
- Penetrating mechanism of injury (1pt)
- Systolic blood pressure less than or equal to 90 mm Hg (1pt)
- Heart rate greater than or equal to 120 (1pt)
- Positive FAST exam (1pt)
-
-
- Initiation of MTP should not be delayed for lab results.
-
- Universally compatible RBC (O Rh-negative) and thawed plasma may be given.
-
- Emergency release blood should be utilized as indicated until MTP blood products are available.
-
- Whole blood is preferred in the initial resuscitation of hemorrhagic shock in patients age 6 and older.
-
- 4 units of whole blood (O positive) are available for trauma resuscitations in the emergency department (ED) and can be found in the ED trauma bay kiosk refrigerator pending inventory availability.
- Use of whole blood in pediatric patients age 6-12 years of age should be limited to 1 unit due to potential risk of hemolysis.
-
- Emergency release blood is located in the following locations:
-
- Emergency Department (ED) trauma bay kiosk refrigerators (2 kiosks located in T1 and T4) each containing 2 units O positive whole blood, 2 units O negative PRBC, 6 units O positive PRBCs, and 3 units A plasma
- Blood bank keeps 4 units O negative PRBC, 12 units O positive PRBC, 12 units A plasma, 8 units platelets, and 25 units pre-pooled cryoglobulin (frozen).
-
- Whole blood is preferred in the initial resuscitation of hemorrhagic shock in patients age 6 and older.
-
- To activate the MTP, the attending physician (or designee) will notify the Blood Bank via telephone (402-559-3639) that MTP is being activated and provide the following information:
-
- Caller name and title
- Caller location
- Caller contact number
- Ordering provider’s name
- Patient’s name (may be the trauma name or real name)
- Patient’s MRN
- Category of MTP being activated (adult, pediatric, neonate/infant)
- Patient’s weight (kg)
-
Blood Product Administration and Transfusion Goals
- Minimize crystalloid or colloid resuscitation to prevent dilutional coagulopathy.
- Utilize emergency release blood products until MTP products are available.
- Blood products are released in 1:1 ratios of whole units but will be administered based on the clinical status of the patient and at the discretion of the attending physician.
-
- Maintaining a 1:1:1 transfusion ration of PRBC to FFP to Platelets is recommended. (Platelets are pooled-packs thus one apheresis platelets should be transfused for every 6 units of PRBC/FFP with the exception of neonatal/infant MTP resuscitations where apheresis platelets serves as FFP and platelet components). These rations help to avoid dilutional coagulopathy and thrombocytopenia and have been associated with decreased mortality.
-
- Pediatric Patients (≤40 kg), recommended volumes include:
-
- Whole blood -- 20 mL/kg
-
- if using whole blood during pediatric MTP, utilize entire unit of whole blood with repeated boluses of 20mL/kg before moving on to blood components.
-
- PRBC – 20 mL/kg
- FFP – 20 mL/kg
- Apheresis Platelets – 5 mL/kg
- Cryoprecipitate – 0.1 unit/kg
-
- Consider cryoprecipitate if serum fibrinogen levels remain less than 150 mg/dL following FFP.
-
- Whole blood -- 20 mL/kg
-
- Massive transfusion products should be administered rapidly and warmed via a rapid infuser with the exception of platelets
-
- For pediatric patients requiring smaller volumes, a “push-pull” system with 60mL syringe, stop-cock, and tubing may be utilized.
-
- Initial rate of transfusion should restore perfusion but allow permissive hypotension until bleeding has been controlled in the operating room or interventional radiology.
- Blood product resuscitation should be based on clinical evidence of ongoing bleeding in addition to quantitative data, such as ROTEM when available.
- Utilization of the patient’s own blood when safe (i.e. cell saver, autotransfusion from chest tube, etc) also provides readily available warm, matched blood.
Therapeutic Adjuncts in MTP
Tranexamic Acid (TXA)
- TXA is an antifibrinolytic used to treat coagulopathy. TXA should be initiated early in the coagulopathic cascade – within the first 3 hours of bleeding, in order to be effective.
- TXA should be administered based on the evidence of shutdown of fibrinolysis or hyper-fibrinolysis on ROTEM and/or provider discretion.
- Recommended dosing:
-
- <12 years:
-
- Loading dose of 15 mg/kg (max dose 1000mg) intravenous administered over 10 minutes
- Maintenance infusion of 2mg/kg/hr intravenous for 8 hours (max dose 1000mg)
-
- ≥12 years/Adult Dosing:
-
- Loading dose of 1000 mg intravenous administered over 10 minutes
- Maintenance infusion of 1000 mg intravenous over 8 hours
-
- <12 years:
-
Calcium
- The rapid rate of transfusion during MTP often exceeds the liver’s capacity to metabolize citrate, leading to severe hypocalcemia. Calcium is also required by several clotting factors for activation, stabilization of thrombus formation and contractility of myocardial and smooth muscle cells. Hypocalcemia can lead to coagulopathy, myocardial depression and vasodilation—all physiologic changes that complicate the management of hemorrhagic shock. Thus, adequate calcium repletion is an important component of MTP.
- Adults (>40 kg): 3g IV calcium chloride should be administered following completion of each MTP cooler.
- Pediatric patients (≤40 kg): 20 mg/kg IV calcium chloride should be administered after every 2 rounds of PRBC/FFP
Anticoagulant Reversal
- Injured patients in hemorrhagic shock with pre-existing anticoagulant use should be reversed with the appropriate reversal agent. See “Guidelines for Management of Bleeding in Patients Receiving Anticoagulation” (MP 11) for additional details.
***Please utilize Pharmacy for any questions regarding dosage and use of therapeutic adjuncts.***
Assessment of Coagulopathy and Transfusion Targets
- Coagulopathy
-
- Recommended initial lab testing at initiation of MTP include:
-
- CBC, PT/PTT, INR, fibrinogen, ROTEM
-
- Ongoing lab testing during MTP include:
-
- CBC, PT/PTT, INR, fibrinogen, and ROTEM every 4 hrs or as clinical situation indicates.
-
- ROTEM parameters
-
- A5EXTEM <35 mm OR ML ≥ 5% (within 60 min) à give TXA
- A5EXTEM <35 mm AND A5FIBTEM <9 mm à give cryoprecipitate
- A5EXTEM <35 mm AND A5FIBTEM ≥9 mm à give platelets
- CTEXTEM >80 s AND A5FIBTEM ≥9 mm à Give PCC or plasma
- CTINTEM > 240 s AND ( CTINTEM/CTHEPTEM) > 1.25 à give protamine, if suspected heparin activity or heparin like effects
- CTINTEM > 240 s AND ( CTINTEM/CTHEPTEM) < 1.25 à give plasma
-
- Recommended initial lab testing at initiation of MTP include:
-
- Acidosis
-
- Goal: Lactic Acid < 2
- Goal: Base Deficit <4
- Ongoing lab testing: Lactic acid and arterial blood gas (ABG) to assess acid-base status every 6 hrs during MTP or as clinical situation indicates.
-
- Hypothermia
-
- Goal: 36 degrees Celsius or warmer
- All trauma patients should undergo passive external rewarming including warmed blankets and increased ambient room temperature
- Administer warm blood products
- Continuously monitor utilizing core temperature probe.
-
- Hypocalcemia
-
- Goal: ionized calcium (iCa) >1.0 mmol/L
- Ongoing testing: iCa should be monitored at initiation of MTP and after completion of each MTP cooler.
-
- Hyperkalemia
-
- Goal: potassium <5
- Ongoing lab testing: Potassium every 6 hours or as clinical situation indicates.
-
Discontinuation and Transition to Goal Directed Therapy
- Ratio-driven massive transfusion may be discontinued and transitioned to goal-directed transfusion based on laboratory findings if surgical bleeding has been controlled or there is radiographic and physiologic evidence of bleeding control after embolization.
- MTP may also be discontinued when there is recognition that further resuscitation is futile.
- Suggested values for Goal Directed Therapy:
-
- Hemoglobin ≥ 10g/dL
- Platelets >150,000/mcL
- PT <18 seconds
- PTT < 35 seconds
- INR <1.5
- Fibrinogen >180
- ROTEM
-
- Clotting time (CT) – CTIN<215 and CTEX<75
- Amplitude 5 min after CT (A5)—A5IN,EX>33
- Amplitude 10 min after CT (A10)—A10IN,EX>45
- Maximum clot firmness (MCF)—MCFIN,EX>56 and MCFFIB>5
- Maximum Lysis (ML)—MLIN,EX,FIB<7%
-
-
Outcome Measures and Guideline Adherance
All trauma massive transfusion activations will be monitored through the trauma performance improvement (PI) process. Specific indicators that will be monitored/assessed include:
- Time from initiation of MTP to infusion of the first unit PRBCs
- Time from initiation of MTP to infusion of the first unit of plasma
- Overall ration of blood product transfusion and at 2 hours
- Total blood products used from MTP activation to 24 hours
- Notifying blood bank within 1 hour of MTP termination
- Use of therapeutic adjuncts
- Complications
Related Policies:
- TX36 Massive Transfusion/Severe Coagulopathy
- MP 11 Guidelines for Management of Bleeding in Patients Receiving Anticoagulation
Key Contributors
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Abby Josef, MD | Division of Acute Care Surgery, Faculty | Author
References
- American College of Surgeons Trauma Quality Improvement Program. (2015) ACS TQIP Massive Transfusion in Trauma Guidelines. Retrieved from transfusion_guildelines.pdf (facs.org)
- American College of Surgeons Advanced Trauma Life Support, 10th Ed. 2018.
- Callcut RA, Cotton B, Mskat P, Fox EE, Wade CE, Holcomb JB, Robinson RH. (2013) Defining when to initiate massive transfusion (MT): A validation study of individual massive transfusion triggers in PROMMTT patients. J Trauma Acute Care Surg.74(1), 59-67.
- Schroll R, Swift D, Tatum D, Courch S, Heaney JB, Llado-Farulla M, Zucker S, Gill F, Brown G, Buffin N, Duchesne J. Accuracy of shock index versus ABC score to predict need for massive transfusion in trauma patients. Injury. 49(1), 15-19.
- Napolitano LM, Cohen MJ, Cotton BA, Schreiber MA, Moore EE (2013). Tranexamic acid in trauma: How we should us it? J Trauma Acute Care Surg. 74(6), 1575-1586.
- Nunez TC, Voskrensensky IV, Dossett LA, Shinal R, Dutton WD, Cotton BA. (2009) Early prediction of massive transfusion in trauma: Simple as ABC (assessment of blood consumption)? J Trauma: Injury, Infection, and Critical Care. 66, 346-352.
- Panteli M, Pountos I, Giannoudis PV. (2016) Pharmacological adjuncts to stop bleeding: Options and effectiveness. Eur J Trauma and Em Surg. 42, 303-310.
- Stettler GR, Moore EE, Nunns GR, Chandler J, Peltz E, Silliman CC, Banerjee A, Sauaia A. (2018) Rotational thromboelastometry thresholds for patients at risk for massive transfusion. J Surg Res. 228: 154-159.
- Chidester SJ, Williams N, Wang W, Groner JI. (2012) A pediatric massive transfusion protocol. J Trauma Acute Care Surg. 73(5), 1273-1277.
- Eckert MJ, Wertin TM, Tyner SD, Nelson DW, Martin MJ. (2014) Tranexamic acid administration to pediatric trauma patients in a combat setting: The pediatric trauma and tranexamic acid study (PED-TRAX). J Trauma Acute Care Surg. 77(6), 852-858.
- Neff LP, Cannon JW, Morrison JJ, Edwards MJ, Spinella PC, Borgman MA. (2015) clearly defining pediatric massive transfusion: Cutting through the fog and friction with combat data. J Trauma Acute Care Surg. 78(1), 22-29.
Last updated:
May, 2024
REBOA Instructions
This page is intended to serve as a quick reference for easy access to the REBOA kit instructions. The information and images are directly from the insertion instructions, and were obtained from http://prytimemedical.com/wp-content/uploads/2017/08/ER-REBOA-Catheter-Quick-Reference-Guide-wall-poster.pdf

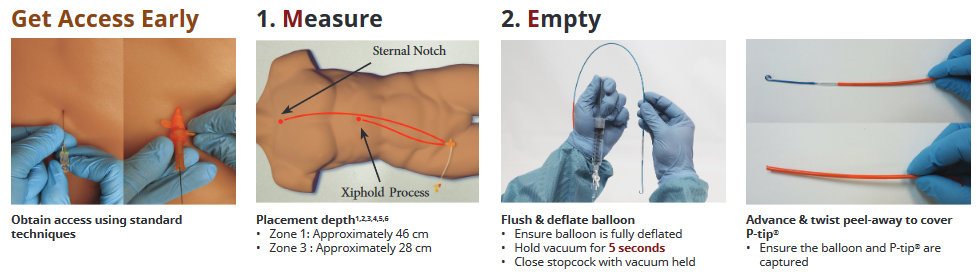
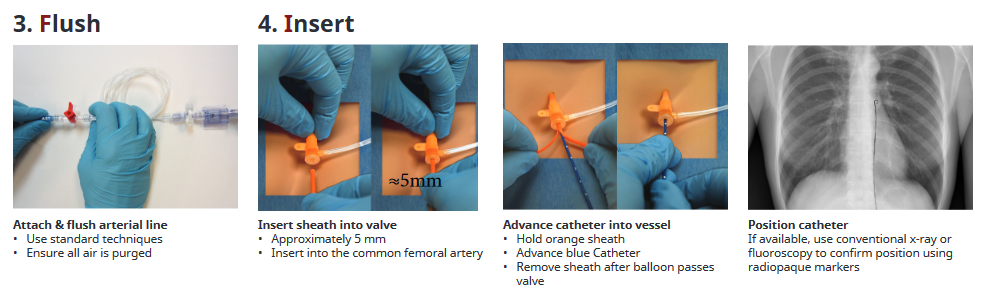
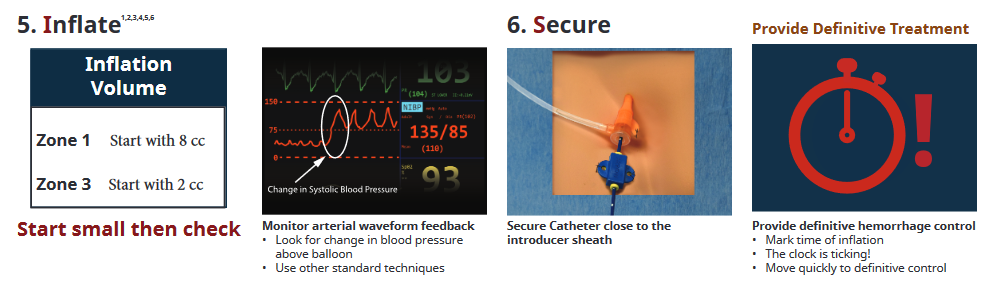
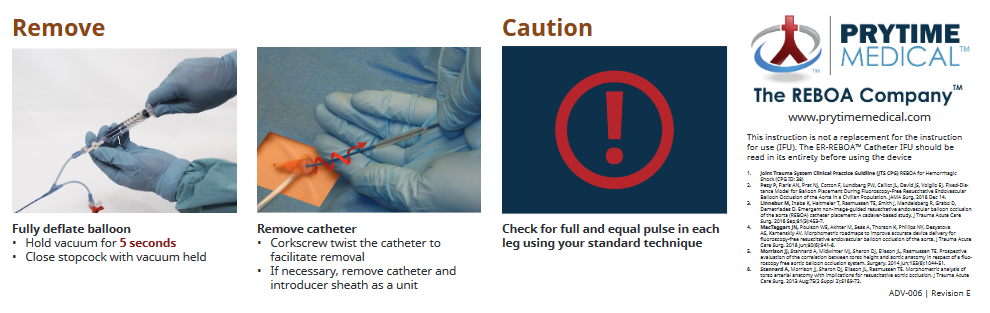
Whole Blood Usage in Trauma
Purpose:
The implementation of a whole blood program at Nebraska Medicine is designed to optimize our resuscitation practices for the hemorrhaging trauma patient. Whole blood, specifically Low Titer O Whole Blood (LTOWB) immediately delivers a balanced product with less preservative than individual components. It also has the advantage of being more convenient by giving one product instead of three to achieve a balanced transfusion ratio. The goal of this document is to standardize the management of resuscitation with LTOWB for hemorrhagic shock from a traumatic mechanism.
Definitions:
Low Titer O Whole Blood (LTOWB): a complete blood product that contains Type O red blood cells, plasma and platelets. It contains low levels of antibodies making it safe to transfuse to a patient with any blood type. Additionally, LTOWB contains less preservative than its respective components.
Protocol:
1. This protocol may be initiated in the Trauma Bay in the Emergency Department of Nebraska Medicine for trauma patients only
2. Whole Blood transfusion can only be activated by the attending physician or their surrogate
3. Patients who meet the following criteria are eligible to receive LTOWB
a. Patient is a male or female 6 years of age or older
b. Patient has significant and potentially life-threatening bleeding
c. Anticipated need for massive transfusion protocol (MTP)
4. Once a patient has been deemed eligible and the decision to transfuse LTOWB has been made, the attending physician or their surrogate will direct the ED nurse to begin the transfusion process in accordance with the established MTP/Severe Coagulopathy/Emergency Release Blood Administration Policy (TX 36)
5. After having been deemed eligible to receive LTOWB, a patient may receive a maximum of two units
6. Once a patient receives two units of LTOWB, the MTP should proceed in the usual manner, if indicated
7. Whole blood transfusion initiated in the Trauma Bay may be continued in other patient care areas such as the operating room, interventional radiology, or the intensive care unit
8. All other aspects of transfusion should proceed per established protocols
9. No additional testing is required following administration of LTOWB as the risk of transfusion reaction and hemolysis is thought to be similar to risks associated with uncrossmatched transfusions
FAQ:
Can LTOWB be used for non-traumatic patients?
- No, not at this time. Trauma pilot will run from Nov 2021 to April 2022, then will review for utilization and cost effectiveness.
2. How do I report blood transfused?
- Report LTOWB units separately. For example: 2 u LTOWB, 5 pRBCs, 5 FFP, 1 plts
3. Turn around time after utilization of the 2 u LTOWB in the trauma bay fridge?
- About 2 weeks
4. Do I need additional labs or studies before or after giving LTOWB?
- No, just a T & S within 10 min of accessing the product
5. When does LTOWB expire?
- 3 week topic life after collection, so will be stored in fridge for 2 weeks, then reprocessed
6. Can I give more than 2 units LTOWB?
- No, the 2 units are a bridge to MTP.
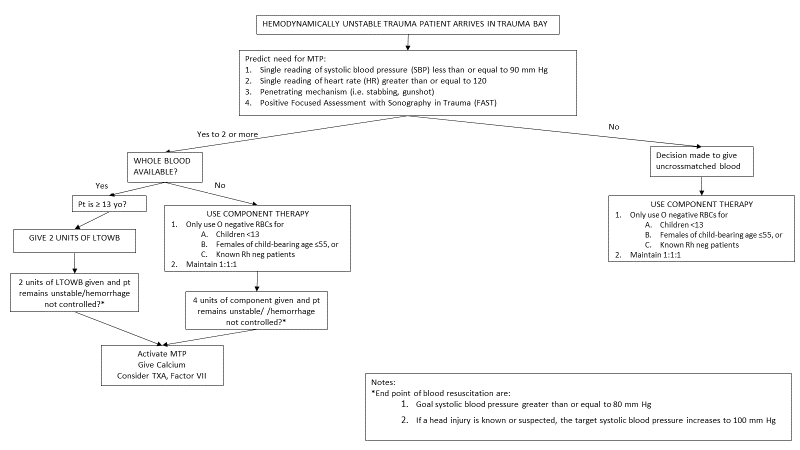
Trauma Bay Adult Acute Agitation Management
Purpose:
Traumatically injured patients presenting to the emergency department (ED) experiencing acute agitation have the potential to harm themselves, hospital staff, and others. Safe and expeditious management of agitation is imperative to prevent potential further harm. However, treatment of acute agitation is challenging due to the heterogenicity of the patient population, cause or source of agitation, and the available therapeutic treatment options.
There are two critical factors that are essential to the management of agitation – early recognition and targeted intervention to the etiology driving the patient’s acutely agitated state. This treatment protocol is designed to help streamline the care of this difficult patient population.
Background/Definitions:
Acutely agitated and/or violent behaviors displayed by trauma patients interfere with the required medical care of the patient. Acute agitation is a medical emergency. Determining the cause or causes of agitation will allow for a more informed management strategy for the patient. However, because of constraints on time, limited information, and lack of patient engagement, one must assess and identify the underlying cause(s) expeditiously. The goal of acute agitation treatment is to calm the patient in the least invasive way, without causing oversedation.
Per policy TX-1, the philosophy of Nebraska Medicine is to reduce/limit the use of physical and chemical restraint while maintaining the safety and preserving dignity, rights, and wellbeing of patients. Nebraska Medicine respects the patient’s right to be free of restraints of any form that are not medically necessary. If a patient’s condition necessitates the use of restraints, the safety and wellbeing of the patient and medical staff caring for the patient is the primary focus of the medical team.
· Severe Agitation:
o Currently violent or aggressive, attacking people and/or objects.
· Moderate Agitation:
o Physically or verbally threatening, difficult to redirect, extremely active, however, not violent.
· Mild Agitation:
o Signs of overt physical or verbal activity but redirectable.
· De-escalation:
o A combination of both verbal and nonverbal strategies intended to calm the patient down to cooperate with their care.
· Sedation and Analgesia:
o Use of pharmacologic agents to create a drug-induced state to reduce physiologic and psychological stress to a patient undergoing medical, surgical, or diagnostic procedures.
Common Medical Causes of Acute Agitation
|
Type |
Examples |
|
Neurological |
Traumatic brain injury, intracranial hemorrhage, seizure/post-ictal, stroke, encephalopathy |
|
Infectious |
Meningitis, sepsis, urinary tract infection (elderly) |
|
Metabolic |
Electrolyte disturbance, hypoglycemia |
|
Respiratory |
Hypoxia |
|
Toxicological |
Environmental toxin, medication reaction, illicit drug use |
|
Endocrine |
Thyrotoxicosis, myxedema coma |
|
Other |
Hyper- or hypothermia, acute pain |
Practice Recommendations for Medical Management:
· De-escalation should always be attempted prior to medication management and physical restraint.
· Restraint may only be imposed to ensure the immediate physical safety of the patient, staff or others and must be discontinued as soon as safely possible, regardless of the scheduled expiration of the order.
· TX_01 will be followed if/when restraint use is required.
· Follow the management considerations, listed in the table below, using the preferred agent(s) as listed in Attachment A. Preferred agents show better clinical properties, including onset of action, efficacy, and lower incidence of adverse effects.
Management Considerations for Agitation
|
Severity of Agitation |
Preferred Route of Administration |
Dosing Considerations |
Special Populations |
|
Severe |
IV, when able IM, if IV not available |
Maximize dose of first agent used, allowing for the onset and effects of the previous dose prior to administering second dose |
Dosing adjustments may be required for elderly, renally/hepatically impaired, and/or when given medication(s) prior to arrival. Lower doses may be required when using concomitant sedating medications. |
|
Moderate |
IV, when able IM, if IV not available |
Smaller doses may be sufficient (as compared to what is required for severe agitation) If able/known, use a patient’s home regimen when patients can tolerate oral therapy. |
|
|
Mild |
PO |
If able/known, use a patient’s home regimen when patients can tolerate oral therapy. |
Attachment A – Preferred Treatment Options for Acute Agitation (Trauma Bay)
Preferred Treatment Options: *
|
Preferred Options |
Medication |
Dose |
Soft Max (Single Dose) |
Onset |
Time to Peak |
Duration |
Patient Considerations |
|
Midazolam |
2-5 mg IV |
5 mg IV |
IV: 1-5 min |
IV: 3-5 min |
IV: 1-2 hours |
Hypotension with larger doses (IV). Delayed onset of action (IM). |
|
|
5-10 mg IM |
10 mg IM |
IM: 15 min |
IM: 30-60 min |
IM: 1-2 hours |
|||
|
Olanzapine |
2.5-5 mg IV |
5 mg IV |
IV: 5-10 min |
15-45 min |
2 hours |
Possible hypotension and respiratory depression with IV use. Caution when used with benzodiazepines due to risk of over-sedation. MAX 30 mg/24 hrs (Cumulative for all routes of administration) |
|
|
10 mg IM |
10 mg IM |
IM: 15 min |
|||||
|
Haloperidol |
5 mg IV/IM |
5 mg |
IV: 3-20 min |
IV: 30 min |
2-4 hours |
Risk of EKG changes Can lower seizure threshold |
|
|
IM: 15 min |
IM: 20-30 min |
||||||
|
Dexmedetomidine |
0.1-0.7 mcg/kg/hr IV, titrate to response |
MAX rate 0.7 mcg/kg/hr IV |
5-15 min |
60 min |
60-240 min (Dose dependent, after drip stopped) |
Restricted for Use in Non-Intubated Patients. Only approved indication is refractory agitated delirium unresponsive to other pharmacologic agents or with contraindications to other pharmacologic agents. Only available with IV access. Can cause bradycardia. Bolus dosing not allowed outside of OR. Restricted to ED, ICU, and OR use only. |
*Subject to drug availability/restrictions secondary to national drug shortage
Management Considerations for Ketamine:
At Nebraska Medicine, ketamine is restricted to the following indications:
· Induction for rapid sequence intubation
· Ventilator management
· Procedural sedation
· Subanesthetic analgesia (restricted ordering to anesthesiology, pain management, emergency medicine, and pediatric critical care medicine)
If ketamine is required for the use of acute agitation, the institutional policy, MS_15 for procedural sedation or MP_33 for subanesthetic ketamine for pain management, will need to be followed. A provider must remain at bedside.
Dosing recommendations:
· Sub-Anesthetic Ketamine for Pain
o Must be ordered by emergency medicine provider (while patient is in the ED).
o Use dosing recommendations per MP_33
· Procedural Sedation
|
Dose |
Soft Max (Single Dose) |
Onset |
Time to Peak |
Duration |
|
0.5 mg/kg IV |
1 mg/kg |
30-60 sec |
5-10 min |
1-2 hours (recovery) |
|
2 mg/kg IM |
3 mg/kg IM |
3-4 min |
5-30 min |
3-4 hours (recovery) |
· (MS_15) Medical Staff: Procedural Sedation and Analgesia Administration Guidelines (Non-Anesthesiology Providers)
· (TX_01) Care of Patients: Restraint Use
o Attachment A: Alternative Interventions to Restraints
· (TX_24) Admission, Transfer and Discharge for Define Levels of Care
· (MP_33) Medication Policy and Guidelines: Low-Dose (Sub-anesthetic) Ketamine for Pain in Non-Intubated Patients
Key Contributors:
· Krysta Baack, PharmD | Department of Pharmacy, Emergency Medicine | Principal Author
· Nathan Sutera, PharmD | Department of Pharmacy, Psychiatric Emergency Services | Author
· Zach Bauman, DO | Division of Acute Care Surgery, Faculty | Author
Last Updated:
July 2024
References:
1. Roppolo LP, Morris DW, Khan F, et al. Improving the management of acutely agitated patients in the emergency department through implementation of Project BETA (Best Practices in the Evaluation and Treatment of Agitation). JACEP Open 2020; 1:898-907.
2. Zareifopoulos N and Panayiotakopoulos G. Treatment options for acute agitation in psychiatric patients: theoretical and empirical evidence. Cureus 2019; 11(11): e6152.
3. Curry A, Malas N, Mroczkowski M, et al. Updates in the assessment and management of agitation. Focus (Am Psychiatr Publ) 2023; 21(1): 35-45.
4. Lexicomp. (2024). Midazolam: dosage & administration. In Lexi-Drugs Online. Retrieved [June 27, 2024.] from https://online.lexi.com.
5. Lexicomp. (2024). Olanzapine: dosage & administration. In Lexi-Drugs Online. Retrieved [June 27, 2024.] from https://online.lexi.com.
6. Lexicomp. (2024). Haloperidol: dosage & administration. In Lexi-Drugs Online. Retrieved [June 27, 2024.] from https://online.lexi.com.
7. Lexicomp. (2024). Dexmedetomidine: dosage & administration. In Lexi-Drugs Online. Retrieved [June 27, 2024.] from https://online.lexi.com.
8. Lexicomp. (2024). Droperidol: dosage & administration. In Lexi-Drugs Online. Retrieved [June 27, 2024.] from https://online.lexi.com.
9. Lexicomp. (2024). Lorazepam: dosage & administration. In Lexi-Drugs Online. Retrieved [June 27, 2024.] from https://online.lexi.com.
10. Lexicomp. (2024). Ketamine: dosage & administration. In Lexi-Drugs Online. Retrieved [June 27, 2024.] from https://online.lexi.com.
11. Li M, Martinelli AN, Oliver WD, et al. Evaluation of ketamine for excited delirium syndrome in the adult emergency department. J Emerg Med. 2019; S0736-S4679(19)30802-9.
12. O'Brien ME, Fuh L, Raja AS, et al. Reduced-dose intramuscular ketamine for severe agitation in an academic emergency department. Clin Toxicol (Phila). 2020;58(4):294-298.
3. Neurological Trauma
Educational materials and pathways regarding the evaluation and management of neurological injuries.
Cervical Spine Evaluation and Management
Cervical Spine Evaluation and Management
Purpose: Although cervical spine injuries are relatively uncommon among all trauma patients presenting to emergency departments (approximately 1-3%), cervical spine fractures and associated spinal cord or blunt cerebrovascular injuries can be potentially devastating to an individual. These guidelines serve to provide our trauma patients with an efficient and thorough evaluation of the cervical spine with either clearance of c-spine precautions or appropriate intervention and treatment of injuries when identified.
C-spine Precautions:
I. Who needs C-spine precautions?
a. All blunt trauma patients should be placed in c-spine precautions until the cervical spine can be appropriately evaluated and cleared.
b. Penetrating trauma patients do not need to be placed in c-spine precautions unless there is other associated blunt trauma or they are unevaluable and blunt force trauma cannot be excluded.
II. “C-spine precautions” includes:
a. Bedrest (until remainder of spine can be cleared/evaluated)
b. Head flat (in a neutral position)
c. C-spine immobilization in a rigid cervical collar (Philadelphia collar or Miami-J) at all times
d. Transport flat or in reverse Trendelenburg on a gurney
III. In low risk patients, after T&L spines have been cleared, the Trauma Attending or Fellow may use his/her judgement and write the c-spine precautions order to include “HOB may be 30 degrees up.”
C-Spine Evaluation and Clearance of Cervical Collar:
I. Routine c-spine clearance includes imaging of the cervical spine COMBINED WITH a clinical exam of the cervical spine.
a. A CT c-spine is the preferred imaging modality for evaluation of the cervical spine if the patient is scheduled to undergo another type of CT examination.
b. If cervical spine x-rays are obtained, they must be considered adequate films which allow complete visualization of all cervical vertebra (from the skull base down to T1).
c. NEXUS CRITERIA--In patients that are a GCS 15, examinable and no further CT scans are planned, the c-collar can be cleared clinically using the National Emergency X-Radiography Utilization Study (NEXUS) criteria without additional c-spine imaging.
i. NEXUS low-risk criteria include:
1. No posterior midline cervical-spine tenderness
2. No evidence of intoxication
3. A normal level of alertness
4. No focal neurologic deficit
5. No painful distracting injuries
If ALL of these criteria are met, no additional imaging is required and the c-collar may be cleared with clinical exam alone. If any of these criteria are not met, one should proceed with CT c-spine to further evaluate for cervical spine injury.
d. Special populations:
i. Pediatric patients (15 and younger)
1. If the child is awake/alert and examinable, the cervical spine should be attempted to be cleared with NEXUS Criteria.
2. If the child is obtaining CT scans for work-up of other injuries, obtain a CT c-spine.
ii. Elderly patients (age 65 yrs and older)
1. Elderly patients are more likely to have cervical spine injury without associated mid-line tenderness. In patients 65 years or older, have a lower threshold to obtain CT c-spine depending on the mechanism of injury.
II. Patients with any spinal fracture should have a radiologic exam of the entire spine.
III. C-spine clearance after negative imaging tests
a. Clinically clearing the c-spine involves performing a physical examination to rule out midline pain or tenderness with palpation and range of motion (ROM).
i. First, palpate the cervical spine down the midline. If the patient denies midline pain and tenderness with palpation, the anterior half of the collar may then be removed.
ii. Next, the patient should then be given clear instructions to slowly move his/her head from side to side (without assistance) and then back to front and to stop at any time if he/she experiences any pain/discomfort. If no midline cervical spine pain is appreciated with ROM, then the c-collar may be removed.
b. Both an order and a progress note (documenting that the patient’s C-spine has been both radiographically and clinically cleared) must be written in order to clarify that the patient no longer requires c-spine precautions.
IV. Any patient with:
a. Midline cervical pain or tenderness
b. A distracting injury or competing pain
c. Intoxication (any intoxicating substance)
d. Any head injury or impaired level of consciousness
e. Focal neurologic deficit
SHOULD NOT undergo attempted clinical exam/clearance until sensorium is cleared.
V. Patients who are obtunded due to injury, intubated for a prolonged period of time or are unable/incapable of having his/her c-spine cleared clinically:
a. C-collar maybe cleared based on negative imaging (CT C-spine) alone at the discretion of the trauma attending
b. consider MRI of the c-spine within the first 72 hours of admission (if clinically stable to do so) to rule out ligamentous injury in patients sustaining poly trauma or injury secondary to high energy mechanisms. If the MRI does not demonstrate signs of ligamentous injury, the C-collar may be removed.
C-spine Injury Present or Unable to Clear C-collar:
I. Any patient with complaints of midline pain or tenderness of the c-spine should be kept in a cervical collar regardless of their radiographic exam results.
II. Negative CT c-spine but persistent pain on clinical exam.
a. A second attempt to clear the cervical collar with exam should be made 12-24 hours following the initial attempt.
b. If still unable to clear a patient’s c-spine:
i. The patient should be instructed to wear the collar for 2 weeks and follow-up in Spine clinic for repeat evaluation and clearance of precautions. This has been approved by Drs. Wilson (Neurosurgery) and Vincent (Ortho Spine).
ii. Consider MRI c-spine in special populations such as elderly where the presence of a c-collar may result in significant dysphagia or impair balance or mobility. This should be discussed with the trauma attending prior to obtaining.
III. Any patient with a c-spine injury noted on imaging or has neurologic deficits present on exam should be maintained in c-spine precautions and receive a formal spine surgery consult (either neurosurgery or orthopedic spine service).
a. If other spine injuries are present, the consulting spine team will be responsible for clearance of the cervical spine.
b. Patients with any cervical or > 3 thoracic/lumbar isolated transverse process or spinous process fractures should receive spine consultation.
IV. Some cervical spine fractures are associated with increased risk of blunt cerebrovascular injury (BCVI) and should be investigated with a CTA neck. Risk factors for BCVI are high energy transfer mechanisms associated with:
a. Displaced mid-face fracture (LeForte II or III)
b. Basilar skull fracture involving carotid canal
c. Closed head injury consistent with diffuse axonal injury and GCS <6
d. Cervical body fracture or transverse foramen fracture, subluxation or ligamentous injury at any level
e. Cervical fractures, at any level
f. Near hanging with cerebral anoxia
g. Clothesline type injury or seatbelt abrasion (sign) with significant swelling, pain or altered mental status.
V. Patients who require a c-collar for extended periods of time are at risk for skin breakdown and pressure wounds.
a. Mechanisms to prevent this include:
i. exchange the Philadelphia collar to a Miami-J collar
ii. ensure collar fits properly and has pads in appropriate locations
iii. consider consulting Hanger or Burton for custom fit cervical collars
iv. nursing is performing appropriate c-collar cares daily
1. cervical collar care performed q shift to assess skin for red/opened areas
2. pads should be changed daily and as needed if soiled
3. if patient is on flat bedrest, consider using ICU occipital back panel with Vista collar to reduce skin breakdown
REFERENCES:
1. Grossman MD, Reilly PM, Gillett T, Gillett D. National survey of the incidence of cervical spine injury and approach to cervical spine clearance in U.S. trauma centers. J Trauma. 1999; 47(4):684-90.
2. Hoffman JR, Mower WR, Wolfson AB, Todd KH, Zucker MI. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. National Emergency X-Radiography Utilization Group. N Engl J Med. 2000; 343(2):94-9.
3. Inaba K, Byerly S, Bush LD, Martin MJ, Martin DT, Peck KA, et al. Cervical Spinal Clearance: A Prospective Western Trauma Association Multi-Institutional Trial. J Trauma Acute Care Surg. 2016; 81(6):1122-30.
4. Ciesla DJ, Shatz DV, Moore EE, Sava J, Martin M, Brown CVR, Alam HB, Vercruysse G, Brasel K, Inaba K. Western Trauma Association critical decisions in trauma: cervical spine clearance in trauma patients. J Trauma Acute Care Surg. 2020;88(2):352-54.
5. Biffl WL, Cothren CC, Moore EE, Kozar R, Cocanour C, Davis JW, McIntyre RC, Jr., West MA, Moore FA. Western Trauma Association critical decisions in trauma: screening for and treatment of blunt cerebrovascular injuries. J Trauma.2009;67(6):1150-3.
6. Patel MB, Humble SS, Cullinane DC, Day MA, et al. Cervical spine collar clearance in the obtunded adult blunt trauma patient: a systematic review and practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg 2015; 78(2):430-441.
Intracranial Hypertension Management Algorithm
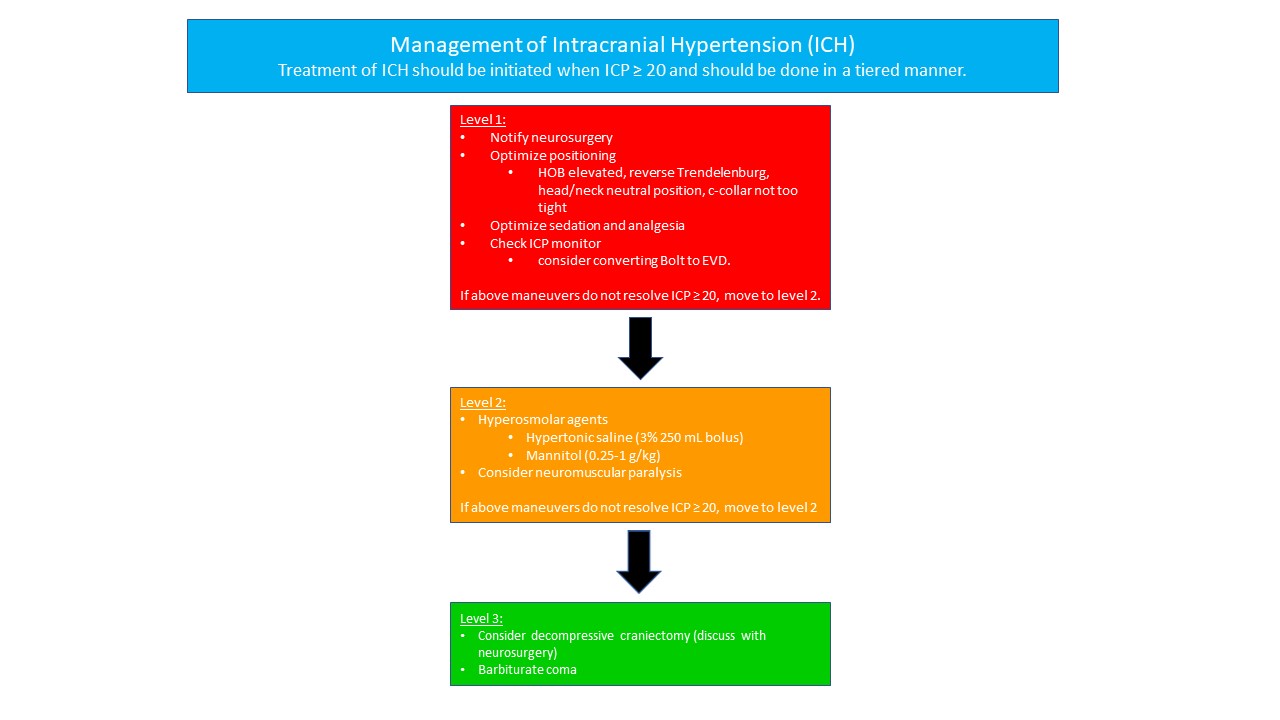
Management of Traumatic Brain Injury
Management of Traumatic Brain Injury
This document provides an overview of considerations and guidelines that are important in the evaluation and management of patients with traumatic brain injury (TBI). It is not intended to be used a rigid set of treatment instructions. Management of TBI must be individualized based on each patient’s clinical situation and the clinical judgment of the providers responsible for directing this aspect of patient care.
Resuscitation and Basic Physiological Goals
The following physiological parameters should be maintained as part of goal directed TBI treatment:
- Primary Parameters:
-
-
-
- Pulse Ox ≥ 90%
- PaO2 ≥ 100 mmHg
- PaCO2 35-40 mmHg
- SBP ≥ 110 mmHg and ≤ 160 mmHg
- pH 7.35-7.45
- ICP < 20 mmHg
- Temp 36.0-38.3⁰C
- Glucose ≤ 160 mg/dL
- INR ≤ 1.3
- Sodium goal
- Normonatremia (Na 135-145 mmol/L) vs permissive hypernatremia (Na 145-155 mmol/L)
-
-
-
- Secondary Parameters
-
-
- Cerebral Perfusion Pressure (CPP)
-
- Avoid aggressive use of pressors or fluids to maintain CPP > 70 mm Hg
- Avoid CPP < 60
- Pediatrics: CPP 40-50 mmHg
-
- Cerebral Perfusion Pressure (CPP)
- PbtO2 ≥ 15 mmHg
-
-
- Required monitoring/measurements in patients with severe TBI requiring mechanical ventilation
-
- Continuous SpO2 and EtCO2 monitors
- Indwelling urinary catheter to monitor UOP; may consider transition to external catheter after first 24 hrs
- Arterial catheter with continuous arterial pressure monitoring
- Hourly neurological exams
-
1. Airway Management
- Patients with a GCS < 8 should be intubated for airway protection
- Patients with a GCS < 10 should be considered for intubation.
- Intubation should be performed with in-line cervical spine immobilization.
- Rapid sequence intubation (RSI) is the preferred method.
- If clinical scenario allows, a baseline neurological exam should be obtained prior to intubation.
- Sedative and analgesic choices should favor short acting agents throughout the initial resuscitation, as temporal assessment of neurological status is critical. In general, the following agents are recommended:
- Etomidate – sedation for induction
- Succinylcholine – paralytic for induction
- Propofol – maintenance of sedation and prevention of agitation. Propofol should not be used as an induction agent in the case of trauma and is to be discontinued if its use results in persistent hypotension requiring vasopressor agents.
- Benzodiazepines – (i.e., midazolam or lorazepam) can be utilized as an initial or substitute sedative agent for propofol.
- Dexmedetomidine (Precedex)—maintenance sedation and analgesia; can also cause hypotension and bradycardia
- Fentanyl – can be used for PRN and maintenance analgesia as well as provide some sedation effects.
2. Oxygenation/Ventilation
- Avoidance of Hypoxia
- Efforts should be made to avoid hypoxia at all times as it has been shown in significantly worsen outcomes in TBI patients.
- Patients with TBI should have a pulse oximetry maintained at SpO2 ≥ 90% and an attempt for PaO2 ≥ 100 mmHg.
- Ventilation
- Hyperventilation should be intensively monitored during the initial resuscitation.
-
- Target PaCO2 is 35-40 mmHg.
- Prophylactic Hyperventilation is not recommended (PaCO2 < 25 mmHg)
- An ETCO2 monitor and serial ABGs should be used as needed to prevent profound hypocarbia or hypercarbia.
- Therapeutic hyperventilation may be necessary for brief periods when there is acute neurological deterioration that coincides with a cerebral herniation syndrome or for refractory elevations in ICP (see section on management of intracranial hypertension).
-
- Hyperventilation should be intensively monitored during the initial resuscitation.
3. Blood Pressure, Volume Resuscitation
- Blood Pressure
- Systolic blood pressure (SBP) and mean arterial pressure (MAP) readings should be recorded from a functioning arterial line, when present, or from non-invasive blood pressure (NIBP) cuff when arterial line is not present or presumed inaccurate.
- Strict blood pressure monitoring and control is required in all TBI patients with care taken to avoid hypotension and hypertension.
-
- Any patient with intra-cranial hypertension must have an arterial line.
- SBP should be kept between 110 mmHg and 160 mmHg for the first 7 days following injury or until discharge if patient discharged prior to 7 days.
-
- it should be noted that even one episode of hypotension (SBP<100mmHg) can significantly worsen outcomes in TBI patients.
-
- It should be recognized that lower blood pressures can represent a “relative” hypotensive state in TBI patients (especially with elevated ICP)
- Normal saline, PRBC, and FFP (when needed) should be used as the initial method of maintaining euvolemia to achieve the target blood pressure
- Use of vasopressors should be considered for treatment of refractory hypotension ONLY AFTER appropriate volume resuscitation has been given.
- Vasopressors and Inotropes including phenylephrine, norepinephrine, epinephrine, dobutamine, dopamine, and vasopressin should not be used to counteract the hemodynamic effects of propofol, Precedex or other sedating medications.
- Labetalol or hydralazine as needed should be administered to treat SBP > 160 mmHg during the initial resuscitation phases.
- If SBP > 160 mmHg is sustained, consider initiation of nicardipine gtt and/or scheduled beta blocker therapy and placement of arterial line, if not already present.
- Review home medication lists and consider resuming anti-hypertensive medications as clinically indicated.
-
- Euvolemia
- The primary target is euvolemia through resuscitation. In many cases, a bedside point of care ultrasound (POCUS) with evaluation of the IVC and cardiac function can give the clinician a reasonable assessment of volume status.
- Avoid use of hypotonic fluids for volume resuscitation and maintenance fluid support.
4. Anemia and Coagulopathy
- Hematologic and coagulation panels (CBC, PT/INR, PTT, TEG, fibrinogen, anti-Xa levels, platelet mapping) should be followed closely, particularly in patients on anti-coagulation medications or pre-existing bleeding dyscrasias.
- Patients on anti-coagulant or anti-platelet medications or those with bleeding disorders should be reversed/corrected as clinically indicated to correct coagulopathy regardless of need for surgical intervention. Potential interventions include the following: FFP, vitamin K, prothrombin complex concentrate (PCC)/KCentra, platelets, DDAVP, and NOAC specific reversal agents.
-
- For patients on antiplatelet medications (i.e. aspirin, Plavix, brilinta), 1 unit of platelets may be transfused if requested by Neurosurgery at the discretion of the trauma or surgical ICU attending. Decision to transfuse additional units of platelets should be based on results of TEG or platelet mapping.
-
- Target coagulation parameters:
-
- Hb > 7 g/dL
- Platelet count > 100 x 103/uL (if clinically feasible)
- INR ≤ 1.5
- Fibrinogen > 150 mg/dL
-
- INR and platelet count should be corrected in anticipation of operative intervention or bedside procedure such as placement of ICP monitor.
5. Imaging
- All patients with suspected or at high risk for possible TBI (i.e., LOC, significant mechanism, amnesia to event, use of anticoagulant/antiplatelet medications) must undergo urgent CT head (CTH) during the initial resuscitation barring need for emergent operative intervention for other life-threatening injuries.
- Repeat CT head will also be obtained at a specified time interval, per neurosurgery recommendations. (within 24 hours of presentation and/or with any significant deterioration in patient’s neurologic status). Additional CT scans will be obtained as needed based on patient clinical condition.
- MRI brain scans should be utilized for assessment of ischemic CVA, DAI, tumors/masses or per certain research protocols. MRI brain can also be used to help prognosticate/determine potential for neurologic viability, particularly in patients with persistent vegetative states. Discussion between Neurosurgery, Neurology, and Trauma can help determine timing and value of the MRI.
6. Sedation and Analgesia for intubated TBI patients
- Sedation and analgesia agents will be chose and titrated at the discretion of the surgical ICU attending’s discretion
-
- Propofol – maintenance of sedation and prevention of agitation. Propofol should not be used as an induction agent in the case of trauma and is to be discontinued if its use results in persistent hypotension requiring vasopressor agents.
- Benzodiazepines – (i.e., midazolam or lorazepam) can be utilized as an initial or substitute sedative agent for propofol.
- Dexmedetomidine (Precedex)—maintenance sedation and analgesia; can also cause hypotension and bradycardia
- Fentanyl/Dilaudid – can be used for PRN and maintenance analgesia as well as provide some sedation effects.
-
- Ideally, initial agents chosen should favor shorter acting agents so that serial neurologic exams can be obtained.
- In general, sedation will be titrated to RASS goal 0 to -2 unless deeper sedation deemed medically necessary by the surgical ICU attending. (i.e. intracranial hypertension, post-traumatic seizures, etc.)
-
- If ICP monitor in place, sedation should be titrated to maintain ICP < 20 mm Hg.
-
Intracranial Pressure (ICP) Monitoring
- Placement of ICP monitoring should be considered in the following:
-
- In patients with a salvageable traumatic brain injury (TBI) if the GCS is </= 8 following the initial resuscitation and the admission CT scan of the brain is abnormal (i.e., hematomas, contusions, edema, herniation or compressed basal cisterns).
- Patients undergoing emergent surgical procedures (orthopedic interventions, exploratory laparotomy, etc.) in whom a moderate to severe brain injury is suspected (GCS 3-12) to help guide appropriate intraoperative ICP management.
- Patients with a normal admission CT scan of the brain but have two or more of the following criteria,
-
-
- Age >40 y/o
- Unilateral or bilateral motor posturing
- Documented episode of hypotension (SBP<90mm Hg)
-
-
-
- ICP monitors may include an intraventricular catheter (EVD) and/or parenchymal monitor (Bolt).
-
- Patients with suspected increase in intracranial pressure and GCS ≤ 8 should receive an intraventricular catheter (EVD) or parenchymal monitor at the discretion of the treating Neurosurgeon as the clinical situation mandates.
-
- Ideally, ICP monitor should be placed within the first 12 hours following admission. ICP monitor placement may also occur later in the resuscitation if the patient’s clinical status declines/changes so that ICP monitoring is now warranted.
- Relative contraindications to ICP monitor placement:
-
- The brain injury is not felt to be salvageable/survivable.
- Coagulopathy (INR>1.3)
- Patient is awake/GCS ≥ 9
- Mass lesion with mass effect at the site of the ventriculostomy site
- Patient known to be post-ictal without obvious brain injury
- Metabolic causes of coma including intoxication without good evidence of head injury
-
- Removal of the ICP monitor will be at the discretion of the treating neurosurgeon but should be considered when:
-
- ICP within normal range
- 48 to 72 hours after interventions for elevated ICP.
-
- Target parameters:
-
- ICP < 20 mmHg
- Cerebral Perfusion Pressure (CCP) ≥ 60 mmHg.
-
Treatment of Intracranial Hypertension
- Intracranial hypertension is defined as sustained elevation in intracranial pressure (ICP) of more than 15 to 20 mmHg sustained for greater than 5 minutes and occurs when the three intracranial components—blood, brain, and cerebrospinal fluid (CSF)—are no longer able to compensate for volume changes occurring within the cranium.
- Treatment for intracranial hypertension should be initiated when ICP ≥ 20 mmHg and is managed with a leveled algorithm with each level representing increasing levels of intensity. Patients should be initiated in Level 1, then staged through Level 3 as indicated. If the treatments in a given level have not sufficiently lowered the ICP within 20 minutes of implementation, then advancements to the next level should be promptly initiated.
-
- Level 1
- Notify Neurosurgery
- Positioning-- Elevate head of patient’s bed to ≥ 30 degrees or reverse Trendelenburg position if the T/L spine has not been cleared or there is a known fracture precluding the upright position. Maintain head and neck aligned in a midline neutral position and ensure cervical collar is not restrictively tight.
- Optimize sedation and analgesia using recommended agents (propofol, fentanyl and versed) in intubated patients.
- ICP monitor – ensure ICP monitor is functioning properly. If EVD in place, lower and/or open to drain CSF to assess patency. If parenchymal monitor in place, consider converting to EVD if situation allows.
- If the above maneuvers have not resolved the elevated ICP, move to Level 2.
- Level 2
- Hyperosmolar agents
-
- Hypertonic Saline – intermittent boluses of 3% saline (250 mL) may be given in the setting of increased ICP and is preferred if the patient has hypotension or is hypovolemic. Serum sodium and osmolality must be assessed every 6 hours and additional doses should be held if the serum sodium exceeds 160 mEq/L or serum osmolality > 360 mOsm/L
- Mannitol – intermittent boluses of mannitol (0.25-1gm/kg body weight) may also be administered Attention must be placed upon maintaining a euvolemic state as mannitol will induce an osmotic diuresis. The serum sodium and osmolality must also be assessed frequently (every 6 hrs) and additional doses should be held if the serum sodium exceeds 320 mOsm/L. Maintain a serum osm < 320 mOsm/L with a targeted serum Na of < 160 mEq/L.
-
- Neuromuscular paralysis: pharmacologic paralysis with a continuous infusion of a neuromuscular blocking agent should be considered if the above measures fail to adequately lower the ICP and restore CPP. The infusions should be titrated to maintain at least two twitches (out of a train of 4) using a peripheral nerve stimulator. Adequate sedation must be utilized if pharmacologic paralysis is employed and can be confirmed with BIS monitoring.
- If the above maneuvers have not resolved the elevated ICP, move to Level 3.
- Hyperosmolar agents
- Level 3
- CTV head should be considered to evaluate for cerebral sinus thrombosis
- Decompressive hemi-craniectomy or bilateral craniectomy should be discussed and performed at neurosurgery attending discretion.
- Barbiturate coma – an induced coma is an option for those patients who have failed to respond to aggressive measures to control malignant ICP including decompressive craniectomy. The use of BIS monitoring or equivalent is needed for assurance of adequate sedation and coma. Side effects include sudden hemodynamic collapse and a high incidence of pneumonia. Appropriate volume resuscitation and hemodynamic monitoring is mandatory. Utilizing vasopressor therapy may be warranted.
- Level 1
-
Adjunctive Medications and Prevention of Complications
- Antiseizure prophylaxis
-
- Keppra (levetiracetam) is the preferred anti-seizure medication given its lower side-effect profile, fewer drug interactions, and less need for tight monitoring of serum levels. Phenytoin/Fosphenytoin (Dilantin) also as efficacy in preventing early post-traumatic seizures in patients with TBI. Seizure prophylaxis should be considered for discontinuation after 7 days if no seizure activity occurs. However, a longer duration should be considered with certain injury patterns or in the presences of post-traumatic seizures.
-
- Stress Ulcer Prophylaxis
-
- Patients with significant TBI requiring mechanical ventilation as well as those with coagulopathies or a history of peptic ulcer disease should receive stress ulcer prophylaxis with either an H-2 block agent (famotidine) or proton pump inhibitor.
-
- Deep Venous Thrombosis (DVT) prophylaxis
-
- All patients with TBI should receive DVT prophylaxis in the form of sequential compression devices upon admission. Chemoprophylaxis (subcutaneous Lovenox or heparin) should be initiated 48 hours following injury/procedure for most intracranial hemorrhages and after craniotomy OR 24 hours following last stable CT head unless specifically requested by the neurosurgical attending. (see guidelines for VTE prophylaxis in trauma patients)
-
- Early Tracheostomy
-
- Tracheostomy within 7 days of admission is recommended in ventilator dependent patients to reduce total days of ET intubation. This is performed at the discretion of the trauma and neurosurgery services.
-
- Nutritional Support
-
- Nutritional support should be initiated via enteral route within 48 hours post injury. Frequent assessment of residual volumes of gastric nutrition should be performed, as patients with TBI frequently do not tolerate intragastric feeding and are at risk for emesis and aspiration. Efforts should be made to obtain post-pyloric feeding access (i.e. Cortrak) when possible. Consider holding tube feeds if gastric residual volumes >500 ml.
-
Surgical Management of TBI
Surgical interventions for severe TBI will ultimately be performed at the discretion of the neurosurgery attending/service. However, there are certain criteria and situations where surgery should be considered.
- Epidural hematomas
-
- An epidural hematoma (EDH) of greater than 30 cm2 should be surgically removed regardless of GCS. Patients with an acute EDH, GCS <9 and anisocoria should undergo emergent EDH evacuation.
- Continued non-operative management should be considered in posterior EDH of venous origin.
- EDH of less than 5mm midline shift in patients with GCS >8 and no focal deficit can be closely monitored in an ICU with serial CT scans. Judicious use of narcotics and sedatives is important to minimize drug related alterations in the neurologic exam. Repeat CT head should be obtained within 6 hours if patients are to be managed non-operatively.
-
- Acute Subdural Hematomas
-
- Acute subdural hematomas (SDH) with a thickness of greater than 10 mm or 5mm of midline sift on CT scan should be considered for emergent evacuation regardless of GCS. (Clinical judgement should be used in patients with significant underlying atrophy)
- A SDH less than 10mm thickness and less than 5mm midline shift should be evacuated emergently if the patient has: GCS decrease by 2 points, asymmetric or fixed pupils, or ICP > 20 mmHg.
- Repeat CT head should be obtained within 24 hours or sooner if there is deterioration in patient’s neurologic status.
-
- Subarachnoid Hemorrhage
-
- In general, subarachnoid hemorrhage (SAH) is managed non-operatively. All patients with GCS ≤ 8 and SAH should have ICP monitoring with an EVD as the preferred monitoring of choice.
- Repeat CT head should be obtained within 24 hours or sooner if there is deterioration in patient’s neurologic status.
-
- Parenchymal lesions
-
- Intraparenchymal hemorrhage (IPH) causing progressive neurological deterioration, medically refractory ICP elevations, or significant mass effect should be considered for emergent evacuation.
- Frontal or temporal contusions with IPH > 3cm3 and >5 mm shift or cistern compression in patients with GCS < 8 should be considered for surgical evacuation.
- Normal ICP should not preclude operative.
- Repeat CT head should be obtained within 24 hours or sooner if there is deterioration in patient’s neurologic status.
-
- Diffuse Medically Refractory Cerebral Edema and Intracranial Hypertension
-
- Decompressive craniectomy (unilateral or bilateral) within 48 hours of injury should be considered for patients with elevated ICP (>20) refractory to medical management.
- Ultra-early decompressive craniectomy prior to ICP monitoring is not recommended unless surgery is performed for a mass occupying lesion (hematoma) and the bone flap is not replaced.
-
- Depressed Skull Fractures
-
- Open skull fractures depressed greater than the thickness of the inner and outer table should be considered for surgical management.
- Referable symptoms attributed to the fracture site are an indication for operative management.
- Open depressed fractures that are less than 1cm depressed and have no dural penetration, no significant intracranial hematomas, no frontal sinus involvement, no gross cosmetic deformity, no pneumocephalus, and/or no gross wound contamination may be non-operatively.
- All open skull fractures should be considered for treatment with prophylactic IV antibiotics with CSF penetration.
-
References
- Brain Trauma Foundation, Guidelines for the Management of Severe TBI, 4th ed. (braintrauma.org)
- Brain Trauma Foundation, Povlishock JT, Bullock MR. Cerebral perfusion thresholds. J Neurotrauma 2007; 24: S59-S64
- Brain Trauma Foundation, Povlishock JT, Bullock MR. Hyperventilation. J Neurotrauma. 2007; 24:S87-S90
Modified Brain Injury Guidelines (mBIG)
mBIG guidelines apply only to adult trauma patients (18 yrs and older). Pediatric trauma patients (less than 18 yrs of age) are excluded from these guidelines and neurosurgical consultation should be obtained for any intracranial hemorrhage.
Modified Brain Injury Guidelines (mBIG)

Treatment Plans:
mBIG 1:
- Place in observation (2OBS) if isolated head injury, otherwise admit to appropriate level of care
- Neuro checks q2 hours (if in 2OBS), otherwise neuro checks q4 hours
- If exam stable after 6 hours in 2OBS, discharge if GCS 15
- No Keppra, no BP goals, OK to start DVT prophylaxis if not being discharged after 6 hours
- Follow-up with neurocritical care outpatient**
mBIG 2:
- Admission to SDCC if isolated head injury, otherwise admit to appropriate level of care
- Neuro checks q2 hours
- Repeat CT-head at 6 hours, OK to start DVT prophylaxis after 24 hours from stable head CT
- Neuro checks q4 hours after 24 hours observation
- Keppra 7 days, no BP goals
- Follow-up with neurocritical care outpatient**
mBIG 3:
- Neurosurgery consultation
- Follow-up with neurosurgery outpatient

Pharmaceutical Management of Post-TBI Neuropsychiatric Symptoms
Definitions
1. Depression: TBI-associated depression is characterized by prolonged, persistent sadness associated with other symptoms such as anhedonia, lack of motivation, decreased self-care, variable sleep and/or appetite pattern, feelings of hopelessness, and/or suicidal thoughts. These symptoms may last for a couple of weeks to months (major depressive episode) or persist in a milder form for two or more years (dysthymia).
2. Mania/Agitation: Subtype of delirium unique to TBI which occurs during period of Post traumatic amnesia (PTA – period of time in which new memory formation is impaired), characterized by excess of behavior that includes some combination of aggression, disinhibition, akathisia, disinhibition, and emotional liability IN ABSENCE of other physical, medical or psychiatric causes.
3. Anxiety: A wide range of anxiety disorders may occur after TBI including generalized anxiety disorder, agoraphobia, social phobia, panic disorder, and obsessive-compulsive disorder.
4. PTSD: Symptoms may include nightmares or unwanted memories of the trauma, avoidance of situations that bring back memories of the trauma, heightened reactions, anxiety, or depressed mood.
5. Psychosis: There are predominantly 2 types of TBI-related psychosis: delusional disorders and schizophrenia-like psychosis.
6. Sleep disturbance: Sleep disturbances are common after TBI and can occur in isolation or as a symptom of a psychiatric disorder. Insomnia is the most common sleep disturbance, seen in about 50% of patients with TBI, although other disturbances such as hypersomnia, sleep apnea, and sleepwalking may also be present.
7. Executive function deficits: The constellation of cognitive impairments following TBI is variable and depends on the severity of the location of the injury on the brain. TBI can affect every cognitive domain, including attention, memory, visual-spatial processing, language, social cognition, and executive functioning.
Assessment and Diagnosis
1. Mania/Agitation- Agitated Behavior Scale where 22-28 is mild agitation, 29-35 is moderate agitation, and 36-56 is severe agitation.
2. Depression- PHQ 9 where 1-4 is minimal depression, 5-9 is mild depression, 10-14 is moderate depression, 15-19 is moderately severe depression and 20-27 is severe depression
3. Anxiety: GAD-7 where 0-4 is minimal anxiety, 5-9 is mild anxiety, 10-14 is moderate anxiety, and 15-21 is severe anxiety
4. PTSD: ITSS where PTSD is evaluated in items 3, 4, 7, 8, 9 and Depression is evaluated in items 1, 2, 3, 5, 6. If the sum of questions 1, 2, 3, 5, and 6 is equal to or greater than 2, the screen is positive for PTSD risk. If the sum of questions 3, 4, 7, 8 and 9 is equal to or greater than 2, the screen is positive for depression risk.
5. Memory deficits, executive function deficits, and inattention: consult Speech Therapy for cognitive evaluation
Pharmacologic Management
General Considerations for all patients:
Propranolol - Patients with TBI by CT and GCS <12, hemodynamically stable at 24 hrs after admission (BP>100, not requiring vasopressor or blood transfusion) should be started on propranolol 20 mg po q12hrs . If patient develops bradycardia (HR<50 bpm) or hypotension (SBP <100mmHg), then propranolol should be stopped. Increase the dose from 20 mg BID to 40 mg BID based upon SBP>140s, and HRs> 110-120s. (Of note, if BP remains high, consider adding another agent). Propranolol should be stopped upon discharge or after 7 days, whichever is sooner.
In patients on home beta-blockers (for hypertension, heart failure, afib rate control), switch to propranolol temporarily and stop the home beta blocker (avoid ordering 2 beta blockers on the same patient). Propranolol dose can be titrated up if needed for BP or HR) or a second antihypertensive ordered.
Clonidine – has unclear role for use in TBI patients for agitation or storming. Its use as adjunct therapy in withdrawal syndromes is longstanding. It is explored for use as a transition-off agent in patients on dexmedetomidine and as an adjunct in treating PSH. Thus, practical uses for clonidine include: treating agitation in conjunction with withdrawal syndromes, treating agitation/delirium in a patient weaning off dexmedetomidine or whom dexmedetomidine was effective, 3-4th line in PSH (after gabapentin, opiates, benzos have been tried/considered). Initial dosing should be 0.1 mg PO TID. If patient is already on dexmedetomidine, the dose can be started at 0.2-0.3 mg TID and the dexmedetomidine can be decreased. Side effects include: hypotension, rebound hypertension, withdrawal.
Antipsychotics and stimulants– Generally for short-term use, should be tapered when symptoms resolve. Use assessment tools prior to initiation of pharmacologic agents to ensure you are treating the correct symptom.
All new antipsychotics and stimulants should be reviewed and weaned (if possible) at time of transfer from ICU to floor, and again, at time of discharge from hospital.
|
Assessment tool |
First line medications |
Standard dosage |
Common adverse effects |
|
|
Depression |
PHQ 9 |
Sertraline |
Start: 25 or 50 mg daily.
May double dose after 1 week, assess for effect in 4 weeks before further increasing. |
Nausea, diarrhea, sexual dysfunction |
|
Manic: acute |
Agitated Behavior Scale |
Quetiapine |
Start: 25-50 mg BID
Increase to effect to maximum of 400 mg/day |
Sedation, Parkinsonism, weight gain, QTc prolongation |
|
Mania: maintenance |
Agitated Behavior Scale |
Valproate |
Start: 250 mg TID
May load with 15 mg/kg for rapid symptom control
May increase every 2-3 days, checking level to ensure not above range |
Hepatotoxicity, hyperammonemia, thrombocytopenia, drug interaction with carbapenems
Safe therapeutic range: 50-125 mcg/mL |
|
Anxiety |
GAD-7 |
Sertraline |
Start: 25 mg daily
May double dose every 2 weeks until 100 mg daily reached. Assess in 4 weeks before further increasing. |
Nausea, diarrhea, sexual dysfunction
Low dosing to avoid worsening anxiety during initiation period |
|
PTSD |
ITSS |
Sertraline or paroxetine |
Sertraline Follow anxiety dosing
Paroxetine Start: 20 mg daily, may increase in 10 mg increments per week up to 60 mg daily. |
Nausea, diarrhea, sexual dysfunction
Paroxetine has higher sedating effect. |
|
Psychosis |
|
Risperidone or quetiapine |
Quetiapine Acute dose: 25 mg If scheduled dose indicated, same as above.
Risperidone Acute dose: 1-2 mg, up to 6 mg in 24 hours |
Parkinsonism, sedation |
|
Apathy |
|
Methylphenidate |
Start: 5 mg BID
|
Agitation, anxiety, insomnia, palpitations, tachycardia |
|
Sleep disturbance |
|
Melatonin
2nd line: Trazodone |
Melatonin 3-9 mg nightly
Trazadone 50 mg nightly |
Daytime drowsiness, sensory distortion, sleep walking |
|
Executive function deficits |
Consult Speech Therapy for cognitive evaluation |
Amantadine |
Start 100 mg BID
May increase in 50 mg increments weekly to max of 200 mg BID |
Headache, nausea, diarrhea, insomnia, orthostasis, psychosis at high doses |
|
Inattention |
Consult Speech Therapy for cognitive evaluation |
Methylphenidate |
Start: 5 mg BID, start >7-10 days post injury
|
Agitation, anxiety, insomnia, palpitations, tachycardia |
Appendix A: Agitated Behavior Scale where 22-28 is mild agitation, 29-35 is moderate agitation, and 36-56 is severe agitation.
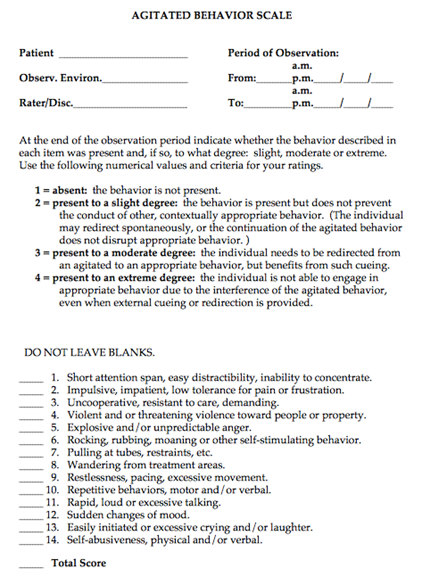
Appendix B: PHQ 9 where 1-4 is minimal depression, 5-9 is mild depression, 10-14 is moderate depression, 15-19 is moderately severe depression and 20-27 is severe depression
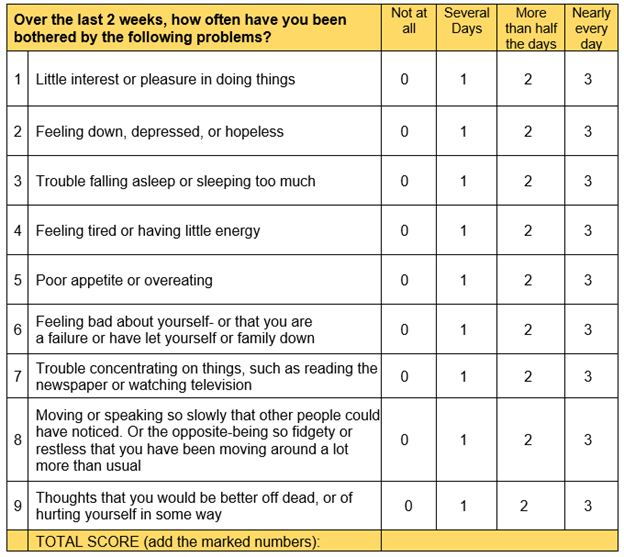
Appendix C: GAD-7 where 0-4 is minimal anxiety, 5-9 is mild anxiety, 10-14 is moderate anxiety, and 15-21 is severe anxiety
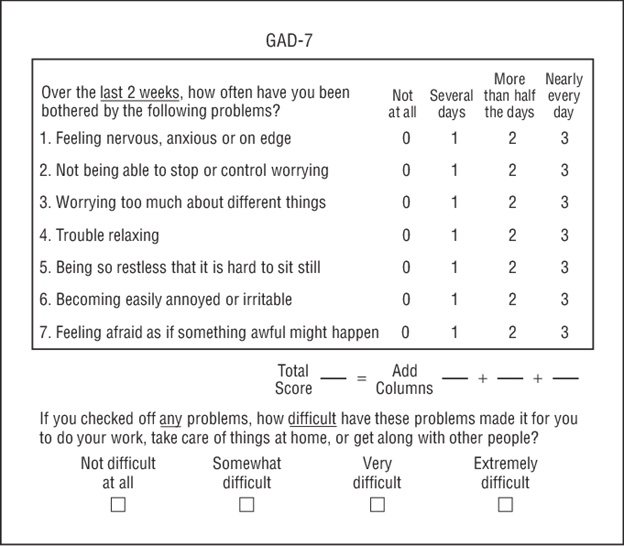
Appendix D: ITSS where PTSD is evaluated in items 3, 4, 7, 8, 9 and Depression is evaluated in items 1, 2, 3, 5, 6. If the sum of questions 1, 2, 3, 5, and 6 is equal to or greater than 2, the screen is positive for PTSD risk. If the sum of questions 3, 4, 7, 8 and 9 is equal to or greater than 2, the screen is positive for depression risk.
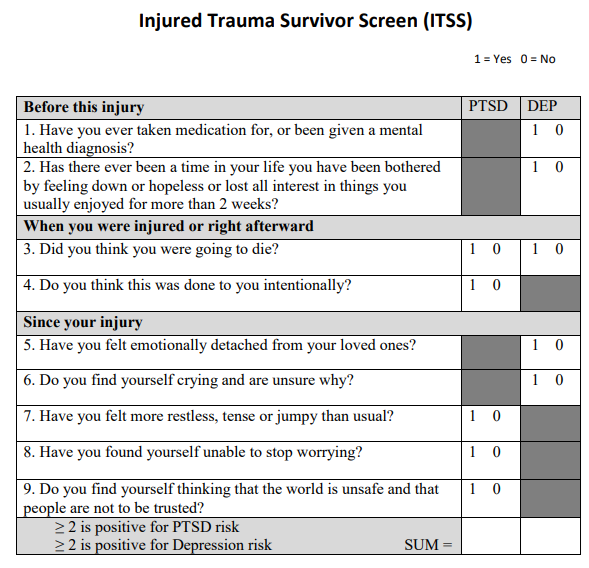
Authors:
Charity Evans, Abby Josef Trauma and Acute Care Surgery
Becca Sedlak, Pharmacy
Last Updated: January 2024
Initial Assessment and Management of Spine Injury
Purpose
To provide an evidence-based, practical guide to the evaluation and management of an adult patient with a spinal injury, including both spinal column fracture (SCF) and spinal cord injury (SCI).
Background/Definitions
Although fractures of the spine represent a small proportion of all fractures from traumatic injury overall (incidence ranging from 4-23 percent), their impact on the individual and the healthcare system is significant due to the potential for long-term disability, associated health care consequences and costs. Additionally, the incidence of traumatic spinal injuries is expected to increase globally as the population ages. Optimal outcomes are closely related to rapid identification of injuries, early surgical intervention when necessary and early mobilization.
Guideline Inclusion Criteria
Adult Trauma patients (15 yrs and older) with spinal column fracture (SCF) and/or spinal cord injury (SCI).
Guideline Exclusion Criteria
Pediatric trauma patients (Less than 15 yrs of age)
Diagnostic Evaluation
- All trauma patients should be initially evaluated per ATLS guidelines, independent of whether an SCF or SCI is suspected or confirmed.
- Cervical and thoracolumbar spinal motion restriction (SMR) should be maintained throughout this evaluation.
-
- DO NOT use force to move the patient’s neck or thoracolumbar spine into a position that elicits pain.
- Perform examinations of the spine by log rolling the patient when necessary.
-
- Examination of the cervical, thoracic, lumbar and sacral spine should include the following:
-
- Gross inspection for abrasions, contusions, hematomas, open wounds, and obvious spinal deformities.
- Systematically palpate the entire spine to evaluate for pain, tenderness, step offs, gaps or any other deformities.
- When a SCI is suspected, perform a digital rectal exam (DRE) before rolling the patient back to the supine position.
- NOTE: physical examination of the spine has low sensitivity for injury. Level of pain and/or tenderness often do not correlate with level of injury on imaging. A normal exam has low sensitivity in ruling out spinal injuries.
-
- Imaging of the spine should be obtained in any patient that has new/acute pain on examination or new neurologic deficit following a traumatic event.
- Imaging of the spine should be considered in trauma patients who present with severe injuries at high risk for associated spinal trauma including traumatic brain injury (TBI), complex maxillofacial trauma, pelvic fractures, thoracic trauma, calcaneal fractures resulting from fall from height, and presence of seat-belt sign. Imaging the spine should also be considered with certain mechanisms of injury including high speed motor vehicle collisions (especially when associated with ejection or roll over), motorcycle/bicycle/ATV or UTV collisions, crush injuries, falls from height, or injuries leading to an axial load on the head (e.g. diving and peds vs auto).
- Age by itself, is considered a high-risk factor for spinal trauma and spinal imaging should be taken into consideration even after low-energy mechanisms such as ground level falls.
- Computed tomography (CT) of the cervical, thoracic, and lumbar spine is the preferred initial imaging modality.
Practice Recommendations for Management
- Once spine fracture is identified on imaging or if acute neurologic deficit present/SCI suspected, consult the appropriate spine surgery service (Orthopedic Spine or Neurosurgery Spine) based on call schedule.
-
- EXCEPTION: 3 or fewer isolated and unilateral transverse or spinous process fractures located in the thoracolumbar spine DO NOT require a spine consult
-
- Spine service will evaluate patient and address the following issues (if able) in consultation note:
-
- Fractures present
-
- Stable vs unstable
-
- Spinal cord injury present
-
- Level/ASIA grade
- Blood pressure goals and length of goals
- Other specific concerns (i.e. presence of epidural hematoma, etc)
-
- Frequency of neurological exams
- Additional imaging
- Injury operative or non-operative
- Need for brace/what type of brace
- Activity restrictions (i.e. maintain full spine precautions, OK for HOB 30 deg, OK for activity in brace, etc)
- Recommendations regarding initiation of DVT prophylaxis
- Attending surgeon staffing consult
- Fractures present
-
- Operative vs non-operative management of SCF will be at the discretion of the consulting spine service and based on patient exam and fracture pattern/stability.
- On admission:
-
- Patient should be initiated on a multi-modality pain regimen to include the following (if not contraindicated):
-
- Acetaminophen 1000 mg q 8 hrs
- Calcitonin 200 IU per day intranasally
- Lidocaine 5% patch to affected area for 12 hrs
- Cyclobenzaprine 10 mg q 8 hrs (avoid in elderly)
- Oxycodone (avoid in elderly)
- Ibuprofen 800 mg q 8 hrs
- Gabapentin 300 mg q 8 hrs
-
- Activity orders
- Appropriate bracing should be ordered.
- Additional consults: physical therapy (PT), occupational therapy (OT)
-
- Consider speech consult in patients with cervical fractures and complaints of dysphonia or dysphagia
- PM&R consult for patients with SCI
-
- Patient should be initiated on a multi-modality pain regimen to include the following (if not contraindicated):
-
- Non-operative spine fractures:
-
- Within 24 hrs of admission:
-
- Appropriate brace delivered to bedside
- Ambulate with nursing staff and/or physical therapy (if not on full spine precautions or limited by concomitant injuries)
- Upright X-rays or additional imaging ordered and obtained.
-
- Once upright X-rays obtained, contact the appropriate spine service for interpretation and additional recommendations.
- Spine service will provide interpretation and additional recommendations within 6hrs of being notified x-rays are complete.
- If upright x-rays are unable to be obtained within 48 hrs of admission, notify spine service and discuss alternatives.
-
-
- 24-48 hrs of admission:
-
- PT/OT evaluations completed with disposition recommendations.
- Social work and case management engaged in disposition and discharge planning.
-
- Within 24 hrs of admission:
-
- Operative spine fractures:
-
- Surgical decompression or stabilization of SCF will ideally be performed within 72 hrs of admission in attempt to optimize outcomes and minimize morbidity related to delayed operative intervention.
-
- If patient unable to undergo recommended operative intervention within 72 hours, document why (i.e. patient factors, OR availability, surgeon availability).
-
- Within 24 hrs post-operatively:
-
- Appropriate brace delivered to bedside (if required)
- Ambulate with nursing staff and/or physical therapy
- Upright X-rays or additional imaging ordered and obtained.
-
- Once upright X-rays obtained, contact the appropriate spine service for interpretation and additional recommendations.
- Spine service will provide interpretation and additional recommendations within 6hrs of being notified x-rays are complete.
-
-
- 24-48 hrs post-operatively:
-
- PT/OT evaluations completed with disposition recommendations.
- Social work and case management engaged in disposition and discharge planning.
-
- Surgical decompression or stabilization of SCF will ideally be performed within 72 hrs of admission in attempt to optimize outcomes and minimize morbidity related to delayed operative intervention.
-
Follow-up Care
· Patients with SCF and/or SCI will follow-up at the discretion of the consulting spine service in the post-hospital setting.
Outcome Measures and Guideline Adherence
- All trauma patients with SCF and/or SCI experiencing a complication will be reviewed by our Trauma PI team for compliance with spinal injury guidelines.
- 6 months following implementation of guidelines, timing to OR for operative spinal injuries and length of stay will be reviewed for compliance and opportunities for improvement.
Related Policies
Cervical spine clearance
Key Contributors
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty
- Charity Evans, MD | Division of Acute Care Surgery, Faculty
- Daniel Surdell, MD | Department of Neurosurgery, Faculty
- Miki Katzir, MD | Department of Neurosurgery, Faculty
- Jamie Wilson, MD | Department of Neurosurgery, Faculty
- Scott Vincent, MD | Department of Orthopedic Surgery, Faculty
Last Updated
March, 2024
References
1. American College of Surgeons. Trauma Quality Improvement Program Spine Injury Best Practice Guidelines. spine_injury_guidelines.pdf (facs.org)
Transverse and Spinous Process Fractures
Background:
The majority of transverse process (TP) and spinous process (SP) fractures are structurally and neurologically stable injuries, which do not require spine service intervention. However there are some features which can be more worrisome for associated spinal cord and/or ligamentous involvement. Transverse process fractures are defined as those involving the transverse process only, without extension into the pedicle, lamina, or facet complex. The spinous process serves to attach muscles and ligaments, which are therefore at risk for injury in the presence of an SP fracture. We sought to create inclusion criteria to ensure that consistent spine consultation is obtained for the most high risk of these generally low-risk, stable fractures.
Guidelines for medical decision-making:
Trauma patients will receive imaging per usual protocol at the discretion of the treating team. TP and/or SP fractures may be identified on CT scan. If present, the following are indications for a spine consult:
· 4 or more contiguous TP fractures / SP fractures
· Bilateral TP fractures / SP fractures (regardless of the # of fractures)
· All C-spine TP fractures / SP fractures
Additionally, Spine consultation is required for ANY fracture (including TP and SP) when a concern for ligamentous injury exists.
Key contributors:
Abby Josef, Trauma
Reviewed by: Jamie Wilson, Neurosurgery and Scott Vincent, Ortho Spine
Version Date:
January 2024
References:
A. Homnick et al. Isolated thoracolumbar transverse process fractures: call physical therapy, not spine. J Trauma. (2007)
L.H. Bradley et al. Isolated transverse process fractures: spine service management not needed. J Trauma (2008)
J. H. Boulter et al. Implications of isolated Transverse Process fractures: Is spine service consultation necessary? World Neurosurgery (2016)
Care of Patients with Spinal Cord Injuries Practice Guideline
Purpose: To optimize the care of the spinal cord injured patient and prevent secondary complications.
Admission: All traumatic SCI patients will be admitted to ICU level of care with either Neurosurgery or Ortho Spine consult.
Spine Stabilization:
1. Patients with SCI should have unstable spinal injuries stabilized as early as possible, goal is within 24-48 hours post injury.
2. Optimize other injuries in multisystem injured patients with SCI to facilitate early spinal surgical stabilization.
3. Patients with SCI should be on bedrest until cleared by Neurosurgery/Ortho Spine. Once spinal injury is stabilized, activity should be liberated.
|
|
Phase 1: ICU |
Phase 2: Step-down or Floor |
|
Neurological |
· Neuro assessments per unit protocol. · Additionally, a neuro assessment should be performed and documented by nursing after any transfer (to new bed, new room, any procedure, etc). · Provider should be immediately notified of any changes in neuro exam. |
· Follow phase 1. |
|
Pain/Spasticity
|
· Assess pain per unit protocol. · Initiate multimodal pain regimen. Neuropathic Pain: · Pregabalin 75mg po q12h (can increase to 150 mg q12h at one week if needed) (reduce dosage if creatinine clearance is < 60mL/min) OR · Gabapentin 300 mg po q8h; > 65 years, 100 mg q8h (max 3600mg/day) · Consult pharmacy for titration. Should be weaned off over 1-2 weeks before discontinuing. · Initiate medication soon after injury. Spasticity: · Baclofen 10mg PO TID (max 120mg/day). · If minimal response to Baclofen, start Dantrolene 25mg PO Q 24 hrs; may titrate every 7 days to max of 400mg/day. Monitor LFTs weekly while actively titrating Dantrolene. Muscle Spasms: · Carisoprodol 350 mg po q6h PRN OR · Cyclobenzaprine 10 mg po q8h PRN |
|
|
Respiratory
|
All Patients: · Monitoring: Continuous pulse oximetry & EtCO2 for 7-10 days in patients with high cord injury and/or risk of respiratory compromise. Assess neurological level of injury daily. · For high cervical spine injuries (C6 and above): Consider daily ABG for 1-2 weeks post injury, with indications for escalation of respiratory support (including intubation) if PaO2 < 50 or PaCO2 > 50 on room air. · Consider monitoring with serial determination of the vital capacity, FEV1, the peak expiratory flow rate, the negative inspiratory force (NIF). If declining trend, order CXR and ABG with considerations as above. · Pts with weak cough, initiate manually assisted coughing (quad cough) Q 4 hrs. · Implement strict oral cares routine: every 2-4hrs and prn for intubated or unconscious patients; all other patients at minimum once per shift. Non-Intubated: · Incentive spirometry (IS) Q 1hr while awake. Nursing to document volume achieved. · If achieved IS volume < 50% predicted, consult Respiratory Therapy (RT) for lung volume expansion. RT Consult in all C spine and upper thoracic injuries- Pulmonary function test + possible addition of oscillatory positive expiratory pressure (OPEP), chest percussion therapy (CPT). Assisted Cough, IPV
Intubated: · In adults: Implement adult ventilator management EPIC order set which includes VAP bundle and ventilator weaning protocol. · Assess need for respiratory suctioning frequently to avoid mucous plugging. · Consider higher tidal volumes (TV) of 10-15 cc/kg to resolve or prevent atelectasis, if no contraindications. · Consider early tracheostomy who are likely to remain ventilator dependent or to wean slowly from mechanical ventilation. (<7 days) · Consult Speech Therapy (ST) to start Passy Muir Valve (PMV) trials · If not unable to tolerate or inappropriate for PMV, consult ST for alternate communication methods. · Consider downsizing trach as early as possible. Secretions: · Consider bronchoscopy. · 3% saline nebulized Q 8 hrs. · Add Guaifenesin · Consult RT for possible addition of oscillatory positive expiratory pressure (OPEP), chest percussion therapy (CPT), cough assist, IPV |
· Follow phase 1 non-intubated patient. Trach: · Consider larger TV (see phase 1 for parameters). · If remains on ventilator, continue weaning per protocol. · If not completed in phase 1, consult ST for PMV and/or alternate communication methods. Secretions: · Same as phase 1. · Discontinue therapies when secretions become thin. |
|
Cardiac |
· Vital signs per unit protocol. · Prevent and treat hypotension. Hypotension: · MAP Goal ≥ 80 x minimum 3-7 days (per Spine consult recommendations) from injury for ASIA A-D injuries. · Utilize Norepinephrine as first line agent. · Place arterial line for accurate hemodynamic monitoring. · Obtain central access if utilizing vasopressors. · If persistent vasopressor requirement > 3 days: Consider Midodrine 5 mg po q8h, titrate up to 40 mg/day. · Apply TED hose and /or ACE wraps to bilateral extremities when getting out of bed to chair, remove once back in bed. Bradycardia: · Assess for presence of mucus plugs (most common cause of acute bradycardia). · Order Atropine 0.5mg IV q1h prn for HR < 40 and have available at bedside. If persistent symptoms of bradycardia: · Start Robinul 0.1-0.2 mg IV or 1-2 mg po q8h to q12h. · Consider external or temporary pacemaker to maintain HR > 60. · If pacing required, consult cardiology. |
Hypotension: · Must be weaned off vasopressors prior to transfer out of ICU. · Continue or initiate Midodrine doses from phase 1 if needed. · Monitor for need or wean dose as tolerates. · Continue TED hose and/or ACE wraps from phase 1 when out of bed. Bradycardia: · Follow phase 1. |
|
Gastrointestinal |
· Gastrointestinal assessment per unit protocol. Monitor for nausea, vomiting, signs and symptoms of an ileus. Monitor for incontinence. · Initiate bowel regimen on admission. · Nursing to notify provider if patient goes more than a day without BM Stress Ulcer Prophylaxis: · Initiate and continue while patient remains ventilated. · Discontinue once patient off ventilator and tolerating goal tube feeds or regular diet x 48 hrs. Bowel Care (Prevent and Treat Constipation): · Initial upper motor neuron (UMN) regimen: Colace 100 mg po tid, Senna 17.6 mg 8-12 hours prior to digital simulation (typically given at lunch for nighttime digital stimulation) and Dulcolax 10 mg per rectum given along with digital stimulation. · Lower motor neuron (LMN) and mixed UMN/LMN injury regimen: Metamucil and manual stool evacuation. · No large volume enemas scheduled or routine. · Once enteral feedings have begun, bowel care should be done consistently at the same time each day, regardless of involuntary stooling between scheduled bowel care. · Schedule Bowel Routine: Dulcolax suppository at the same time daily with digital/manual stimulation. Discontinue only if excessive diarrhea. · Digital/Manual stimulation: Position patient left side down. Always use lubricant for comfort and to prevent autonomic dysreflexia. Should be done with scheduled Dulcolax suppository. · No BM by 72 hrs of admission: Check for impaction by positioning left side down. No impaction then increase Dulcolax to Q 12 hrs and start Lactulose 20grams PO Q 12 hrs until first BM. Diarrhea (liquid >500cc every Q 8 hrs or > 3 stools/day for 2 days): · Hold bowel regimen. · Start Metamucil 1 packet PO Q 12 hrs · Start Nutrisource Fiber 1 packet TID PO prn. · Consider checking stool for C.Difficile Toxin. |
· Follow phase 1. · Cervical level SCI requires 4 weeks of GI ppx |
|
Nutrition
|
· Consult Speech Therapy for swallow evaluation prior to initiating any oral intake in any SCI patient with cervical spinal cord injury, prolonged intubation, tracheostomy, halo fixation, or after any cervical spine surgery. · Obtain feeding access and initiate enteral support within 48 hrs of injury if no evidence of ongoing shock or hypoperfusion and off IV vasopressors. · Nutrition consult for assessment of calorie and protein needs. Also to provide nutrition support recommendations. · Once full estimated needs are being consistently provided consider ordering indirect calorimetry and/or 24 hour urine urea nitrogen to determine adequacy of nutrition. · Order calorie count when transitioning patient off enteral nutrition to oral intake to assist with titration. · Obtain prealbumin, CBC, CMP, folate and vitamin B12 every Sunday. · Maintain normoglycemia. |
· Follow phase 1 - continue current diet orders. · Nutrition to continue to monitor/intervene as per consult. · Transition to oral diet, if not on one, once patient passes ST swallow evaluation. |
|
Genitourinary |
· Genitourinary assessment per unit protocol. · Place indwelling catheter unless contraindicated, catheter cares per policy. · Remove indwelling catheter once patient is hemodynamically stable and no longer needs strict I&Os – then assess for volitional bladder control.
For patients without volitional bladder control: · Once Foley is removed: STRICT q4h straight cath & 2L fluid restriction. · If volumes are consistently less than 400 mL, can stop fluid restriction and go to q6h straight cath schedule. · Nursing or OT to teach self-cath technique. · Once patient is on the floor, closely follow ins/outs to ensure cath schedule is followed.
For patients with some volitional bladder control: · Check PVR after emptying bladder to assess need for above regimen.
For all patients: · Outpatient urodynamic evaluation with Urology to be scheduled 3 months following injury. |
· Follow phase 1. Work towards schedule for time straight caths. · Encourage moderate fluid intake spaced out throughout day to facilitate timed straight caths.
|
|
Integumentary
|
· Skin checks Q shift, pay close attention to bony prominences and under medical devices. · Give extra caution when assessing darker skin complexions as early signs of pressure injuries can go unnoticed. · If wound or skin concern identified, notify primary team and consult wound care per protocol. · Reposition pt at least every Q 2 hrs while maintaining spinal precautions (this includes all SCI pts –pre & post spine fixation, halo traction). · Position wedges above & below bony prominences to offload pressure. · Order and utilize TAPS turning system. · Patient with c-spine injury must be turned WITH wedges, not pillows to at 30+ degrees. Side lying preferred. · Sand beds for c-spine patients. Consider for high T-spine injury or patients with BUE weight bearing restrictions and consult with PT/OT. · Place on low air loss mattress. · Avoid friction, shearing, moisture and heat. Keep areas under patient clean and dry. · Implement pressure injury prevention skin bundle. · Consider placing Mepilex sacral dressing to coccyx/sacrum. · Order PRAFO and Prevalon boots. Alternating between the two Q 2 hrs. · Incision and drain wound care per orders. · Maintain normothermia. |
· Follow phase 1. · Consider specialty bed for floor · Order ROHO or GeoMatt cushion for wheelchair, utilize any time pt out of bed in chair. |
|
Mobility & Rehab |
· Consult physical therapy (PT) and occupational therapy (OT) for evaluate and treat. (should be seen within the first week, even if sedated/intubated) · Consult PM&R. · For cervical spine injuries, continue c-collar at all times. · Utilize brace, if ordered, when HOB > 30° and out of bed (confirm with neurosurgery). · Splinting should be considered for all patients at risk of contracture. · Let fingers flex passively and DO NOT overextend. This can cause loss stretch-induced paresis. · Sip and puff call light if pancake call light isn’t sufficient. Can consult OT for assistance with hydration system. · Consult SLP for communication needs (eye gaze system, etc.) · Early and aggressive mobilization. Head of Bed: · A gradual increase in HOB elevation, beginning at 15–30 degrees and advancing to 45 degrees or higher as tolerated, to promote upright tolerance and reduce the risk of orthostatic hypotension. · Unstable spinal injury requiring surgical fixation: Do not elevate HOB. Keep patient in reverse Trendelenburg unless contraindicated. · Stable fractures or post spinal fixation: HOB should remain elevated to at least 30° unless contraindicated. Activity: · Unstable spinal injury requiring surgical fixation, bedrest until fixation occurs. · Once spinal stabilization has occurred, discontinue bedrest order and place activity order. · Passive ROM should be performed daily for all major joints to prevent contractures. Active ROM when able. · Assess patient with the Bedside Mobility Assessment Tool before initiation of out of bed mobility. · Goal: Out of bed to chair or wheelchair Q 12 hrs once medical and spinal stability has been achieved. · For best practice, while in chair recline pt every 30 mins for 2 minutes or every 15 mins for 1 minute to achieve pressure relief then return to full upright position. · Consider utilizing ROHO or GeoMatt cushion when in chair or wheelchair. |
· Follow phase 1, continue to increase activity as tolerates. · PT/OT to assess need for orthotics of UE/LE. |
|
VTE Prophylaxis
|
· Pneumatic compression +/- Graduated compression stockings- ASAP when no LE injury C/I. Order SCDs, to be worn while in bed or sitting. (Including children of all ages) · No routine DVT screening. · Consider IVC filter if delay in starting chemical prophylaxis; otherwise no routine IVC filter placement. Chemical VTE prophylaxis · First line acute phase – Lovenox 30 mg BID. Recommendation against Heparin unless LMWH not available or contraindicated Timing of initiation · Stable spinal injury requiring no surgical fixation: Initiate Lovenox 30mg BID 24 hr. after admission. · Unstable spinal injury requiring surgical fixation: Start DVT PPX 24 hrs. post injury, if no other C/I and there is delay in OR for spine fixation. Hold morning dose on the day of surgery. · Unstable spinal injury post spinal fixation: <48 hrs. (as early as 24 hrs. post is safe) after surgery initiate Lovenox 40mg Q daily for 5 or 7 days then can transition to Lovenox 30mg BID dosing. (Check with Surgeon) · For patients with renal dysfunction, utilize Heparin 8000u SQ Q 8hrs. · Continue chemical prophylaxis for at least 8 weeks post injury in patients with limited mobility. Consider longer duration in motor complete injuries, lower-extremity fractures, older age, previous VTE, cancer, and obesity · Rehab phase – LMWH preferred, other options warfarin (INR 2-3) or DOAC. · Chemical VTE prophylaxis should be held prior to drain removal post-surgical fixation. Neurosurgery or Ortho spine to place this hold order. |
· Continue SCDs and chemical DVT prophylaxis. |
|
Psychosocial |
· Consult psychology. · Assess for depression. · Foster effective coping strategies. · Utilize assistive devices including specialty call lights and communication boards. · Identify, educate, and support family/caregivers. · For pediatric patients or patients with children or younger siblings consult child life. |
· Follow phase 1. |
|
Discharge Planning |
· Communicate early with care transitions to determine disposition options. · Consult social work to facilitate placement. |
· Continue discharge planning. |
|
Education |
· Begin teaching family and/or family/caregiver cares early on in stay once patient medically stable. Respiratory: How to manually assist coughing. Trach – suctioning and trach cares.
Cardiac: How to apply TED hose or ACE wraps prior to getting patient out of bed.
GI: Importance of bowel care schedule and how to manually stimulate.
GU: How to preform clean straight caths and catheter cares.
Integumentary: Importance of maintaining skin integrity and frequent assessments of skin.
Autonomic Dysreflexia (typically develops a few months post-SCI): Signs and symptoms, causes, prevention and treatment. |
· Continue to follow phase 1. Reinforce education and practice. |
Keely Buesing, MD, Trauma & Acute Care Surgery
Dan Pierce, MD, Physical Medicine & Rehabilitation
January 2026
References:
1. Beom, J., & Seo, H. (2018). The need for early tracheostomy in patients with traumatic cervical cord injury. Clinics in Orthopedic Surgery, 10(2), 191-196. doi: 10.4055/cios.2018.10.2.191
2. Cabahug, P., Pickard, C., Edmiston, T., & Lieberman, J. A. (2020). A Primary Care Provider's Guide to Spasticity Management in Spinal Cord Injury. Topics in spinal cord injury rehabilitation, 26(3), 157–165. https://doi.org/10.46292/sci2603-157
3. Consortium for Spinal Cord Medicine. (2008). Early acute management in adults with spinal cord injury: a clinical practice guideline for health-care professionals. Journal of Spinal Cord Medicine, 31(4), 403-479. doi: 10.1043/1079-0268-31.4.408
4. Dhall, S, Hadley, M., Aarabi, B., Gelb, D., Hurlbert, J., Rozzelle, C., Ryken, T., Theodore, N. & Walters, B. (2013). Deep venous thrombosis and thromboembolism in patients with cervical spinal cord injuries. Neurosurgery, 72, 244-254. doi: 10.1227/NEU.0b013e31827728c0
5. Fehlings, M., Tetreault, L., Wilson, J., Aarabi, B., Anderson, P., Arnold, P., Brodke, D., Burns, A., Chiba, K., Dettori, J., Furlan, J., Hawryluk, G., Holly, L., Howley, S., Jeji, T., Kalsi-Ryan, S., Kotter, M., Kurpad, S., Marino, R., …Harrop, J. (2017). A clinical practice guideline for the management of patients with acute spinal cord injury and central cord syndrome: Recommendations on the time (≤ 24 hours versus > 24 hours) of decompressive surgery. Global Spine Journal, 7, 195S-202S. doi: 10.1177/2192568217706367.
6. Groah, S., Schladen, M., Pineda, C., & Hsieh, C. (2015). Prevention of pressure ulcers among people with spinal cord injury: A systematic review. PM&R: The Journal of injury, function, and rehabilitation, 7(6), 613-636. doi: 10.1016/j.pmrj.2014.11.014
7. Liu, Y., Xu, H., Liu, F., Lv, Z., Kan, S., Ning, G., & Feng, S. (2017). Meta-analysis of heparin therapy for preventing venous thromboembolism in acute spinal cord injury. International Journal of Surgery, 43, 94-100. doi: 10.1016/j.ijsu.2017.05.066
8. Saadeh, Y., Smith, B., Joseph, J., Jaffer, S., Buckingham, M., Oppenlander, M., Szerlip, N., & Park, P. (2017). The impact of blood pressure management after spinal cord injury: a systematic review of the literature. Journal of Neurosurgery, 43(5), 1-7. https://doi.org/10.3171/2017.8.FOCUS17428
9. Sabit, B., Zeiler, F., & Berrington, N. (2018). The impact of mean arterial pressure on functional outcome post trauma-related acute spinal cord injury: A scoping systematic review of human literature. Journal of Intensive Care Medicine, 33(1), 3-15. doi: 10.1177/0885066616672643.
10. Stein, D., & Knight, W. (2017). Emergency neurological life support: Traumatic spine injury. Neurocritical Care, 27, 170-180. doi: 10.1007/s12028-017-0462-z.
11. Walters, B., Hadely, M., Hurlbert, R., Aarabi, B., Dhall, S., Gelb, D., Harrigan, M., Rozelle, C., Ryken, T., & Theodore, N. (2013). Guidelines for the management of acute cervical spine and spinal cord injuries: 2013 update. Neurosurgery, 60, 82-91. doi: 10.1227/01.neu.0000430319.32247.7f.
12. Zakrasek, E., Nielson, J., Kosarchuk, J., Crew, J., Ferguson, A. & McKenna, S. (2017). Pulmonary outcomes following specialized respiratory management for acute cervical spinal cord injury: a retrospective analysis. Spinal Cord, 55(6), 559-565. doi: 10.1038/sc.2017.10
4. Head and Neck Trauma
Educational materials and pathways regarding the evaluation and management of head and neck injuries.
5. Thoracic Trauma
Educational materials and pathways regarding the evaluation and management of thoracic injuries.
Care of Patients with Rib Fractures
Purpose
Rib fractures occur in approximately 10% of patients with traumatic injury. They are associated with greater injury burden especially when coupled with head, extremity, abdominal and blunt cardiac injury. Mortality rates increase with the number of fractured ribs (5.8% for a single rib to 34.4% mortality with 8 or more rib fractures). Flail chest and pulmonary contusion also increase mortality. Rib fractures are associated with multiple pulmonary complications including pneumonia, adult respiratory distress syndrome (ARDS) and pneumothorax. Rib fractures are also associated with an increased ICU length of stay (LOS), hospital LOS, and ventilator days. The purpose of this guideline is to standardize our approach to the management of traumatic rib fractures.
Admission Criteria:
Admit to unit based on age, injury burden, degree of pulmonary compromise, comorbidities, and trauma attending discretion.
- Consider admission to ICU if:
-
- mechanical ventilation
- age > 60 yrs
- 4 or more rib fractures
- lung parenchymal abnormality or contusion
- flail segment
- volume expansion protocol needed more frequently than every 2 hours
- incentive spirometry <1000 cc.
- COPD, home O2 use, current tobacco user, current antiplatelet use
-
- Consider admission to STEP DOWN Unit if:
-
- <3 rib fractures
- age >45 yrs with rib fractures and flail segment or sternal fracture
- O2 requirement greater than or equal to 5L nasal canula
- volume expansion protocol needed every 2-3 hrs
- incentive spirometry 1000-1500 cc
-
- Consider admission to FLOOR if:
-
- pain control is adequate
- incentive spirometry >1500 cc
-
Initial Management:
- Consult to respiratory therapy for "Lung Volume Expansion" (if no pneumothorax)
- Continous pulse oximetry
- Incentive spirometry for 10 times/hr while awake
- Supplemental oxygen as needed to maintain SpO2>90% (or >88% in patients with known history of COPD).
- Chest X-ray (portable) every morning x 3 days (+/1 days based on clinical judgement)
- Physical therapy consult for early mobilization. When cleared, patient should ambulate 3x daily at minimum.
- Judicious use of intravenous fluids. Avoid boluses if possible and, if boluses are indicated, utilize small boluses. If unresponsive to 2 boluses, notify trauma attending.
- Multimodality pain management:
-
- PCA or hourly PRN IV pain medication
- Consult APS for epidural or paravertebral block if not contraindicated.
-
- contraindications for an epidural include: platelets <80K, infection at site of insertion, epidural or spinal cord hematoma, INR >1.2, prophylactic LMWH within 12 hrs or therapeutic dose within 24 hrs, hemodynamic instability.
- contraindications to a paravertebral block include: platelets <80k, infection at site of insertion, INR <1.5, transverse process fractures in proximity to level of insertion.
-
- Lidocaine patch over rib fractures
- Tylenol 1000 mg PO every 6 hrs scheduled + Flexeril 10 mg PO every 8 hrs scheduled + Oxycodone immediate release 5-15mg PO every 4 hrs as needed (PRN).
- Add ibuprofen 800 mg PO every 8 hrs scheduled if not contraindicated due to age, renal function, or bleeding risk; strongly consider a COX-2 inhibitor if ibuprofen is contraindicated.
-
Non-invasive mechanical ventilation (BiPAP or CPAP):
Should only be used if the patient is normally on this treatment prior to injury.
- BiPAP/CPAP is rarely appropriate for patients with chest injuries and progressive respiratory distress. Early intubation in these patients is more appropriate.
- BiPAP should be used for reversible ventilation issues such as hypercarbia, COPD exacerbation, and/or pulmonary edema.
- BiPAP is a bridge to all time for interventions (e.g. Lasix administration for volume overload) to be performed that may prevent intubation.
- BiPAP should only be used as a short term option, ideally no more than 6 hours.
- Monitor the patient closely while on BiPAP for further respiratory decline.
- If respiratory status does not improve within 6 hours or less, consider intubation.
Surgical Stabilization of Rib Fractures (Rib Plating):
Consider rib plating in the following clinical situations: (see Trauma Policy PRO06 Surgical Stabilization of Rib Fractures):
- Non-intubated patients with respiratory insufficiency due to pain despite continuous epidural/paravertebral anesthesia and use of multi-modality pain regimen.
- Intubated patients with flail chest who fail to wean from ventilator.
- Patients with extensive anterolateral flail chest and progressive displacement of fractured ribs.
- Patients who require thoracotomy due to associated intra-thoracic injury.
- Painful nonunion
- Patient complaints of painful movement of ribs (popping, clicking).
References
- Carver T, Milia D, Somberg C, Brasel K, Paul J. Vital capacity helps predict pulmonary complications after rib fractures. J Trauma Acute Care Surg. 2015;79(3):413-416.
- Chen J, Jeremitsky E, Philp R, Fry W, Smith R. A chest trauma scoring system to predict outcomes. J Surg. 2014;156(4): 988-994.
- Gonzalez K, Ghneim M, Kang F, Jupiter D, Davis M, Regner J. A pilot single-institution predictive model to guide rib fracture management in elderly patients. J Trauma Acute Care Surg. 2015; 78(5):970-975.
- Leininger S, Rib fracture protocol advancing the care of the elderly patient. Crit Care Nursing. 2017;40(1).
- Mastroianni S. Implementing a rib fracture management pathway and PIC scoring tool to reduce ICU readmissions. San Francisco, CA: University of San Francisco Scholarship Repository; May 22, 2015, Spring.
- Sahr S, Webb M, Hacket Renner C, Sokol R, Swegle J. Implementation of a rib fracture triage protocol in elderly trauma patients. J Trauma Nursing. 2013;20(4):172-175.
- Simon B, Ebert J, Bkhari F, Capella J, Emohoff T, Hayward T, Rodriguez A, Smith L. Management of pulmonary contusion and flail chest. An Eastern Association for the Surgery of Trauma practice management guidelines. J Trauma Acute Care Surg. 2012;73(5):S351-S361.
- Witt C, Bulger E. Comprehensive approach to the management of the patient with multiple rib fractures: A review and introduction of a bundled rib fracture management protocol. Trauma Surg and Acute Care Open. 2017;2(1): 1-7.
Author(s)
Trauma Leadership
Last Reviewed
July, 2017
Surgical Stabilization of Rib Fractures (SSRF or Rib Plating)
Purpose
Surgical Stabilization of rib fractures should be considered in patients with flail chest, flail sternum, and painful rib fractures associated with movement that have been refractory to conventional pain management in order to improve morbidity and mortality.
Indications
- Non-ventilated patients:
-
- Chest wall instability
-
- 3 or more segmental rib fractures (flail chest)
- 3 or more bi-cortically displaced/offset rib fractures
- clinical findings of paradoxical motion
- instability or "clicking" on palpation of chest wall or as reported by the patient
-
- 3 or more displaced rib fractures
-
- with displacement of >50% the rib width AND 2 or more pulmonary physiological derangements.
-
- Chest wall instability
-
- Ventilated patients:
-
- Chest wall instability
-
- 3 or more segmental rib fractures (flail chest)
- 3 or more bi-cortically displaced/offset rib fractures
- clinical findings of paradoxical motion
- instability or "clicking" on palpation of chest wall or as reported by the patient
-
- Failure to wean from ventilator
- Chest wall instability
-
Contraindications
- Absolute
-
- shock/ongoing resuscitation
- severe traumatic brain injury
- acute myocardial infarction
- fractures outside of ribs 3-10
-
- Relative
-
- Age <18 yrs
- Age >80 yrs
- unstable spine injury
- empyema
- history of chest wall radiation
- mild to moderate traumatic brain injury
-
Timing
- Non-ventilated patients
-
- when feasible, less than 24 hrs is optimal
- should be performed within 72 hours of injury
- SSRF should be delayed in the face of higher priority injuries
-
- Ventilated patients
-
- earliest feasible time for flail indication
- should be performed within 72 hrs of injury for non-flail indications.
- SSRF should be delayed in the face of higher priority injuries.
-
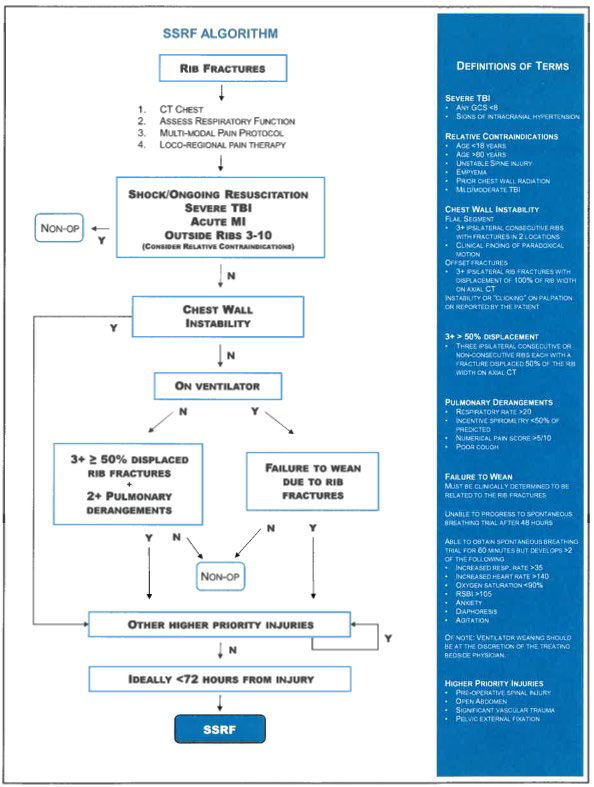
References
Author(s)
Zachary Bauman, DO
Last Updated
May, 2020
6. Abdominal Trauma
Educational materials and pathways regarding the evaluation and management of abdominal injuries.
Blunt Abdominal Trauma
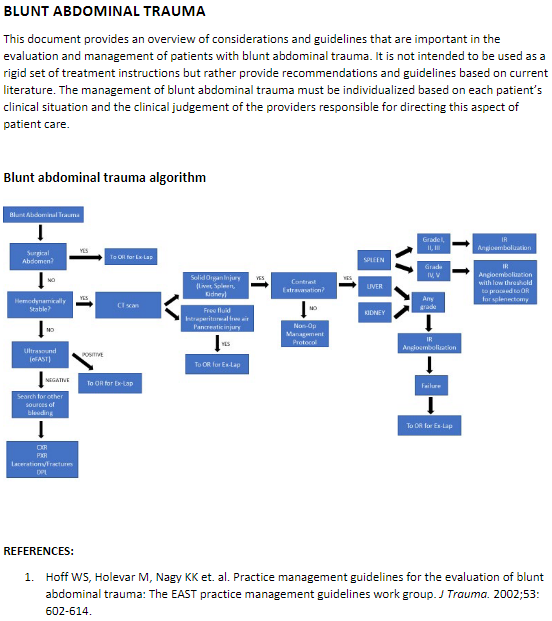
Evaluation and Management of Blunt Splenic Injury
Purpose
Splenic injury is one of the most common injuries following blunt abdominal trauma and can result in significant bleeding given the vascular nature of this organ. Unrecognized injury can be a cause of preventable death following trauma. The following guidelines outline the approach that should be taken when evaluating and managing a trauma patient with splenic injury and the decision-making process between operative and non-operative management.
Background/Definitions
During the last century, management of blunt splenic injury has shifted from observation/expectant management in the early 1900s to operative intervention for all injuries, to the current practice of selective operative and non-operative management of splenic injury. The current non-operative paradigm in adults was stimulated by the success of non-operative management of solid-organ injuries in hemodynamically stable children. The potential advantages of non-operative management include lower hospital cost, earlier discharge, avoiding nontherapeutic laparotomies (as well as associated cost and morbidity), fewer intra-abdominal complications, and reduced transfusion rates associated with an overall mortality of these injuries. While the non-operative approach to blunt splenic injury has been proven to work well in hemodynamically stable patients with lower grade injuries, there is still a role for operative and/or endovascular intervention in those patients who are hemodynamically unstable or those with higher grade injuries.
Splenic injuries are classified by a grading system established by the AAST (American Association for the Surgery of Trauma). In general, the higher the grade equals more severe injury and potential for associated morbidity and mortality.
AAST Splenic Injury Grading Scale

https://www.aast.org/resources-detail/injury-scoring-scale#spleen
Guideline Inclusion Criteria
- All trauma patients sustaining blunt abdominal trauma should be evaluated for potential splenic injury.
Guideline Exclusion Criteria
- Patients who no longer have a spleen.
- Pediatric patients <15 yrs age.
Diagnostic Evaluation
- All trauma patients should be initially evaluated per ATLS guidelines with work-up as mechanism and clinical presentation dictate.
- Resuscitative measures should be initiated as clinical status/presentation dictates.
- Labs, imaging and additional tests should be obtained as clinical status/presentation dictates.
- If a patient is hemodynamically UNSTABLE, minimal testing/imaging should occur prior to interventions for hemorrhage control.
Practice Recommendations for Management
- Once splenic injury is suspected and/or confirmed, management of that injury is dictated largely by the clinical status of the patient.
-
- If a patient is hemodynamically UNSTABLE:
-
- Initiate/continue resuscitative measures.
- Obtain an eFAST exam.
- If eFAST is positive, proceed to OR for surgical exploration.
-
- If a patient is hemodynamically STABLE:
-
- May continue with evaluation and work-up as mechanism and presentation dictate.
- Obtain imaging as indicated, including a multi-phase CT abd/pelvis with IV contrast
- Determine appropriate management strategy based on grade of injury, presence of blush/extravasation on imaging, and clinical status and injury burden of patient.
-
- If a patient is hemodynamically UNSTABLE:
-

603730a847af494fa170694b778b703a.pdf (cvent.com)
- Operative Management
-
- Should be used in all patients who are hemodynamically unstable or those with peritonitis on exam.
- Should be considered in patients who are transient responders to resuscitation or in those with injury burden (head injury) in which hypotension secondary to hemorrhagic shock would be detrimental.
- Operative plan should be exploratory laparotomy for trauma with splenectomy vs splenorrhaphy.
-
- Splenic salvage/splenorrhaphy may be considered in Grade I-II injuries depending on the clinical status of the patient.
- Splenectomy should be performed in Grade III-V injuries or in patients with ongoing bleeding.
-
-
- IR Angioembolization
-
- Should be considered in patients who are transient responders to resuscitation, those with evidence of active extravasation/blush on CT abd/pelvis, those with high grade injuries (Grade III-V) or those with injury burden (e.g. head injury) in which hypotension secondary to hemorrhagic shock would be detrimental.
-
- Non-operative Management
-
- Non-operative management of splenic injuries should ONLY be considered in hemodynamically stable patients.
- Patients undergoing non-operative management should be monitored closely for deterioration in clinical status suggestive of ongoing hemorrhage (i.e. failure of non-operative management) with vitals per unit protocol, serial labs, abdominal exams and repeat imaging as indicated.
- Bedrest is not routinely indicated for blunt splenic injuries that are managed non-operatively. In general, patients may be activity as tolerated unless bedrest is required for a concurrent injury or at trauma attending discretion.
- Admission level of care will be at the trauma attending’s discretion. In general, higher grade injuries (III, IV, V) should be initially monitored in the ICU or Step Down Unit and lower grade injuries (I, II) be initially monitored on the floor or Step Down Unit depending on clinical status and injury burden.
- Suggested non-operative management strategy is as follows:
-

603730a847af494fa170694b778b703a.pdf (cvent.com)
-
-
- Repeat imaging for splenic injuries managed non-operatively
-
- A repeat multi-phase CT abd/pelvis with IV contrast should be obtained for all Grade III or higher splenic injuries between 3-5 days post injury or prior to discharge to evaluate for development of post-traumatic pseudoaneurysms.
- If pseudoaneurysms are present, then IR should be consulted for consideration of splenic angioembolization.
-
- Repeat imaging for splenic injuries managed non-operatively
-
- Follow-up Care:
-
- Post splenectomy vaccines
-
- Patients undergoing splenectomy as management of their splenic injury should obtain the following vaccines prior to discharge or at 14 days post-op (whichever date comes first)
-
- Quadravalent meningococcus (Menactra or Menomune)
- Pneumococcus (Pneumovax 23)
- H.influenzae B (HIB, ActHIB)
- Viral influenza vaccine (depending on time of year)
-
- Patients undergoing splenic angioembolization do not routinely require vaccinations.
- Patients undergoing splenectomy as management of their splenic injury should obtain the following vaccines prior to discharge or at 14 days post-op (whichever date comes first)
-
- All patients with splenic injury should follow-up in trauma clinic 1-2 weeks following discharge pending clinical status at time of discharge and hospital length of stay following injury.
- Post splenectomy vaccines
-
Outcome Measures and Guideline Adherence
- Time to OR/IR and interventions for all hemodynamically unstable patients will be tracked through our performance improvement process/initiatives.
- Patients failing non-operative management (i.e. those requiring IR angioembolization or exploratory laparotomy in a delayed fashion) will be tracked through our performance improvement process/initiatives.
- Adherence to obtaining repeat imaging for Grade III or higher splenic injuries at post-injury day 3-5 and need for subsequent interventions will be assessed every 6 months.
Key Contributors
· Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
Last Updated
July, 2023
References
- Stassen NA, Bhullar I, Cheng JD, et. al. Selective nonoperative management of blunt splenic injury: An Eastern Association for the Surgery of Trauma practice management guidelines. J Trauma Acute Care Surg. 2012;73(5): S294-300.
- Rowell SE, Biffl WL, Brasel K, et. al. Western Trauma Association critical decisions in trauma: Management of adult blunt splenic trauma—2016 updates. J Trauma Acute Care Surg. 2016; 82(4): 787-93.
- Wallen TE, Clark K, Baucom MR, et al. Delayed splenic pseudoaneurysm identification with surveillance imaging. J Trauma Acute Care Surg. 2022;93(1):113-117.
- Freeman JJ, Yorkgitis BK, Haines K, et al. Vaccination after spleen embolization: A practice management guideline from the Eastern Association for the Surgery of Trauma. Injury. 2022;53(11):3569-3574.
Evaluation and Management of Hepatic Injury
Purpose
The liver is the most frequently injured abdominal organ. Most injuries are minor and can heal spontaneously without operative management. Unrecognized injury can be a cause of preventable death following trauma. The following guidelines outline the approach that should be taken when evaluating and managing a trauma patient with hepatic injury and the decision-making process between operative and non-operative management.
Background/Definitions
During the last century, the management of blunt force trauma to the liver has changed dramatically. A shift away from operative management has resulted in a decline in mortality. The current nonoperative paradigm in adults was encouraged by the success of nonoperative management of solid organ injuries in hemodynamically stable children. As early as 1960, Shaftan advocated “observant and expectant treatment” rather than mandatory laparotomy in the management of penetrating abdominal injury. This was reinforced in 1969 by Nance and Cohn for the management of abdominal stab wounds. The advantages of nonoperative management include lower hospital cost, earlier discharge, avoiding nontherapeutic laparotomies, fewer intra-abdominal complications, and reduced transfusion rates. Gunshot wounds to the abdomen, however, are still commonly treated with mandatory exploration because of multiple reports emphasizing a high incidence of intra-abdominal injuries and the complications of a missed injury or an injury delayed in recognition and treatment. Multiple studies and review of National Trauma database have demonstrated that only 13.7% of hepatic injuries are now managed operatively. Complications develop in 2.5 to 41% of all trauma patients undergoing unnecessary laparotomy, and small bowel obstruction, pneumothorax, ileus, wound infection, myocardial infarction, visceral injury, and even death have been reported secondary to unnecessary laparotomy. It is important to recognize the importance of different mechanisms of penetrating injury (stab versus gunshot versus shotgun wounds), the velocity of the agent (low versus high) as well as the different regions of the abdomen (intraperitoneal, retroperitoneal, and thoracoabdominal areas).
These issues were first addressed by the Eastern Association for the Surgery of Trauma (EAST) in the Practice Management Guidelines for Non-operative Management of Blunt Injury to the Liver and Spleen published online in 2003. The practice management guideline update was split into separate recommendations for the nonoperative management of blunt hepatic and splenic injuries in adult trauma patients, with the last set of guidelines being published in 2012 for blunt hepatic injuries and in 2010 for penetrating injuries.
Hepatic injuries are classified by a grading system established by the AAST (American Association for the Surgery of Trauma). In general, the higher the grade equals more severe injury and potential for associated morbidity and mortality.

https://www.aast.org/resources-detail/injury-scoring-scale#liver
Guideline Inclusion Criteria
- All trauma patients sustaining abdominal trauma should be evaluated for potential hepatic injury.
Guideline Exclusion Criteria
- Pediatric patients <15 yrs of age.
Diagnostic Evaluation
- All trauma patients should be initially evaluated per ATLS guidelines with work-up as mechanism and clinical presentation dictate.
- Resuscitative measures should be initiated as clinical status/presentation dictates.
- Labs, imaging and additional tests should be obtained as clinical status/presentation dictates.
- If a patient is hemodynamically UNSTABLE, minimal testing/imaging should occur prior to interventions for hemorrhage control.
Practice Recommendations for Management
- Once hepatic injury is suspected and/or confirmed, management of that injury is dictated largely by the clinical status of the patient.
-
-
- If a patient is hemodynamically UNSTABLE:
-
- Initiate/continue resuscitative measures.
- Obtain an eFAST exam.
- If eFAST is positive, proceed to OR for surgical exploration.
-
- If a patient is hemodynamically STABLE:
-
- May continue with evaluation and work-up as mechanism and presentation dictate.
- Obtain imaging as indicated, including a multi-phase CT abd/pelvis with IV contrast.
- Determine appropriate management strategy based on grade of injury, presence of blush/extravasation on imaging, and clinical status and injury burden of patient.
-
- If a patient is hemodynamically UNSTABLE:
-
- Operative Management
-
-
- Should be used in all patients who are hemodynamically unstable or those with peritonitis on exam.
- Should be considered in patients who are transient responders to resuscitation or in those with injury burden in which hypotension secondary to hemorrhagic shock would be detrimental.
- Operative plan should be exploratory laparotomy for trauma with consideration of cauterization, topical hemostatic agents, hepatorrhaphy or packing +/- endovascular procedures.
- Diagnostic laparoscopy may be considered as a tool to evaluate diaphragmatic lacerations as well as peritoneal penetration.
- In severe/high grade liver injuries, interventional radiology for angioembolization may also be considered for hemorrhage control in conjunction with operative interventions.
-
-
- IR Angioembolization
-
- Should be considered in patients who are transient responders to resuscitation, those with evidence of active extravasation/blush on CT abd/pelvis, those with high grade injuries (Grade III-V) or those with injury burden (e.g. head injury) in which hypotension secondary to hemorrhagic shock would be detrimental.
-
- Non-operative Management
-
- Non-operative management of hepatic injuries should ONLY be considered in hemodynamically stable patients.
- Patients with penetrating injury isolated to the right upper quadrant of the abdomen may be managed without laparotomy in the presence of stable vital signs, reliable examination and minimal to no abdominal tenderness.
- The severity of hepatic injury (as suggested by CT grade or degree of hemoperitoneum), neurologic status, age of more than 55 years, and/or the presence of associated injuries are not absolute contraindications to a trial of nonoperative management in a hemodynamically stable patient.
- Patients undergoing non-operative management should be monitored closely for deterioration in clinical status suggestive of ongoing hemorrhage (i.e. failure of non-operative management) with vitals per unit protocol, serial labs, abdominal exams and repeat imaging as indicated.
- Interventional modalities including endoscopic retrograde cholangiopancreatography (ERCP), angiography, laparoscopy, or percutaneous drainage may be required to manage complications (bile leak, biloma, bile peritonitis, bilious ascities, and hemobilia)
- Bedrest is not routinely indicated for blunt hepatic injuries that are managed non-operatively. In general, patients may be activity as tolerated unless bedrest is required for a concurrent injury or at trauma attending's discretion.
- Admission level of care will be at the trauma attending's discretion. In general, higher grade injuries (III, IV, V) should initially be monitored in the ICU or Step Down Unit and lower grade injuries (I, II) be initially monitored on the floor or Step Down Unit depending on the clinical status and injury burden of the patient.
- Suggested non-operative management strategy is as follows (Table 1):
-
Table1. Blunt Hepatic Injury Guidelines for Nonoperative and Postintervention Management

- Repeat imaging for hepatic injuries managed non-operatively
- Clinical factors such as a persistent systemic inflammatory response, increasing persistent abdominal pain, jaundice, or an otherwise unexplained drop in hemoglobin should prompt reevaluation by CT scan.
- A repeat multi-phase CT abd/pelvis with IV contrast should be obtained for all Grade III or higher blunt hepatic injuries between 3-5 days post injury or prior to discharge to evaluate for development of post-traumatic pseudoaneurysms, AV fistulas or biliary issues.
Figure 1. Western Trauma Association algorithm for the diagnosis and management of blunt hepatic injury in adults. Circled letters correspond to lettered section in the articles text. OR, operating room; IR, interventional radiology. (Keric N, Shatz DV, Schellenberg M, et al. Adult blunt hepatic injury: A Western Trauma Association critical decisions algorithm. J Trauma Acute Care Surg. 2024 Jan 1;96(1):123-128. Doi:10.1097/TA.0000000000004141. Epub 2023 Sep 25. PMID: 37747241)

Figure 2. Operative management of blunt hepatic injury in adults.

- Follow-up Care
-
- All patients with hepatic injury should follow-up in trauma clinic 1-2 weeks following discharge pending clinical status at time of discharge and hospital length of stay following injury.
-
Outcome Measures and Guideline Adhearance
- Time to OR/IR and interventions for all hemodynamically unstable patients will be tracked through our performance improvement process/initiatives.
- Patients failing non-operative management (i.e. those requiring IR angioembolization or exploratory laparotomy in a delayed fashion) will be tracked through our performance improvement process/initiatives.
Key Contributors
· Gina Lamb, MD | Division of Acute Care Surgery, Faculty | Principle Author
Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Author
Last Updated
February, 2024
References
- Tinkoff G, Esposito T, Reed J, et al. American Association for the Surgery of Trauma Organ Injury Scale I: spleen, liver, and kidney, validation based on the National Trauma Data Bank. J Am Coll Surg. 2008;207:646–655
- Como J, Bokhari F, et al. Practice Management Guidelines for Selective Nonoperative Management of Penetrating Abdominal Trauma. J Trauma. 2010;68: 721–733
- Stassen, N, Bhullar, I, et al. Nonoperative management of blunt hepatic injury. An Eastern Association for the Surgery of Trauma practice management guideline. Journal of Trauma and Acute Care Surgery 73(5):p S288-S293, November 2012.
- Wagner ML, Streit S, Makley AT, Pritts TA, Goodman MD. Hepatic Pseudoaneurysm Incidence After Liver Trauma, Journal of Surgical Research, Volume 256, 2020, Pages 623-628
- Keric N, Shatz DV, Schellenberg M, et al. Adult blunt hepatic injury: A Western Trauma Association critical decisions algorithm. J Trauma Acute Care Surg. 2024 Jan 1;96(1):123-128. Doi:10.1097/TA.0000000000004141. Epub 2023 Sep 25. PMID: 37747241
- Coccolini F, Coimbra R, Ordonez C, Kluger Y, et al. WSES expert panel. Liver trauma: WSES 2020 guidelines. World J Emerg Surg. 2020 Mar 30;15(1):24. doi: 10.1186/s13017-020-00302-7. PMID: 32228707; PMCID: PMC7106618
7. Orthopedic Trauma
Educational materials and pathways regarding the evaluation and management of orthopedic injuries.
Antibiotic Prophylaxis in Open Fractures
BACKGROUND
Open fractures are high energy injuries with an increased risk of infection due to potential exposure of bone and deep tissue to a variety of environmental debris. Infection can lead to serious complications including nonunion of wounds and osteomyelitis.
DEFINITIONS
The Gustilo-Anderson classification system is the most commonly used grading system for open fractures. Fractures are designated as one of three types based on wound size, soft tissue involvement, contamination, and fracture pattern.
Table 1: Gustilo-Anderson Classification System
| Type I fracture | Open fracture with clean wound <1 cm long |
| Type II fracture | Open fracture with laceration >1 cm long without extensive soft tissue damage |
| Type III fracture | Open segmental fracture, open fracture with extensive soft tissue damage, or traumatic amputation |
BETA-LACTAM ALLERGY MANAGEMENT: Cefazolin is a safe option in patients with documented penicillin allergies due to its unique structural characteristics. Cross reactivity between PCN and advanced generation cephalosporins is also very rare. These agents (ceftriaxone) are generally considered safe for patients with distant (>10 years) or non-severe reactions to PCN. Patients who report a rash only or have previously tolerated cephalosporins of any kind may safely be given the agents listed in this guideline.
USE OF METRONIDAZOLE WITH ALCOHOL: The CDC no longer recommends avoiding alcohol when taking metronidazole. Current evidence doesn’t support that metronidazole use with alcohol results in vomiting (a disulfram-like reaction). It does not inhibit liver aldehyde dehydrogenase nor does its use with alcohol increase levels of acetaldehyde. Thus, metronidazole is considered safe to use in patients who have recently used alcohol or are intoxicated.
RECOMMENDATIONS
Type I and II Fractures
• Preferred: Cefazolin 2 g (3 g if > 120 kg) IV q8h
• Severe cephalosporin allergy: Clindamycin 900 mg IV q8h
• Known MRSA colonization: Add vancomycin 15 mg/kg IV q12h
• Duration of prophylaxis: 24 hours
Type III Fractures
• No gross contamination:
o Preferred: Ceftriaxone 2g IV q24h
o Severe cephalosporin allergy: levofloxacin 500 mg IV q24h
o Known MRSA colonization: Add vancomycin 15 mg/kg IV q12h
o Duration of prophylaxis: 48 hours or 24 hours after wound closure, whichever is shorter
• Contamination with soil or fecal material:
o Preferred: Ceftriaxone 2 g IV q24h + metronidazole 500 mg IV q8h
o Severe Cephalosporin allergy: Levofloxacin 500 mg IV q24h + metronidazole 500 mg IV q8h
o Known MRSA colonization: Add vancomycin 15 mg/kg IV q12h
o Duration: 48 hours after wound closure
o Consider orthopedic infectious diseases consult
• Contamination with standing water:
o Preferred: Piperacillin/tazobactam 4.5 g IV q8h over 4 hours
o Penicillin allergy: Levofloxacin 500 mg IV q24h + metronidazole 500 mg IV q8h
o Known MRSA colonization: Add vancomycin 15 mg/kg IV q12h
o Duration: 48 hours after wound closure
o Consider orthopedic infectious diseases consult
Guidance Summary
| Preferred therapy |
Severe cephalosporin allergy |
Duration |
|
| Type 1 and 2 Fracture |
Cefazolin 2g q8h | Clindamycin 900mg q8h | 24 hours |
| Type 3 Fracture |
Ceftriaxone 2g q24h | Levofloxacin 500mg IV q24h | 48 hours (or 24 hours after wound closure, whichever is shorter) |
| Type 3 Fracture contaminated with soil or fecal material |
Ceftriaxone 2g q24h PLUS Metronidazole 500mg IV q8h | Levofloxacin 500mg IV q24h PLUS Metronidazole 500mg IV q8h | 48 hours (or 24 hours after wound closure, whichever is shorter) |
| Type 3 Fracture with standing water exposure |
Piperacillin/tazobactam 4.5g q8h over 4hours | Penicillin Allergy: Levofloxacin 500mg IV q24h PLUS Metronidazole 500mg IV q8h | 48 hours (or 24 hours after wound closure, whichever is shorter) |
| Known MRSA colonization |
Add Vancomycin 15 mg/kg q12h |
Key Contributors
Kelley McGinnis, PharmD
REFERENCES
• Rodriguez L, Jung HS, Goulet JA, et al. Evidence-based protocol for prophylactic antibiotics in open fractures: improved antibiotic stewardship with no increase in infection rates. J Trauma Acute Care Surg. 2013;77(3):400-8.
• Hauser CJ, Adams CA Jr, Eachempati SR. Surgical infection society guideline: prophylactic antibiotic use in open fractures: an evidence-based guideline. Surg Infect (Larchmt). 2006;7(4):379-405.
• Dunkel N, Pittet D, Tovmirzaeva L, et al. Short duration of antibiotic prophylaxis in open fractures does not enhance risk of subsequent infection. Bone Joint J. 2013;95-B:831-7.
• Anderson A, Miller AD, Categoriestaver PB. Antimicrobial prophylaxis in open lower extremity fractures. Open Access Emergency Medicine. 2011:3:7-11.
• Hoff WS, Bonadies JA, Cachecho R, Dorlac WC. East Practice Management Guidelines Work Group: update to practice management guidelines for prophylactic antibiotic use in open fractures. J Trauma. 2011;70(3):751-4
• Mergenhagen KA, Wattengel BA, Skelly MK, et al. Fact versus Fiction: a Review of the Evidence behind Alcohol and Antibiotic Interactions. Antimicrob Agents Chemother. 2020;64:e02167-19.
• Visapaa JP, Tillonen JS, Kaihovaara PS, et al. Annals of Pharmacother. 2002;36:971-4.
• Workowski KA, Bachmann LH, Chan PA, et al. CDC Sexually Transmitted Infections Treatment Guidelines, 2021. https://www.cdc.gov/std/treatment-guidelines/bv.htm
Hand/Finger Reimplantation
Patients Requiring Hand/Finger Reimplantation
Decision to transfer/divert a patient needing revascularization/replantation will be made based upon:
· Patients with isolated, or near isolated, amputation or devascularization injuries should be transferred to nearest hand reimplantation center.
· Recovery of devascularized or amputated parts with mechanism of injury reasonable for replantation
· Determination of warm/cold limb ischemia time and ability to transport to appropriate replantation center prior to exceeding replantation time limits
o Digit
§ Warm Ischemia <12hrs
§ Cold Ischemia <24hrs
o Hand/Limb
§ Warm Ischemia <6hrs
§ Cold Ischemia <12hrs
· If patient is unable to reach a replant center prior to the ischemia limit, transfer to nearest regional trauma center for additional care.
***Important to note: Patients with multiple traumatic injuries, including hand/arm amputation/devascularization, may not be appropriate for transfer to nearest reimplantation center due to concomitant injuries. In these situations, it may be “life over limb” so transport to the nearest trauma center should take precedent.***
Never hesitate to contact your regional trauma center for guidance on patient transport appropriateness.
Regional Hand Reimplantation Centers:
Adults and Pediatrics
· Nebraska Medicine- consider for potential replantation/revascularization:
402-559-BEDS (9337)
· Denver Health Trauma:
1-855-602-5280 OR 303-628-1550
· University of Iowa
1-866-890-5969
· St. Louis (Barnes-Jewish: Adults/St. Louis Children’s: Pediatrics)
800-678-HELP (4357)
· Regions Hospital- St. Paul, MN:
888-588-9855
· Mayo Clinic
507-255-2910
Adults Only:
· Faith Regional Hospital in Norfolk- Dr. Hartzell
402-371-4880
· KU- Kansas City
913-588-1227
· University of Missouri
573-882-4141
Pediatric Only:
· Children’s Mercy Kansas City, MO
1-800-GO-MERCY
1-800-46-63729
Isolated Hip Fracture Protocol
Section One: Timing and Care Sequence:
1. Presentation to the Emergency Room
a. Assessment by the ED
b. Radiographs
i. Low AP pelvis, AP of affected hip, AP and lateral of affected femur
ii. MRI indicated if high suspicion but no clear fracture on x-ray, CT scan if MRI not available
2. Admission and Consultation
a. Patient admitted to Trauma
After tertiary survey
i. Trauma remains primary and SCM signs off
ii. Trauma signs off, Ortho takes primary, SCM remains on case
Trauma provider re-assigns primary treatment team so that all teams are aware of responsibilities.
b. Ortho consult (called by Trauma provider)
c. SCM consult (called by Trauma provider)
d. Pain consult - Ortho confirms with patient they consent to a block; then calls APS (@ 402-650-9676) for FIB to be done within 4 hours.
e. DEM consult (L. Armas will be contacted by Ortho)
f. consider palliative care consult- can be consulted by any service
g. SW consult (call not needed, just order)
h. PT/OT consult on admission but not to begin evaluation or treatment until the morning after surgery. If arthroplasty, pt will have posterior hip precautions in place
i. Foley only if clinically indicated
3. Orders
a. Preoperative labs drawn
i. CBC, CMP, PT/INR/PTT
ii. Type and Screen. If Hgb < 8 Type and Cross.
iii. Vitamin D: 25(OH)D level **Need to specify mass spect method
b. Chest radiograph if clinically indicated (hx of heart or lung problems or sx)
c. ECG if clinically indicated (hx of heart problems or new sxs)
d. Pain Control
i. Fascia Iliac block* see protocol below (The Ortho provider should call the Anesthesia Acute Pain Service 24/7 @ 402-650-9676 to notify them of the patient). Block should be placed within 4 hrs. of APS notification. (Catheter to be removed at end of OR case)
ii. Tylenol 1000mg TID scheduled; 650mg po TID if history of liver disease
iii. Celebrex 100mg BID scheduled
iv. If age>70, start Oxycodone 2.5mg po Q 3 hours prn, Dilaudid 0.4mg Q2hour prn severe pain
v. If age<70, start Oxycodone 5mg po Q 3 hours prn, Dilaudid 0.6 mg Q2 hours prn severe pain
vi. Weight-bearing Orders – toe touch weight-bearing
vii. Activity as tolerated
e. Warfarin
i. Hold warfarin
ii. If arthroplasty planned, give Vitamin K 2.5 mg IV x1 ASAP (Do not wait for labs)
f. For patients admitted in the evening, keep NPO in anticipation of OR next day, for patients admitted in the morning keep NPO for possibility of OR the same day. Allow Ensure Pre- Surgery CHO drink evening before; consume before midnight
g. Hold ACE-Is and ARBs at admission to decrease the risk of intraoperative hypotension, restart POD #1
Continue ACE-Is and ARBs if systolic BP > 160
Continue ACE-Is and ARBs if LVEF know to be < 30%
h. Continue beta-blockers/rate control medications
i. Order 2000 IU Vitamin D3 daily
4. Patient taken to OR: Goal is patient in the OR next day after admission (Goal: 24-48 hrs.)
5. Postoperative Course
a. Standard postoperative antibiotics x 1 dose (orthopedics orders)
b. Postop CBC, BMP, other labs as needed or based on medical comorbidities, not routine
c. Evaluate pre op anticoagulation medication. Consider Lovenox 30 mg subQ q 12 hours (pharmacy consult for dosing) for VTE prophylaxis x 4 weeks to start POD#1
d. Calcium carbonate 1000 mg (400 mg of elemental calcium) start once daily with food
e. If arthroplasty - nursing communication order for arthroplasty- input full order set for mobility
f. If present, remove Foley on POD #1, straight cath. if retention
g. Goal discharge to home or facility is < 48 hours
h. Mobility: Encourage Dangle within 6-8 hours of surgery with QID ambulation beginning on POD 1, activity as tolerated, WB as tolerated
i. Diet: Patient may resume normal diet post op day 0, protein supplements with each meal/snacks
j. Patient up in chair for all meals x 3
k. Multimodal pain regimen to include combination of Tylenol/NSAIDs
iii. Tylenol 1000mg TID scheduled; 650mg po TID if history of liver disease
iv. Celebrex 100mg BID scheduled
v. Narcotic regimen per Arthroplasty Order Set
Oral Opioids - Moderate/Severe Pain (GFR 30 or less, age 79 yrs. or less)
oxycodone 5 mg, oral, every 2 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 12 hours PRN, moderate pain, severe pain
IV Opioids - Breakthrough Pain (GFR 30 or less, age 79 yrs. or less)
hydromorphone 0.5 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
Oral Opioids - Moderate/Severe Pain (GFR 30 or less, age 80 yrs. or more)
oxycodone 2.5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 12 hours PRN, moderate pain, severe pain
IV Opioids - Breakthrough Pain (GFR 30 or less, age 80 yrs. or more)
hydromorphone 0.2 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
Oral Opioids - Moderate/Severe Pain (GFR more than 30, age 79 yrs. or less)
oxycodone 5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
morphine 7.5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 6 hours PRN, moderate pain, severe pain
IV Opioids - Moderate/Severe Pain (GFR more than 30, age 79 yrs. or less)
morphine 2 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds OR
hydromorphone 0.5 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
Oral Opioids - Moderate/Severe Pain (GFR more than 30, age 80 yrs. or more)
oxycodone 2.5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 6 hours PRN, moderate pain, severe pain
IV Opioids - Moderate/Severe Pain (GFR more than 30, age 80 yrs. or more)
morphine 1 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds OR
hydromorphone 0.2 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
l. Vaccine reconciliation
m. Use of Recovery Milestone Checklist while in hospital
n. Develop Discharge Criteria
o. Gum chewing (sugar free) TID for 20 minutes
p. Utilize Static Meds Initiative (Early AM Meds to Beds delivery program)
6. Discharge: (3 appointments need to be made: bone health, orthopedics, primary care,
a. BONE HEALTH: with Dr. Armas
b. ORTHOPEDICS FOLLOW UP: Orthopedics team resident schedules Orthopedic Surgery
c. PRIMARY CARE: Primary team makes appointment with PCP within 2weeks
d. Primary service ensures detailed post-op instructions
i. Wound care/dressing
ii. PT/Activity
iii. Follow up anticipatory guidance
iv. Specific instructions on when to call the doctor (PCP vs Orthopedic Surgeon)
v. Updated medication list
vi. Continue calcium and vitamin D if they were on admission list or started inpatient.
Section Two: Specific Considerations for Anesthesia and Surgery
1. Anesthesia PreOp
a. Consider Neuraxial in all patients
b. Tranexemic Acid 1 gm IV at the beginning and end of the case
c. Any specific concerns for contraindications to surgery must be discussed between Attendings
2. Surgery
a. Arthroplasty: See pathway for anticoagulation
Case scheduled as Hip hemi-arthroplasty possible total hip.
b. CRPP/ORIF: See pathway for anticoagulation
Case scheduled as CRPP Hip, IMN Hip Fracture, Antegrade Femur Nail
c. Tranexemic Acid 1 gm IV at time of incision- same as spine
d. Standard preop antibiotics.
Section Three: Anticoagulation, Co-Morbidities and Specific Conditions
A. Anticoagulation
1. Anticoagulation for Arthroplasty (determined by Ortho upon eval in ED)
a. Antiplatelet agents
i. Continue Aspirin if history of CAD, stroke, TIA, or PAD. Irreversible antiplatelet effect persists for at least 5 days. If taking > 81 mg daily, reduce to 81 mg daily
ii. Discontinue P2Y12 inhibitors (clopidogrel, ticagrelor, or prasugrel) unless the patient is in the high risk window following coronary stent placement (policy MS54): Acute coronary syndrome within the past 12 months, bare metal stent in the past 1 month, or drug-eluting stent in the past 6 months
b. Warfarin (policy MP11)
i. If initial INR > 3, give additional Vitamin K 2.5 mg IV
ii. If initial INR > 1.5, type and cross for 2-4 units FFP
iii. Re-check INR 12 hours after vitamin K dose
iv. Goal INR for OR is 1.5 or less
v. Can proceed with surgery if INR 1.8 or less and patient can get FFP on the way to the OR (patient will receive GETA)
vi. Consider K Centra
d. DOACs (dibigatran, rivaroxaban, apixiban, edoxaban) (policy MS55)
i. Hold, clearly document time of last dose.
ii. Timing of surgery following last dose of DOAC
a. Factor Xa inhibitor (apixaban, edoxaban, rivaroxaban)
1. eGFR ≥ 30 = 24 hours
2. eGFR < 30 = 48 hours
b. Dabigatran
1. eGFR ≥ 80 = 24 hours
2. eGFR 30-80 = 48 hours
3. eGFR < 30 = 72 hours
c. Risks and benefits should be weighed by teams (ortho, medicine, geriatrics, and anesthesia) if delay > 24 hours is being considered.
2. Anticoagulation for ORIF/CRPP/IMN (Not arthroplasty)
a. Antiplatelet agents
i. Continue Aspirin if history of CAD, stroke, TIA, or PAD. Irreversible antiplatelet effect persists for at least 5 days. If taking > 81 mg daily, reduce to 81 mg daily
ii. Continue P2Y12 inhibitors (clopidogrel, ticagrelor, or prasugrel) if any of the following. Irreversible antiplatelet effect persists for at least 5 days. Acute coronary syndrome within the past 12 months, any cardiac stent, any peripheral artery stent, history of stroke or TIA
b. Warfarin
i. If initial INR > 3.0, administer Vitamin K 2.5 mg IV x 1
ii. If initial INR > 3.0, type and cross for 2-4 units FFP
iii. Goal INR for OR is 3.0 or less
iv. Can proceed with surgery if INR 3.0 or less
c. DOACs (dibigatran, rivaroxaban, apixiban, edoxaban)
i. Hold
ii. Do not delay surgery
3. Bridging Anticoagulation
a. Bridging therapy applies only to patients taking warfarin
b. Bridging therapy with heparin indicated if any of the very high risk conditions below (policy MS55):
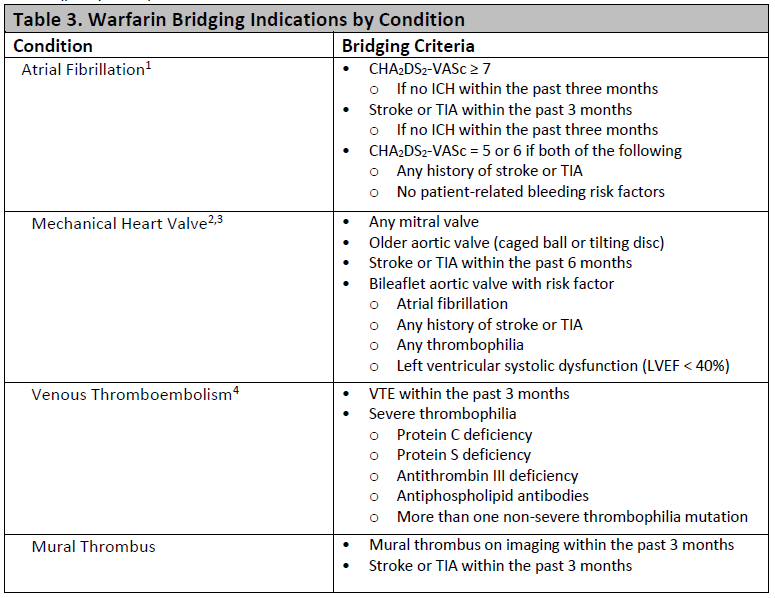
B. Comorbidity
Only unstable conditions should delay surgery. Evaluation of stable conditions must be completed within 24 hours of admission. If delay greater than 24 hours is anticipated, discussion between anesthesiology, Trauma, and hospital medicine is required within 8 hours of admission.
Statement of surgical readiness: One of these statements must be included in the SCM consultation report. If statement c is chosen, a discussion with anesthesiology, Trauma, and orthopedic surgery is required.
a. The patient is medically appropriate to proceed to surgery without further evaluation or management.
b. The patient will be medically appropriate to proceed to surgery when …
c. The patient is not medically appropriate to proceed to surgery. Delay or cancellation recommended.
Indications for surgical delay
a. Active Acute Coronary Syndrome (EKG changes or elevated troponin)
i. Cardiology consult
ii. Delay OR until optimized
b. Unstable Arrhythmia (hypotension or significantly uncontrolled)
i. Cardiology consult
ii. Delay OR until optimized
c. Decompensated CHF with new symptoms: see “Patients requiring an echo”
i. Obtain TTE,
ii. Cardiology consult
iii. delay OR until optimized
d. Acute respiratory failure
i. Obtain ABG for diagnosis of acute respiratory failure
a. SaO2 < 89
b. PO2 < 55
c. PCO2 > 55 with pH < 7.35
ii. Obtain pa/lat CXR, procalcitonin, b-natriuretic peptide
iii. Delay OR until optimized
e. Sepsis
i. Follow sepsis bundle for evaluation and treatment
ii. Delay OR until optimized
Other Comorbidity (not a reason to delay surgery)
a. Cardiac
i. Revised Cardiac Risk Index (RCRI) score: {NUMBERS 0 TO 6)
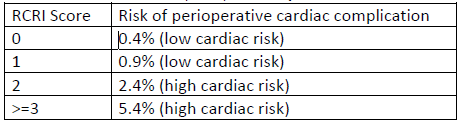
ii. Based on RCRI score and exercise tolerance:
a. Beta blockade indicated: continue if currently taking
b. Statin therapy indicated: continue if currently taking, start if indicated based on 10-year ASCVD risk
c. Inpatient telemetry monitoring recommendation: indicated if significant arrhythmia or RCRI score > 2
iii. Echocardiogram indications
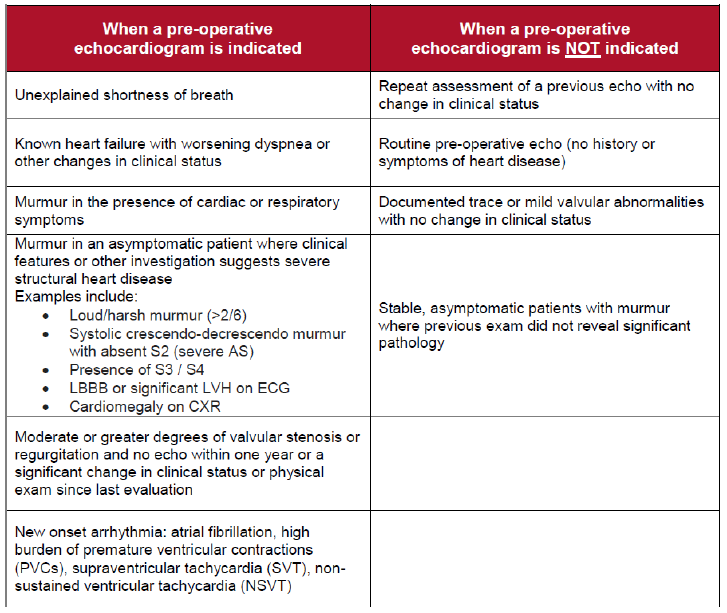
b. Pulmonary
i. STOP-BANG score, OSA risk: (high risk if STOP-BANG > 5 or if known OSA not treated with CPAP)
ii. Management of high risk patients
a. Continuous oximetry
b. Continuous elevation of the head of the patient's bed
c. Complete avoidance of benzodiazepines and sedatives
iii. Management of home CPAP while inpatient
a. Begin CPAP therapy at home settings in the PACU and don't remove it for 48 hours unless the patient is eating or is out of bed.
b. After 48 hours, CPAP with sleep only
c. Diabetes or hyperglycemia (glucose > 180)
i. Avoid dextrose-containing IV fluid
ii. Hold oral diabetes medications while inpatient
iii. Institute basal-bolus insulin therapy
iv. Goal glucose 100-180
d. Hypertension
i. See above for ACEI and ARB management
ii. Continue other antihypertensive medication without interruption
iii. Goal BP < 180/105
e. Delirium
i. High risk for delirium if any of the following
a. Diagnosis of dementia or mild cognitive impairment
b. History of delirium
c. Age ≥ 80 years
e. Transfer from a facility
ii. Prevention of delirium in high risk patients
a. Avoid sedatives (including benzodiazepines and sleep aids) and anticholinergics (including scopolamine patch)
b. Minimize opioids as able.
c. Frequent re-orientation and opening of window shades during the day recommended.
d. Allow sleep
f. Stress dose steroids
i. Continue the patient's home oral steroid regimen without interruption perioperatively
ii. If the patient takes > 7.5 mg prednisone (or equivalent dose of another steroid) daily, administer stress dose steroids. Hydrocortisone 100 mg IV in pre-op followed by 50 mg IV every 8 hours for 3 total doses.
g. Alcohol Use- see CIWA and Phenobarbital protocols
Key Contributors
Zach Bauman,
UNMC Division of Acute Care Surgery, 2024
Isolated Orthopedic Injury Admission Guidelines
Purpose
· To identify which isolated traumatically injured patients can appropriately be admitted to the Orthopedic Service
Background/Definitions
Quality of care and length of stay continue to be areas for improvement at Nebraska Medicine. Given Orthopedic Surgery’s expertise and current workflow/resources, certain trauma patients with isolated Orthopedic issues, may be better served on the Orthopedic Service to improve quality of care and expedite disposition.
Guideline Inclusion Criteria
- Isolated traumatic fracture patients.
- Minimal medical problems or past medical issues which are currently stable and not exacerbated by the injury
- Deemed appropriate for admission to the Orthopedic Service by both the Trauma and Orthopedic Service.
- “Full” or “Limited” activations with isolated injuries.
Guideline Exclusion Criteria
- Poly-trauma patients with fractures.
- Deemed inappropriate for admission to the Orthopedic Service based on medical complexity. If the patient has minimal medical problems or past medical issues which are currently stable and not exacerbated by the injury, then the patient should be admitted to the Orthopedic service. It is highly encouraged for a Trauma/Orthopedic staff conversation in these situations
Diagnostic Evaluation
- Standard trauma work-up per ATLS standards.
- Routine trauma lab work.
- Body region X-ray and/or CT scan
- Pan scan CT as indicated by mechanism or provider discretion
- Trauma Team consultation to make sure trauma work up is complete and no other injuries are present. Also to evaluate appropriateness of Orthopedic Surgery admission.
- Orthopedic Surgery consultation to evaluate patient’s isolated traumatic injury and determine disposition (admission to hospital versus outpatient follow-up) as well as to evaluate appropriateness of Orthopedic Surgery admission.
Practice Recommendations for Management
Patient Entrance into Nebraska Medical Center
- Patients transferred in from an outside institution will be directed to Nebraska Medicine ED (ER→ER). Trauma Team will do the initial trauma evaluation and work-up in the emergency department.
- Patient primarily presents to NMC and meets criteria for an activation (Full or Limited), both the Emergency Medicine and Trauma Team will respond appropriately and the trauma work-up will be conducted as per usual.
- If the patient does not meet activation criteria, Emergency Medicine will perform the initial evaluation.
**If a fracture is identified, Trauma Surgery should be consulted for additional trauma evaluation to make sure the trauma work-up is complete. In all instances, they will be responsible for completion of the tertiary exam.**
Admitting Service and Consultant Involvement
- If a fracture is identified along with other injuries, Orthopedic Surgery will be consulted as well as other consulting services as needed
-
-
- Patient will be admitted to Nebraska Medical Center (NMC) by the Trauma Service for further trauma management as deemed appropriate.
-
-
- If an isolated fracture is identified, Orthopedic Surgery will be consulted for their recommendations.
-
-
- If the decision to admit the patient is made in order to repair the isolated fracture, Orthopedic Surgery will admit the patient to their service based on ACS requirements that trauma patients need to be admitted by a surgeon.
-
-
- If there is concern from the Trauma Service or Orthopedic Service that Orthopedics should not admit the patient, a staff-to-staff conversation should be held between the two services to decide which service the patient should be admitted to.
- Whether the patient needs surgery or not, the standard Nebraska Medicine Enhanced Recovery after Surgery (NERAS) pathway that has been established for isolated fracture patients will be followed.
-
-
- If the decision to admit the patient is made in order to repair the isolated fracture, Orthopedic Surgery will admit the patient to their service based on ACS requirements that trauma patients need to be admitted by a surgeon.
-
-
-
-
- If the decision to discharge the patient is made, the discharge paperwork should be completed by the accepting/managing team with outpatient follow-up orders to be placed by the Orthopedic Surgery service.
-
** Regardless of the admitting service, the Surgical Co-Management Service should be consulted for all fragility fractures (e.g. resulting from ground level fall) and in any other cases for which preoperative risk stratification is desired. **
Follow-up Care
- If the patient is a poly-trauma patient and admitted to NMC per the Trauma Service, discharge and follow-up recommendations will be provided by all consulting services as needed and PT/OT.
-
- All attempts will be made to discharge patient to appropriate location based on patient/family preferences, PT/OT recommendations, and discretion of the Trauma Service
-
- If the patient is an isolated fracture patient admitted to NMC per the Orthopedic Service, discharge and follow-up recommendations will be provided by Orthopedic Surgery and PT/OT.
-
- All attempts will be made to discharge patient to appropriate location based on patient/family preferences, PT/OT recommendations, and discretion of the Orthopedic Service.
-
Outcome Measures and Guideline Adherence
- All traumatically injured patients, whether poly-trauma or isolated Orthopedic injured patients, will be tracked and entered into the NMC and National Trauma Database.
- Performance improvement opportunities will be review by the appropriate service when needed based on the ACS pre-defined hospital complications (see ACS 2022 Trauma Standards Grey Category).
- Non-surgeon admissions of trauma patients will be tracked and updated monthly to the individual services as well as at the monthly PIPS meeting. Each non-surgeon admission will be reviewed per the PI process based on ACS Trauma Standards to determine appropriateness.
Key Contributors
- Zachary Bauman, DO, MHA
- Justin Siebler, MD
- Sara Putnam, MD
- Jason Schiffermiller, MD
Last Updated
February, 2024
References
- American College of Surgeons 2022 Trauma Standards
Orthopedic Trauma Discharge VTE Prophylaxis
Not Indicated:
- In general, VTE prophylaxis at discharge is not indicated for the following injuries:
-
- isolated upper extremity fractures (i.e. clavicle, humerus, elbow, forearm)
- non-operative isolated pelvic fractures (i.e. pubic rami, sacral ala)
-
Indicated:
- In general, if a patient has a lower extremity fracture and is NWB or TTWB for 6 weeks or greater, he/she will require VTE prophylaxis on discharge.
-
- Length of recommended VTE prophylaxis begins from the time of surgery for that particular orthopedic injury.
- If the patient has multiple orthopedic injuries undergoing operative fixation and requiring post-op VTE prophylaxis, pick the longest of the recommended therapies.
-
- While inpatient, a patient should remain on standard VTE prophylaxis for the trauma patient (typically Lovenox BID) and be continued on VTE prophylaxis upon discharge with the recommended therapy and remaining length of treatment as noted for each specific injury.
Recommendations:
- Operative Pelvis Fracture (i.e. pelvic ring, SI joint, pubic symphysis, acetabulum)
-
- VTE Prophylaxis: Lovenox 40 mg subcutaneous daily x 3 weeks followed by Aspirin 81mg PO BID x 3 weeks.
-
- Hip or Femur Fracture
-
- VTE prophylaxis: Lovenox 40mg subcutaneous daily x 3 weeks followed by Aspirin 81mg PO BID x 3 weeks
-
- Patella Fracture
-
- VTE prophylaxis: Aspirin 81 mg BID x 6 weeks
-
- Tibial Fracture
-
- VTE prophylaxis: Lovenox 40 mg subcutaneous daily x 3 weeks, followed by Aspirin 81 mg BID x 3 weeks.
- ***Unless stated otherwise in Dr. Putnam op-note: Aspirin 81 mg BID x 6 weeks
-
- Ankle Fracture
-
- Typical VTE prophylaxis: Aspirin 81 mg BID x 6 weeks
- Pilon fracture/Ex-fixed ankle: Lovenox 40 mg subcutaneous daily x 3 weeks followed by Aspirin 81 mg PO BID x 3 weeks.
- Low risk (no-comorbidities): Aspirin 81 mg BID x 30 days.
-
- Operative food fracture (i.e. calcaneous/tallus/navicular/cuboid)
-
- VTE prophylaxis: Aspirin 81 mg BID x 30 days
-
- Operative Lisfranc injuries (typically ex-fixed initially)
-
- VTE prophylaxis: Lovenox 40 mg subcutaneous daily x 3 weeks followed by Aspirin 81mg PO BID x 3 weeks.
-
- Lower extremity amputation
-
- VTE prophylaxis: none unless considered high risk (co-morbidities, other fractures, etc)
-
- Toe amputation
-
- Antibiotics: oral antibiotics until 1st follow-up appointment
- VTE prophylaxis: none
-
Management of Open Fractures
Purpose
Open fractures are high energy injuries that have increased risk of infection due to potential exposure of bone and deep tissue to a variety of environmental debris. Infection can lead to serious complications including nonunion of wounds and osteomyelitis.
Definitions
Gustilo-Anderson Classifications for open fractures
| Type I fracture |
open fracture with clean wound <1cm long |
| Type II fracture | open fracture with laceration >1cm long without extensive soft tissue damage |
| Type III (A-D) fracture | open segmental fracture, open fracture with extensive soft tissue damage, or traumatic amputation. |
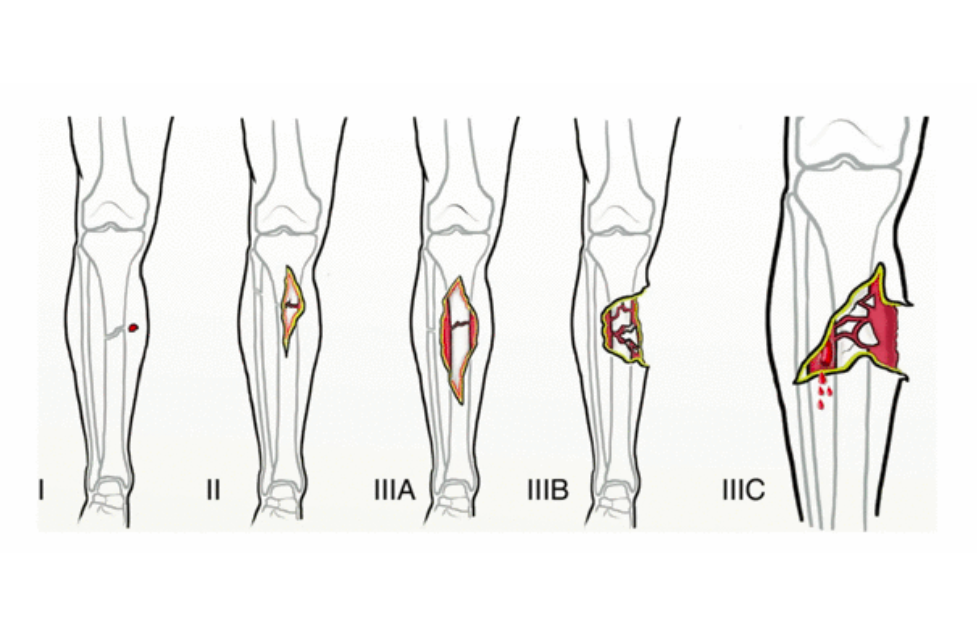
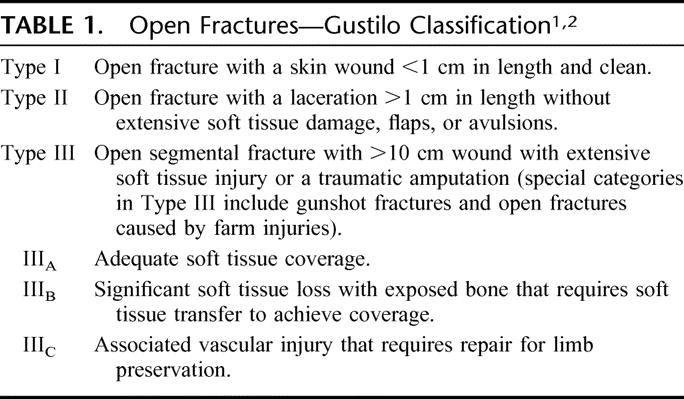
Antibiotic Prophylaxis:
- Intravenous antibiotic prophylaxis should be given to patients with open fractures within 60 minutes of presentation to reduce the risk of infection.
- Antibiotic prophylaxis and duration is based upon the risk of infection utilizing the Gustilo-Anderson Classification System (listed above), with increasing rates of infection associated with higher grades.
- Please refer to: Antimicrobial Stewardship Program Open Fracture Prophylaxis Protocol on the Nebraska Medicine intranet (https://www.unmc.edu/intmed/divisions/id/asp/surgical-prophylaxis/index.html), or the EPIC order set entitled Antibiotic Prophylaxis for Open Fractures (304010005108) for specific antibiotics, dosing, and frequency.
Operative Treatment:
- Open fractures should be taken to the operating room on an urgent basis for irrigation and debridement within 24 hours of initial presentation or sooner whenever possible.
- When possible, skin defects overlying open fractures should be closed at the time of initial debridement.
Performance Improvement:
- All long bone open fractures will be monitored through the Trauma Performance Improvement Process. Specific indicators include:
-
- Time from arrival to first antibiotic dose.
- Time from arrival to initial irrigation and debridement.
-
References
- American College of Surgeons Trauma Quality Improvement Program. ACS TQIP Best Practices in the Management of Orthopedic Trauma. 2015. Retrieved from https://www.facs.org/~/media/files/quality-programs/trauma/tquip/ortho_guidelines.ashx.
- Anderson A, Miller AD, Bookstaver PB. Antimicrobial prophylaxis in open lower extremity fractures. Open Access Emergency Medicine. 2011;3:7-11. doi:10.2147/OAEM.S11862.
- Drunkel N, Pittet D, Tovmirzaeva L, Suva D, Bernard L, Lew D, Hoffmeyer P, Uckay I. Short duration of antibiotic prophylaxis in open fractures does not enhance risk of subsequent infection. The Bone and Joint Journal. 2013;95-B(6):831-837.
- Hauser CJ, Adams CA Jr., Eachempati SE. Surgical infection society guideline: Prophylactic antibiotic use in open fractures: An evidence-based guideline. Surgical Infections. 2006:74(4)379-405.
- Hoff WS, Bonadies JA, Cachecho R, Dorlac WC. EAST practice management guidelines work group: Update to practice management guidelines for prophylactic antibiotic use in open fractures. J Trauma Acute Care Surg. 2011;70(3):751-754.
- Rodriguez L, Jung HS, Goulet JA, Cicalo A, Machado-Aranda DA, Napalitano LM. Evidence-based protocol for prophylactic antibiotics in open fractures: Improved antibiotic stewardship with no increase in infection rates. J Trauma Acute Care Surg. 2014;77(3):400-408.
Author(s)
Justin Siebler, MD, Chief of Orthopedic Trauma
Last Updated
May, 2021
Mangled Extremity Management
Purpose: To aid in the rapid evaluation of a trauma patient presenting with a severely injured limb, providing a decision-making tool for limb salvage vs. amputation in a multidisciplinary fashion.
Background: Patients with a mangled extremity, defined as an extremity with an injury to at least three out of four systems (soft tissue, bone, nerves, and vessels) represent a high-risk patient population requiring expedient care to salvage life and limb. These patients frequently have multi-system and life-threatening injuries and balancing these issues is extremely important. Prompt re-establishment of vascular integrity and fracture stabilization is imperative for limb salvage, when possible. The coordination of multiple surgical services (Trauma, Orthopedics, Vascular, and Plastics) is essential.
Limb salvage versus amputation
Current injury severity scoring systems, specifically the Predictive Salvage Index (PSI) and Mangled Extremity Severity Score (MESS), for mangled extremities do not predict functional recovery of patients who undergo successful limb reconstruction. Limb salvage should be attempted if the other injuries are minimal, the patient is hemodynamically stable and the extremity injuries are amendable to salvage. The involved faculty should have a brief but focused discussion in the OR regarding priorities of care.
Questions for the teams involved:
Orthopedics: can the bone ultimately be saved/reconstructed and/or temporarily stabilized?
Vascular: can the acute arterial injury (if present) be repaired or bypassed in a timely fashion?
Trauma surgery: is the patient stable enough hemodynamically and metabolically to undergo acute revascularization and a prolonged reconstruction?
Plastic surgery: can the wound ultimately be covered or managed? (may be difficult to tell at initial presentation, but should weigh in)
If there is consensus among the involved teams, i.e. all the answers are affirmative to the above questions, then proceed with limb salvage (revascularization/reconstruction procedures). If one or many of the answers to the above questions are are in the negative then proceed with acute amputation.
All services must document their agreement of findings accordingly.
Indications for early amputation:
· Hemodynamic and physiologic instability secondary to complex injured extremity as determined by Trauma surgery faculty, i.e. “life over limb”
· unreconstructible osseous injuries as determined by Orthopedic surgery faculty
· unreconstructible soft tissue injuries as determined by Plastic Surgery faculty
· irreparable vascular injuries as determined by Vascular or Trauma Surgery faculty
· severe loss of soft tissue
Indications for limb salvage:
· all other patients not meeting above criteria
Updated:
· September 2023
Authors
Abby Josef, MD
References:
Ly TV, Travison TG, Castillo RC, Bosse MJ, MacKenzie EJ, LEAP Study Group. Ability of lower-extremity injury severity scores to predict functional outcome after limb salvage. J Bone Joint Surg Am. 2008;90: 1738-1743.
Prasarn ML, Helfet DL, Kloen P. Management of the mangled extremity. Strat Traum Limb Recon. 2012;7: 57-66.
Bonanni F, Rhodes M, Lucke JF. The futility of predictive scoring of mangled lower extremities. J Trauma.1993;34:99-104.
Potter BK, Bosse MJ. American Academny of Orthopaedic Surgeons Clinical Practice Guideline Summary for Limb Salvage or Early Amputation. J Am Acad
8. Vascular Trauma
Educational materials and pathways regarding the evaluation and management of vascular injuries.
Management of Blunt Cerebrovascular Injuries (BCVI)
Management of Blunt Extra – Cranial Carotid and Vertebral Artery Injury in Adults (BCVI)
PURPOSE:
To define guidelines in caring for the trauma patient with diagnosis of blunt extra – cranial carotid and vertebral artery injuries (BCVI)
GUIDELINE:
Screening (Denver Criteria)
Signs/Symptoms
· Potential arterial hemorrhage from neck/nose/mouth
· Cervical bruit (<50 years old)
· Expanding cervical hematoma
· Focal neurologic defect: TIA, hemiparesis, vertebrobasilar symptoms, Horner’s syndrome
· Neurologic deficit inconsistent with head CT
· Stroke on CT or MRI
Risk Factors for BCVI
· High-energy transfer mechanism
· Displaced midface fracture (Lefort II or III)
· Mandible Fracture
· Complex skull fracture/basilar skull fracture/occipital condyle fracture
· Severe TBI with GCS <6
· Cervical spine fracture, subluxation, or ligamentous injury at any level
· Near hanging with anoxic brain injury
· Clothesline type injury or seat belt abrasion with significant swelling, pain, or altered mental status
· TBI with thoracic injuries
· Scalp degloving
· Thoracic vascular injuries
· Blunt cardiac rupture
· Upper rib fracture
Screening Modality
High quality CT Angiography of the neck is an acceptable modality.
Digital subtraction 4-vessel angiography may be required if metallic foreign bodies prevent adequate visualization on CTA
Duplex Ultrasound is not adequate for screening for BCVI.
*** If CTA is ordered to screen for BCVI, a TEG needs to be drawn***
Grading Scale
Grade 1 – Intimal irregularity with < 25% narrowing.
Grade 2 – Dissection or intramural hematoma with > 25% narrowing
Grade 3 – Pseudoaneurysm
Grade 4 – Occlusion
Grade 5 – Transection with extravasation
Treatment
Patients with extracranial carotid and vertebral artery injuries should be treated as outlined below unless: Arterial transection with active hemorrhage is present and/or risk of bleeding from other traumatic injuries prohibits the use of anticoagulation.
Recommendation based on injury grade
Grade 1 and 2
· 81 mg Aspirin
Grade 3
· 81 mg Aspirin
· Neurosurgeon and/or Neuro Interventionalist consultation
· Unlikely to resolve spontaneously with antithrombotic therapy alone. Close follow-up needed.
· Stenting should be avoided due to increased risk for stent thrombosis.
Grade 4
· 81 mg Aspirin
· Neurosurgeon and/or Neuro Interventionalist consultation
· Goal to prevent propagation of thrombus
Grade 5
· Neurosurgeon and/or Neuro Interventionalist consultation
· Endovascular intervention depending on clinical picture:
-
-
-
- Cerebral ischemic events despite the use of anticoagulation or antiplatelet therapy.
- Progressing luminal stenosis despite adequate antithrombotic therapy
- Clinical or radiographic evidence of cerebral perfusion failure due to inadequate collateral blood flow.
- Vertebral artery pseudoaneurysms, as they can rupture into the spinal canal producing epidural and subarachnoid hemorrhage
- Carotid pseudoaneurysms do not require urgent endovascular therapy, as they pose no significant risk of bleeding.
-
-
***Should results of TEG reveal a hypercoagulable state in the setting of BCVI (MA >63 or angle > 77), strong consideration for early initiation of antithrombotic therapy should be made despite competing risk factors due to increased risk for CVA***
Monitoring
· Repeat CTA at 7-days post injury for injury grades 1-3 to assess for resolution of injury and monitor for any progression of luminal stenosis despite antithrombotic therapy, which may benefit from endovascular intervention
· Continued aspirin for 3 months
· CTA is recommended at 3 months to determine the status of the BCVI and the need for further medical or endovascular therapy.

APPROVAL:
Reviewer: Division of Acute Care Surgery, University of Nebraska Medical Center
Approval Date: 1/12/2022
References:
- Cogbill TH, Moore EE, Meissner M, et al. The spectrum of blunt injury to the carotid artery: a multicenter perspective. J Trauma. 1994;37(3):473-479. doi:10.1097/00005373-199409000-00024
- Biffl WL, Moore EE, Ryu RK, et al. The unrecognized epidemic of blunt carotid arterial injuries: early diagnosis improves neurologic outcome. Ann Surg. 1998;228(4):462-470. doi:10.1097/00000658-199810000-00003
- Mutze S, Rademacher G, Matthes G, Hosten N, Stengel D. Blunt cerebrovascular injury in patients with blunt multiple trauma: diagnostic accuracy of duplex Doppler US and early CT angiography. Radiology. 2005;237(3):884-892. doi:10.1148/radiol.2373042189
- Miller PR, Fabian TC, Croce MA, et al. Prospective screening for blunt cerebrovascular injuries: analysis of diagnostic modalities and outcomes. Ann Surg. 2002;236(3):386-395. doi:10.1097/01.SLA.0000027174.01008.
- Burlew CC, Sumislawski JJ, Behnfield CD, et al. Time to stroke: A Western Trauma Association multicenter study of blunt cerebrovascular injuries. J Trauma Acute Care Surg. 2018;85(5):858-866. doi:10.1097/TA.0000000000001989
- Biffl WL, Moore EE, Offner PJ, Brega KE, Franciose RJ, Burch JM. Blunt carotid arterial injuries: implications of a new grading scale. J Trauma. 1999;47(5):845-853. doi:10.1097/00005373-199911000-00004
- Russo RM, Davidson AJ, Alam HB, et al. Blunt cerebrovascular injuries: Outcomes from the American Association for the Surgery of Trauma PROspective Observational Vascular Injury Treatment (PROOVIT) multicenter registry. J Trauma Acute Care Surg. 2021;90(6):987-995. doi:10.1097/TA.0000000000003127
- Bromberg WJ, Collier BC, Diebel LN, et al. Blunt cerebrovascular injury practice management guidelines: the Eastern Association for the Surgery of Trauma. J Trauma. 2010;68(2):471-477. doi:10.1097/TA.0b013e3181cb43da
- Kim DY, Biffl W, Bokhari F, et al. Evaluation and management of blunt cerebrovascular injury: A practice management guideline from the Eastern Association for the Surgery of Trauma [published correction appears in J Trauma Acute Care Surg. 2020 Aug;89(2):420]. J Trauma Acute Care Surg. 2020;88(6):875-887. doi:10.1097/TA.0000000000002668
- Biffl WL, Moore EE, Offner PJ, et al. Optimizing screening for blunt cerebrovascular injuries. Am J Surg. 1999;178(6):517-522. doi:10.1016/s0002-9610(99)00245-7
- Sumislawski JJ, Moore HB, Moore EE, Swope ML, Pieracci FM, Fox CJ, Campion EM, Lawless RA, Platnick KB, Sauaia A, Cohen MJ, Burlew CC. Not all in your head (and neck): Stroke after blunt cerebrovascular injury is associated with systemic hypercoagulability. J Trauma Acute Care Surg. 2019 Nov;87(5):1082-1087. doi: 10.1097/TA.0000000000002443. PMID: 31453984.
Mangled Extremity Management
Please see full page under orthopedic trauma section
9. Thermal Injury
Educational material and pathways regarding the management of thermal injury.
Care of Trauma Patient with Accidental Hypothermia Practice Guidelines
Purpose:
The purpose of this practice guideline is to provide guidance and standardize the approach to the management of trauma patients with accidental hypothermia.
Definition:
Hypothermia is defined as the involuntary drop of core temperature below 36°C (95°F). Symptoms vary based on severity of hypothermia (see section A. Clinical Signs).
A. Clinical Signs
|
Hypothermia |
Body temperature |
Clinical features |
|
|
Mild |
32.2°C to 36°C (90°F to 96.8°F) |
||
|
Hypertension |
|||
|
Shivering |
|||
|
Tachycardia |
|||
|
Tachypnea |
|||
|
Vasoconstriction |
|||
|
Apathy |
|||
|
Ataxia |
|||
|
Cold diuresis—kidneys lose concentrating ability |
|||
|
Hypovolemia |
|||
|
Impaired judgment |
|||
|
Moderate |
28°C (82.4°F) to 32.2°C (90°F) |
Atrial dysrhythmias |
|
|
Decreased heart rate |
|||
|
Decreased level of consciousness |
|||
|
Decreased respiratory rate |
|||
|
Dilated pupils |
|||
|
Diminished gag reflex |
|||
|
Extinction on shivering |
|||
|
Hyporeflexia |
|||
|
Hypotension |
|||
|
J wave |
|||
|
Severe |
< 28°C (82.4°F) |
||
|
Coma |
|||
|
Decreased or no activity on electroencephalography |
|||
|
Nonreactive pupils |
|||
|
Oliguria |
|||
|
Pulmonary edema |
|||
|
Ventricular dysrhythmias/asystole |
|||
B. General Principles
- Room temperature should be maintained at approximately 85ºC (29.4ºF). Use of overhead heating lamps should be considered in the trauma bay.
- Rewarming of the trunk should be undertaken BEFORE the extremities to minimize hypotension and acidemia due to arterial vasodilation and core temperature drop.
- Initiate or maintain CPR if required – Palpate pulse for full minute – An initial attempt at defibrillation can be made but if unsuccessful, further attempts at defibrillation and antiarrhythmic intravenous medications should be held until the patient is warmed to above 30°C.
- Gingerly handle patients to reduce risk of inducing malignant dysrhythmia.
C. Re-Warming
- Mild Hypothermia 32.2°C to 36°C (90°F to 96.8°F)
-
- Room temperature should be maintained at approximately 85ºC (29.4ºF).
-
- Remove all wet clothing.
- Obtain rectal temperature. If temperature will not register, insert a temperature sensing foley catheter or rectal probe thermometer.
-
- Rewarm patient using passive and active external rewarming:
-
- Heated blankets in neck, groin, axilla, torso
- Bair Hugger
-
- RT to place on warmed, humidified O2.
- Infuse Warm intravenous (IV) Fluids:
-
- Warmed isotonic crystalloids or
- Place IV fluids on rapid infuser to utilize warming mechanism. Adjust flow rate so fluids are not delivered at rapid rate unless there is an indication for rapid fluid resuscitation.
-
- Room temperature should be maintained at approximately 85ºC (29.4ºF).
-
- Moderate to Severe Hypothermia 28°C to 32.2°C (82.4°F - 90°F) to < 28°C (<82.4°F)
-
- Obtain temperature using either temperature sensing foley, esophageal temperature sensing probe or rectal temperature sensing probe (if utilizing gastric and/or bladder lavage, use the rectal temperature sensing probe).
- Employ all interventions listed under mild hypothermia.
- Consider use of Artic Sun device.
- Consider use of body bag to maintain the warm air around the patient.
- Per MD order, assist with active internal rewarming via:
-
- Gastric lavage
- Bladder lavage
- Peritoneal lavage
- Thoracic lavage
-
- Continuous Veno-Venous Hemodialysis (CVVHD) – Consider consulting nephrology for initiation of CVVHD.
- Extracorporeal Membrane Oxygenation (ECMO) – Consider consulting ECMO team and Cardiothoracic Surgery for initiation of ECMO.
-
D. Rate of Rewarming
- Slow rewarming - increases temperature by approximately 0.3-1.2°C/h.
-
- Warmed IV solutions.
- Heated, humidified oxygen by mask/endotracheal tube.
- Warmed blankets and/or Bair Hugger
-
- Moderate rewarming – increases temperature by approximately 3°C/h.
-
- Artic sun
- Warmed gastric lavage
- Warmed bladder lavage
- Warmed peritoneal lavage
-
- Rapid rewarming – increases temperature by approximately 6°C – 19°C/h.
-
- Warmed thoracic lavage
- CVVHD
- ECMO
-
E. Traumatic hypothermic cardiac arrest
1. Continuation of resuscitation in traumatic hypothermic cardiac arrest will be at the discretion of the trauma surgeon and/or emergency medicine physician in accordance with previously established guidelines for traumatic cardiac arrest resuscitation (Reference 1,2,7).
References:
- American College of Surgeons. (2018). Advanced trauma life support: Student course manual.
- Burlew, C., Moore, E., Moore, F., Coimbra, R., McIntyre Jr., R., Davis, J, Sperry, J., & Biffl, W. (2012). Western Trauma Association critical decisions in trauma: Resuscitative thoracotomy. Journal of Trauma and Acute Care Surgery, 73(6),1359-1363.
- Duong H, Patel G. Hypothermia. [Updated 2021 Jan 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545239/
- Essentials of Emergency Medicine, Chapter 6, Temperature Related Disorders, 2006
- Paal, P., Brugger, H., & Strapazzon, G. (2018). Accidental hypothermia. In Romanovsky, A. (Ed), Thermoregulation: From basic neuroscience to clinical neurology (pp.547-561). Elsevier Science Inc. https://doi.org/10.1016/B978-0-444-64074-1.00033-1
- Paal, P., Gordon, L., Strapazzon, G., Brodman Maeder, M., Putzer, Walporth, B., Wansher, M., Brown, D., Holzer, M., Broessner., & Brugger, H. (2016). Accidental hypothermia-an update. Scandinavia Journal of Trauma, Resuscitation and Emergency Medicine, 24, 111. doi: 10.1186/s13049-016-0303-
- Seamon, M., Haut, E., Van Arendonk, K., Barbosa, R., Chiu, W., Dente, C., Fox, N., Jawa, R., Khwaja, K., Lee, J., Magnotti, L., Mayglothling, J., McDonald, A., Rowell, S., To, K., Falck-Ytter, Y., & Rhee, P. (2015). An evidence-based approach to patient selection for emergency department thoracotomy: A practice management guideline from the Eastern Association for the Surgery of Trauma. Journal of Trauma and Acute Care Surgery, 79(1), 159-173.
- StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan. Available fro
- Zafren, K., & Giesbrecht, G. (2014, July). State of Alaska: Cold injuries guidelines. http://dhss.alaska.gov/dph/emergency/documents/ems/documents/alaska%20dhss%20ems%20cold%20injuries%20guidelines%20june%202014.pdf
Developed by: Trauma Program Coordinator
Reviewed by: Trauma Operations Committee and Trauma Performance Improvement and Patient Safety (PIPS) Committee
Last Updated
February, 2022
Guidelines for the Initial Management of Frostbite
Purpose:
- Provide guidance on the initial evaluation and management of patients sustaining frostbite injuries as well as recommendations regarding wound care and soft tissue management.
Background/definitions:
- Frostbite is the tissue damage resulting from exposure to cold temperatures, usually from freezing of tissues, which results in cellular damage and tissue necrosis. The extent of frostbite depends on the temperature and duration of exposure.
Guideline Inclusion Criteria:
- Patients with history of recent cold exposure with evidence of soft tissue injury (frostbite) presenting to UNMC/NM emergency department
Guideline Exclusion Criteria:
- Patients without history of recent cold exposure
- Patients with history of cold exposure but without evidence of soft tissue injury 72 hrs after exposure.
- Referrals/transfers from outside hospitals—These patients should be referred to closest regional burn center.
Diagnostic Evaluation:
- Diagnosis of frostbite is based on history and clinical exam.
- History:
- Patients should have clinical history consistent with diagnosis of frostbite (i.e. exposure to cold or wet environment)
- Physical exam:
- Frostbite most commonly occurs on hands, feet, ears, and nose. However, can be present on any part of the body exposed to cold or wet conditions for a period of time.
- Findings consistent with frostbite include:
-
- Initially reddish (lighter skin), grayish (darker skin), pale/white or bluish/cyanotic discoloration in involved tissues.
- Tingling, stinging sensations or decreased/loss of sensation
- Involved tissues feel cold, stiff, or woody to palpation
- Blisters may or may not be present on initial examination but often develop over first 24-48 hours
-
- Additional labs and imaging should be obtained at physician discretion based on clinical status of patient, length of cold exposure, associated trauma, need for resuscitation, etc.
Practice Recommendations for Management:
- Initial frostbite management:
- Remove any wet clothing.
- Assess and resuscitate hypothermic patients as indicated (see hypothermia guidelines)
- Avoid re-freezing.
- Rapid re-warming of injured parts
-
- Water baths at temperatures of 37⁰-39⁰ C (98.6⁰-102.2⁰F) over 30 minute intervals is recommended.
- Other methods for active re-warming include: warm IV fluids, warm blankets, Bair hugger, etc.
- Clinical findings, such as the return of sensation, presence of flushing in involved tissues, and involved tissues are pliable or soft (i.e. not hard and frozen), will determine the length of time of rewarming.
-
- Determine grade and depth of frostbite
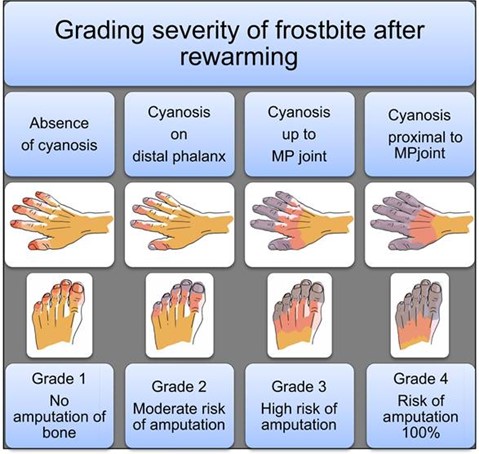
-
-
-
-
- Depth
-
- Superficial – no blisters present
- Partial thickness – serous blisters present
- Full thickness – hemorrhagic blisters present
-
- Depth
-
-
-
-
-
-
-
- patients with grade 3 or 4 frostbite (cyanosis persisting proximal to the distal phalanx after rewarming) and/or demonstrated loss of perfusion at or proximal to the proximal interphalangeal joint of a finger or toe, or the interphalangeal joint of the great toe or thumb immediately after rewarming, consider thrombolytic therapy. (see Guidelines for Thrombolytic Therapy for Frostbite)
-
-
- Pain control:
-
- The re-warming process is often painful and analgesics (including narcotics) should be provided on an as needed basis.
-
- Tetanus prophylaxis should be provided if not up to date/given in the last 5 years.
- Patients should be kept NPO until initial evaluation is complete and need for thrombolytic therapy ruled out.
- Determine need for admission.
-
- If admission required, patients should be admitted to the trauma service.
-
-
- Photos:
- Photo documentation of wounds should be obtained on admission, 24 hours following admission and then serially every 2 days thereafter until discharge.
- Initial Wound care of frostbite
- Wound Care consult should be placed on admission.
- Wound care should be performed twice daily with nursing orders for wound care as indicated.
- Suggested soft tissue management:
-
- Recommendations regarding wound care and activity are based on depth of injury.
- Of note, frostbite may take up to 72 hrs before the depth of frostbite becomes apparent. (i.e. blisters form)
- Superficial thickness:
-
- No blisters present
- Wound care: consider aloe vera, place dry dressings, keep warm
- Activity: limited/gentle weight bearing of affected extremity for the first 48 hrs until soft tissue has fully declared. Following this, may weight bear as tolerated. Keep affected extremity elevated as able.
-
- Partial thickness:
-
- Serous blisters present
- Wound care:
- Activity: Avoid ambulation if on plantar aspects of feet. Otherwise, limited/gentle weight bearing and active range of motion of affected extremity for the first 48 hrs until soft tissue has fully declared. Following this, may weight bear as tolerated. Keep affected extremity elevated as able.
-
- Full thickness
-
- Hemorrhagic blisters present
- Wound care:
-
- blisters do not generally require debridement.
- Dress blisters and open areas in bacitracin followed by xeroform and gently secured with gauze. Avoid tight dressings.
-
- Activity: No weight bearing on the affected extremity for 72 hours. Active range of motion only. Keep affected extremity elevated.
-
- Additional topical agents:
-
- Choice of topical agents may vary between providers and can include (but are not limited to) the following:
-
- Aloe vera – topical thromboxane inhibitor
- Bacitracin – topical antibiotic
- Silver sulfadiazine – topical antibiotic
-
- Choice of topical agents may vary between providers and can include (but are not limited to) the following:
-
-
-
-
-
- Cotton, web roll, or lambs wool should be placed between digits/toes for extra protection and warmth.
- Affected extremities should be elevated with splinting/padding (i.e. Rooke boots) as needed
- For those patient’s with frostbite of the feet, ambulation should occur in protective footwear (i.e. off-loading shoe)
- PT/OT consults should be placed on admission to assist in mobility, range of motion and splinting of the affected extremity as indicated.
- In general, similar to burns, frostbite injuries will evolve over the first 72 hours and can take an extended period of time to demarcate. Waiting until the full extent of necrosis is apparent is recommended prior to surgical amputation (if needed) to allow for as much tissue salvage as possible.
- For patients with Grade 2, 3, and 4 frostbite where amputations may be required, inpatient consultation of orthopedic or plastic surgery may be obtained as needed at the discretion of the trauma attending.
-
-
- Medications for frostbite injury:
- Anti-platelet plus analgesia therapies
-
- The following regimen should be initiated on admission for any frostbite patient NOT undergoing thrombolytic therapy or AFTER completion of thrombolytic therapy/therapeutic anticoagulation in grade 3 or 4 frostbite patients unless contraindicated by medical history (i.e. renal insufficiency, h/o PUD/GI bleed, recent intracranial hemorrhage, etc.)
-
- Aspirin 81mg PO daily x 30 days
- Gabapentin 300 mg q8 hrs x 30 days
- Ibuprofen 600 mg q6 hrs x 14 days
-
- The following regimen should be initiated on admission for any frostbite patient NOT undergoing thrombolytic therapy or AFTER completion of thrombolytic therapy/therapeutic anticoagulation in grade 3 or 4 frostbite patients unless contraindicated by medical history (i.e. renal insufficiency, h/o PUD/GI bleed, recent intracranial hemorrhage, etc.)
-
- Additional multi-modal pain control should be provided as needed.
- In general, prophylactic antibiotics are not indicated.
- Anti-platelet plus analgesia therapies
Admission Guidance:
- Acute frostbite (<72 hours since cold exposure):
- Admit to trauma
-
- Consult orthopedics for management and outpatient follow-up
- Consult hand for upper extremity frostbite and outpatient follow-up
-
- Admit to trauma
- Chronic wounds secondary to frostbite (>72 hours since cold exposure):
- If no other injuries or hypothermia, admit to primary home admitting service (Hospital Medicine, UNMC family medicine, or Clarkson Family Medicine
-
- Consult orthopedics for management and outpatient follow-up
- Consult hand for upper extremity frostbite and outpatient follow-up
-
- If no other injuries or hypothermia, admit to primary home admitting service (Hospital Medicine, UNMC family medicine, or Clarkson Family Medicine
- Frostbite re-admissions
- Admit to primary home admitting service (Hospital Medicine, UNMC family medicine, or Clarkson Family Medicine), NOT trauma
-
- Consult orthopedics for management and outpatient follow-up
- Consult hand for upper extremity frostbite and outpatient follow-up
-
- Admit to primary home admitting service (Hospital Medicine, UNMC family medicine, or Clarkson Family Medicine), NOT trauma
Follow-up Care:
- Patients with frostbite injuries will follow-up in trauma surgery clinic for ongoing wound care with referrals to orthopedic or plastic surgery clinics as needed.
Outcome Measures and Guideline Adherence:
- Track patients with Grade 2 and higher frostbite every 6 months for adherence to guidelines
- Measures: status of wounds, need for amputation, need for thrombolytic therapies, involvement of consulting services (orthopedics, plastic surgery, wound care clinic, etc)
Related Policies:
- Hypothermia Guidelines
- Thrombolytic Therapy for the Management of Severe Frostbite
Key Contributors:
· Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
· Abby Josef, MD | Division of Acute Care Surgery, Faculty | Author
· Zach Bauman, MD | Division of Acute Care Surgery, Faculty | Author
· Ashley Farrens | Division of Acute Care Surgery, Trauma Program Manager | Reviewer
· Meghan Blais, PharmD | Clinical Pharmacist, Nebraska Medicine | Reviewer
Last updated:
· 11/19/2025
References:
- Zaramo TZ, Green JK, Janis JE. Practical review of the current management of frostbite injuries. Plast Reconstr Surg Glob Open. 2022 Oct 24;10(10):e4618
- Murphy JV, Banwell PE, Roberts AH, McGrouther DA. Frostbite: Pathogenesis and treatment. J Trauma. 2000 Jan;48(1):171-8.
- Hickey S, et. al. Guidelines for thrombolytic therapy for frostbite. J Burn Care Res. 2020 Jan 30;41(1):176-183.
- Lacey AM, et al. An institutional protocol for the treatment of severe frostbite injury—A 6-year retrospective analysis. J Burn Care Res. 2021 Aug 4;42(4):817-820.
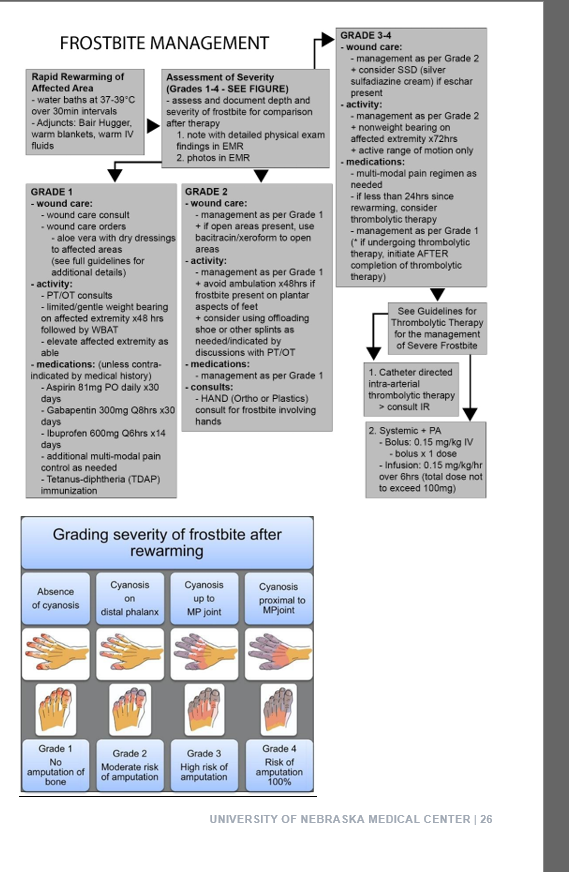
Initial Management of Burns
Purpose:
Provide a brief overview of the classification of burns, initial resuscitation and management, as well as guidelines on triage.
Classification of Burn Injuries:
- First Degree Burn (superficial)
- Involves only the epidermis (no penetration into the dermis)
- Skin appearance: warm, erythematous, no blistering or eschar present
- Painful
- Management: supportive cares (i.e. pain management, aloe vera or soothing lotions); these burns are typically self-limiting, do not scar and will heal without intervention.
- Second Degree Burns (partial thickness)
- Superficial Partial Thickness
-
- Involves the epidermis and papillary dermis
- Skin appearance: blistering, red or pink, moist, blanches with pressure
- Extremely painful
- Management: will usually heal with local wound care; low potential for scarring
-
- Deep Partial Thickness
-
- Involves epidermis, papillary dermis and reticular dermis
- Skin appearance: blistered, waxy, variable in color from red/pink to white, non-blanching
- Less painful
- Management: few smaller burns will heal with good wound care but most will require surgical excision and grafting; high risk for scarring and pigment changes
-
- Superficial Partial Thickness
- Third Degree Burn (full thickness)
- Penetration through epidermis/dermis and into subcutaneous tissues
- Skin appearance: dry, inelastic, waxy or leathery, non-blanching, white/yellow/brown in color with eschar.
- Insensate, not painful
- Management: will not heal without intervention, often requires surgical excision and grafting; high risk for scarring and contractures
- Fourth Degree Burn
- Extends down into the muscle, tendon, or bone
- Skin appearance: charred, black, skeletonized
- Insensate
- Management: will not heal without intervention; often requires surgery/amputation.
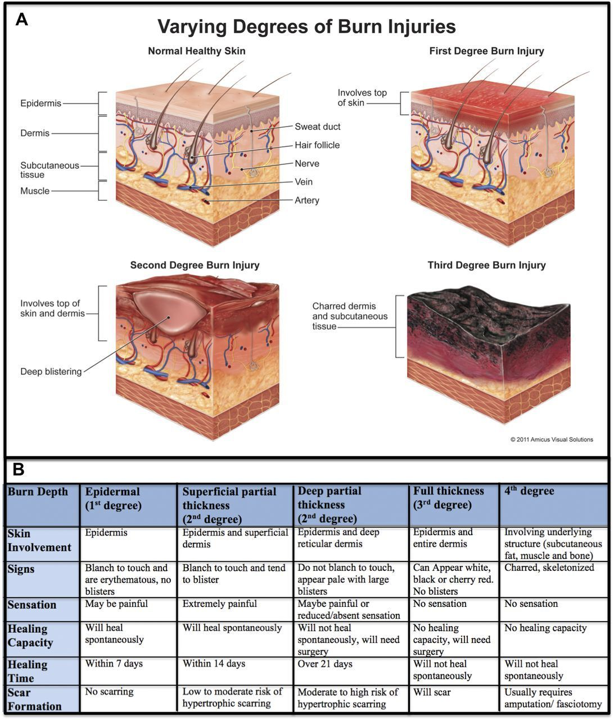
Extent of Burn Injuries
- Accurate determination of burn size ensures proper treatment and resuscitation
- The total body surface area (TBSA) of burns in adults can be estimated using the “Rule of Nines” or by using the patient’s open palm to equal approximately 1% TBSA.
 \
\ - Since body proportions in children differ with age, TBSA in children should be estimated using a Lund-Browder chart (see below) or by using the patient’s open palm to equal approximately 1% TBSA.
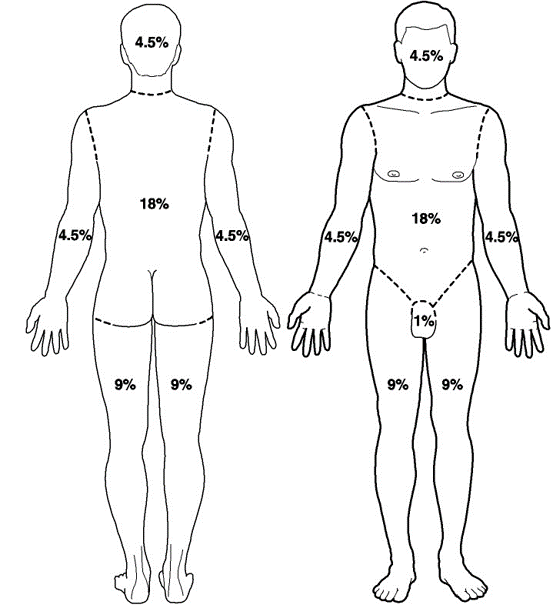
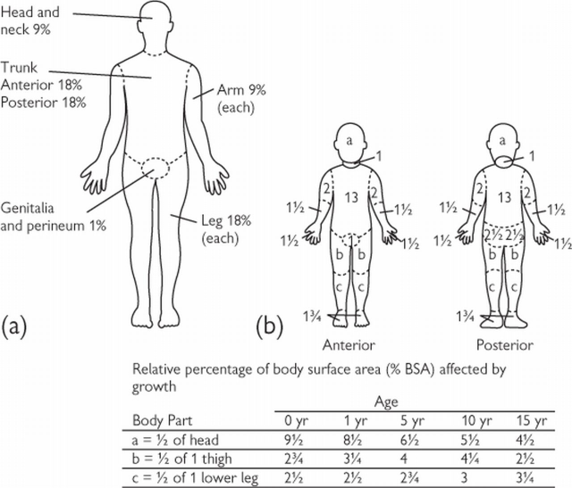
Burn Resuscitation
- The initial approach to a burn resuscitation is similar to standard ATLS
- Please see Special Considerations regarding Inhalational Injury and Escharotomies
- Volume Resuscitation is based upon the % TBSA, age, and weight of the patient
-
- TBSA > 20% require formal resuscitation in all ages
- TBSA > 10% require resuscitation in children and elderly patients
-
- American Burn Association Consensus Formula
-
- 2-4 ml/kg/% TBSA (using LR) in the first 24 hours
- Give 1/2 in the first 8 hours
- Give 1/2 in the subsequent 16 hours
-
- Adults: 2 mL/kg/% TBSA
- Children: 3 mL/kg/% TBSA
-
- Adjust fluid rate for goal urine output 1 cc/kg/hr if child < 14 yr
- If child is < 30 kg, add maintenance fluids that include dextrose (D5LR or D5 1/2 NS) in addition to the consensus formula
-
- Electrical: 4 mL/kg/% TBSA
- Initial Wound Care
-
- Wrap wounds with clean, dry gauze, wrapped in Kerlix
-
- Please note that any dressings or wound care performed will be quickly removed upon transfer to the referring hospital
-
- Wrap wounds with clean, dry gauze, wrapped in Kerlix
-
- Other caveats
-
- Pain Control
- Clarify time of burn and crystalloid received prior to arrival into calculations for initial burn resuscitation
- Update Tetanus
- Consider Cyanokit with appropriate mechanism/circumstances of burn and/or markedly high lactic acidosis
-
Special Considerations
- Inhalational Injury
-
- Significantly increases morbidity and mortality of burn patients
- Present in approximately 1/3 of burn patients
- Injury due to 1. direct injury, 2. edema leading to airway obstruction, and 3. massive inflammatory response
- Diagnosis is subjective and objective
-
- History: mechanism, duration of exposure, location
- Exam: facial burns, singed facial/nasal hair, carbonaceous sputum, soot in oropharynx, voice hoarseness, stridor, erythema and/or edema of the oropharynx
- Work-up: carboxyhemoglobin, chest x-ray, ABG, oxygen saturations
- Flexible bronchoscopy is the gold standard for diagnosis.
-
- Treatment
-
- Supplemental oxygen and pulmonary toilet
- Need for intubation/mechanical ventilation at discretion of the Trauma and ED providers
- Adjuncts: beta-agonists, nebulized acetylcysteine (NAC) and/or heparin, nebulized racemic epinephrine
-
-
- Electrical Burns
-
- Arc burn
-
- Generated by heat from an electrical arc
- Similar treatment to thermal burns
-
- Current burn
-
- Electrical current passes through the body
- Entrance and exit marks are common, as is history of tetany
- Risk for compartment syndrome; evaluation of compartments in an obtunded patient should be performed
-
- Arc burn
-
- Chemical Burn
-
- Identify the chemical, mechanism of exposure, and duration of exposure
- Remove contaminated clothing and follow decontamination protocol per hospital/facility policy
- Affected areas should be copiously irrigated with water
-
- Do not attempt to neutralize the solution as this can result in heat production and worsen injury
-
-
- Escharotomy
-
- Surgical division of nonviable eschar is sometimes required in deep partial and full thickness burns
- The inelastic tissue of the eschar can cause a tourniquet effect over inflamed extremities/compartments and body cavities
- Most commonly performed in extremities with circumferential deep partial or full thickness burns; but may also be required in the neck (airway compromise), chest (diminished chest wall compliance resulting in inadequate ventilation/oxygenation) and abdomen (abdominal compartment syndrome)
- Procedure:
- division through the epidermal and dermal layers (eschar) into the subcutaneous fat following the LAID pneumonic (Longitudinal incisions, axial planes, into normal skin, down into subcutaneous fat)
- usually performed at bedside with sterile drapping
- utilize electrocautery device
- have adequate analgesia and sedation available

-
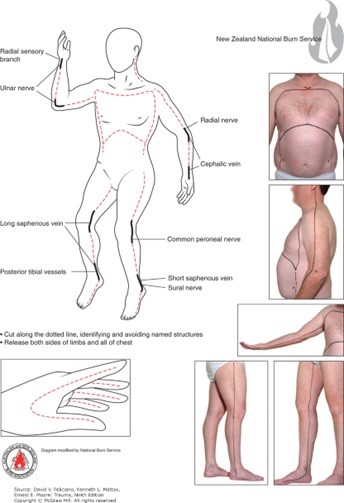
- Non-Accidental Trauma
-
- Burns in children can be the result of child abuse or neglect
- Maintain a high index of suspicion for burns presenting with inconsistent stories for how burn occurred or those presenting in "stocking patterns" suggestive for water immersion burns that are uniform in nature and have a well demarcated line indicated depth of immersion
-
Burn Referral Criteria
- A burn center may treat adults, children, or both. Burn injuries that should be referred to a burn center include the following:
-
- Partial-thickness burns of > 10 % of the TBSA.
- Burns that involve the face, hands, feet, genitalia, perineum, or major joints.
- Third-degree burns in any age group.
- Electrical burns, including lightning injury.
- Chemical burns.
- Inhalation injury.
- Burn injury in patients with preexisting medical disorders that could complicate management, prolong recovery, or affect mortality.
- Burns and concomitant trauma (such as fractures) when the burn injury poses the greatest risk of morbidity or mortality. If the trauma poses the greater immediate risk, the patient’s condition may be stabilized initially in a trauma center before transfer to a burn center. Physician judgment will be necessary in such situations and should be in concert with the regional medical control plan and triage protocols.
- Burns in children; children with burns should be transferred to a burn center verified to treat children. In the absence of a regional pediatric burn center, an adult burn center may serve as a second option for the management of pediatric burns.
- Burn injury in patients who will require special social, emotional, or rehabilitative intervention.
- Trauma Surgeon Discretion
-
Regional Burn Centers Contact Information
- Isolated Burn
- St. Elizabeth’s Burn Center, Lincoln, NE
-
- Transfer Line 1st: (800) 877-2876
- Burn RN Station: (402) 219-7680
- Fax: (402) 219-8773
- Outpatient Burn Clinic: (402) 219-8770
-
- St. Elizabeth’s Burn Center, Lincoln, NE
- Burn with Traumatic Injuries
-
- University of Kansas (KU) Medical Center, Kansas City, KS: 1-877-738-7286
- University of Iowa Medical Center, Iowa City, IA: 1-866-890-5969
-
Note: Requests for photographic evidence of burns sent over SMS/Text are not HIPAA protected and therefore not permitted
Contributors
Last Updated: Feb 14, 2023
References:
1. Levi, Benjamin; Vercruysse, Gary. 2021. Chapter 51: Burns and Radiation. Trauma, 9e. Feliciano DV, Mattox KL, Moore EE. McGraw Hill.
2. Resources for Optimal Care of the Injured Patient. Guidelines for Trauma Centers Caring for Burn Patients. American College of Surgeons, Committee on Trauma, Chicago, Ill. 2014
3. Chapter 9: Thermal Injuries. Advanced Trauma Life Support (ATLS®): The Tenth Edition. 2018. ATLS Subcommittee. American College of Surgeons’ Committee on Trauma; International ATLS working group. Chicago, IL. American College of Surgeons
Thrombolytic Therapy for the Management of Severe Frostbite
Purpose
- Provide guidance on the administration of thrombolytic therapy (t-PA) for the purpose of improving tissue perfusion in the management of severe frostbite injuries.
Background/Definitions
- Frostbite is the tissue damage resulting from exposure to cold temperatures, usually from the freezing of tissues, which results in cellular damage and tissue necrosis. The extent of frostbite depends on the temperature and duration of exposure.
- In more severe forms, frostbite can impair perfusion to digits and extremities.
Inclusion Criteria
- Patients with severe frostbite (grades 3 or 4) in the distal limbs and digits with:
- Absent or weak doppler signals in limbs and/or digits, and no improvement after rewarming OR no perfusion on bone scan.
- Less than 24 hrs of warm ischemia time (defined as time from passive or active rewarming)
Exclusion Criteria
- Contraindications to thrombolytic agents in frostbite include:
-
- Repeated freeze-thaw cycles
- Concurrent or recent (within 30 days) intracranial hemorrhage or traumatic injury with active bleeding
- Recent (within 3 months) intracranial or intraspinal surgery
- Recent (within 3 months) serious head trauma or stroke
- History of gastrointestinal bleeding
- Current severe and uncontrolled hypertension (SBP>180 mm Hg and/or DBP>105 mm Hg)
- Pregnancy
- Uncorrected coagulopathies (INR>1.7, PT>50, PTT>40)
- Thrombocytopenia (Platelets <50)
- Recent hemorrhage or bleeding diasthesis
- Drug or alcohol intoxication
-
(Healthcare provider discretion may override some contraindications as patient's condition warrants)
Diagnostic Evaluation
- The healthcare provider should follow the "Guidelines for the Initial Management of Frostbite".
- In addition to those guidelines, the healthcare provider should also obtain the following:
-
- a thorough history to identify indications and contraindications to t-PA use
- a thorough physical exam should also be performed to include:
-
- an extended neurologic examination
- a detailed description of frostbite, grade of frostbite injury and vascular exam of the involved digit(s) or extremity, and photos of the involved areas.
-
-
- Order baseline labs: CBC, BMP + Mg/Phos, PT/INR, PTT, CK, TEG, and type and screen
- Obtain baseline vital signs
- Obtain CT head if there is any history of associated trauma or if patient is altered and unable to provide a reliable history.
- Obtain Tech-99 bone scan, if possible, to document perfusion status of involved extremity.
Practice Recommendations for Management
- Based on history, physical exam findings, and additional imaging/lab results--the TRAUMA ATTENDING will make the decision to initiate t-PA for frostbite.
- if t-PA is indicated,
-
- Insert 2-3 large bore peripheral IVs (if not already present) with one line dedicated to t-PA administration.
- Ensure blood pressure is controlled prior to initiation of t-PA (SBP<180 and DBP<105)
- Insert/perform any invasive tubes, lines or procedures (if possible) prior to initiating t-PA. Otherwise, wait until t-PA infusion is complete.
- Order TDAP vaccination, if indicated, to be given prior to initiation of t-PA.
- Admit patient to the surgical ICU.
- Notify the ICU charge nurse and pharmacist that thrombolytic therapy is being ordered.
-
- The decision for systemic vs catheter directed intra-arterial thrombolytic therapy will be made at the discretion of the trauma attending.
-
- Catheter directed intra-arterial thrombolytic therapy
-
- Consult interventional radiology
- Orders and infusion rates of thrombolytics to be placed by interventional radiology
-
- Systemic t-PA
-
- Order using the "t-PA for frostbite" order set in EPIC (***currently awaiting build, so in meantime discuss with pharmacy for assistance in ordering***)
- t-PA dose:
-
- Bolus: 0.15 mg/kg IV bolus x 1
- Infusion: 0.15 mg/kg/hr over 6 hours (total dose not to exceed 100mg)
-
-
- Catheter directed intra-arterial thrombolytic therapy
-
- Patient care considerations during thrombolytic therapy:
-
- Patients must undergo q1hr vitals and neurologic checks during infusion of t-PA and or 24 hours following completion of infusion.
- Blood pressure should remain less than 180 mm Hg systolic and 105 mm Hg diastolic during t-PA infusion
- Neurovascular checks of the affected extremity should occur q1hr while t-PA is infusion followed by q4-24 hr checks after infusion is completed.
- CBC, PT/INR, and TEG should be performed q6 hrs while thrombolytics are infusing and for 24 hrs following completion of infusion.
- Limit invasive procedures or punctures while thrombolytics infusing.
- Patients should remain on bedrest while thrombolytics are infusion but should be encouraged to continue with active and functional range of motion while in bed to improve circulation.
-
- Once thrombolytic therapy is complete, the patient should be initiated on therapeutic anticoagulation with either Lovenox or Heparin infusion for 7 days. (If patient is to be discharged prior to 7 days, can consider DOAC for completion of therapy.)
- Additional frostbite wound care and management should follow those listed in the Guidelines for the Initial Management of Frostbite.
Follow-up Care
- Patients with frostbite injuries will follow-up in trauma surgery clinic for ongoing wound care as needed with referrals to orthopedic and plastic surgery clinic as indicated.
Outcome Measure and Guideline Adherence
- All frostbite patients receiving thrombolytic therapy will be reviewed yearly for adherance to guidelines, bleeding complications, status of wounds, need for amputations, and involvement of consulting services.
Related Policies:
- Guidelines for the Initial Management of Frostbite
Key Contributors
Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
Meghan Blais, PharmD | Clinical Pharmacist, Nebraska Medicine | Author
Last Updated
February, 2023
References
- Hickey S, et. al. Guidelines for thrombolytic therapy for frostbite. J Burn Care Res. 2020 Jan 30;41(1):176-183.
- Lacey AM, et al. An institutional protocol for the treatment of severe frostbite injury—A 6-year retrospective analysis. J Burn Care Res. 2021 Aug 4;42(4):817-820.
- Drinane J, Kotamarti VS, O'Connor C, et al. Thrombolytic salvage of threatened frostbitten extremeties and digits: A systematic review. J Burn Care Res. 2019; 40 (5): 541-549.
- Jones LM, Coffey RA, Natwa MP, et al. The use of intravenous tPA for the treatment of severe frostbite. Burns. 2017; 43(5): 1088-1096.
10. Critical Care for Trauma
Educational materials and pathways regarding the evaluation and management of the critically ill.
Adult ICU Electrolyte Replacement
Purpose
To define patients eligible for the electrolyte replacement protocol; to define the process for a provider to order the electrolyte replacement protocol; for a nurse to order and administer electrolyte replacement using this protocol; for a pharmacist to ensure safe dosing of electrolyte replacement; and for when the provider should be contacted when a patient has the electrolyte replacement protocol order set placed.
Policy
Standardized electrolyte replacement will be available for eligible adult ICU patient using an interdisciplinary approach. This includes but is not limited to medication management and monitoring.
Exclusion criteria are as follows:
- Pediatric patients (less than 19 yrs of age)
- Weight < 40 kg
- Renal dysfunction (serum creatinine 1.5 mg/dL or greater or increase in serum creatinine by 50% or renal replacement therapy) within the past 3 days
- pH <7.2 or pH >7.5 within the past 24 hours
- Diabetic ketoacidosis
Procedure
- The ICU Electrolyte Replacement Order Set will be initiated by the ordering provider. The provider will select which electrolytes (magnesium, potassium) they would like to have replaced via protocol, as well as the goal electrolyte level and preferred route of replacement.
-
- NOTE: if exclusion criteria has been met, the provider will be unable to place the order.
-
- The ICU Electrolyte Replacement Order Set will be continued perpetuity and should be evaluated daily to ensure appropriateness of continuation. If a patient develops exclusion criteria and the electrolyte protocol is still ordered, the nurse will be notified of the exclusion criteria that the patient has met and will be instructed to contact the provider regarding replacement.
- With the provider initiating and signing the ICU Electrolyte Replacement order, this allows the nurse to enter appropriate replacement and laboratory monitoring orders.
- When entering subsequent orders the nurse will enter those orders using the appropriate provider name and "Per protocol: cosign required".
Magnesium Replacement
-
-
- The ICU Magnesium Replacement Order Set will be initiated by the ordering provider. They will be required to select the preferred route of replacement (enteral/parenteral or IV only) as well as the magnesium goal level.
- With the provider initiating and signing the ICU Electrolyte Replacement Order Set, this allows the nurse to enter the appropriate replacement and laboratory monitoring orders per Table A or B.
- when entering subsequent orders, the nurse will enter those orders using the appropriate provider name and "Per protocol: cosign required".
- If the Magnesium Replacement Order Set is initiated and the patient has sub-therapeutic magnesium levels within the previous 3 hours, a task will be added to the nursing work list.
- To address the magnesium electrolyte replacement, the nurse will access the ICU Electrolyte Replacement Order Sets within the manage orders tab. The order set will be listed under suggestions. Upon opening the order set, appropriate replacement and lab orders will be presented to the nurse per Table A or B, to enter and sign.
- During verification, the pharmacist will confirm that the order is appropriate per Table A or B.
-
- Duplicate replacement orders will flag on the verification screen.
- "Off protocol" oral replacement will be allowed in certain instances (i.e., continuation of home scheduled magnesium regimen).
-
- After pharmacist verification and acknowledgement of the order, the nurse will administer the ordered dose orally or via the infusion pump.
- The following situations describe when the ordering provider or designee MUST be contracted:
-
- The patient meets exclusion criteria and is ineligible to receive ongoing electrolyte replacement via this protocol.
- The magnesium level is below threshold specified by Table A or B.
-
-
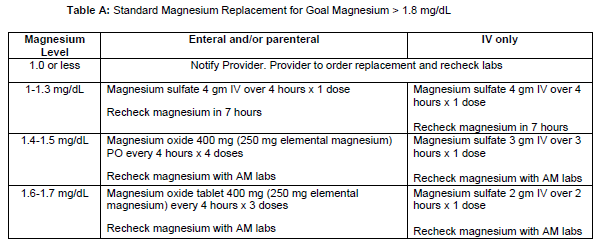
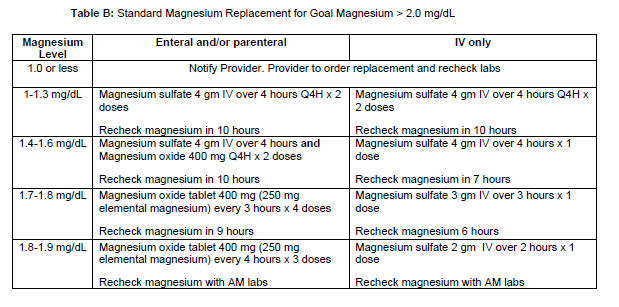
Potassium Replacement
-
-
- The Potassium Replacement Order Set will be initiated by the ordering provider. They will be required to select the preferred route (enteral/parenteral or IV only) as well as the potassium goal level.
- With the provider initiated and signing the ICU Electrolyte Replacement Order Set, this allows the nurse to enter appropriate replacement and laboratory monitoring orders per Table C or D.
- When entering subsequent orders, the nurse will enter those orders using the appropriate provider name and "Per protocol: cosign required".
- If the Potassium Replacement Order Set is initiated and the patient has sub-therapeutic potassium levels within the previous 3 hours, a task will be added to the nursing work list.
- To address the potassium electrolyte replacement, the nurse will access the ICU Electrolyte Replacement Order Sets within the manage orders tab. The order set will be listed under suggestions. Upon opening the order set, appropriate replacement and lab orders will be presented to the nurse per Table C or D, to enter and sign.
-
- NOTE: if the RN has central line access, but is unable to administer using the central line due to concomitant infusions, they will contact the pharmacist to request a change in concentration.
- NOTE: if the RN has central line access, but is unable to administer using the central line due to concomitant infusions, they will contact the pharmacist to request a change in concentration.
-
- During verification the pharmacist will confirm that the order is appropriate per Table C or D.
-
- Duplicate replacement orders will flag on the verification screen.
- "Off protocol" oral replacement will be allowed in certain instances (i.e., continuation of home scheduled potassium regimen or intermittent loop diuretic doses).
-
- After pharmacist verification and acknowledgement of the order, the nurse will administer the ordered dose orally or via the infusion pump.
- The following situations describe when the ordering provider or designee MUST be contacted:
-
- The patient meets exclusion criteria and is ineligible to receive ongoing electrolyte replacement via this protocol.
- The potassium level is below threshold specified by Table C or D.
-
-
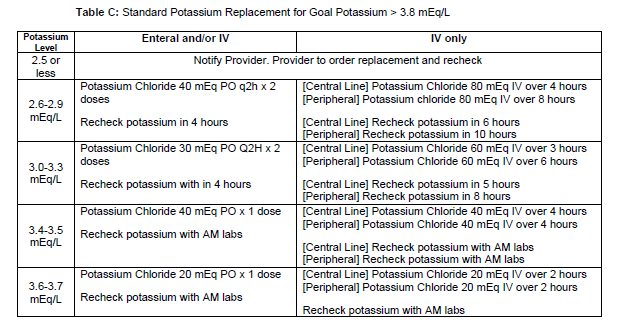
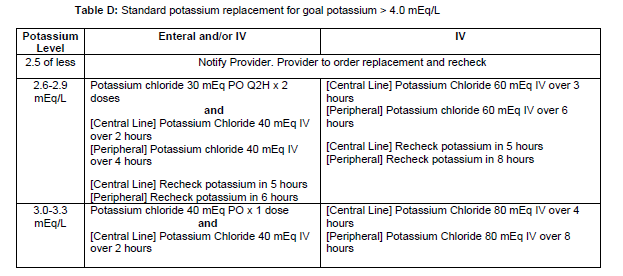
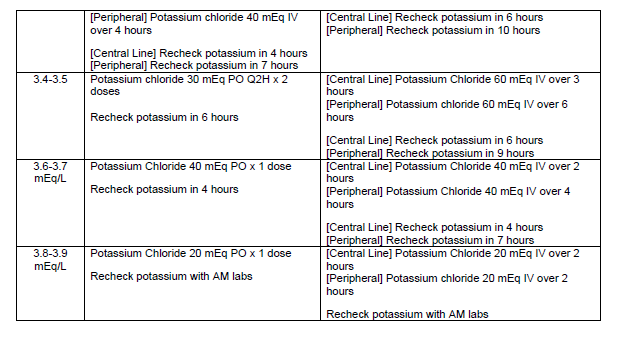
Authors
- Medication Management Committee (06/2022)
- P&T Formulary Committee (06/2022)
- Clinical Governance (07/2022)
Last Updated
7/2022
Evaluation and Management of Atrial Fibrillation
Purpose
- Establish a unified guideline for the diagnosis and treatment of new-onset atrial fibrillation (AF) in Acute Care Surgery patients.
Background/Definitions
- Primary AF: AF with no precipitating cause
- Secondary AF: AF precipitated by a secondary or reversible condition (e.g., surgery, sepsis, acute MI, etc. --most of our ICU patients)
Inclusion Criteria
- Patients with new onset atrial fibrillation.
Exclusion Criteria
- Patients with chronic atrial fibrillation.
Diagnostic Evaluation
- History:
- previous history of arrhythmia?
- currently on anticoagulation?
- Physical:
- irregular heart rhythm
- Imaging/Labs/Tests:
- ECG
- BMP+Mg+Phos
- Other labs at discretion of provider (CBC, blood cultures/infectious work-up, cardiac enzymes, etc)
Practice Recommendations for Management
- New-onset, secondary AF is an organ dysfunction that signals something is wrong--need to address underlying cause while seeking to control rate/rhythm.
- Helpful questions to guide initial approach of patient with AF:
- 1) is the AF causing an immediate problem?
- 2)why is AF happening now (is this primary or secondary AF)?
- 3) should I worry about longer-term problems from the AF?
- Is the AF causing an immediate problem?
- When to consider rhythm control first:
-
- Emergent AF with severe decompensation:
-
- hypotension (SBP<100 or <110 for patients 65 and older), acute heart failure, altered mental status, cardiac ischemia
- if yes --> DCCV (direct current cardioversion)
- consider pairing DCCV with anti-arrhythmic such as amiodarone to increase probability of longer-term success.
-
- Non-emergent AF:
-
- consider a rhythm control strategy first if you think the patient needs atrial kick (i.e. severe mitral stenosis, aortic stenosis) or cannot tolerate nodal blocker (Wolf Parkinson White Syndrome)
-
- Emergent AF with severe decompensation:
-
- When to consider rate control first:
-
- Note: in most instances you can use rate control FIRST.
- Heart rate is higher than it would be with acute illness, but not immediately life threatening to require DCCV.
- Patient has contraindications to anticoagulation.
- Evidence to support a rate control strategy first during secondary AF: success of DCCV is low in secondary AF (as in ICU) --43% at 1 hr, 23% at 24 hrs remain in NSR.
-
- When to consider rhythm control first:
- Why is AF happening now?
- Fix electrolytes (magnesium is an effective rhythm control treatment).
- Fix volume status.
- Look for untreated infection.
- Remove beta-agonists.
- Should I worry about long-term problems from the AF?
- Arterial thromboembolism and AF recurrence are long-term concerns after new-onset AF in critically ill patients
- 44% af AF recurrence in 1 year after new-onset AF in sepsis.
- Cardiology follow-up (either inpatient or outpatient) for long-term rhythm monitoring and treatment plan should be considered.
Outcome Measures and Guideline Adherence
- AF (arrhythmia) is a PI filters for Trauma and Critical Care Surgery that is actively tracked/monitored.
Related Policies
Key Contributors
- Keely Buesing ,MD, FACS, Acute Care Surgery Division
Last Updated
February, 2023
References
- 2019 AHA/ACC/HRS Update
- 2014 AHA/ACC/HRS Guideline
- Um K et al. Pre- and post-treatment with amiodarone for elective electrical cardioversion of atrial fibrillation: a systematic review and meta-analysis. Europace. 2019;21(6):856-863.
- Arrigo M et al. Disappointing success of electrical cardioversion for new-onset atrial fibrillation in cardiosurgical ICU patients. Crit Care Med. 2015;43(11):2354-2359.
- Walkey AJ et al. Practice patterns and outcomes of treatments for atrial fibrillation during sepsis: a propensity-matched cohort study. Chest. 2016;149:74-83.
- Bosch NA et al. Comparative effectiveness of heart rate control medications for the treatment of sepsis-associated atrial fibrillation. Chest. 2021;159(4):1452-1459.
- Davey MJ et al. A randomized controlled trial of magnesium sulfate, in addition to usual care, for rate control in atrial fibrillation. Ann Emerg Med. 2005;45(4):347-353.
- Onalan O et al. Meta-analysis of magnesium therapy for the acute management of rapid atrial fibrillation. Am J Cardiol. 2007;99(12):1726-1732.
- Bosch NA et al. Atrial fibrillation in the ICU. Chest. 2018;154:1424-1434.
Supplemental Materials
- “Etiology of Atrial Fibrillation” schematic.
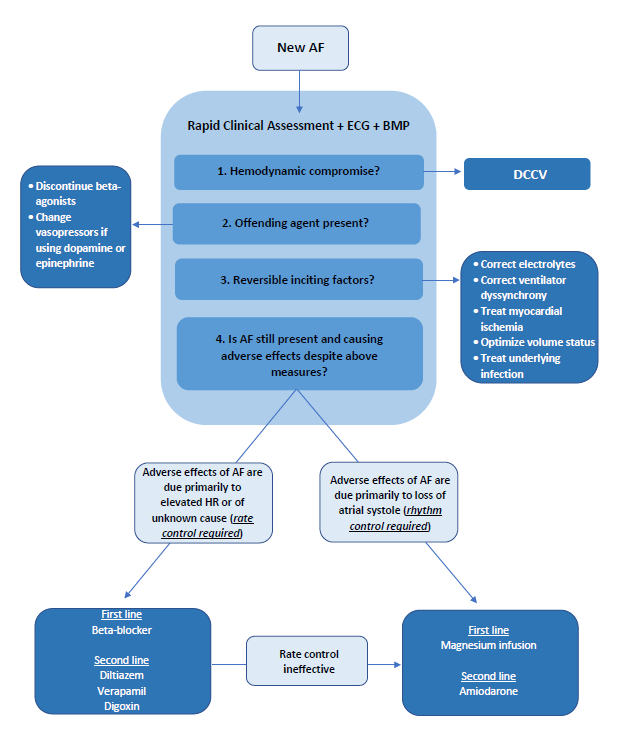
Nebraska Medicine Brain Death Criteria
Nebraska Medicine Policy Number: MS 29
Purpose
To give an accurate and complete description required to establish a diagnosis of breath death/Death by Neurological Criteria (BD/DNC), and to describe the roles and responsibilities of various clinicians and staff members in the process.
Scope
This policy applies to all patients at least 37 weeks corrected gestational age or older at Nebraska Medicine for whom a diagnosis of BD/DNC is considered.
Background
Nebraska Medicine follows the definition of BD/DNC as established by the State of Nebraska in statute 71-7202 and utilizes the accepted medical standards for determining BD/DNC.
A diagnosis of breath death is a clinical diagnosis that can only be established by a staff physician with privileges in neurology or critical/intensive care medicine. The staff physician will document the results of the brain death evaluation in the medical record. The time of death is determined at the time the evaluation is complete. Physicians in training, who are at an advanced level of training and deemed appropriate by the staff physician and working under the staff physician's direct supervision, can perform parts of the examination. The staff physician is fully responsible for the diagnosis, declaration, and documentation of brain death.
Brain Death Evaluation
A complete brain death evaluation consists of three components. All three components must be completed to establish a diagnosis of brain death:
- Establish permanent and proximate cause of coma
- Establish absence of cortical function and brain stem reflexes by neurologic examination
- Establish absence of spontaneous respirations by performing an apnea test
Completion of the three components of the brain death evaluation is sufficient to establish a diagnosis of brain death.
Ancillary Testing
Ancillary testing is not required if all three of the above components are completed. Ancillary tests may be used to support the diagnosis of brain death when uncertainty exists about the reliability of parts of the neurologic exam, when parts of the exam cannot be performed, or to shorten the interval between exams. the current acceptable ancillary tests are: Cerebral angiography, cerebral scintigraphy, and transcranial doppler (if age appropriate).
The interpretation of these tests must be interpreted by a staff physician with the required level of expertise.
Special circumstances:
- Physicians with recognized or potential conflicts of interest in relation to the outcome of the patient's care must remove themselves from the BD/DNC evaluation. For instance, a transplant service physician whose patient expires and has the potential for organ donation should excuse himself/herself from declaring the patient brain dead.
References
- Nebraska State Statute 71-7202. Determination of death. Source: Laws 1992, LB 906, 2.
- Pediatric and Adult Brain Death/Death by Neurologic Criteria Consensus Guideline. Neurology. Dec 12, 2023 issue: 101(24):1112-1132. Greer DM, Kirschen MP, Lewis A, Gronseth GS, Rae-Grant A, Ashwal S, Babu MA, Bauer DF, Billinghurst L, Corey A, Partap S, Rubin MA, Shutter L, Takahashi C, Tasker RC, Varelas PN, Wijdicks E, Bennett A, Wessels SR, Halperin JJ.
- The 2023 AAN/AAP/CNS/SCCM Pediatric and Adult Brain Death/Death by Neurologic Criteria Consensus Practice Guideline. A Comparison with the 2010 and 2011 Guidelines. Ariane Lewis, MD https://orcid.org/0000-0002-075807320, Matthew P. Kirschen MD, PhD https://orcid.org/0000-0003-358502687, and David Greer, MD https://orcid.org/0000-0002-2026-8333 AUTHORS INFO & AFFILIATIONS. December 2023 issue.
Related Policies and Procedures
Acute Bereavement Care -- TX02
Staff Accountability:
- Critical Care Medicine (09/2024)
- Medical Ethics Committee (09/2024)
- Pediatric Quality Committee (11/2024)
- Medical Staff Bylaws Committee NMC (11/2024)
- Medical Staff Medical Executive Committee NMC (11/2024)
- Board of Directors (11/2024)
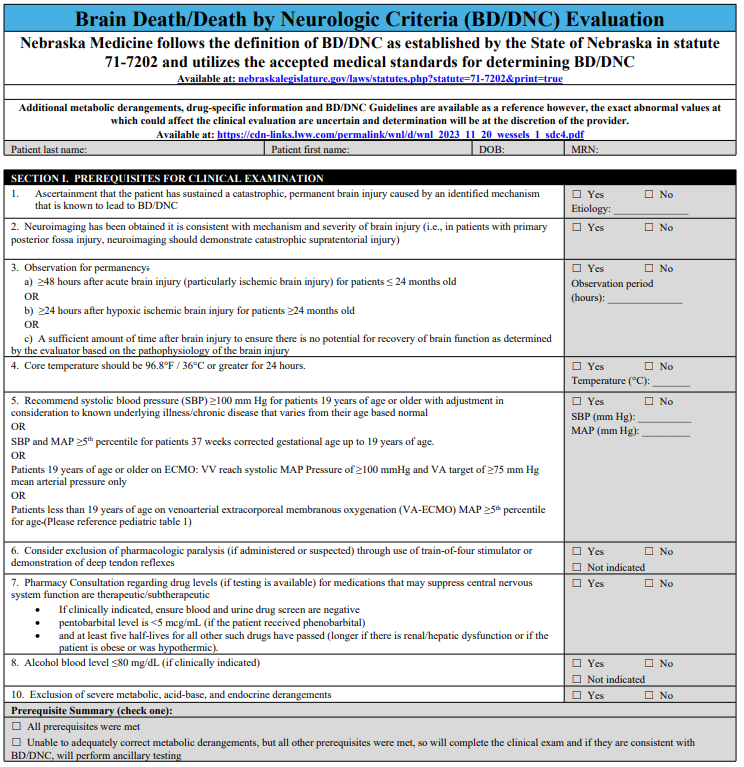
Percutaneous Tracheostomy Protocol
Purpose
To provide guidance on safe practices to perform percutaneous tracheostomy in the operating room and ICU settings.
Preprocedural Planning
- Indications for tracheostomy at the discretion of the attending surgical intensivist.
- The procedure should be scheduled through the operating room by calling OR Charge Nurse.
- Two Attending Physicians must present at bedside to safely perform the procedure. One provider with perform the tracheostomy and one will be managing sedation. A procedure note and a sedation note need to be completed upon completion of the tracheostomy.
- Bronchoscopic guidance is required
- Medications for the procedure consist of an anxiolytic, a narcotic pain medication, and a neuromuscular paralytic. Additionally, local anesthetic may be requested.
- An intubation/airway cart with associated equipment is required at the bedside should reintubation or emergent airway be needed.
Equipment
- Blue Rhino Percutaneous Tracheostomy Kit
- Cuffed Tracheostomy (Size 6 and/or Size 8)
- Sterile Drapes and Chlorohexidine Prep
- Sterile Gowns and Gloves
- Eye protection and Head Coverings
- Bronchoscope
- Sterile water and Lubrication
- Airway cart (associated supplies needed for reintubation if needed)


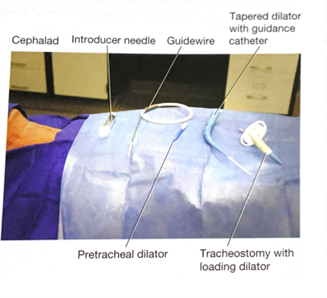
Team
- Attending Intensivist to perform the tracheostomy
- Attending Intensivist to manage sedation
- Trainees (ICU Fellows, Surgical Residents, Medical Students)
- Critical care Nurse
- Respiratory Therapist
- OR Nursing Staff
Room Set-up and Patient Positioning
- The patient should be positioned supine with the neck slightly hyperextended with a shoulder roll if possible. If there is concern for or confirmed cervical spine injury, inline stabilization with the neck in a neutral position must be maintained with securely placed tape.

- The patient’s arms should be placed at patient’s side to ensure access to the neck bilaterally. The bed needs to be positioned to allow for access to the head of the bed so that orotracheal reintubation can be performed if needed.
- For right-handed surgeons, the bronchoscopy cart is generally placed on the patient’s left with the person performing the tracheostomy on the patient’s right. The respiratory therapist should be at the head of the bed with easy access to the patient’s airway. A second provider will be at the head of the bed performing the bronchoscopy. The patient’s nurse needs to have easy access to the patients IV in order to administer medications in a timely manner and the monitor with vital signs and pulse oximetry with audio easily visible to all.

- Set the ventilator to deliver a set volume and rate with 100% FiO2 to preoxygenate the patient. The ICU monitor should set so the pulse oximeter is audible. Continuous hemodynamic monitoring should be achieved with ekg and arterial line or frequent BP cuff monitoring (every 3 minutes).
Technical Steps
- Prior to the start of the procedure, a through “timeout” should be performed. All members of the team should be present and attentive.
- Adequate sedation should be achieved with anxiolytic and narcotic pain medications. This is followed by paralysis.
- Palpate the neck to identify relevant anatomy. Ideal location for placement of the tracheostomy is between the 2nd and 3rd tracheal ring.

- Don all appropriate PPE. Standard sterile surgical technique should be implemented.
- Surgically prepare neck and upper chest with chlorohexidine skin prep. Standard sterile technique and draping should be performed. Consideration for easy access to the endotracheal tube to allow for easy airway exchange after trach is placed.
- Anesthetize the skin and subcutaneous tissue with local anesthetic.

- Using a #15 scalpel, make a 2-3 cm vertical, midline incision approximately 40 mm cephalad (1-2 finger breaths) to the sternal notch and just below the cricoid cartilage. If an anterior jugular vein is encountered in the incision (even if no injury is suspected), consider ligation proximally and distally as this is easiest to perform before the tracheostomy tube has been placed.

- Using a hemostat, bluntly dissect the subcutaneous tissue and muscle in midline to the pretracheal tissue along the length of the incision to better palpate the trachea to determine the point of entry.
- With the bronchoscope adaptor in place, advance the bronchoscope into the airway. Inspect the trachea and bronchial trees and clear any secretions.
- With the assistance of the respiratory therapist, while keeping the bronchoscope at the end of the endotracheal tube, retract both the endotracheal tube and bronchoscope simultaneously until the subglottic structures are visualized and one can see the anterior wall of trachea being palpated by the surgeon. The bronchoscope should be always kept within the endotracheal tube during this portion of the procedure in order to maintain control of the airway and ensure that the bronchoscope is not damaged.
- ***Although usually unnecessary, cautery may be used prior to entering the trachea with the introducer needle. After entry into the trachea, cautery should not be used do to the risk of fire with open oxygen source.***
- An introducer needle is used the enter the anterior portion of the trachea between the 2nd and 3rd tracheal ring (approximately 1 finger breadth below the cricoid cartilage). With the bevel of the needle facing downward, the guidewire is passed into the trachea. Visualization of the guide wire going in the direction of the carina is required. Advance the guidewire slightly passed the carina into the right or left mainstem bronchus.



- Using the Seldinger technique, with constant Bronchoscopic visualization and control of the wire within the trachea, the trachea is sequentially dilated. The dilator handle is hydrophobic which makes it less likely to slip in a wet environment while the actual dilating portion is hydrophilic which only requires water/liquid to be lubricated. First the small tracheal dilator is advanced over the wire to dilate the pretracheal tract. Next the single-stage tapered dilator and the guiding catheter are advanced as a unit over the wire to dilate the trachea. Markings on the side of the progressive dilators guide the depth to which they are inserted. All catheters (pretracheal dilator, tapered dilator, and guiding catheter) should enter perpendicular to the trachea as to prevent pretracheal dissection or false passage. If the patient has limited ventilatory reserve prior to the procedure, the bronchoscope can be removed prior to the dilation portion of the procedure.




- The tapered dilator is removed from the guiding catheter and the guidewire, leaving the guiding catheter and the guidewire in place. If there is a longer distance between the tracheal surface and the skin surface, a finger can be used to dilatate the tract to help facilitate placement of the tracheostomy during the next step.
- Next, an appropriately sized and well lubricated tracheostomy tube with introducer is advanced over the wire and guiding catheter into the trachea. The wire, guiding catheter and loading trocar is then removed, keeping the tracheostomy in place.


- Inflate the tracheostomy cuff, insert the inner canula and connect tracheostomy to ventilator circuit. The presence of end-tidal carbon dioxide after ventilation resumes confirms placement in the airway.
- A bronchoscopy should be performed through the newly placed tracheostomy to visually confirm that it is within the trachea in proper position. Only remove ET tube after placement of tracheostomy tube within the trachea is confirmed.
- The tracheostomy is secured with a tracheostomy collar or ties to help prevent accidental dislodgement and provide time for adequate to tract formation.
- Obtain a chest x-ray to confirm appropriate positioning of the tracheostomy tube, rule out pneumothorax, and evaluate for bronchial obstruction.
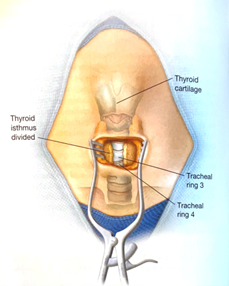

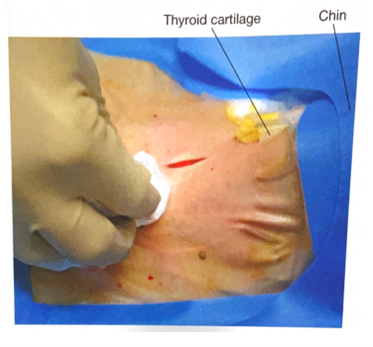





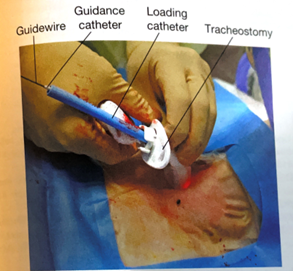
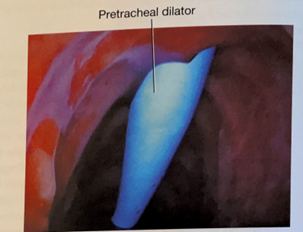

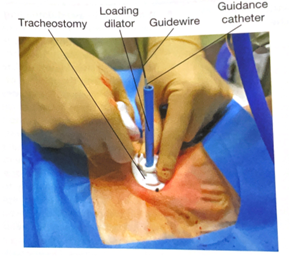
{kind=link}
Tracheostomy Care
- Following tracheostomy placement, standardized tracheostomy care bundles should be implemented. These protocols include steps to ensure the tracheostomy is secure, suctioning techniques, daily stoma hygiene and knowledge of emergency protocols should the newly placed airway be compromised. Special attention should be given to prevent pressure ulceration, particularly along the inferior aspect of the tracheostomy faceplate, especially if the flange is sutured to the skin.
- The tracheostomy tube should be exchanged no sooner than post-operative day 7.
- Once the patient is liberated from the ventilator and secretions are reasonably managed the process of tracheostomy tube downsizing can occur. The downsizing if the tracheostomy tube allows for improved patient comfort and the ability to participate in speech therapy.
- After the tracheostomy is no longer necessary, the patient can be decannulated. The stoma is covered with sterile occlusive dressing generally closes within two to four days.
Key Contributors
Bennett Berning, MD
Last Updated
March, 2023
References
- Cheung NH, Napolitano LM. Tracheostomy: epidemiology, indications, timing, technique, and outcomes. Respir Care. 2014 Jun;59(6):895-915; discussion 916-9.
- Young D, Harrison DA, Cuthbertson BH, Rowan K, TracMan Col- laborators. Effect of early vs late tracheostomy placement on survival in patients receiving mechanical ventilation: the TracMan randomized trial. JAMA 2013;309(20):2121-2129.
- Holevar M, Dunham JC, Brautigan R, Clancy TV, Como JJ, Ebert JB, Griffen MM, Hoff WS, Kurek SJ Jr, Talbert SM, Tisherman SA. Practice management guidelines for timing of tracheostomy: the EAST Practice Management Guidelines Work Group. J Trauma. 2009 Oct;67(4):870-4.
- Delaney A, Bagshaw SM, Nalos M. Percutaneous dilatational tracheostomy versus surgical tracheostomy in critically ill patients: a systematic review and meta-analysis. Crit Care 2006;10(2):R55.
- Hashimoto DA, Axtell AL, Auchincloss HG. Percutaneous Tracheostomy. N Engl J Med. 2020 Nov 12;383(20):e112.
- Hawn, M. T., Berning, B. J., & de Moya, M. A. (2023). Tracheostomy: Open and Percutaneous. In Operative techniques in surgery (2nd Edition, Vol. Volume Two, pp. 2506–2512). Wolters Kluwer.
11. Geriatric Trauma
Educational materials and pathways regarding the evaluation and management of geriatric trauma patients.
Advanced Care Planning and Palliative Care Consultation in Acute Care Surgery
Purpose
· To engage injured or ill patient’s and/or families in discussions regarding goals of care and advanced care planning early and provide guidelines for Palliative Care consultation to assist in facilitating discussions surrounding goals of care and expectations of recovery following injury.
Background/Definitions
· Injury and illness is sudden, unpredictable and often life-altering. Patients and families display a variety of reactions after trauma and understanding the patient’s pre-existing psychosocial functioning is imperative to providing complete holistic care. Palliative care consultation can be a helpful service to patients by providing in depth discussion on goals of care related to prognosis and patient preferences, transitional planning, family support and symptom relief management.
Inclusion Criteria
- Age 55 years old or older
- ICU or SDCC admission (all ages)
- Multisystem injuries, specifically an upper and lower extremity injury
- >5 comorbidities
- Or provider discretion (consider things like homelessness, mental health, low social support, challenging injury)
- Should be done once in the inpatient setting- ie. Should not be done upon injury/in ER
Exclusion Criteria
- No absolutes
Diagnostic Evaluation
· Patients should be assessed per ATLS guidelines with labs, imaging, consults, and interventions as deemed necessary by trauma team to determine extent of injuries, co-morbid conditions, and general prognosis.
Similarly, emergency general surgery patients should be evaluated and managed as deemed appropriate for the current clinical status/diagnosis.
Practice Recommendations for Management
All acute care surgery patients: WITHIN 24 HRS OF ADMISSION
- An advanced care planning discussion should be held with patients (and/or the patient’s decision-making proxy) admitted to the trauma or emergency general surgery services within 24 hours of admission.
-
- For patient’s less than 19 years of age, discussions should occur with the patient’s legal guardian/parent.
-
- This initial advanced care planning discussion should be led by an acute care surgery service provider (physician or APP).
- The initial advanced care planning discussion should address the following:
-
- Code status
- Identification of health care proxy and decision maker in event patient is unable to make decisions.
- Identification of any advanced directives
- Prognostication based on patient’s injuries, co-morbid conditions, and clinical status.
- Goals and expectations throughout hospitalization and upon discharge.
- Frailty assessment in all patients >60 years of age (see Table 1) or in younger patients who have more than 5 pre-existing chronic medical conditions
-
Palliative care consultation screening (see Table 2)
- Palliative care consultation indicated/not indicated
-
- All advanced care planning discussions should be documented in the electronic medical record under the note type “advanced care planning”.
-
- Note template: .ACSACPINITIALACPDISCUSSION
-
-
Please use the ACP as an opportunity for a therapeutic discussion about the patient’s injuries and prognosis, and likely need for additional support. The goal should be to help explain the patient’s injuries, and guide expectations. If they are likely to need a facility, you can set the expectation that they may not go home, but give them encouragement to return home.
Triggers for Palliative Care Consultation based on initial advanced care planning discussion:
- Palliative care consultation should be considered if any of the following are present:
-
- Positive palliative care screen (Category 1 or 2)
- Frailty score greater than 3 (based on Frail Questionnaire, Table 1)
- Pre-existing end-stage or terminal condition
- A diagnosis with median survival less than 6 months
- Death expected during same ICU/hospital stay
- GCS<8 for greater than 1 week in patients >55 yrs.
- Multi-system organ failure
- Family disagreement with team, advanced directive or each other (lasting >2 days)
- Futility considered or declared by the medical team.
- Family request
- Acute Care Surgery attending discretion
-
- Palliative Care consultation ideally should occur early in patient's hospital course with a goal of assessing and managing the patient via "palliative care bundle" (see Table 3) within 72 hours of admission.
Triggers for Geriatrics Consultation for trauma patients based on initial advanced care planning discussion:
- All patients >75 years of age at admission
- Age 65-75, consider geriatric consultation if conditions listed below are present:
-
- dementia
- 10 or more home prescription medications
- 2 or more ED visits or inpatient admission in past 6 months
- not living independently or residents of nursing homes or assisted living facilities
- provider discretion
-
- in cases where patient's meet criteria for both Geriatrics and Palliative Care consultation:
-
- Request consultation of both services. Geriatrics will primarily assist with geriatric medical conditions, whereas Palliative Care will primarily assist with advance care planning/goals of care.
- This should occur with ongoing communication between Geriatric Medicine, Palliative Care and Trauma teams.
-
Triggers for Family Meeting WITHIN 72 HRS OF ADMISSION
- All Category II patients require a family meeting within 72 hrs of admission.
- Any patient lacking an advanced directive or healthcare proxy AND potential for challenging hospitalization or disposition.
- Family meeting may be led by Palliative Care, Geriatric Medicine or Trauma.
-
- An acute care surgery provider should be present for this discussion regardless of who leads the meeting.
-
- This advanced care planning discussion should be documented in the electronic medical record under the note type “advanced care planning”.
-
- Note template: .ACSACPFOLLOWUP
-
- The 72hr family meeting/follow-up discussion should address the following:
-
- Update on patient’s current clinical status with prognostication based on patient’s injuries, co-morbid conditions, and clinical status.
- The patient and/or family’s insight into the current problem(s).
- Hopes and fears for current hospitalization.
- Focused care plans based on patient’s injuries, co-morbid conditions, and clinical status (i.e. best case scenario, more-likely scenario, worst case scenario) with a set time-frame for when we will re-evaluate the situation.
-
- This should also include potential “what if’s” (e.g. trachs, PEGs/Feeding tubes, etc)
-
-
Follow-up Care
- Significant changes in a patient’s clinical status, should prompt additional advanced care planning discussions as needed.
- If consulted, palliative care will continue to follow the patient throughout his/her hospital course as indicated.
Outcome Measures and Guideline Adherence
- Timing and documentation of initial advanced care planning discussions will be monitored on 80% of all trauma patients
- Timing and utilization of palliative care services will be monitored on all trauma mortalities and hospice/CMO discharges.
- Pathway will be re-assessed following a 3 month pilot study.
Key Contributors
- Emily Cantrell, MD | Division of Acute Care Surgery | Author
- Charity Evans, MD | Division of Acute Care Surgery | Author
- Elizabeth Mahal, MD | Department of Emergency Medicine | Author
- Carrie Siedlik, APRN-NP | Palliative Care Medicine | Author
- Remy Kaslon, APRN-NP | Palliative Care Medicine | Author
- Katie Circo, RN | Nursing Professional Development Specialist MICU and SICU, Nebraska Medicine | Author
- Katherine Maliszewski, MD | Internal Medicine/Geriatric Medicine | Author
- Abby Josef, MD | Division of Acute Care Surgery | Updates Author
Last Updated
October, 2024
References
- American College of Surgeons. Trauma Quality Improvement Program Palliative Care Best Practice Guidelines. https://www.facs.org/media/g3rfegcn/palliative_guidelines.pdf
- American College of Surgeons. Trauma Quality Improvement Program Geriatric Trauma Management Guidelines. https://www.facs.org/media/314or1oq/geriatric_guidelines.pdf
- Fiorentino M, et al. Palliative care in trauma: Not just for the dying. J Trauma and Acute Care Surg. 2019:87(5):1156-1163.
Appendix and Supplemental Materials
Figure 1. Model for advanced care planning discussions and consultation of palliative care in trauma.

Table 1. 5 item FRAIL Questionnaire

Table 2. Palliative Care Screening in Trauma

*Surprise question example: “Would you be surprised if the patient died in the next 12 months?”
Table 3. Palliative Care Bundle

Guideline Algorithm
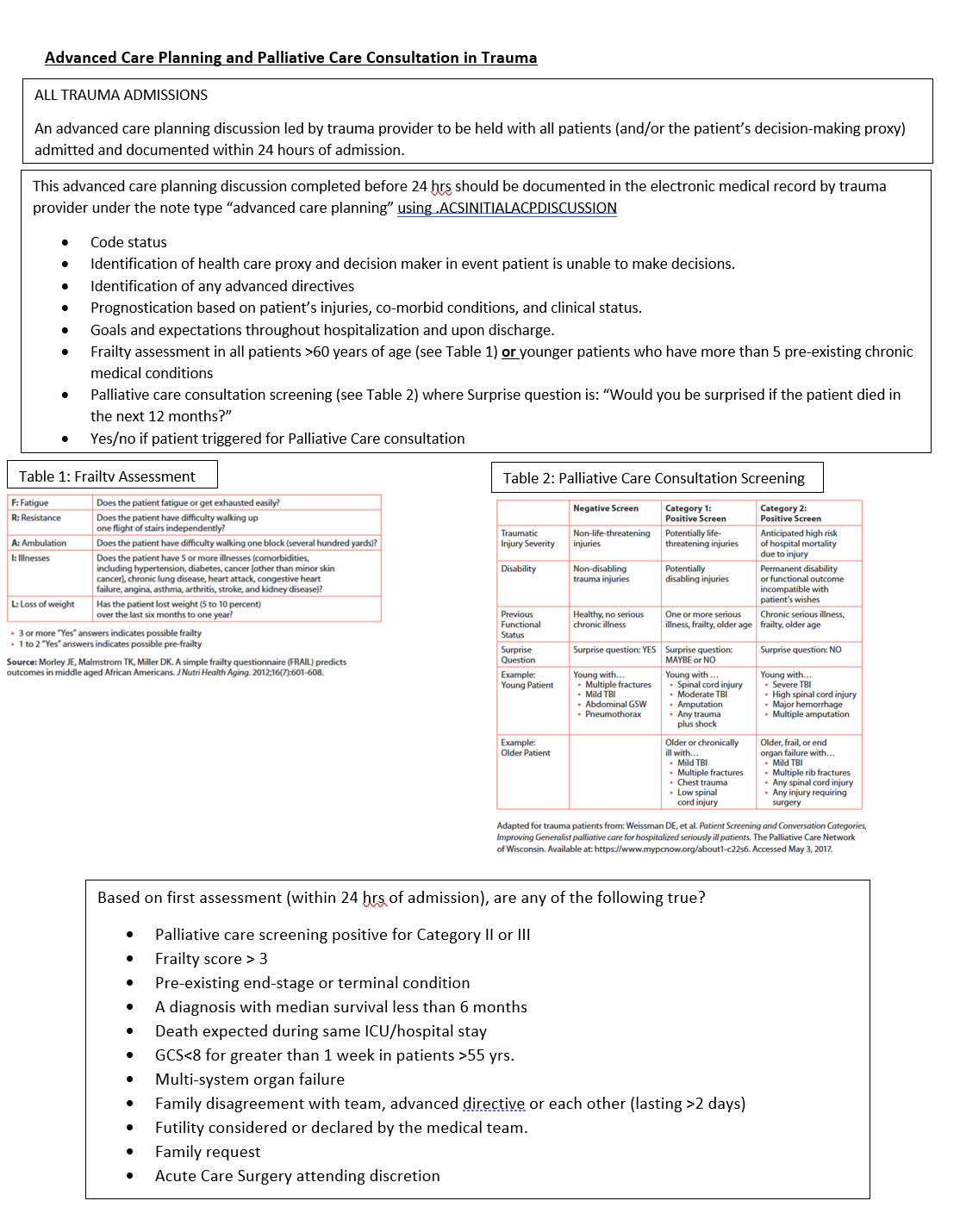
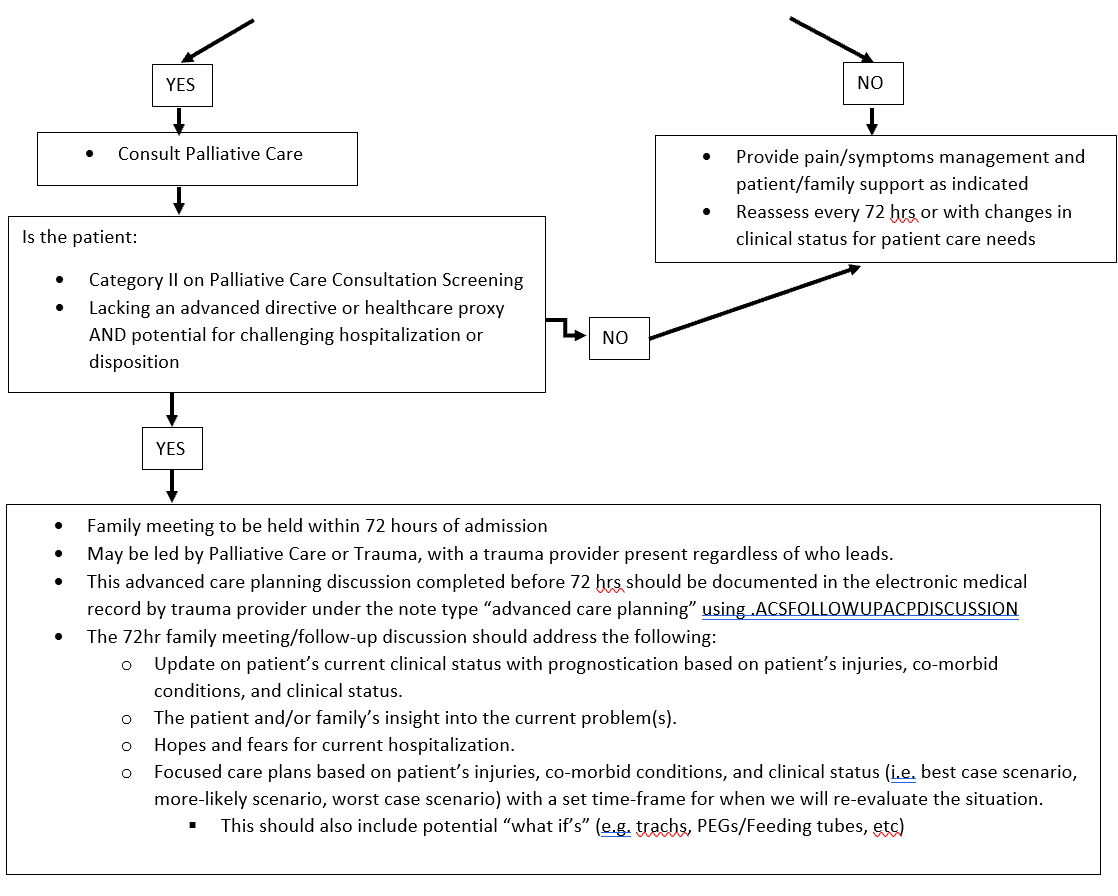
Indications for Geriatric Consultation In Trauma Patients
Purpose
Identify criteria for early geriatric consultation and geriatric expertise on the multidisciplinary trauma care team at the time of admission in order to optimize care of geriatric trauma patients throughout his/her hospital stay.
Criteria for Consultation
- All patients >75 years of age at the time of admission.
- For patients age 65-75 years of age, consider geriatric consultation if any of the following conditions are present on admission:
-
- Dementia
- Greater than or equal to 10 home prescription medications
- greater than or equal to 2 ED or inpatient hospital admissions in the last 6 months
- Not living independently at the time of admission (i.e. residents of nursing facilities or assisted living facilities)
- Provider discretion
-
Author(s)
Trauma Operations Committee
Katherine Maliszewski, MD PhD, Geriatrics Trauma Liaison
Last Updated
June, 2023
Isolated Hip Fracture Protocol
Section One: Timing and Care Sequence:
1. Presentation to the Emergency Room
a. Assessment by the ED
b. Radiographs
i. Low AP pelvis, AP of affected hip, AP and lateral of affected femur
ii. MRI indicated if high suspicion but no clear fracture on x-ray, CT scan if MRI not available
2. Admission and Consultation
a. Patient admitted to Trauma
After tertiary survey
i. Trauma remains primary and SCM signs off
ii. Trauma signs off, Ortho takes primary, SCM remains on case
Trauma provider re-assigns primary treatment team so that all teams are aware of responsibilities.
b. Ortho consult (called by Trauma provider)
c. SCM consult (called by Trauma provider)
d. Pain consult - Ortho confirms with patient they consent to a block; then calls APS (@ 402-650-9676) for FIB to be done within 4 hours.
e. DEM consult (L. Armas will be contacted by Ortho)
f. consider palliative care consult- can be consulted by any service
g. SW consult (call not needed, just order)
h. PT/OT consult on admission but not to begin evaluation or treatment until the morning after surgery. If arthroplasty, pt will have posterior hip precautions in place
i. Foley only if clinically indicated
3. Orders
a. Preoperative labs drawn
i. CBC, CMP, PT/INR/PTT
ii. Type and Screen. If Hgb < 8 Type and Cross.
iii. Vitamin D: 25(OH)D level **Need to specify mass spect method
b. Chest radiograph if clinically indicated (hx of heart or lung problems or sx)
c. ECG if clinically indicated (hx of heart problems or new sxs)
d. Pain Control
i. Fascia Iliac block* see protocol below (The Ortho provider should call the Anesthesia Acute Pain Service 24/7 @ 402-650-9676 to notify them of the patient). Block should be placed within 4 hrs. of APS notification. (Catheter to be removed at end of OR case)
ii. Tylenol 1000mg TID scheduled; 650mg po TID if history of liver disease
iii. Celebrex 100mg BID scheduled
iv. If age>70, start Oxycodone 2.5mg po Q 3 hours prn, Dilaudid 0.4mg Q2hour prn severe pain
v. If age<70, start Oxycodone 5mg po Q 3 hours prn, Dilaudid 0.6 mg Q2 hours prn severe pain
vi. Weight-bearing Orders – toe touch weight-bearing
vii. Activity as tolerated
e. Warfarin
i. Hold warfarin
ii. If arthroplasty planned, give Vitamin K 2.5 mg IV x1 ASAP (Do not wait for labs)
f. For patients admitted in the evening, keep NPO in anticipation of OR next day, for patients admitted in the morning keep NPO for possibility of OR the same day. Allow Ensure Pre- Surgery CHO drink evening before; consume before midnight
g. Hold ACE-Is and ARBs at admission to decrease the risk of intraoperative hypotension, restart POD #1
Continue ACE-Is and ARBs if systolic BP > 160
Continue ACE-Is and ARBs if LVEF know to be < 30%
h. Continue beta-blockers/rate control medications
i. Order 2000 IU Vitamin D3 daily
4. Patient taken to OR: Goal is patient in the OR next day after admission (Goal: 24-48 hrs.)
5. Postoperative Course
a. Standard postoperative antibiotics x 1 dose (orthopedics orders)
b. Postop CBC, BMP, other labs as needed or based on medical comorbidities, not routine
c. Evaluate pre op anticoagulation medication. Consider Lovenox 30 mg subQ q 12 hours (pharmacy consult for dosing) for VTE prophylaxis x 4 weeks to start POD#1
d. Calcium carbonate 1000 mg (400 mg of elemental calcium) start once daily with food
e. If arthroplasty - nursing communication order for arthroplasty- input full order set for mobility
f. If present, remove Foley on POD #1, straight cath. if retention
g. Goal discharge to home or facility is < 48 hours
h. Mobility: Encourage Dangle within 6-8 hours of surgery with QID ambulation beginning on POD 1, activity as tolerated, WB as tolerated
i. Diet: Patient may resume normal diet post op day 0, protein supplements with each meal/snacks
j. Patient up in chair for all meals x 3
k. Multimodal pain regimen to include combination of Tylenol/NSAIDs
iii. Tylenol 1000mg TID scheduled; 650mg po TID if history of liver disease
iv. Celebrex 100mg BID scheduled
v. Narcotic regimen per Arthroplasty Order Set
Oral Opioids - Moderate/Severe Pain (GFR 30 or less, age 79 yrs. or less)
oxycodone 5 mg, oral, every 2 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 12 hours PRN, moderate pain, severe pain
IV Opioids - Breakthrough Pain (GFR 30 or less, age 79 yrs. or less)
hydromorphone 0.5 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
Oral Opioids - Moderate/Severe Pain (GFR 30 or less, age 80 yrs. or more)
oxycodone 2.5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 12 hours PRN, moderate pain, severe pain
IV Opioids - Breakthrough Pain (GFR 30 or less, age 80 yrs. or more)
hydromorphone 0.2 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
Oral Opioids - Moderate/Severe Pain (GFR more than 30, age 79 yrs. or less)
oxycodone 5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
morphine 7.5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 6 hours PRN, moderate pain, severe pain
IV Opioids - Moderate/Severe Pain (GFR more than 30, age 79 yrs. or less)
morphine 2 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds OR
hydromorphone 0.5 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
Oral Opioids - Moderate/Severe Pain (GFR more than 30, age 80 yrs. or more)
oxycodone 2.5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 6 hours PRN, moderate pain, severe pain
IV Opioids - Moderate/Severe Pain (GFR more than 30, age 80 yrs. or more)
morphine 1 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds OR
hydromorphone 0.2 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
l. Vaccine reconciliation
m. Use of Recovery Milestone Checklist while in hospital
n. Develop Discharge Criteria
o. Gum chewing (sugar free) TID for 20 minutes
p. Utilize Static Meds Initiative (Early AM Meds to Beds delivery program)
6. Discharge: (3 appointments need to be made: bone health, orthopedics, primary care,
a. BONE HEALTH: with Dr. Armas
b. ORTHOPEDICS FOLLOW UP: Orthopedics team resident schedules Orthopedic Surgery
c. PRIMARY CARE: Primary team makes appointment with PCP within 2weeks
d. Primary service ensures detailed post-op instructions
i. Wound care/dressing
ii. PT/Activity
iii. Follow up anticipatory guidance
iv. Specific instructions on when to call the doctor (PCP vs Orthopedic Surgeon)
v. Updated medication list
vi. Continue calcium and vitamin D if they were on admission list or started inpatient.
Section Two: Specific Considerations for Anesthesia and Surgery
1. Anesthesia PreOp
a. Consider Neuraxial in all patients
b. Tranexemic Acid 1 gm IV at the beginning and end of the case
c. Any specific concerns for contraindications to surgery must be discussed between Attendings
2. Surgery
a. Arthroplasty: See pathway for anticoagulation
Case scheduled as Hip hemi-arthroplasty possible total hip.
b. CRPP/ORIF: See pathway for anticoagulation
Case scheduled as CRPP Hip, IMN Hip Fracture, Antegrade Femur Nail
c. Tranexemic Acid 1 gm IV at time of incision- same as spine
d. Standard preop antibiotics.
Section Three: Anticoagulation, Co-Morbidities and Specific Conditions
A. Anticoagulation
1. Anticoagulation for Arthroplasty (determined by Ortho upon eval in ED)
a. Antiplatelet agents
i. Continue Aspirin if history of CAD, stroke, TIA, or PAD. Irreversible antiplatelet effect persists for at least 5 days. If taking > 81 mg daily, reduce to 81 mg daily
ii. Discontinue P2Y12 inhibitors (clopidogrel, ticagrelor, or prasugrel) unless the patient is in the high risk window following coronary stent placement (policy MS54): Acute coronary syndrome within the past 12 months, bare metal stent in the past 1 month, or drug-eluting stent in the past 6 months
b. Warfarin (policy MP11)
i. If initial INR > 3, give additional Vitamin K 2.5 mg IV
ii. If initial INR > 1.5, type and cross for 2-4 units FFP
iii. Re-check INR 12 hours after vitamin K dose
iv. Goal INR for OR is 1.5 or less
v. Can proceed with surgery if INR 1.8 or less and patient can get FFP on the way to the OR (patient will receive GETA)
vi. Consider K Centra
d. DOACs (dibigatran, rivaroxaban, apixiban, edoxaban) (policy MS55)
i. Hold, clearly document time of last dose.
ii. Timing of surgery following last dose of DOAC
a. Factor Xa inhibitor (apixaban, edoxaban, rivaroxaban)
1. eGFR ≥ 30 = 24 hours
2. eGFR < 30 = 48 hours
b. Dabigatran
1. eGFR ≥ 80 = 24 hours
2. eGFR 30-80 = 48 hours
3. eGFR < 30 = 72 hours
c. Risks and benefits should be weighed by teams (ortho, medicine, geriatrics, and anesthesia) if delay > 24 hours is being considered.
2. Anticoagulation for ORIF/CRPP/IMN (Not arthroplasty)
a. Antiplatelet agents
i. Continue Aspirin if history of CAD, stroke, TIA, or PAD. Irreversible antiplatelet effect persists for at least 5 days. If taking > 81 mg daily, reduce to 81 mg daily
ii. Continue P2Y12 inhibitors (clopidogrel, ticagrelor, or prasugrel) if any of the following. Irreversible antiplatelet effect persists for at least 5 days. Acute coronary syndrome within the past 12 months, any cardiac stent, any peripheral artery stent, history of stroke or TIA
b. Warfarin
i. If initial INR > 3.0, administer Vitamin K 2.5 mg IV x 1
ii. If initial INR > 3.0, type and cross for 2-4 units FFP
iii. Goal INR for OR is 3.0 or less
iv. Can proceed with surgery if INR 3.0 or less
c. DOACs (dibigatran, rivaroxaban, apixiban, edoxaban)
i. Hold
ii. Do not delay surgery
3. Bridging Anticoagulation
a. Bridging therapy applies only to patients taking warfarin
b. Bridging therapy with heparin indicated if any of the very high risk conditions below (policy MS55):
B. Comorbidity
Only unstable conditions should delay surgery. Evaluation of stable conditions must be completed within 24 hours of admission. If delay greater than 24 hours is anticipated, discussion between anesthesiology, Trauma, and hospital medicine is required within 8 hours of admission.
Statement of surgical readiness: One of these statements must be included in the SCM consultation report. If statement c is chosen, a discussion with anesthesiology, Trauma, and orthopedic surgery is required.
a. The patient is medically appropriate to proceed to surgery without further evaluation or management.
b. The patient will be medically appropriate to proceed to surgery when …
c. The patient is not medically appropriate to proceed to surgery. Delay or cancellation recommended.
Indications for surgical delay
a. Active Acute Coronary Syndrome (EKG changes or elevated troponin)
i. Cardiology consult
ii. Delay OR until optimized
b. Unstable Arrhythmia (hypotension or significantly uncontrolled)
i. Cardiology consult
ii. Delay OR until optimized
c. Decompensated CHF with new symptoms: see “Patients requiring an echo”
i. Obtain TTE,
ii. Cardiology consult
iii. delay OR until optimized
d. Acute respiratory failure
i. Obtain ABG for diagnosis of acute respiratory failure
a. SaO2 < 89
b. PO2 < 55
c. PCO2 > 55 with pH < 7.35
ii. Obtain pa/lat CXR, procalcitonin, b-natriuretic peptide
iii. Delay OR until optimized
e. Sepsis
i. Follow sepsis bundle for evaluation and treatment
ii. Delay OR until optimized
Other Comorbidity (not a reason to delay surgery)
a. Cardiac
i. Revised Cardiac Risk Index (RCRI) score: {NUMBERS 0 TO 6)
ii. Based on RCRI score and exercise tolerance:
a. Beta blockade indicated: continue if currently taking
b. Statin therapy indicated: continue if currently taking, start if indicated based on 10-year ASCVD risk
c. Inpatient telemetry monitoring recommendation: indicated if significant arrhythmia or RCRI score > 2
iii. Echocardiogram indications
b. Pulmonary
i. STOP-BANG score, OSA risk: (high risk if STOP-BANG > 5 or if known OSA not treated with CPAP)
ii. Management of high risk patients
a. Continuous oximetry
b. Continuous elevation of the head of the patient's bed
c. Complete avoidance of benzodiazepines and sedatives
iii. Management of home CPAP while inpatient
a. Begin CPAP therapy at home settings in the PACU and don't remove it for 48 hours unless the patient is eating or is out of bed.
b. After 48 hours, CPAP with sleep only
c. Diabetes or hyperglycemia (glucose > 180)
i. Avoid dextrose-containing IV fluid
ii. Hold oral diabetes medications while inpatient
iii. Institute basal-bolus insulin therapy
iv. Goal glucose 100-180
d. Hypertension
i. See above for ACEI and ARB management
ii. Continue other antihypertensive medication without interruption
iii. Goal BP < 180/105
e. Delirium
i. High risk for delirium if any of the following
a. Diagnosis of dementia or mild cognitive impairment
b. History of delirium
c. Age ≥ 80 years
e. Transfer from a facility
ii. Prevention of delirium in high risk patients
a. Avoid sedatives (including benzodiazepines and sleep aids) and anticholinergics (including scopolamine patch)
b. Minimize opioids as able.
c. Frequent re-orientation and opening of window shades during the day recommended.
d. Allow sleep
f. Stress dose steroids
i. Continue the patient's home oral steroid regimen without interruption perioperatively
ii. If the patient takes > 7.5 mg prednisone (or equivalent dose of another steroid) daily, administer stress dose steroids. Hydrocortisone 100 mg IV in pre-op followed by 50 mg IV every 8 hours for 3 total doses.
g. Alcohol Use- see CIWA and Phenobarbital protocols
Key Contributors
Zach Bauman,
UNMC Division of Acute Care Surgery, 2024
12. Pediatric Trauma
Information dedicated to the care of injured children
Alcohol and Substance Misuse Screening, Brief Intervention and Referral for Treatment (SBIRT) Guidelines for Pediatric Trauma Patients at Nebraska Medicine
Policy and Procedure Statement
The pediatric co-management team will be consulted on all pediatric trauma patients (18 years and younger) admitted to Nebraska Medicine following injury.
As part of their role in the patient’s care, pediatric co-management will assist the trauma team in performing alcohol and substance misuse screening, brief intervention and treatment (SBIRT) as indicated on pediatric trauma patients age 11 years and older.
Screening:
- Pediatric trauma patients age 12 years and older will be routinely screened for alcohol and substance use on admission by laboratory screening using blood alcohol level and/or urine drug screen (UDS). Pediatric trauma patients less than 12 years of age will undergo laboratory screening as needed based on history or suspicion of alcohol or substance misuse.
- A HEADSS assessment will be performed on all admitted pediatric trauma patients age 11 years and older by the pediatric co-management team once the patient reaches floor status.
- If HEADSS assessment is positive for the questions pertaining to drug/alcohol use and exposure AND/OR if blood alcohol (ETOH) or urine drug screen (UDS) testing is positive on admission labs, a CRAFFT screening questionnaire will also be administered.
-
- If the patient is unable to be screened due to the medical condition or refuses, this will be documented in the medical record.
-
Intervention and Referral for Treatment:
- A CRAFFT score of 2 or higher indicates a positive screen. Patients with a positive screen will receive a brief intervention conducted and documented by the pediatric co-management provider, social worker or member of child psychiatry team with referrals for outpatient treatment as indicated.
-
- All pediatric patients who screen positive will receive a social work consult for information on area alcohol/substance misuse programs and assistance with referrals as indicated.
- Child psychiatry may be consulted at the discretion of the trauma or pediatric co-management providers for either inpatient or outpatient assessment of alcohol/substance misuse.
-
Documentation:
The HEADDS assessment, results of alcohol and urine drug screen and CRAFFT assessment (if performed) will be documented in a pediatric co-management team progress note in the patient’s electronic medical record when consulted. For those patients remaining in the ICU for entire hospital course, alcohol and substance misuse screening and interventions will be performed and documented as indicated by the trauma service.
Performance Improvement:
Per American College of Surgeons (ACS) Standards, a minimum of 80% of trauma patients with a hospital stay of >24 hours must be screened for alcohol misuse and a minimum of 80% of patients screening positive must receive an intervention.
Documentation of SBIRT will be done in the trauma registry database.
Any patients that had missed screenings or interventions will be reviewed in the trauma performance improvement process.
References:
- Cohen E, MacKenzie RG, Yates GL. HEADSS, psychosocial risk assessment instrument: Implications for designing effective intervention programs for runaway youth. J Adolesc Health (1991); 12(7):539-544.
- Katzenellenbogen R, HEADSS: The “Review of systems” for adolescents. Virtual Mentor (2005) Mar 1; 7(3): virtualmentor.2005.7.3.cprl1-0503.
- Knight JR, Sherritt L, Shrier LA, Harris SK, Chang G. Validity of CRAFFT substance abuse screening test among adolescent clinic patients. Arch Pediatr Adolesc Med. (2002) Jun;156(6):607-614.
- American College of Surgeons, Resources for the Optimal Care of the Injured Patient, 2022 Standards.


Behavioral Consultation Team Contact Information

Child Life in Trauma Resuscitations
Child Life ED Presentation.pdf
Discharging a Pediatric Trauma Patient Against Medical Advice (AMA)
PURPOSE:
To establish guidelines for addressing situations when minor/pediatric trauma patients depart prior to dismissal by provider (discharge against medical advice) and recognize the right of the patient’s legally recognized representative to make that determination, unless otherwise limited by law.
When any patient leaves prior to dismissal or elopes, it is the policy of Nebraska Medicine to act in accordance with the welfare of the patient and the public while respecting the patient’s rights and complying with applicable laws.
These guidelines are created specifically for the pediatric trauma patient and may not be applicable to adult trauma patients or other service lines. For more information regarding Nebraska Medicine hospital policy, please refer to LD21—Patient Departure Prior to Dismissal (AMA).
DEFINITIONS:
- Departure Prior to Dismissal (also known as departure against medical advice – AMA): departure of a patient who is admitted to the hospital as an inpatient, outpatient or observation status, or who is in a dedicated Emergency Department but has had a medical screening examination completed; patient may or may not make their intention known to staff.
- Elopement: unauthorized departure of a patient from a staffed, around the clock care setting, including the Emergency Department.
- Imminent Risk for Harm: immediate and impending threat of physical harm to self or others, as assessed by provider.
- Minor (pediatric) patient: any individual receiving care under the age of 19 (as defined by Nebraska state laws)
- Legally recognized representative: A parent, guardian, or other person with legal authority to make healthcare decisions on behalf of the minor child.
POLICY
- The legally recognized representative (i.e. parent, legal guardian) of a minor patient has the right to terminate the care encounter and remove the patient from the premise at any time, except when prohibited by law.
-
- Patients who are under a legal hold may not have the right to leave the premises at a time of their choose (see policy LD 12-Legal Status Holds).
- Questions about restrictions related to specific legal holds should be referred to Legal or Risk Management.
-
- If staff believe that the minor patient may be at risk for serious or imminent harm (i.e medical neglect) if removed from the care environment, it may be appropriate to consider reporting the concern an appropriate authority, such as Child Protective Services or law enforcement.
-
- If there are questions or further discussion regarding the specific situation is warranted, providers are encouraged to call Risk Management at 402-559-0060 (24/7 hotline).
-
- Nebraska Medicine will make reasonable efforts to ensure that the minor patient and the legally recognized representative for the minor is informed of the risks of leaving against the advice of the provider.
- Nebraska Medicine respects the minor patient’s/legally recognized representative’s right to choose to accept or decline care. A patient’s or representative’s decision to leave against medical advice of the provider will not negative influence the patient’s ability to receive future care with Nebraska Medicine.
PROCEDURE
- If a minor patient or a patient’s legally recognized representative expresses the desire to leave the premises prior to dismissal against medical advice:
-
- AND the patient’s legally recognized representative has the capacity to make healthcare decisions AND is not under a legal hold:
-
- Staff will attempt to request that the patient and legally recognized representative stay to speak with the trauma provider.
- Staff will notify the trauma provider of the plan to leave against medical advice and may initiate a care discussion, to the extent that the patient and legally recognized representative is willing to participate.
-
- The trauma provider will subsequently notify the trauma attending immediately following notification of a minor patient/representative expressing desire to leave premises against medical advice.
-
- The trauma attending will discuss and inform patient and/or legally recognized representative of the risks and benefits of leaving against medical advice, to the extent that the patient is willing to participate.
-
- If staff or providers believe the patient may be at imminent risk for harm if removed from the current care environment, contact Child Protective Services (CPS) or law enforcement as indicated.
- If there are questions regarding case or presence of imminent risk for harm/medical neglect, contact Risk Management at 402-559-0060.
-
- The trauma attending/trauma providers, with appropriate assistance from staff, will provide plan for care outside the hospital and instructions appropriate to the patient’s specific needs (i.e. prescriptions, follow-up appointments, DME, etc), to the extent that the patient/representative are willing to participate.
- Encounter will be documented in the electronic medical record by the trauma attending or designee using the AMA note template (.AMA) and should include the following information:
-
- Patient/representative’s intent to leave and reasons for leaving, if known.
- Specifics of case/injuries known
- Decision making capacity of the patient’s legally recognized representative
- Description of attempts to inform the patient/representative of risks of leaving against medical advice and their response.
- Parent or legal guardian sign the Informed Refusal of Healthcare Services Form. This document will be included in the patient's electronic health record (EHR) as a part of the permanent medical record. If the patient or legal guardian refuses to sign the form, ED personnel (or trauma attending if the patient is already admitted) will complete the form noting patient/legal guardian's refusal to sign. When a patient/legal guardian refuses to sing, two witnesses should sign the form.
- Time of departure and condition of the patient as assessed by provider.
- If CPS report filed or law enforcement contact.
- Mode of departure and plans for care outside the hospital and instructions given to patient/representative, as applicable.
-
-
- AND the patient’s legally recognized representative has the capacity to make healthcare decisions AND is not under a legal hold:
-
RELATED POLICIES/PROCEDURES
- Patient Departure Prior to Dismissal (AMA) – LD21
- Legal Status Hold – LD12
- Patients Leaving Against Medical Advice -- OPS17
KEY CONTRIBUTORS
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Manager | Co-Author
Evaluation and Management of Blunt Solid Organ Injuries in Pediatric Trauma Patients
Purpose:
These guidelines are meant to help guide the provider through the initial evaluation and management of pediatric trauma patients sustaining blunt solid organ injuries to the liver, spleen, or kidney at Nebraska Medicine.
Background/definitions:
Solid organ injuries may occur to the liver, spleen or kidney. Non-operative management of solid organ injuries in the setting of blunt trauma is preferred when possible and is considered the standard of care in hemodynamically stable pediatric patients, irrespective of the grade of injury. Literature reveals that non-operative management of pediatric blunt solid organ injuries is associated with a low overall morbidity and mortality and does not result in increased length of stay, need for blood transfusions, bleeding complications or associated hollow viscous injuries as compared with operative management.
Guideline Inclusion Criteria:
- Pediatric trauma patients less than 15 years of age with a radiographically identified blunt liver, splenic or kidney injury at Nebraska Medicine.
Guideline Exclusion Criteria:
- Penetrating mechanism of injury
- Trauma patients 15 years of age and older (See separate adult guidelines for management of blunt solid organ injuries).
Diagnostic Evaluation:
- All trauma patients should be initially evaluated per ATLS guidelines with work-up as mechanism and clinical presentation dictate.
- Resuscitative measures should be initiated as clinical status/presentation dictates.
- Labs, imaging and additional tests should be obtained as clinical status/presentation dictates. (See “Guidelines For
- Imaging the Pediatric Trauma Patient”)
- If a patient is hemodynamically UNSTABLE, minimal testing/imaging should occur prior to interventions for hemorrhage control.
Practice Recommendations for Management:
- Once solid organ injury is suspected and/or confirmed, management of that injury is dictated largely by the clinical status of the patient.
- Initial Evaluation/Resuscitation:
-
- o Management of the hemodynamically UNSTABLE patient as evidence by moderate to severe tachycardia and/or hypotension
-
- Initial resuscitative measures should include the following:
-
- Placement of 2 large bore peripheral IVs (or equivalent central venous access as able)
- Bolus 20 ml/kg NS or LR (if blood not immediately available)
- Type and Cross 2-4 units PRBC (age and weight dependent)
- Transfuse uncrossed PRBC (or whole blood if age≥13 and available) 20mL/kg if hypotension unresponsive to crystalloid bolus.
- Obtain labs (VBG, CBC, PT/INR, etc.)
- Obtain eFAST.
- If eFAST is positive and/or patient remains UNSTABLE (i.e. tachycardia and hypotension persist) despite appropriate resuscitative measures:
-
- Activate the Massive Transfusion Protocol (MTP; see policy TX-36 “Massive Transfusion/Severe Coagulopathy/Emergency Release Blood” and PRO09 “Massive Transfusion in Trauma Guidelines”)
- Consider proceeding to OR for emergent laparotomy or IR for angioembolization.
-
-
- Initial resuscitative measures should include the following:
-
- o Management of the hemodynamically UNSTABLE patient as evidence by moderate to severe tachycardia and/or hypotension
-
- Management of the hemodynamically STABLE patient as evidenced by mild tachycardia without hypotension OR patients that become STABLE with initial resuscitative measures listed above (responders)
-
- Initial resuscitative measures as listed above should be performed as indicated based on clinical status of child. At minimum,
-
- Ensure and maintain IV access
- If fluid resuscitation not indicated, initiate maintenance IV fluids at weight-based rate, typically with NS or LR
- Send type and screen on all patients and consider type and cross 2 units PRBC depending on any patient with history of hemodynamic instability or those with higher grade injuries.
-
- Obtain multi-phase CT abdomen/pelvis with IV contrast as indicated by Imaging guidelines for pediatric trauma patients to diagnose/confirm presence of solid organ injury.
-
- If renal injury identified, also obtain a delayed imaging phase to assess for involvement of the collecting system.
-
- Determine appropriate management strategy based on grade of injury, presence of blush/contrast extravasation on imaging, and clinical status/injury burden of the patient.
- Consult urology for renal injuries with disruption/involvement of the collecting system
- Initial resuscitative measures as listed above should be performed as indicated based on clinical status of child. At minimum,
-
- Management of the hemodynamically STABLE patient as evidenced by mild tachycardia without hypotension OR patients that become STABLE with initial resuscitative measures listed above (responders)
-
- Disposition and cares following initial resuscitation:
-
- Admission Level of Care
-
- Decision for level of care should be based on clinical status of patient, not grade of injury, and is ultimately at the discretion of the trauma attending.
- ICU admission is indicated for the following patients
-
- Patients with current hemodynamic instability
- Patients with transient response to initial volume resuscitation
- Patients requiring intervention for hemorrhage control (i.e. IR angioembolization or operative intervention)
-
- Floor or Progressive Care should be considered for hemodynamically stable patients or those who become stable with sustained response to initial volume resuscitation.
-
- Activity
-
- Bedrest until vitals normal
- Once hemodynamically stable, activity as tolerated with no restrictions.
-
- Labs
-
- CBC on admission and Q6hr until vitals normal and Hb/HCT stable x 2
- Renal function should be monitored with BUN/CRT in setting of kidney injury.
-
- Diet and IV fluids
-
- NPO until vitals normal and Hb/HCT stable
- Once hemodynamically stable, regular diet as tolerated
- Continue maintenance IV fluids until meeting oral hydration goals
-
- Vital Signs
-
- Per unit protocol (ICU-q1hr, Progressive Care-q2hr, Floor-q4hr)
-
- Transfusion
-
- Unstable vitals after 20 mL/kg bolus of isotonic IVF
- Hemoglobin <7
- Signs of ongoing or recent bleeding
-
- Other Orders
-
- Strict Intake and Output (I&O)
- Pain control: Tylenol PRN, additional medications at discretion of trauma provider.
- Be mindful of using aspirin or ibuprofen/NSAIDs and limit use when able.
- VTE prophylaxis per “VTE prophylaxis in Trauma Patients” (PRO 10) guidelines
-
- Angioembolization or Operative Exploration
-
- Should be considered in patients with signs of ongoing bleeding despite blood product transfusion
- Angioembolization is NOT indicated for contrast blush on admission CT without unstable vitals
- Operative exploration may be indicated when additional procedures or information are needed
- Patients presenting with or who develop peritonitis should undergo operative exploration.
-
- Discharge Criteria
-
- Hb/HCT stable x 2
- Acceptable pain control with oral pain medications
- Tolerating diet
- Vital signs within normal limits
-
- Admission Level of Care
-
- Late Presentation
-
- Management of stable patients presenting 24-48 hours post injury is at the discretion of the trauma surgeon and may be based on the reason for finally seeking care (pain, ileus, etc.)
- Consider observation for serial exams vs discharge home with follow up and ground level activity.
- Hemoglobin rechecks are optional and based on clinical status
- Diet and activity restrictions are based on clinical status
-
- Repeat Imaging
-
- Routine follow-up imaging is not required. Decision to obtain repeat imaging should be based on clinical status of patient and at discretion of trauma attending.
-
- Post splenectomy vaccines
-
- Patients undergoing splenectomy as management of their splenic injury should obtain the following vaccines prior to discharge or at 14 days post-op (whichever date comes first)
-
- Quadravalent meningococcus (Menactra or Menomune)
- Pneumococcus (Pneumovax 23)
- H.influenzae B (HIB, ActHIB)
- Viral influenza vaccine (depending on time of year)
-
- Patients undergoing splenectomy as management of their splenic injury should obtain the following vaccines prior to discharge or at 14 days post-op (whichever date comes first)
-
Follow-up Care:
- Upon discharge from hospital, patient may return to school and resume ground level activities with restrictions as noted below:
-
- Grade of Injury + 2 weeks = # weeks of activity restrictions (for example: Grade 2 injury + 2 weeks = 4 weeks of activity restrictions)
- Activity restrictions include: no gym/PE, recess, playground play, sports, no wheeled equipment, manual labor, farm labor, large animal care, or other activities where one could fall/sustain blow to abdomen.
-
- Patient should be instructed to call trauma surgery with any increasing pain, pallor, dizziness, vomiting, worsening shoulder pain, GI bleeding or black tarry stools, or jaundice.
- Follow-up in trauma surgery clinic:
-
- Grade 1 and 2 injuries = 2 weeks or with a follow up phone call
- Grade 3, 4, or 5 injuries or those undergoing operative/IR intervention = 2 weeks.
-
- Routine follow-up imaging is not required. Repeat imaging should be based on clinician determination and clinical situation.
- For kidney injuries, refer to primary care provider/pediatrician for ongoing blood pressure monitoring.
Outcome Measures and Guideline Adherence:
- Time to OR/IR and interventions for all hemodynamically unstable patients and patients failing non-operative management will be tracked through our performance improvement process.
- Adult guidelines for management of blunt solid organ injuries
- Guidelines For Imaging the Pediatric Trauma Patient
- Massive Transfusion for Trauma Guidelines (PRO 10)
Key Contributors:
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Abby Josef, MD | Division of Acute Care Surgery, Faculty | Reviewer
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Coordinator | Reviewer
Last updated:
· August, 2024
References:
- Williams RF, Grewal H, Jamshidi R et al. Updated APSA guidelines for the management of blunt liver and spleen injuries. J Pediatr Surg. 2023; 58:1411-1418.
- Gates RL, Price M, Cameron DB, et al. Non-operative management of solid organ injuries in children: an American pediatric surgical association outcomes and evidence based practice committee systemic review. J Pediatr Surg.2019 Aug: 54(8):1519-1526.
- Linnaus MR, Langlais ME, Garcia NM, et al. Failure of nonoperative management of pediatric blunt liver and spleen injuries: A prospective Arizona-Texas-Oklahoma-Memphis-Arkansas Consortium Study. J Trauma and Acute Care. 2017; 82(4):672-679.
Appendix/supplemental materials:
- Updated American Pediatric Surgical Association (APSA) Blunt Liver/Spleen Injury Guidelines
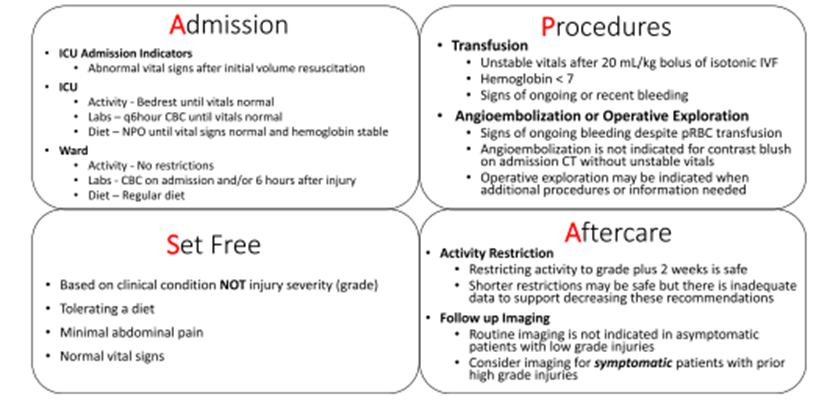
2. AAST Injury Grading Scales



Evaluation and Management of Non-Accidental Trauma (NAT) in Children at Nebraska Medicine
Purpose:
To provide guidance and a standardized approach for the initial evaluation, management and reporting of children with injuries concerning for abuse.
Background/Definitions:
Annually, nearly 1 million children are victims of child maltreatment in the United States. It is estimated that 1:4 children will experience some form of child abuse or neglect in their lifetime (1:7 in the past year) accounting for a total lifetime economic cost upward of $124 billion.
The Centers for Disease Control (CDC) defines child maltreatment as “any act or series of acts of commission or omission by a parent or other caregiver that results in harm, potential for harm, or threat of harm to a child.”
- Physical abuse, sexual abuse, and psychological abuse are types of abuse resulting from acts of commission.
- Acts of omission or neglect (e.g. delays in seeking treatment/care, inappropriate supervision, not using vehicle restraints) can worsen outcomes when the child is abused.
The Child Abuse Prevention and Treatment Act (CAPTA) establishes that standard legal definition of child abuse and neglect as “any recent act or failure to act on the part of the parent or caretaker which results in death, serious physical or emotional harm, sexual abuse or exploitation; or an act or failure to act, which presents an imminent risk of serious harm.”
In 2019, there were approximately 656,000 victims of child abuse and/or neglect in the United States as confirmed by state child protective service agencies.
- This equates to a national rate of 8.9 victims per 1,000 children in the population.
- Approximately 28% of victims were in the range of birth through 2 years old. 14.9% of all victims were younger than 1 year. The rate is highest for children younger than 1 year old at 25.7 per 1,000 children in the population of the same age.
Nationally, there were an estimated 1,840 children who died from abuse and neglect in 2019.
- This is a rate of 2.5 deaths per 100,000 children in the population. This is an approximate 10.8% increase from the 2015 estimation.
- Approximately 70% of all child fatalities were younger than 3 years old and close to half (45.4%) of all child fatalities were younger than 1 year old.
- The child fatality rates mostly decrease with age. Younger children are the most vulnerable to death as the result of child abuse and neglect.
- Nearly 80% of all fatalities involved one or both of the parents.
Sentinel injuries are injuries suspicious for physical abuse with rates of abuse high enough to warrant routine evaluation of abuse if the injury is present. Sentinel injuries can seem minor, and high level of suspicion and familiarity with high-risk injuries is critical for identification.
For the purposes of this guidelines, a non-ambulatory child is a child who cannot take two independent steps without the assistance of a person or inanimate object for support. Cruising is not considered ambulatory.
Guideline Inclusion Criteria:
· Children from newborn through adolescence (18 years and younger) with an injury concerning for physical abuse.
Guideline Exclusion Criteria:
· Injured patients age >18 years.
· Children involved in a motor-vehicle collision, regardless of age or ambulatory status, are excluded from this guideline.
Diagnostic Evaluation:
While any injury can be the result of physical abuse, there are NO injuries that are pathognomonic. The following are reasons to be concerned that injuries could be related to physical abuse (this list is not exhaustive):
History:
- No explanation or vague explanation of injury.
- An important detail of the explanation changes significantly.
- An explanation that is inconsistent with the pattern, age or severity of the injury or injuries.
- An explanation that is inconsistent with the child’s physical and/or developmental capabilities.
- Different caregivers provide different explanations for the injury or injuries, or a single caregiver provides history that changes over time.
- Unwitnessed injury
- Delay in seeking care for an injury.
- Prior ED visits for injury
- Domestic violence in home
- Premature infant (<37 weeks)
- Low birth weight/IUGR
- Presence of chronic medical conditions
Physical Exam:
- Age:
-
- All ages
- Non-ambulatory and non-verbal children are particularly vulnerable.
- All ages
-
- Bruising:
-
- Bruising in children <9 months of age
- Any bruise in non-ambulatory children
- Patterned bruising
- Extensive or clustered bruising
- Intraoral injuries (i.e. frenulum tears, pharyngeal injury) <9 months or non-ambulatory
- The TEN-4-FACESp Bruising Clinical Decision Rule is a highly sensitive and specific tool in identifying bruising that is concerning for abuse.
-
- “TEN”: bruising on Torso (chest, abdomen, back buttocks, GU region, hips), Ears or Neck.
- “FACES”: bruising on Frenulum, Angle of jaw, Cheek (fatty portion), Eyelids, Subconjunctivae
- “4”: “TEN-FACES” bruising on a child younger than 4 years old or any bruising in an infant 4 months or younger.
- “p”: Patterned bruising
-
-
- Burns
-
- Patterned burns (i.e. suspected cigarette burns or other burns with a particular shape)
- Stocking or glove immersion burns
- Burns in non-ambulatory patients.
-
- Fractures (Highly specific for physical abuse)
-
- Classic metaphyseal lesions (i.e. long bone fractures at the infant growth plate)
- Rib fractures (particularly posteromedial)
- Scapular or sternal fractures
- Spinous process fractures
-
- Fractures (moderately specific for physical abuse)
-
- Non-ambulatory child
- Digit fractures
- Complex skull fractures
- Vertebral body fractures/subluxations
- Epiphyseal separations
- Fractures of varying ages
- Multiple fractures, especially bilateral
- Pelvic fractures
-
- Abusive head trauma (AHT)
-
- Vague presenting signs and symptoms may be associated with AHT. AHT should be considered in the differential diagnoses of young children with non-specific history of/findings such as:
-
- Altered mental status (lethargy, fussiness)
- Seizures/seizure-like activity
- Vomiting
- Cyanosis
- Marked change in muscular tone
- Apnea/reported apnea
- Decreased or irregular breathing
- Enlarging head circumference
- Diffuse intracranial hemorrhage
- Mixed density intracranial hemorrhage
- Bilateral intracranial hemorrhage
- Intracranial hemorrhage with altered mental status
- Intracranial hemorrhage with no history of trauma
- Intracranial hemorrhage with ischemic parenchymal injury
- Intracranial hemorrhage with spinal/paraspinal hemorrhage and/or spinal ligamentous injury
- Intracranial hemorrhage with other evidence of injury (cutaneous, skeletal, intraabdominal)
- Parenchymal injury (contusion, tear, diffuse axonal injury)
- Diffuse cerebral edema without identifiable intracranial hemorrhage on head CT.
- Retinal hemorrhages (those that are too numerous to count/diffuse in one or both eyes, present in multiple layers of retina, and extending into the retinal periphery are most concerning)
-
- Vague presenting signs and symptoms may be associated with AHT. AHT should be considered in the differential diagnoses of young children with non-specific history of/findings such as:
-
Practice Recommendations for Management:
Injured children presenting to Nebraska Medicine should be initially evaluated and managed in accordance with ATLS guidelines. Clinicians should first ensure the child is medically stable. If during the assessment concerns for physical abuse/non-accidental trauma are raised, the following additional work-up should ensue as early as practical based on the severity of injuries and clinical status of the child.
Initial Management:
Children 0 to 24 months meeting at least one of the following criteria:
- Less than 24 months with an injury concerning for abuse
- Non-ambulatory with a skeletal fracture
- Less than 12 months with a skeletal fracture
- Thorough history
-
- Detailed description of illness/injury from the time the child was last well. Include any history of trauma as well as circumstances leading to the discovery of the injury.
- It is important to document the history as early as practical in the process.
- Note inconsistencies and changing histories as well as delays in care.
- Full medical history of the child (birth history, prior hospitalizations/ED visits/injuries/wellness visits), development (normal vs abnormal) and social history (all caregivers and other who live in household, domestic violence prior CPS/police contact)
-
- Head to toe physical assessment
-
- Review vital signs, neurologic exam, thorough skin assessment including ears and frenula.
- Detailed documentation of all the abnormal findings.
-
- Social work consultation.
-
- Social worker can assist in obtaining a detailed psychosocial history and assessment from family/caregivers, assist in communication with law enforcement and CPS as indicated, and communication with the Children’s Advocacy Team.
-
- Children’s Advocacy Team (CAT) consultation (Most consults can be called during regular business hours, M-F, 8am-5pm).
- Make report to Child Protective Services (CPS).
-
- Report may be made by any provider/person involved in child’s care who has reasonable cause to believe that the child subjected to abuse or neglect. It is a criminal offense to NOT report if abuse/neglect is suspected.
-
- CPS report number should be documented in a progress note in the patient’s electronic medical record.
-
- Trauma attending must be notified that a CPS report has been filed.
- Inform parents/caregivers of child if a CPS referral has been filed and should ideally be done by trauma attending or next most senior provider or social worker involved in child’s care.
- Report may be made by any provider/person involved in child’s care who has reasonable cause to believe that the child subjected to abuse or neglect. It is a criminal offense to NOT report if abuse/neglect is suspected.
-
- If child is felt to be in imminent danger, involve law enforcement/police (based on location of where the alleged abuse/neglect occurred)
- Skeletal survey
- Transaminase levels (AST/ALT) and serum lipase
- Head CT without contrast
-
- All children less than 6 months
- Children 6-12 months with neurologic abnormality and/or external evidence of head injury.
- See “abusive head trauma” (AHT) section
-
- Photo documentation in the electronic medical record of all external injuries, including burns, if the injury is concerning for abuse.
Children >24 months with an injury concerning for abuse will receive the following:
- Thorough history
-
- Detailed description of illness/injury from the time the child was last well. Include any history of trauma as well as circumstances leading to the discovery of the injury
- It is important to document the history as early as practical in the process.
- Note inconsistencies and changing histories as well as delays in care.
- Full medical history of the child (birth history, prior hospitalizations/ED visits/injuries/wellness visits), development (normal vs abnormal) and social history (all caregivers and other who live in household, domestic violence prior CPS/police contact)
-
- Head to toe physical assessment
-
- Review vital signs, neurologic exam, thorough skin assessment including ears and frenula.
- Detailed documentation of all the abnormal findings.
-
- Social work consultation.
-
- Social worker can assist in obtaining a detailed psychosocial history and assessment from family/caregivers, assist in communication with law enforcement and CPS as indicated, and communication with the Children’s Advocacy Team.
-
- Children’s Advocacy Team (CAT) consultation (Most consults can be called during regular business hours, M-F, 8am-5pm).
- Make report to Child Protective Services (CPS).
-
- Report may be made by any provider/person involved in child’s care who has reasonable cause to believe that the child subjected to abuse or neglect. It is a criminal offense to NOT report if abuse/neglect is suspected.
-
- CPS report number should be documented in a progress note in the patient’s electronic medical record.
-
- Trauma attending must be notified that a CPS referral has been filed.
- Inform parents/caregivers of child if a CPS referral has been filed and should ideally be done by trauma attending or next most senior provider or social worker involved in child’s care.
- Report may be made by any provider/person involved in child’s care who has reasonable cause to believe that the child subjected to abuse or neglect. It is a criminal offense to NOT report if abuse/neglect is suspected.
-
- If child is felt to be in imminent danger, involve law enforcement/police (based on location of where the alleged abuse/neglect occurred).
- Skeletal survey—recommended only in children up to 5 years on a case by case basis:
-
- i.e. unconscious patient, non-verbal patient, non-ambulatory patient, or inadequate exam.
-
- Transaminase levels (AST/ALT) and serum lipase
-
- Recommended with multiple or severe injuries or with concern for abdominal or pelvic trauma
-
- Head CT without contrast
-
- Children with neurologic abnormality and/or external evidence of head injury.
- See “abusive head trauma” (AHT) section
-
- Photo documentation in the electronic medical record of all external injuries, including burns, if the injury is concerning for abuse.
Additional Laboratory and Diagnostic Evaluation
Additional labs, imaging and testing may be obtained as indicated specific to the injury or individual circumstances. If there are questions regarding what additional testing is needed, please discuss with the CAT.
- Laboratory:
-
- Urine and serum toxicology
-
- Concern for ingestion
- Evidence of neurologic abnormality
-
-
- If CT head is obtained due to concerns for abusive head trauma (fussiness, vomiting, seizures, brief resolved unexplained event (BRUE), etc.), urine and serum toxicology is also indicated.
-
-
- Report or suspicion of substance abuse in caregiver, either by history or presentation.
-
- CBC, PT/INR, PTT, vW panel, Factor VIII and IX levels
-
- Intracranial hemorrhage (ICH) concerning for abusive head trauma
- Consider in patient with diffuse cerebral edema without identifiable ICH on CT head.
- Bruising concerning for inflicted injury
-
-
- Factors which increase the likelihood of abusive bruising include:
-
- <9 months of age
- Non-ambulatory child
- Bruising which meets the TEN-4-FACESp Bruising Clinical Decision Rule Criteria.
-
- Factors which increase the likelihood of abusive bruising include:
-
-
- Other injuries associated with bleeding
-
- Solid organ injury concerning for inflicted trauma
-
- Children with clinically significant bleeding
-
- Bone abnormality evaluation (25-hydroxy-Vit D, bioactive PTH, Alkaline Phosphatase, Calcium, Phosphorus levels)
-
- Recommended in children with >1 skeletal fracture concerning for abuse
- Recommended in children with a skeletal fracture(s) with radiographic concern for osteopenia or metabolic bone disease
- Special consideration (after discussion with CAT team)
-
- Ionized calcium
-
- Children with hypoalbuminemia or who appear malnourished or concern for failure to thrive
-
- Serum copper, ceruloplasmin, and vitamin C
-
- Consider in children at risk for scurvy or copper deficiencies in the setting of metaphyseal irregularities
-
- Ionized calcium
-
-
- Urine and serum toxicology
-
- Imaging:
-
- CT Abdomen/Pelvis with IV contrast
-
- Abnormal abdominal exam such as bruising, distention, tenderness, vomiting
- Consider with >10 RBCs per HPF on urinalysis
- ALT or AST >80 mg/dL or Lipase >100
-
- Or admit to trauma service for observation and serial abdominal exams.
-
- May be indicated as per CAT.
-
- MRI/MRV brain with and without contrast
-
- May be indicated with ICU to further delineate injury, per Trauma, Neurosurgery, or CAT.
-
- MRI cervical, thoracic, lumbar spine without contrast
-
- May be indicated with ICU to further delineate injury, per Trauma, Spine (neurosurgery or orthopedic surgery), or CAT.
-
- CT Abdomen/Pelvis with IV contrast
-
Consultation
Admission/Disposition
- For children with injuries requiring admission for medical or surgical management, the TRAUMA SERVICE will be the primary admitting service with CAT, Pediatrics (either pediatric critical care or pediatric co-management team depending on level of care), and subspecialty consultation as indicated.
-
-
-
- The family should be informed of the plan to involve CAT if applicable.
-
- Isolated injuries with no ongoing concerns for abuse may be admitted to the appropriate surgical subspecialty as appropriate (i.e. orthopedics, neurosurgery, etc.).
- Other considerations:
-
- Non-surgical admissions
-
-
-
- In general, children with traumatic injury felt to be secondary to abuse should NOT be admitted to a non-surgical service unless it is felt to be in the best interest of the patient (i.e. medically complex with minor traumatic injury not requiring intervention). If the child is being admitted to a non-surgical service, the attending trauma surgeon must explicitly document why he/she feels the child would be better served by a non-surgical service.
-
-
-
- Children admitted for a medical/non-traumatic diagnosis (i.e. seizures, failure to thrive, etc.) and are later suspected or discovered to have a traumatic injury should have a trauma consultation as soon as the injury is discovered. Trauma team consultation should not be delayed for a sub-specialty surgical consult.
- Non-surgical admissions
-
-
-
- For children with injuries that do NOT require admission for medical/surgical management but have reasonable concern for abuse,
-
- Consult the ED social worker who will email CAT (CATRN@childrensnebraska.org) with details of the case for review.
-
- CAT will contact the family if follow-up is indicated.
- Do not instruct the family to call CAT.
-
- CPS report is made.
-
- Request CPS involvement for discharge. If/when a safe disposition has been established by CPS and agreed upon by ED/Trauma/SW providers, the patient may be discharged from the ED.
- If a safe disposition cannot be developed by CPS in the ED in a timely fashion, the patient will be admitted to the Trauma Service for observation until a plan is in place.
-
- Consult the ED social worker who will email CAT (CATRN@childrensnebraska.org) with details of the case for review.
-
- For children with injuries that do NOT require admission for medical/surgical management, but provider is unsure if there is reasonable concern for abuse,
-
-
-
- During normal business hours (M-F, 8a-5p), provider to call CAT at 402-955-6250 or by calling the Children’s Physician Priority line at 855-850-KIDS (5437) and asking for provider on call for CAT.
- If after hours/weekends, provider to call the on-call CAT provider by calling the Children’s Physician Priority line at 855-850-KIDS (5437)
- ED social worker emails CAT (CATRN@childrensnebraska.org) with details of case for review.
- Provider is to call the on-call CAT provider to discuss and develop a plan.
-
- CAT will contact the family if follow-up is indicated.
- Do not instruct the family to call CAT.
-
- CPS report at discretion of providers/SW/CAT
-
- If CPS is notified, request CPS involvement for discharge. Once a safe disposition has been established by CPS and agreed upon by ED/Trauma/SW providers, the patient may be discharged from the ED.
- If a safe disposition cannot be developed by CPS in the ED in a timely fashion, the patient will be admitted to the Trauma Service for observation until a plan is in place.
-
-
-
-
***Please see algorithm from Pediatric Trauma Society and Western Trauma Association below as an additional guide to what is stated above***
Reminders:
- Do not accuse or treat families/caregivers any differently than others. Keep the discussion neutral and patient centered/focused.
- Discuss suspected abuse reporting requirements with family/caregivers.
- Consider having the senior staff (APP or attending) or senior resident as the primary providers for these cases.
Important phone numbers:
- Nebraska Child Protective Services Hotline: 800-652-1999
- Iowa Department of Human Services Hotline: 800-362-2178
- Children’s Advocacy Team: 402-955-6250
- Children’s Social Work Department: 402-955-5418
- Children’s Physician Priority Line: 855-850-KIDS (5437)
- Omaha Police Department, Child Victim/Sexual Assault Unit: 402-222-5636 or 402-444-4135
- Bellevue Police Department: 402-293-3100
- Children’s Advocacy Team (CAT) email: CATRN@childrensnebraska.org
Follow-up Care:
- Injured children may follow-up with trauma and consulted subspecialty teams as indicated for injuries.
- Children’s Advocacy Team as indicated for all aspects of care related to and sequela of abuse/neglect.
Outcome Measures and Guideline Adherence:
- All cases of traumatic injury secondary to non-accidental trauma will be reviewed by the pediatric trauma medical director and pediatric trauma program manager at a primary level. Additional levels of review will be performed on a case-by-case basis and involve consultant teams and Child Advocacy Team as needed.
- Nebraska Medicine Policy PE02, “Identification of Abuse or Neglect”
- Nebraska Medicine Policy PE 03, “Reporting of Abuse, Neglect, or Injury”
Key Contributors:
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principal Author
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Coordinator | Co-Author
- Suzanne Haney, MD, MS, FAAP | Division Chief, Child Abuse Pediatrics | Reviewer
Last updated:
· June 2024
References:
- Prevention CDCa. Child Maltreatment: Fact-Sheet. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention; 2014. http://www.cdc.gov/ncipc/factsheets/cmfacts.htm.
- Prevention CDCa. Child Abuse and Neglect Prevention. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention; 2017. http://www.cdc.gov/violenceprevention/childmaltreatment/.
- Finkelhor D, Turner HA, Shattuck A, Hamby SL. Violence, crime, and abuse exposure in a national sample of children and youth: an update. JAMA Pediatr. 2013;167(7):614-21.
- Leeb RT, Paulozzi L, Melanson C, et al. Chile Maltreatment Surveillance: Uniform Definitions for Public Health and Recommended Data Elements, Version 1.0. In: Center for Disease Control and Prevention NCflPaC, editor. Atlanta, GA. 2008.
- U.S. Department of Health and Human Services ACYF, Administration on Children, Youth and Families, Children’s Bureau. Child Maltreatment 2016. Washington, D.C.: Children’s Bureau (Administration for Children, Youth, and Families, Administration for Children and Families) of the U.S. Department of Health and Human Services, 2018.
- Berger RP, Lindberg DM. Early recognition of physical abuse: Bridging the gap between knowledge and practice. J Pediatr. 2018; 204:16-23.
- Pierce MC, Kaczor K, Aldridge S, O’Flynn J, Lorenz DJ. Bruising characteristics discriminated physical child abuse from accidental trauma. Pediatrics, 2010: 125(1); 67-74.
- Pierce MC, Kaczor K, Lorenz DJ, Bertocci G, Fingarson AK, Makoroff K, Berger RP. Validation of a clinical decision rule to predict abuse in young children based on bruising characteristics. JAMA Netw Open. 2021; 4(4):e215832.
- Kleinman PK, ed. Diagnostic Imaging of Child Abuse. 3rd ed. Cambridge University Press, 2015.
- ACS Trauma Quality Programs Best Practice Guidelines for Trauma Center Recognition of Child Abuse, Elder Abuse, and Intimate Partner Violence. abuse_guidelines.pdf (facs.org) November, 2019.
- Burg B, Dougherty M, Snyder K, Shanghvi D, Naiditch J, et al. Dell Children’s Medical Center, Evidence-based Outcome Center, “Evaluation for Occult Injury Guideline”. February, 2022.
- Rosen NG, Escobar MA, Brown CV, et al. Child physical abuse trauma evaluation and management: A Western Trauma Association and Pediatric Trauma Society critical decisions algorithm. J Trauma Acute Care Surg.2021; 90(4): 641-651.
Western Trauma Association and Pediatric Trauma Society complete algorithm for the evaluation and management of children with Child Physical Abuse (CPA) trauma.



Guidelines for Imaging the Pediatric Trauma Patient
Purpose:
These guidelines are meant to help guide the provider’s decision-making regarding imaging of the pediatric trauma patient during the initial trauma evaluation.
Background/Definitions:
There is considerable agreement that diagnostic imaging, particularly with computed tomography (CT), results in significant radiation exposure in children. In addition, while the precise implications of this radiation exposure have not been defined, there is consensus that it is associated with a low, but real, increase in the long-term development of fatal malignancy. Children are particularly sensitive to the effects of radiation given their small size (increase dose per unit area) and the long latent times between exposure and the resultant cancer. Exposure to diagnostic radiation in children has increased dramatically in recent years with increasing use of CT. The primary indication for these scans is for the evaluation of trauma and appendicitis. Both the American Academy of Pediatrics and the American Pediatric Surgical Association have recently published statements encouraging their members to adhere to the ALARA principle, “As Low as Reasonably Achievable,” when obtaining imaging in pediatric patients (1, 2).
While the use of CT to diagnosis injuries in children has been increasing, there is a growing body of literature to suggest that CT is not required for routine evaluation resulting in the creation of several prediction rules to help guide the physician on what type and when imaging might be indicated to adequately assess the pediatric trauma patient.
In light of this evidence, we recommend adherence to the ALARA principle when imaging pediatric trauma patients. Specifically, we recommend:
- Avoidance of the use of protocols which automatically result in the performance of multiple CT scans (i.e. head, cervical spine, chest, and abdomen and pelvis) in pediatric patients.
- Avoid further CT imaging once the decision to transfer to definitive care is made, unless the accepting institution specifically requests a scan prior to transfer.
- All CT scans on children should be performed using “pediatric” weight-based dose-reduction protocols per Nebraska Medicine radiology procedures.
- Accepting institution should avoid repeating scans unnecessarily and when possible utilize alternative imaging strategies.
Guideline Inclusion Criteria:
- Pediatric trauma patients less than 19 years of age.
Guideline Exclusion Criteria:
- Patients 19 years of age and older.
Practice Recommendations for Management:
Initial Assessment:
- Pediatric trauma patients should be assessed per ATLS guidelines on arrival to ED.
-
- Chest x-ray and pelvis x-ray should be used as adjuncts to the primary survey as indicated by patient’s clinical status and mechanism of injury.
-
- Can consider not obtaining chest x-ray in low-grade mechanisms of injury if patient is able to be observed following injury.
- Chest x-ray should be obtained in setting of high-grade mechanism of injury, abnormal physiology and/or intubation.
-
- Routine use of eFAST in pediatric trauma patients is not supported by literature due to decreased sensitivity and specificity in pediatric patients when compared to adults. eFAST, however, may still be beneficial in decision making for certain clinical scenarios (i.e. hypotensive, blunt trauma patient) and should be utilized at the discretion of the trauma provider.
- Chest x-ray and pelvis x-ray should be used as adjuncts to the primary survey as indicated by patient’s clinical status and mechanism of injury.
-
- The use of a skilled child life specialist to help minimize the injured child’s fear and anxiety can markedly reduce the amount of sedation required during the initial assessment and subsequent imaging. Their liberal use is recommended when available.
- If the child requires sedation to complete the trauma assessment or imaging, experienced pediatric personnel with credentials to administer sedation are recommended.
Additional Imaging:
- Pediatric Head Imaging
-
- Decision to obtain CT imaging of the head in pediatric trauma patients should be based on PECARN (Pediatric Emergency Care Applied Research Network) criteria which are as follows:
-


-
-
- Routine repeat CT head is not recommended but should be considered if there is a decline in GCS/worsening neurological exam, in sedated patients who cannot be evaluated, or at discretion of neurosurgical team.
-
- Pediatric Cervical Spine Imaging:
-
- The asymptomatic child with a reliable normal exam does not require imaging to clear the cervical spine, regardless of mechanism.
- The overall incidence of c-spine injury in children is low (<1%). However, may be seen in up to 30% of pediatric TBI patients and overall incidence of approximately 15% in non-accidental trauma.
- Injury is most difficult to assess in the 2-5 year age group.
- The risk for a higher anatomical injury is greater the younger the child.
-
- Younger children are more likely to suffer ligamentous injury than fracture.
-
- Canadian C-spine Rule (CCR) and NEXUS criteria are standard for adults but are not sensitive or specific enough to be used for children <10 years of age.
- Decision to obtain c-spine imaging in pediatric patients following blunt trauma should be based on PECARN criteria or the AAST scoring system for patients less than 3 years of age.
-
- PECARN Criteria:
-
- Consider CT c-spine in the following:
-
- GCS 3-8 or AVPU =U
- Abnormal airway, breathing, or circulation
- Focal neurologic deficits
-
- Consider c-spine x-rays in the following:
-
- GCS 9-14, AVPU=V or P, or other signs of altered mental status
- Self-reported neck pain or neck tenderness on examination
- “substantial” head or torso injury (“substantial” injuries defined as warranting inpatient observation or surgical intervention such as skull fracture, pneumothorax, solid organ injury, spine fracture, pelvic fracture)
-
- If none of the above listed risk factors are present, then consider clinical clearance.
- Consider CT c-spine in the following:
-
- PECARN Criteria:
-
-

-
-
-
-
- AAST scoring system for patients less than 3 years:
-
- Criteria examined:
-
- GCS<14 = 3 points
- GCS (eye criterion) =1 = 2 points
- Motor vehicle crash (MVC), fall from height>10ft, intentional injury as mechanism of injury = 2 points
- Age 24-36 months = 1 point
-
- Scoring:
-
- 0-1 = no imaging
- 2-4 = imaging a clinician discretion
- 5-8 = imaging (CT c-spine) recommended
-
- Criteria examined:
-
- Non-contrast CT c-spine is generally the recommended study of choice for evaluating the cervical spine, as the sensitivity and specificity of c-spine x-rays is inconsistent.
- Consider MRI c-spine if neck pain is out of proportion to CT results or concerned for spinal cord injury or ligamentous injury.
- SCIWORA—(spinal cord injury without radiographic abnormality) term used to descript neurologic deficit in the absence of findings on plain radiographs or CT scan. MRI is recommended next, but up to 40% of affected patients do not have an injury detected by MRI.
- AAST scoring system for patients less than 3 years:
-
-
-
- Screening for Blunt Cerebrovascular Injury (BCVI) in pediatric trauma patients
-
- Routine use of CTA neck for BCVI screening in pediatric trauma patients should be avoided due to the associated radiation exposure and low incidence of BCVI in the population.
- The McGovern Score should be utilized to help determine if a patient should undergo CTA neck for screening of BCVI.
-
- A score of ≥3 points is high-risk for BCVI and CTA neck should be performed.
-
- Routine use of CTA neck for BCVI screening in pediatric trauma patients should be avoided due to the associated radiation exposure and low incidence of BCVI in the population.
-

- Pediatric Chest Imaging
-
- X-ray
-
- Chest x-ray is recommended in the initial evaluation of all pediatric trauma patients, regardless of age, in the presence of abnormal physiology, high-grade mechanism of injury, or intubation.
-
- Ultrasound
-
- a pericardial US should be considered if the chest x-ray reveals a normal mediastinum, but other injuries (e.g. rib fractures, sternal fracture, scapula fracture, pneumothorax or contusion) are present.
-
- CT scan
-
- CT chest should be used selectively in the evaluation of pediatric trauma patients to reduce unnecessary imaging.
-
- A CT chest is reported to have no impact on management of the pediatric trauma patient with absent or minor abnormalities on chest x-ray (ex. simple pneumothorax, simple hemothorax, pulmonary contusion, or isolated rib fractures).
- if indicated, a CT chest should be obtained with IV contrast.
- A CT chest is reported to have no impact on management of the pediatric trauma patient with absent or minor abnormalities on chest x-ray (ex. simple pneumothorax, simple hemothorax, pulmonary contusion, or isolated rib fractures).
-
- A CT chest is recommended for children with abnormal mediastinal contour of an age-appropriate shaped chest, more significant abnormalities on chest x-ray or an abnormal pericardial US.
- CT chest should be used selectively in the evaluation of pediatric trauma patients to reduce unnecessary imaging.
-
- X-ray
-

- Pediatric Abdominal Imaging
-
- Ultrasound
-
- Routine use of eFAST in pediatric trauma patients is not supported by literature due to decreased sensitivity and specificity in pediatric patients when compared to adults.
- eFAST, however, may still be beneficial in decision making for certain clinical scenarios and IS RECOMMENDED for the assessment of pediatric trauma patients presenting in shock (i.e. hypotensive), when CT is not available or feasible or at the discretion of the trauma provider.
-
- CT scan
-
- The PECARN Prediction Rule or the Streck Criteria should be applied to pediatric patients presenting after high-energy blunt mechanism or with blunt abdominal trauma to help determine when CT scans are indicated
- CT abdomen/pelvis should be used selectively in the evaluation of pediatric trauma patients to reduce unnecessary imaging.
- If indicated, a CT abdomen/pelvis should be obtained with IV contrast in at least 2 phases (typically arterial and venous) to help identify and distinguish active hemorrhage.
-
- The portal venous phase is optimal for evaluation of visceral parenchyma.
- delayed excretory phase images are essential for the evaluation of genitourinary trauma (e.g. renal collecting system or bladder injuries) and should be considered in the setting of gross hematuria or microscopic hematuria with hypotension.
- oral contrast is typically not indicated unless there is concern for duodenal injury.
-
-
- Ultrasound
-

- Pediatric Thoracic and Lumbar Spine imaging
-
- Routine imaging of the spine based on mechanism of injury alone is generally not recommended.
- AP and lateral x-rays are indicated for physical examination findings or symptoms.
-
- Obesity/body habitus and other factors may affect the quality of the x-rays.
-
- If a patient is undergoing CT chest, abdomen or pelvis, obtain thoracic and lumbar spine reconstructions.
- If patient has a neurologic deficit/abnormality, consider obtaining MRI for evaluation of the spine.
-
- Pediatric Orthopedic Injury Imaging
-
- Plain x-rays of the injured area are the standard for initial assessment of possible orthopedic injury.
-
- Use “rule of twos” when ordering x-rays:
-
- Two views – at least obtain an AP and lateral view of the injured limb/area
- Two joints—consider obtaining x-rays of the joints above and below the site of injury to rule out an potential associated fracture or dislocation.
- Two limbs—after consultation with orthopedic surgery, a request for x-rays of the injured and non-injured limb is made to aid in evaluation/diagnosis of certain injuries.
- Two times—pre- and post- reduction x-rays are needed to assess the adequacy of any fracture or dislocation manipulation or reduction.
-
- Use “rule of twos” when ordering x-rays:
-
- CT is not indicated for the routine evaluation of many orthopedic injuries and should only be ordered following consultation with orthopedic surgery when needed for pre-operative planning of complicated fractures.
- MRI of affected area can be helpful in identifying occult injuries or further evaluating certain injuries. MRI is rarely indicated in the acute setting and should be considered following consultation with orthopedic surgery.
- Plain x-rays of the injured area are the standard for initial assessment of possible orthopedic injury.
-
- Imaging for pediatric extremity vascular injury
-
- Extremity vascular imaging in the pediatric population is similar to that of adults.
- CTA of affected extremity remains the gold standard to evaluate for vascular injury in extremity trauma in the hemodynamically stable patient without hard signs of vascular injury.
-
- Vasospasm cannot be reliably diagnosed by CTA and may require catheter angiography.
-
- Hard signs of vascular injury
-
- Bruit/thrill
- Active/pulsatile hemorrhage
- Pulsatile/expanding hematoma
- Signs of limb ischemia and/or compartment syndrome including the 5 “P’s” (pallor, paresthesia, pulse deficit, paralysis, and pain on passive extension)
- Diminished or absent pulses
-
- Soft signs of vascular injury
-
- Hypotension or shock
- Neurologic deficit
- Nonexpanding/nonpulsatile hematoma
- Proximity of wound to major vascular structures

-
-
Outcome Measures and Guideline Adherence:
- All pediatric trauma patients will be reviewed for imaging obtained and adherence to above stated imaging guidelines. Deviations from guidelines will be investigated further for with intervention and education as needed when trends or opportunities for improvement are identified.
- Adherence to guidelines will be reported in the Pediatric Performance Improvement Process (PIPs) meeting.

Key Contributors:
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Abby Josef, MD | Division of Acute Care Surgery, Faculty | Reviewer
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Coordinator | Co-Author
-
Megan Samland, DNP, APRN-NP, AGACNP-BC, FNP-BC | Division of Acute Care Surgery, APP | Co-Author
Last updated:
· February, 2026
References:
- Brody, Frush, Huda, Brent, and the Section of Radiology, “Radiation Risk to Children from Computed Tomography,” Pediatrics 120: 677-682, 2007.
- Rice, Frush, Farmer, Waldhausen, and the APSA Education Committee, “Review of radiation risks from computed tomography: essential for the pediatric surgeon. J Pediatr Surg 42: 603-7, 2007.
- Kupperman N, Holmes JF, Dayan PS, et al. Pediatric Emergency Care Applied Research Network (PECARN). Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet. 2009; 374(9696): 1160-70.
- Pieretti-Vanmarcke R, Velmahos GC, Nance ML, et al Clinical clearance of the cervical spine in blunt trauma patients younger than 3 years: A multi-center study of the American Association for the Surgery of Trauma. J Trauma 2009; 67(3):543-550.
- Markel, Kumar, Koontz, et al. The utility of computed tomography as a screening tool for the evaluation of pediatric blunt chest trauma. J Trauma 67:23-28, 2009.
- Singh, Kalra, Moore, et al. Dose reduction and compliance with pediatric CT protocols adapted to patient size, clinical indication, and number of prior studies. Radiology 252: 200-208, 2009.
- Chwals, Robinson, Sivit, et al. Computed tomography before transfer to a level I pediatric trauma center risks duplication with associated increased radiation exposure. J Pediatr Surg 43 2268-2272, 2008.
- ACS Trauma Quality Programs Best Practice Guidelines in Imaging. imaging_guidelines.pdf (facs.org) October, 2018.
- Holmes JF, Yen K, Ugaldge IT, et al. PECARN prediction rules for CT imaging of children presenting to the emergency department with blunt abdominal or minor head trauma: a multicentre prospective validation study. Lancet Child Adolesc Health. 2024 May; 8(5):339-347.
- Leonard JC, Harding M, Cook LJ, et a.l PECARN prediction rule for cervical spine imaging of children presenting to the emergency department with blunt trauma: a multicentre prospective observational study. Lancet Child Adolesc Health. 2024 Jul; 8(7):482-490.
- Chung S, Mikrogianakis A, Wales PW, et al. Trauma Association of Canada Pediatric Subcommittee National Pediatric Cervical Spine Evaluation Pathway: Consensus guidelines. J Trauma. 2011; 70(4):873-884.
- Nigrovic LE, Rogers AJ, Adelgais KM, et al. Pediatric Emergency Care Applied Research Network (PECARN) Cervical Spine Study Group. Utility of plain radiographs in detecting traumatic injuries of the cervical spine in children. Pediatr Emerg Care. 2012; 28(5):426-432.
- Herbert JP, Venkataraman SS, Turkmani AH, Zhu L, et al. Pediatric blunt cerebrovascular injury: The McGovern screening score. J Neurosurg Pediatr. 2018; 21(6):639-649.
- Venkataraman SS, Herbert JP, Ravindra VM, et al. Multi-center validation of the McGovern Pediatric Blunt Cerebrovascular Injury Screening Score. J Neurotrauma. 2023; 40(13-14):1451-1458.
- Emergency Medical Services for Children Innovation and Improvement Center (EIIC) (2025). EIIC: Best Practices in Pediatric Trauma Imaging. https://emscimprovement.center/education-and-resources/peak/multisystem-trauma/imaging/
Indications to Consult Pediatric Critical Care
Purpose
The trauma service frequently encounters critically injured pediatric patients (aged 18 years or less) that require admission to the pediatric ICU for resuscitation and management of injuries. To optimize outcomes, assistance in resuscitation and care of these critically injured pediatric trauma patients is often enhanced by the involvement of pediatric critical care medicine (PCCM). As a result, collaboration between the trauma and pediatric critical care services is essential and the following guidelines are meant to outline when pediatric critical care should be consulted to assist in the management and care of injured children requiring admission to the pediatric ICU.
Indications to Consult Pediatric Critical Care Medicine (PCCM)
- All injured children requiring ICU or progressive care level admission, age 12 years and younger.
- Injured children with pre-existing or congenital conditions that would benefit from the expertise of a pediatric intensivist, age 18 and under.
- At the admitting trauma attending’s discretion.
Consulting Pediatric Critical Care Medicine (PCCM)
- The trauma service will contact the PCCM provider listed “on call” on PerfectServe for consultation/handoff if the patient is being admitted/transferred to the PICU.
- The trauma service will need to place an “Inpatient consult to pediatric critical care” consult order. Reason for consultation can be “medical co-management.”
-
- Use the PEDATRIC TRAUMA ADMISSION – 12 years old and younger order set. Select “Inpatient consult to Pediatric Critical Care Medicine” order under Physician Consults-Academic section followed by also selecting the associated order “Notify physician/provider—Please contact Pediatric Critical Care Medicine regarding invasive/non-invasive respiratory support, sedation, CRRT settings, and adjustment of existing pressors. For ALL OTHER CONCERNS, contact the TRAUMA TEAM” located in the Vital Signs/Notify Physician section.
-
- Direct verbal communication should occur between the trauma and PCCM providers caring for the patient on admission/transfer to the pediatric ICU and with any change in patient status/condition.
General Requirements
- When consulted, PCCM will assist with management until the patient is transferred out “critical care” status. At which time, a pediatric co-management consult should be considered.
- The trauma service will serve as the patient’s PRIMARY team. As a result, the trauma surgeon/team must be kept informed of and concur with all major therapeutic and management decisions when care is being provided by the PCCM team. 
-
-
- A minimum of daily communication between the trauma and PCCM teams should occur to discuss patient care plans.
- The trauma and PCCM teams will round daily on patients and write daily progress notes.
- If it is determined that the trauma team should no longer be the primary team on a patient (i.e. transferring to another pediatric service), the trauma service will be responsible for finding an accepting primary service, placing the necessary orders for transfer, communicating plans for transfer with PCCM team, and documentation of transfer to include patient’s current status/injury management/follow-up/transfer details/etc. (“sign off” note)
-
-
- If PCCM is consulted, adult critical care surgery (CCS) services will not be involved in the care of the pediatric trauma patient unless specifically requested by the trauma service.
Responsibilities of Pediatric Critical Care Medicine (PCCM) Team
- Management of vasopressors and other continuous infusions (i.e. sedation, analgesia, etc.).
- Management of ventilator.
- Placement and management of central venous catheters, PICC line, and arterial lines (in collaboration with trauma team).
- Medication management, review, and reconciliation.
-
- Including guidance for dosing by weight and age (in collaboration with pediatric pharmacy).
- including electrolyte replacement, glucose management, seizure management, and antibiotics (in collaboration with the trauma team).
-
- Ensuring adjunctive modalities are used for delirium prevention, pain control, and refusal of PO/medications by child or parent.
- Discrepancies between orders (in collaboration with the trauma team).
- Management of pre-existing/chronic medical conditions.
- Responding to all acute decline and decompensation events.
-
- In addition, will contact the trauma team to provide updates on significant events or status changes.
-
- Screening and interventions for non-accidental trauma, as deemed necessary (in collaboration with the trauma team).
- Counseling and guidance of injury prevention, including causative injury and other preventative measures, to patient and family.
- Communication with primary pediatrician/PCP.
- Facilitate pediatric specialist consults and follow-up (in collaboration with the trauma team).
- Assist the trauma team with facilitating discharge to inpatient rehabilitation.
Responsibilities of the Trauma Service
- Contacting all consult services based on patient injuries and clinical findings.
- Coordinating and managing all procedural and operative interventions.
- Admission and discharge orders and notes.
- Diet/nutrition management and associated orders.
- Activity orders.
- Wound care management and associated orders.
- Imaging and lab orders.
- Determination of need, orders, and management of DVT prophylaxis (in collaboration with PCCM and pharmacy).
- Blood product transfusions (in collaboration with PCCM).
- Management of new medical issues (in collaboration with PCCM).
- Chest tube placement and management (in collaboration with PCCM).
References
- Rosen, N. G., Escobar Jr, M. A., Brown, C. V., Moore, E. E., Sava, J. A., Peck, K., ... & Martin, M. J. (2021). Child physical abuse trauma evaluation and management: a Western Trauma Association and Pediatric Trauma Society critical decisions algorithm. Journal of Trauma and Acute Care Surgery, 90(4), 641-651.
- American College of Surgeons Trauma Quality Improvement Program (2019). ACS Trauma Quality Program Best Practices Guidelines for Trauma Center Recognition of Child Abuse, Elder Abuse, and Intimate Parner Violence. Release November 2019. Available at https://www.facs.org/media/o0wdimys/abuse_guidelines.pdf. Accessed March 20, 2024.
Authors
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principal Author
- Megan Samland, DNP | Division of Acute Care Surgery, Advanced Practice Provider | Principal Author
- Eleanor Gradidge, MD | Department of Pediatrics, Division of Pediatric Critical Care, Faculty | Principal Author
Last Updated: June, 2024
Indications to Consult Pediatric Co-Management Team for Pediatric Trauma Patients
Purpose:
The trauma service frequently admits and cares for injured children (aged 18 years or less). To optimize outcomes and inpatient care, assistance in the management and care of these injured pediatric trauma patients is enhanced by involvement of the pediatric co-management team. As a result, collaboration between the trauma and pediatric co-management team is essential. These guidelines outline when pediatric co-management team should be consulted to assist in the management and care of pediatric trauma patients.
Indications to Consult Pediatric Co-Management
- injured children age 18 and under upon admission or transfer to a pediatric floor
Consulting Pediatric Co-Management
- The trauma service will contact the Pediatric Co-Management provider listed “on call” on PerfectServe under “General Pediatric and Neonatology Academic Service TNMC” (choose general pediatric inpatient) for consultation/handoff if the patient is being admitted/transferred to the pediatric floor.
- The trauma service will need to place an “Inpatient consult to pediatrics academic” consult order in EPIC. Reason for consultation can be “medical co-management.”
- Direct verbal communication should occur between the trauma and pediatric co-management providers caring for the patient on admission/transfer to the pediatric floor and with any change in patient status/condition. The pediatric resident may be reached at 402-619-9157.
General requirements:
- When consulted, Pediatric Co-Management will assist with management of pediatric trauma patients once they are considered floor status.
- The trauma service will serve as the patient’s PRIMARY team. As a result, the trauma surgeon/team must be kept informed of and concur with all major therapeutic and management recommendations by the pediatric co-management team. 
-
-
- A minimum of daily communication between the trauma and pediatric co-management teams should occur to discuss patient care plans.
-
-
- The pediatric co-management provider will contact the trauma team daily and as needed via PerfectServe (“Trauma Academic Service) with recommendations after seeing the patient.
-
-
- The trauma team will round daily on patients and write daily progress notes. Following the initial consultation and screenings, the pediatric co-management team will evaluate pediatric patients daily and write progress notes as needed to reflect any updates or changes in recommendations.
- If it is determined that the trauma team should no longer be the primary team on a patient (i.e. transferring to another pediatric service), the trauma service will be responsible for finding an accepting primary service, placing the necessary orders for transfer, communicating plans for transfer with the pediatric co-management team, and documentation of transfer to include patient’s current status/injury management/follow-up/transfer details/etc. (“sign off” note)
- A minimum of daily communication between the trauma and pediatric co-management teams should occur to discuss patient care plans.
-
-
Responsibilities of pediatric co-management team
- Medication management, review, and reconciliation.
-
- Including guidance for dosing by weight and age (in collaboration with pediatric pharmacy).
-
- management of pre-existing/chronic medical conditions
- Responding to all acute decline and decompensation events.
-
- In addition, will contact the trauma team to provide updates on significant events or status changes.
-
- discrepancies between orders (in collaboration with the trauma team)
- communication with primary pediatrician/PCP
- substance and alcohol misuse screening with interventions as needed
- screening and interventions as determined necessary for non-accidental trauma (in conjunction with the trauma team)
- Counseling and guidance of injury prevention, including causative injury and other preventative measures, to patient and family.
- Facilitate pediatric specialist consults and follow-up (in collaboration with the trauma team).
- Assist the trauma team with facilitating discharge to inpatient rehabilitation.
- Mental health screening
Responsibilities of Trauma Service
- Contacting all consult services based on patient injuries and clinical findings.
- Coordinating and managing procedural/operative interventions
- Admission and discharge orders and notes
- Diet/nutrition management and associated orders
- Blood product transfusions
- Electrolyte replacement, glucose management, bowel regimen orders and other routine daily cares (in collaboration with pediatric co-management and pharmacy)
- Activity orders
- Pain Management (in collaboration with pediatric co-management)
- Wound care management and associated orders.
- Imaging and lab orders
- Determination of need, orders, and management of DVT prophylaxis (in collaboration with Pediatric co-management and pharmacy)
- Management of new medical issues (in collaboration with Pediatric co-management)
- Line and tube placement and management (central lines, chest tubes, etc.)
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principal Author
- Katherine MacKrell, MD | Department of Pediatrics, Division of Hospital Medicine, Faculty | Principal Author
Last Revised
July, 2024
Managment of Open Pediatric Orthopedic Fractures
Purpose:
To provide guidance on the management of open orthopedic fractures in pediatric trauma patients.
Background/definitions:
An open fracture is a fracture in which there is an open wound or break in the skin near the site of the broken bone. Most often, this wound is caused by a fragment of bone breaking through the skin at the time of injury. The fractured bone is exposed to contamination from the external environment and is susceptible to infection.
Guideline Inclusion Criteria:
- Injured children and adolescents 18 years and younger with confirmed or suspected open fractures.
Guideline Exclusion Criteria:
- Injured patients >18 years old.
Practice Recommendations for Management:
- Orthopedic surgery should be consulted on all open pediatric orthopedic fractures.
- Classification is made according to the Gustillo classification of open fractures. This classification is made at the time of operative debridement.
-
- Type I: open fracture with wound <1cm long; clean
- Type II: open fracture with wound >1cm long; soft tissue damage, avulsions, tissue flap, minimal to moderate contamination
- Type III: extensive soft tissue damage, open segmental fracture; significant contamination.
-
- Type IIIA: soft tissue coverage is adequate (primary closure/delayed primary closure or skin graft)
- Type IIIB: periosteal stripping, bone exposure, massive contamination; will require either rotational flap or free flap for coverage
- Type IIIC: open fracture with arterial injury requiring repair to salvage limb
-
-
- Antibiotics should be initiated within 60 minutes of patient arrival:
-
- Type I and II:
-
- Preferred: Cefazolin 30 mg/kg IV now and q8hr x 3 total doses (not to exceed 2000mg/dose)
- Severe cephalosporin allergy: Clindamycin 10mg/kg IV now and q8hr x 3 doses (not to exceed 900 mg/dose)
- Known MRSA colonization: add vancomycin 15mg/kg IV q12hr
- Duration of prophylaxis: 24 hours
-
- Type III
-
- No gross contamination:
-
- Preferred: Cefazolin 30 mg/kg IV now and q8hr x 3 total doses (not to exceed 2000mg/dose)
- Severe cephalosporin allergy: Clindamycin 10mg/kg IV now and q8hr x 3 doses (not to exceed 900 mg/dose)
- Known MRSA colonization: add vancomycin 15mg/kg IV q12hr
- Duration of prophylaxis: 48 hours or 24 hours after wound closure, whichever is shorter
-
- Contamination with soil or fecal material
-
- Preferred: ceftriaxone 75mg/kg IV now and q24hr (not to exceed 2000mg/dose) AND metronidazole 15mg/kg IV now and q8hr (not to exceed 500 mg/dose)
- Severe cephalosporin allergy: Clindamycin 10mg/kg IV now and q8hr (not to exceed 900 mg/dose)
- Known MRSA colonization: add vancomycin 15mg/kg IV q12hr
- Duration of prophylaxis: 48 hours after wound closure
- Consider orthopedic infectious disease consult
-
- Contamination with standing water:
-
- a. Preferred: Piperacillin/tazobactam 100mg/kg IV q8hr over 4 hours (not to exceed 4.5g IV)
- b. Penicillin allergy: Clindamycin 10mg/kg IV now and q8hr (not to exceed 900 mg/dose) AND metronidazole 15mg/kg IV now and q8hr (not to exceed 500 mg/dose)
- c. Known MRSA colonization: add vancomycin 15mg/kg IV q12hr
- d. Duration of prophylaxis: 48 hours after wound closure
- e. Consider orthopedic infectious disease consult
-
- No gross contamination:
- Variances in dosing within 5mg/kg are acceptable based upon dosage rounding in Pharmacy.
- If there are any drug-related questions (drug choice, dosing, allergies, alternative options), discuss with pharmacy.
-
- Type I and II:
-
- Tetanus toxoid should be administered if the patient had an incomplete immunization, if it has been >1- years since the last booster, or if immunization history is unknown or unclear. Tetanus immunoglobulin should be administered if patient has never been immunized and present with wound that is felt to be tetanus prone.
- Patients with open fractures should be taken to the operating room for irrigation and debridement within 24 hours of initial presentation whenever possible. Patients with severe fractures associated with gross wound contamination should be brought to the operating room as soon as clinically feasible based on the patient’s condition and resources available. All patients will receive an initial bedside irrigation with removal of obvious foreign contamination and application of clean dressings to wounds in the emergency department.
- Whenever possible, skin defects overlying open fractures should be closed at the time of in initial debridement in the operating room.
- Soft tissue coverage should be completed within seven days of injury whenever possible for open fractures associated with wounds requiring skin grafting or soft tissue transfers.
- Skeletally mature patients between 14 and 18 years of age may follow the adult open fracture protocol (PRO 12 Management of Open Fractures).
Outcome Measures and Guideline Adherence:
- Orthopedic response times for urgent consults, time to antibiotic administration, time to OR for debridement and time to wound coverage for open fractures will be monitored through the pediatric trauma performance improvement process.
- PRO 12 Management of Open Fractures
- Antibiotic Prophylaxis in Open Fractures
Key Contributors:
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Manager | Co-Author
- Sara Putnam, MD, ABOS MD| Department of Orthopedic Surgery, Faculty | Reviewer
Last updated:
· July, 2024
References:
- Davis M, Della Rocca G, Brenner M, et al. (2022) ACS TQIP Best Practices in the Management of Orthopedic Trauma. Best Practices in the Management of Orthopedic Trauma | ACS TQIP (facs.org)
Management of Pediatric Long Bone Fractures
Purpose:
To provide guidance on the management of long bone fractures in pediatric trauma patients.
Background/definitions:
A long bone is defined as any bone of the extremity that has a length greater than the width to include:
- Femur
- Tibia/fibula
- Humerus
- Radius/Ulna
Management of pediatric long-bone injuries is highly dependent upon skeletal maturity. In general, the pediatric orthopedic surgery attendings manage long bone injuries in patients with immature skeletons (i.e. open growth plates), while adult orthopedic surgery attendings manage injuries in patients with mature skeletons (i.e. closed growth plates). The general cutoff is 16 years of age, although the final decision for management of an individual patient is at the discretion of the orthopedic surgery attending on-call, and can involve a discussion between the on-call attending surgeons for pediatric and adult orthopedic surgery. Discretion of casting versus operative care of these injuries is at the discretion of the orthopedic attending on call.
Guideline Inclusion Criteria:
- Injured children and adolescents 18 years and younger with a long bone fracture
Guideline Exclusion Criteria:
- Injured patients >18 years old.
Practice Recommendations for Management:
- Long bone fractures should be stabilized as early as possible.
- Orthopedic surgery will be consulted on all pediatric long bone fractures.
- In the absence of polytrauma, definitive long bone stabilization of femoral shaft fractures should occur within 24 hours of arrival.
-
- Other long bone fractures should undergo early fixation as deemed appropriate by the orthopedic team.
-
- For the polytrauma patient, medical stability and concomitant injuries should be assessed prior to internal fixation. A damage control approach should be taken and the internal fixation of long bone fractures should be delayed until the patient is adequately resuscitated.
-
- Internal fixation should occur within 48 hours of arrival in the polytrauma patient and after initial stabilization.
- External fixation devices should be utilized until internal fixation is appropriate.
-
- Children younger than thirty-six months with a diaphyseal femur fracture should be evaluated for child abuse.
-
- For children younger than one year of age, the Child Advocacy Team (CAT) should be consulted for evaluation.
- For children above one year of age, consultation of the Child Advocacy Team (CAT) will be at the discretion of the pediatric orthopedic and trauma surgery attendings on call.
-
- Management of pediatric diaphyseal femur fractures will be at the discretion of the pediatric orthopedic attending on call, with reference to the 2020 AAOS Clinical Practice Guideline (pdffcpg.pdf (aaos.org)) on this injury.
- Transfer of pediatric long bone fractures to Children’s Nebraska for definitive management may be considered in the absence of polytrauma and requires approval from the trauma surgery attending on call.
Outcome Measures and Guideline Adherence:
- Orthopedic response times for urgent consults as well as time to OR for definitive management of long bone fractures will be monitored through the pediatric trauma performance improvement process.
- All transfers to Children’s Nebraska will be reviewed through the pediatric trauma performance improvement process.
Key Contributors:
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Manager | Co-Author
- Sara Putnam, MD, ABOS MD| Department of Orthopedic Surgery, Faculty | Reviewer
Last updated:
· July, 2024
References:
- Davis M, Della Rocca G, Brenner M, et al. (2022) ACS TQIP Best Practices in the Management of Orthopedic Trauma. Best Practices in the Management of Orthopedic Trauma | ACS TQIP (facs.org)
- American Academy of Orthopedic Surgeons. (2022). Treatment of Pediatric Diaphyseal Femur Fractures. https://www.aaos.org/globalassets/quality-and-practice-resources/pdff/pdffcpg.pdf
Management of Pediatric Pelvic Fractures
Purpose:
Provide guidance on the initial evaluation and management of pediatric trauma patients with pelvic fractures.
Background:
Injures to the pelvis range from benign to life threatening. They include pelvic ring fractures, acetabular fractures, avulsion, and iliac wing fractures. The pelvis in children consists of high cartilaginous volume with greater elasticity at the sacroiliac joints and symphysis. Therefore, the pediatric pelvis is less prone to fracture and more able to dissipate a relatively large amount of energy. Most pediatric pelvic injuries are due to high-energy blunt trauma, which increases the likelihood of concomitant injuries to the head, chest, abdomen, and extremities.
Guideline Inclusion Criteria:
- Pediatric trauma patients age 18 years and younger with confirmed or suspected pelvic fractures
Guideline Exclusion Criteria:
- Trauma patients >18 years of age
Practice Management Guidelines:
- Orthopedic surgery will evaluate the patient within 30 minutes of consultation request; interventional radiology (IR) should be notified if there is any consideration for embolization.
- Initial evaluation
-
- Patient should be assessed and managed per ATLS guidelines. Physical examination should be performed by the trauma team in conjunction with the orthopedic team to specifically include:
-
- Urologic/vaginal exam
- Perineum exam
- Rectal exam
-
- An AP pelvis x-ray will be obtained in the trauma bay. The decision to forego AP pelvis x-ray and proceed directly to CT imaging is at the discretion of the trauma surgery attending.
- Pediatric trauma patients that require pelvic stabilization via binder or sheet are limited to: unstable pelvic fracture and hemodynamically unstable patient
-
- This includes patients who arrived hemodynamically unstable and have since stabilized.
- The pelvic binder or sheet should be placed at the level of the greater trochanters
- Patients who arrive to the trauma bay with a pelvic binder or stabilization sheet already in place should not have it removed until either AP pelvis x-ray is obtained to determine necessity, or unless directed by Orthopedic Surgery.
-
- It is acceptable to briefly remove the binder or stabilization sheet for adequate patient assessment.
-
-
- CT scan of the pelvis, including reconstructions, are obtained to evaluate for associated injuries.
- Initial evaluation should include determination if a urinary catheter is necessary.
-
- The Orthopedic Surgery team will include any recommendations for urinary catheterization in the consult note, and either Orthopedic Surgery or Trauma Surgery will place the order for urinary catheter in the electronic medical record.
- Timely urinary catheter insertion is essential. Any barriers to insertion should be promptly escalated to Orthopedic Surgery or Trauma Surgery.
- Questions related to permissible patient positioning during urinary catheter insertion should be directed to Orthopedic Surgery. If there are difficulties in obtaining proper positioning or if there is concern related to fractures as it relates to positioning, Orthopedic Surgery may be contacted for bedside assistance.
- Consider urology consult if there are concerns related to urethral injury or if urinary catheterization attempts are unsuccessful.
- External catheters, such as Pure Wick, are not an acceptable substitution and should not be utilized in acute pelvic fracture management.
- Mobile patients without activity restrictions may utilize a bedpan.
-
- Patient should be assessed and managed per ATLS guidelines. Physical examination should be performed by the trauma team in conjunction with the orthopedic team to specifically include:
-
- Management is based upon hemodynamic stability
-
- Ultimate decision for fracture treatment is determined by the Orthopedic Surgeon
- Volume resuscitation with appropriate blood products and maintenance of core temperature must be continued during all phases of resuscitation. Activation of Massive Transfusion Protocol (MTP) will be utilized as indicated per policy (PRO 09- Massive Transfusion in Trauma Guidelines). Blood products will be administered via rapid transfuser.
- For patients in a pelvic binder:
-
- Repeat AP pelvic x-ray should be obtained to assess reduction
- Binder should not remain in placed for longer than 48 hours unless there are extenuating circumstances that prevent operative intervention.
- Skin checks should be performed by the orthopedic surgery service ever 12 hours while the binder is in place, with removal of the binder ever 24 hours for more thorough skin check (maintaining precautions to prevent movement of the pelvis).
- Skeletal traction may be placed at the discretion of the orthopedic surgery attending.
-
- For hemodynamically unstable patients despite adequate resuscitation and/or patients with evidence of contrast extravasation on CT imaging related to pelvic fractures, consider consultation of IR for possible angioembolization.
-
Pediatric Pelvic Fracture Pathway

Key Contributors:
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Manager | Co-Author
- Sara Putnam, MD, ABOS MD| Department of Orthopedic Surgery, Faculty | Reviewer
Last updated:
· July, 2024
References:
- Coccolini, F. (2017) Pelvic Trauma: WSES classification and guidelines, World Journal of Emergency Surgery, 12(5), 1-18.
- DeFrancesco CJ, Sankar, WN. (2017). Traumatic pelvic fractures in children and adolescents. Seminars in Pediatric Surgery, 26(1), 27-35.
- Hermans E, Cornelisse ST, Biert J, et al. (2017) Paediatric pelvic fractures, how do they differ from adults? Journal of Children’s Orthopeadics, 11, 49-56.
- Swaid F, Peleg K, Alfici R, et al. (2017). A comparison study of pelvic fractures and associated abdominal injuries between pediatric and adult trauma patients. Journal of Pediatric Surgery, 52, 386-389.
- Swenson SJ, Otsuka NY. (2022) Pelvic Fractures. Pediatric Orthopedic Society of North America. Pelvic Fractures | Pediatric Orthopaedic Society of North America (POSNA).
- Tosounidis TH, Sheikh H, Giannoudis PV. (2015). Pelvic fractures in paediatric polytrauma patients: Classification, concomitant injuries and early mortality. The Open Orthopedics Journal. 9(1), 303-312.
Mental Health Screening and Intervention Guidelines for Pediatric Trauma Patients at Nebraska Medicine
Childhood traumatic stress happens when unexpected, violent, life-threatening, or devastating events overwhelm the ability to cope. The ACS reports that 20-30% of pediatric trauma patients report mental health symptoms and/or decreased quality of life following a traumatic event.
The purpose of this guideline is to identify pediatric trauma patients at high risk for post-trauma mental health adjustment disorder post-injury and facilitate brief interventions and appropriate referrals for longer term management and care.
1. A HEADSS assessment will be performed on all admitted pediatric trauma patients age 11 years and older by the pediatric co-management team once the patient reaches floor status.
2. Patients with a positive HEADSS assessment in the mental health categories AND/OR any pediatric patient experiencing the following traumatic events:
a. Neglect and psychological, physical, or sexual abuse.
b. Victim of community and school violence.
c. Victim of gun-related violence (intentional self-inflicted GSW or suicidal attempt will prompt child psychiatry consult)
d. Serious traumatic event causing life-threatening and devastating injuries (traumatic brain injury, spinal cord injury, loss of limb, mutilating/deforming injuries, etc)
e. Prolonged hospital stay (longer than 1 week)
f. Death of friend/family member in traumatic event
g. Care provider discretion.
These patients are identified as high risk for post-injury mental health disorder(s) will undergo additional screening using the ASC6/ASC3 screening tool derived from the Acute Stress Checklist (ASC-Kids) or consultation with behavioral health/child psychiatry.
3. Patients admitted following self-inflicted injury or suicide attempt as well as patients with suicidal or homicidal ideation will receive inpatient consultation with child psychiatry.
4. Patients who screen positive on the ASC6/ASC3 will receive one or more of the following intervention(s):
a. Consultation of child psychiatry for inpatient assessment of mental health concerns
b. Referral to child psychiatry or psychology for outpatient assessment and management of mental health concerns
c. Notification of primary pediatrician of mental health concerns for assistance in longer term follow-up and/or outpatient mental health referrals as indicated
5. For patients who do not screen positive but have experienced one of the above traumatic events, the patient’s primary pediatrician should be notified with the recommendation to perform a repeat assessment of the patient’s mental health in 4-6 weeks time.
Documentation
The HEADDS, ASC6/ASC3 assessment (if performed), and interventions provided will be documented in a progress note by the pediatric co-management teams in the patient’s electronic medical record when consulted. For those patients remaining in the ICU for entire hospital course, mental health screening will be performed as indicated by the trauma service.
References:
1. American College of Surgeons. (2022, December). Best Practices Guidelines: Screening and Intervention for mental health disorders and substance use and misuse. https://www.facs.org/media/nrcj31ku/mental-health-guidelines.pdf
2. The Acute Stress Checklist (ASC-kids) (2016), https://www.healthcaretoolbox.org/acute-stress-checklist

Non-Surgical Service Admissions of Pediatric Trauma Patients at Nebraska Medicine
SCOPE AND PURPOSE
The document is applicable to pediatric patients (age <19) assessed and cared for at Nebraska Medicine.
POLICY AND PROCEDURE STATEMENTS
The pediatric trauma accreditation standards, as set forth by the American College of Surgeons, encourage all injured patients to be admitted to a surgical service. Children may be admitted to a pediatric general or subspecialty service when a medical diagnosis was initially made based on history and physical exam or for care of a pre-existing medical condition. In those rare instances, the following policy has been formulated to guide the management of an injured patient admitted to a non-surgical service.
- When it is known that a physical injury has occurred, a Trauma Surgery consult must be obtained. Assessment and recommendations for care will be documented in the electronic medical record.
- In conjunction with the admitting pediatrician, the trauma surgery attending will determine a plan of care that includes transfer to a surgical service when injury is the primary reason for admission. Concurrent care with pediatric critical care medicine (PCCM), pediatric co-management team or other pediatric specialists will continue during the child’s hospitalization. (See “Indications to consult Pediatric Critical Care Medicine for pediatric trauma patients” and “Indications to consult Pediatric Co-Management for pediatric trauma patients”)
- All patients who are found to have physical injuries must be evaluated for rehabilitative and social work needs.
- If suspicion of child abuse or neglect is identified, a referral to the Child Advocacy Team (CAT) and social work must occur promptly with subsequent additional work-up as indicated. (See “Evaluation and Management of Non-Accidental Trauma (NAT) in Children at Nebraska Medicine”)
- All non-surgical service admissions (NSA) of injured patients will be reviewed through the pediatric trauma performance improvement process.
-
- NSA with trauma or other surgical consultations, with ISS≤9, or without other identified opportunities for improvement may be closed in primary review.
- NSA without trauma or other surgical consultation, with ISS>9, or with identified opportunities for improvement must at a minimum be reviewed by the Pediatric Trauma Medical Director in secondary review.
-
APPROVALS:
|
Authorized: |
Emily Cantrell, MD Pediatric Trauma Program Medical Director |
|
Approved: |
Lora Hofstetter, MSN, RN, CCRN, C-NPT Pediatric Trauma Program Manager |
DATE OF ORIGIN AND REVIEWS
Date of Origin: 8/2024
Date of Reviews:
CONTENT REVIEWERS AND CONTRIBUTORS
Pediatric Trauma Program Liaisons, Pediatrics
Pediatric Needle Cricothyroidotomy
Pediatric Needle Cricothyroidotomy
Supplies
- (Kit located in 2nd Drawer of Pediatric Grey Trauma Cart—Trauma Bay 2)
- 16G Angiocath (IV catheter)
- Macrobore IV Extension Tubing
- End of a 3.0 ETT
- 10 ml Syringe with 5ml saline (for air placement confirmation)
Process for Cannot Intubate and Cannot Ventilate (CICV) Emergency
Video available here: https://youtu.be/EEqXqiOyKr4?si=iF8VRp-n3FwuVeIB
- Identify landmarks and stabilize the larynx with non-dominant hand
- Access the cricothyroidotomy membrane with a 16G angiocath, aim in the caudad direction
- Connect syringe with saline and pull-back to confirm placement by air aspiration
- If placement is confirmed, connect macrobore tubing to catheter and then place 3.0 ETT end on tubing (See picture).
- Connect to a pressure limiting bag or a jet ventilation device
- Breaths should be delivered over 1 second and allowing for 2 second exhalation
- Observe for complications such as: subcutaneous emphysema, hemorrhage, hypoventilation, equipment failure, catheter kink, & false placement.

Additional Resources:
- https://www.paediatricemergencies.com/intubationcourse/course-manual/cricothyroidotomy/
- https://medicine.uiowa.edu/iowaprotocols/needle-cricothyroidotomy
Please contact Dr. Emily Cantrell, Pediatric Trauma Medical Director, or Lora Hofstetter, Pediatric Trauma Program Coordinator for questions and additional training.
Pediatric Transport Contact Information
Critical Pediatric Trauma Patient Transfer Requests
Please be prepared with the following information:
-
Provider's name requesting transport and call back number
-
Patient's name, age, DOB, and weight
-
Chief complaint/diagnosis and present conditions
-
Medical history and allergies, if known
-
Current vitals and ABCs
-
Treatment, medications started, and IV access
If requesting transport to Children’s Nebraska:
· Children’s Nebraska Transport 855-850-5437
o Ask for assistance in coordinating a transport to Children’s Nebraska for (state the need) i.e. Trauma, PICU, Orthopedics, Neurology, etc.
If Children’s Nebraska Transport team is unavailable:
· LifeNet or StarCare (AirMethods programs) 844-359-9111
o Ask for assistance in coordinating transport of a patient to Children’s Nebraska
o This will get you to an AirMethods Team that is closest.
If requesting transport of a patient to outside Omaha:
· Children’s Nebraska Transport 855-850-5437
o Ask for assistance in coordinating transport of a patient from Nebraska Medicine to [Destination]
o You will be connected to a team member to triage call.
· Children’s Mercy 800-466-3729
o Ask for assistance in coordinating transport of a patient from Nebraska Medicine to [Destination]
o Communication specialists will connect you to the appropriate physician or team to coordinate transport.
If Specialized Pediatric Transport teams are unavailable:
· LifeNet or StarCare (AirMethods) 844-359-9111
o Ask for assistance in coordinating transport of a patient from Nebraska Medicine to [Destination]
o This will get you to an AirMethods Team that is closet with the appropriate asset.
Alternate Resource:
· MercyOne (Sioux City, IA) 800-247-1911
o Same process as LifeNet
**Air/Ground transport may be dependent on program regulations, weather, & team availability. For the safety of the team & patient, never pressure a team to change a decision based on decline for weather or comfort.
Contact Information for Pediatric Trauma Patients
Common Consults for Traumatic Injuries:
- Cardiothoracic Surgery
-
-
-
- PerfectServe: Cardiac Surgery Academic Service TNMC
-
-
-
- FACE (ENT, OMFS, Plastics)
-
-
-
- PerfectServe: Facial Trauma Unassigned TNMC
-
-
-
- HAND (Plastics, Ortho)
-
-
-
- PerfectServe: Hand—TNMC (Hand Trauma and Consults – Ortho, Plastics)
-
-
-
- Neurosurgery
-
-
-
- PerfectServe: Neurosurgery Academic Service TNMC
-
-
-
- OB-GYN
-
-
-
- PerfectServe: Obstetrics and Gynecology Academic Service TNMC
-
-
-
- Ophthalmology
-
-
-
- PerfectServe: Ophthalmology Academic Service TNMC
-
-
-
- Orthopedic surgery
-
-
-
- PerfectServe: Orthopedic Academic Service TNMC
-
-
-
- Pediatric Surgery
-
-
-
- Call Children’s Nebraska Access Center at 1-855-850-KIDS (5437) and request to be put in contact with provider on call for specific service.
- Please utilize as first to call in pediatric trauma patients <15 years of age for assistance in general surgical injuries with the exception of emergent complex hepatobiliary injuries.
-
-
-
- Transplant/Hepatobiliary Surgery
-
-
-
- PerfectServe: Transplant – Liver & Bowel TNMC
-
-
-
- Spine (Ortho, NSGY)
-
-
-
- M/W/F/Sun—
-
- PerfectServe: Neurosurgery Academic Service TNMC
-
- T/Th/Sat—Orthopedic Spine Service
-
- PerfectServe: Orthopedic Academic Service TNMC
-
- M/W/F/Sun—
-
-
-
- Urology
-
-
-
- PerfectServe: Urology Academic Service (Genitourinary-GU)
-
-
-
- Vascular Surgery
-
-
-
- PerfectServe: Vascular Surgery Academic Service TNMC
-
-
-
***In general, pediatric specialists will manage injuries in pediatric trauma patients <15 years of age with some variability between service lines and attendings. Pediatric surgery should be utilized for patients <15 years of age for general traumatic injuries. In patients 15 years and older, adult general surgery subspecialties (MIS, CRS, surgical oncology) may be consulted for second opinions/area expertise if needed but may defer consultation to pediatric surgery in certain circumstances (i.e. congenital issues, complex/prior pediatric surgery history, etc). Transplant/Hepatobiliary Surgery should be considered for the first call in the setting of emergent complex traumatic hepatobiliary injuries.***
***Pediatric attendings will be contacted by his/her respective resident. If there are questions or uncertainty involving the case, the trauma attending should reach out and discuss case with the on-call attending for that specific specialty***
***Decision to engage pediatric orthopedic specialists will be based on injury, skeletal maturity and discretion of orthopedic attending on call. If orthopedic injury is isolated and transfer to Children’s hospital for management is requested, the trauma attending should be notified and agree to transfer. The pediatric TMD should also be notified of the plan to transfer a patient***
General Pediatric and Pediatric Subspecialties:
- Pediatric Floor and ICU (main desk): 402-559-7400
- PICU/Pediatric Lead Nurse (Volte): 531-557-3201
- Melanie Anderson (nurse manager, PICU/general pediatrics): 402-885-0156
- Pediatric Anesthesia
-
-
-
- Call anesthesia attending phone at (402)-650-5748 to discuss specific needs.
-
- In house anesthesia (preferentially pediatric anesthesia when available) will handle emergent issues (intubations, starting emergent cases, etc.).
- Overnight, pediatric anesthesia is on home call and can be mobilized if needs arise.
-
- Call anesthesia attending phone at (402)-650-5748 to discuss specific needs.
-
-
-
- Pediatric Cardiology
-
-
-
- PerfectServe: Children’s Hospital Cardiology
- PREFERRED: Call Children’s Nebraska Access Center at 1-855-850-KIDS (5437) and specify if you need consult, echo, EP, etc.
-
-
-
- Pediatric Co-Management
-
-
-
- PerfectServe: General Pediatric and Neonatology Academic Service TNMC OR Pediatrics Nebraska Medicine à General Pediatric Inpatient
- Pediatric resident pager: 402-619-9157
-
-
-
- Pediatric Critical Care Medicine
-
-
-
- PerfectServe: Pediatric Critical Care Medicine Academic Service TNMC
- PICU APP pager number: 402-888-7226; office located in pediatric unit
-
-
-
- Pediatric Endocrine
-
-
-
- Not currently available. Hired new staff and working to find out when they will provide consult support again.
-
-
-
- Pediatric Gastroenterology
-
-
-
- PerfectServe: Pediatric Gastroenterology Academic Service TNMC (Pedi GI)
- Physically present on the pediatric unit daily, M-F at 10:30am and Sat-Sun at 9am.
-
-
-
- Pediatric Hematology-Oncology
-
-
-
- PerfectServe: Pediatric Hematology Oncology Academic Service TNMC
-
-
-
- Pediatric Infectious Disease
-
-
-
- PerfectServe: Pediatric Infectious Disease Academic Service TNMC (Pedi ID)
-
-
-
- Pediatric Nephrology
-
-
-
- PerfectServe: Pediatric Nephrology Academic Service TNMC
-
-
-
- Pediatric Neurology
-
-
-
- PerfectServe: Pediatric Neurology Academic Service TNMC
-
-
-
- Pediatric Palliative Care
-
-
-
- Call Children’s Nebraska Access Center at 1-855-850-KIDS (5437) and request to be put in contact with provider on call for specific service.
-
-
-
- Pediatric PM&R
-
-
-
- PerfectServe: PM&R – Physical Medicine and Rehabilitation TNMC
- Dr. Pierce and Dr. D’Angelo staff the pediatric patients at NM.
-
-
-
- Pediatric Pulmonology
-
-
-
- Call Children's Nebraska Access Center at 1-855-850-KIDS (5437) and request to be put in contact with provider on call for specific service.
-
-
-
- Pediatric Psychiatry
-
-
-
- PerfectServe: Psychiatry Academic Service TNMC à Is this regarding a child? à Inpatient Child Psychiatry
-
-
-
- Pediatric Surgery
-
-
-
- Call Children’s Nebraska Access Center at 1-855-850-KIDS (5437) and request to be put in contact with provider on call for specific service.
-
-
-
*****If there is difficulty in contacting specific pediatric subspecialties or find that any of these numbers are incorrect/out of date, please contact Dr. Emily Cantrell (pediatric TMD) of Lora Hofstetter (pediatric trauma program coordinator) for additional assistance*****
Last updated: March, 2025
Recommendations for Acute Pain Treatment and Procedural Pain and Sedation Management for Pediatric Patients
Common medical procedures used to assess and treat children can cause significant pain and distress. Before initiating any non-emergent procedure in pediatric trauma patients, please take a moment to try and optimize pain and sedation management. Below are two links with recommendations and suggestions on how to approach pain and sedation management in pediatric patients before procedures. Of note, NM does not have all of the recommended drugs/products available on formulary. Please discuss with pharmacy if there are any questions regarding drug choice and dosage prior to use.
- Pediatric Education and Advocacy (PEAK): Bottom Line Recommendations: Pain Treatment
- Pediatric Education and Advocacy Kit (PEAK): Bottom Line Recommendations: Procedural Pain
- Pediatric Education and Advocacy Kit (PEAK): Bottom Line Recommendations: Procedural Sedation
Date Created: March, 2025
Pediatric Presence at Pediatric Trauma Activations
Purpose:
The trauma service frequently encounters critically injured pediatric patients that require pediatric specific resuscitation measures. To optimize patient outcomes and experiences, assistance in the initial resuscitation and care of these critically injured pediatric trauma patients is often enhanced by the presence and involvement of pediatric nursing and/or pediatric critical care provider. The following guidelines outline when pediatric nursing and providers will be present at pediatric trauma activations.
Criteria for Pediatric Presence at Pediatric Trauma Activations:
- When available, the pediatric critical care provider (APP and/or attending) will present to all FULL trauma activations in patients age 12 years and younger.
- For LIMITED activations or other pediatric trauma encounters in the ED, the presence of the pediatric critical care provider (APP and/or attending) may be requested on an as needed basis.
-
-
-
- The pediatric ICU APP may be contacted via PerfectServe (Pediatric Critical Care Medicine Academic Service TNMC) or by paging 402-888-7226.
-
-
-
- The presence of the pediatric ICU (PICU)/pediatric lead nurse (or designee) may be requested for any pediatric trauma activation/encounter in the ED when pediatric specific skill set felt to be beneficial to case.
-
-
-
- The PICU/Pediatric Lead Nurse may be contacted via Volte phone at 531-557-3201.
-
-
-
***Due to staffing and responsibilities in the pediatric ICU, the pediatric critical care provider and pediatric ICU lead nurse (or designee) may not always be immediately available to respond in person to activations. If the pediatric critical care provider and/or nurse are not present at a pediatric trauma activation and presence is needed, please contact at above listed numbers.***
Responsibilities:
Responsibilities and involvement of pediatric nursing and pediatric critical care provider during the initial trauma resuscitation will be in collaboration with the trauma team and at the discretion of the trauma attending. Responsibilities include, but are not limited to, the following:
- Pediatric Nurse:
-
-
-
- Assist in obtaining IV access
- Assist in nursing procedures (NG, OG, foley placement, etc)
- Assist in administration and titration of medications or IV fluids
- Assist in transfusion of blood products
-
-
-
- Pediatric Critical Care Provider:
-
-
-
- Assistance with procedures (central lines, arterial lines, chest tubes, etc)
- Assistance with medication selection and dosage (in collaboration with pharmacy)
- Coordination and assistance with fluid and blood product resuscitation (in conjunction with trauma team)
- Assistance with ventilator management
- assistance in consultation of pediatric subspecialties
-
-
-
Transferring Pediatric Trauma Patients to Children's Nebraska Emergency Department
Process for Transferring Pediatric Trauma Patients to Children’s Nebraska Emergency Department
As a level II pediatric trauma center, every effort should be made to care for pediatric trauma patients at Nebraska Medicine (NM). However, based on allocation of resources and specialty services, certain pediatric traumatic injuries may benefit from transfer to Children’s Nebraska. In general, these injuries include but are not limited to the following:
- Isolated orthopedic injury in skeletally immature children
- Orthopedic injury in skeletally immature children with minor additional injuries that do not require admission/monitoring
- Need for cardiopulmonary bypass or ECMO in children <15 yrs of age
Patients with multiple injuries, particularly those requiring active monitoring for risk of hemodynamic decompensation or need for rapid intervention, should stay at NM and be primarily admitted and managed by the trauma service with appropriate consulting services as indicated by injury/clinical status.
If transfer to Children’s Nebraska is deemed necessary, the following steps should be taken:
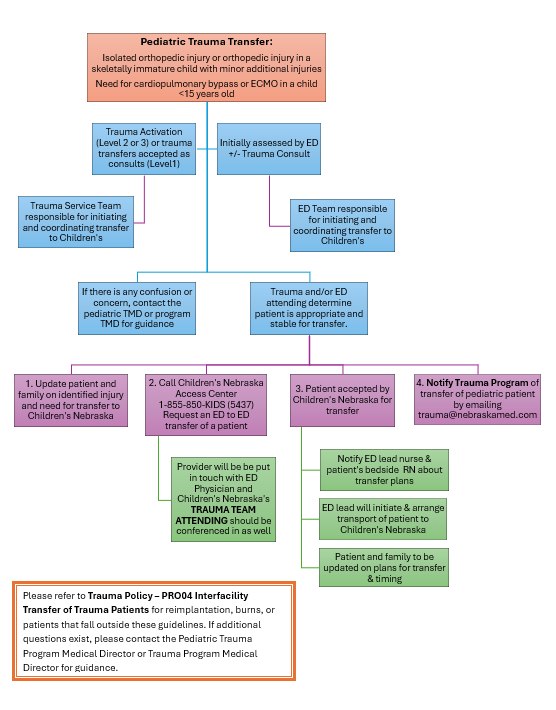
13. VTE Prophylaxis in Trauma
Orthopedic Trauma Discharge VTE Prophylaxis
Not Indicated:
- In general, VTE prophylaxis at discharge is not indicated for the following injuries:
-
- isolated upper extremity fractures (i.e. clavicle, humerus, elbow, forearm)
- non-operative isolated pelvic fractures (i.e. pubic rami, sacral ala)
-
Indicated:
- In general, if a patient has a lower extremity fracture and is NWB or TTWB for 6 weeks or greater, he/she will require VTE prophylaxis on discharge.
-
- Length of recommended VTE prophylaxis begins from the time of surgery for that particular orthopedic injury.
- If the patient has multiple orthopedic injuries undergoing operative fixation and requiring post-op VTE prophylaxis, pick the longest of the recommended therapies.
-
- While inpatient, a patient should remain on standard VTE prophylaxis for the trauma patient (typically Lovenox BID) and be continued on VTE prophylaxis upon discharge with the recommended therapy and remaining length of treatment as noted for each specific injury.
Recommendations:
- Operative Pelvis Fracture (i.e. pelvic ring, SI joint, pubic symphysis, acetabulum)
-
- VTE Prophylaxis: Lovenox 40 mg subcutaneous daily x 3 weeks followed by Aspirin 81mg PO BID x 3 weeks.
-
- Hip or Femur Fracture
-
- VTE prophylaxis: Lovenox 40mg subcutaneous daily x 3 weeks followed by Aspirin 81mg PO BID x 3 weeks
-
- Patella Fracture
-
- VTE prophylaxis: Aspirin 81 mg BID x 6 weeks
-
- Tibial Fracture
-
- VTE prophylaxis: Lovenox 40 mg subcutaneous daily x 3 weeks, followed by Aspirin 81 mg BID x 3 weeks.
- ***Unless stated otherwise in Dr. Putnam op-note: Aspirin 81 mg BID x 6 weeks
-
- Ankle Fracture
-
- Typical VTE prophylaxis: Aspirin 81 mg BID x 6 weeks
- Pilon fracture/Ex-fixed ankle: Lovenox 40 mg subcutaneous daily x 3 weeks followed by Aspirin 81 mg PO BID x 3 weeks.
- Low risk (no-comorbidities): Aspirin 81 mg BID x 30 days.
-
- Operative food fracture (i.e. calcaneous/tallus/navicular/cuboid)
-
- VTE prophylaxis: Aspirin 81 mg BID x 30 days
-
- Operative Lisfranc injuries (typically ex-fixed initially)
-
- VTE prophylaxis: Lovenox 40 mg subcutaneous daily x 3 weeks followed by Aspirin 81mg PO BID x 3 weeks.
-
- Lower extremity amputation
-
- VTE prophylaxis: none unless considered high risk (co-morbidities, other fractures, etc)
-
- Toe amputation
-
- Antibiotics: oral antibiotics until 1st follow-up appointment
- VTE prophylaxis: none
-
VTE Prophylaxis in Trauma Patients
Purpose
Venous thromboembolism (VTE), in the form of either deep vein thrombosis (DVT) or pulmonary embolism (PE), can result in significantly increased morbidity and mortality for patients. Trauma patients, in particular, are at increased risk for development of VTE due to a prothrombotic state created by the traumatic event, injuries sustained, and resulting impaired mobility. This practice guideline is to provide guidance on preventing VTE in the trauma patient population.
Risk Stratification
|
Low Risk |
· Expected length of stay less than 48 hours · Patients in observation status · Patients no longer (or never) ill who are awaiting disposition · Ambulating cancer patient admitted for short stay chemo infusion · Ambulating patients not meeting criteria for moderate or high risk (trauma patients very rarely are in this group) |
|
Moderate Risk |
· Moderate/major surgery with impaired mobility · Moderate/major surgery with any VTE risk factor* · Active cancer with acute medical illness, reduced mobility, or other VTE risk factors · Medical/surgical patient with reduce mobility and acute illness · Medical/surgical patient with prior history of VTE |
|
High Risk |
· Orthopedic joint/bone surgery in pelvis or lower extremity · Major orthopedic trauma · Surgery of abdominal or pelvic cancers · Critically ill patients in the ICU · Acute spinal cord injury with paresis · Craniotomy surgery · Spinal surgery for cancer or spinal fusion · Major Trauma victims (presence of >1 of following): o ISS>15 o GCS<9 for more than 4 hours o Lower extremity fractures o Multiple spine fractures o Major pelvic fracture o Multiple (>3) long bond fractures (>/= 1 in the lower extremity) o Spinal cord injury with paraplegia or quadriplegia o Laparotomy, thoracotomy, or laparoscopy o Co-morbid risk factors* including prior history of DVT/PE, obesity, known sepsis, malignancy, hypercoagulable state, and pregnancy. |
VTE Risk Factors:
- Age greater than 50
- History of prior VTE
- History of myocardial infarction
- History of cancer
- History of atrial fibrillation
- History of ischemic stroke
- History of diabetes mellitus
- History of congestive heart failure
- History of obesity
- History of paralysis
- History of varicose veins
- Use of hormone replacement therapy
- History of inhibitor deficiency state:
-
- Factor V leiden
- Prothrombin gene mutation
- Protein S deficiency
- Protein C deficiency
- Antithrombin III deficiency
- Anticardiolipin antibodies
-
Diagnosis of VTE
- Given the increased risk of VTE in trauma patients, the clinician must always maintain a high index of suspicion.
- Physical exam findings:
-
- PE: tachycardia, tachypnea, mental status changes, diaphoresis
- DVT: extremity pain, fever, localized edema/swelling of the extremity, warmth/erythema of the extremity
-
- Lab and Radiology findings:
-
- Arterial blood gas—respiratory alkalosis, hypoxemia
- Chest x-ray—nonspecific, peripheral wedge defect
- Extremity duplex—occlusive/non-occlusive thrombosis
- CTA chest—filling defect(s)
- Echocardiography—impaired right ventricular function, intraventricular septum bulging into the left ventricle, dilated proximal pulmonary arteries, elevated right atrial pressure, elevated pulmonary artery pressure
-
VTE Prophylaxis Practice Management Guidelines for Trauma Patients
- Mechanical VTE prophylaxis
-
- All trauma patients, unless otherwise specified, should receive mechanical VTE prophylaxis with sequential compression devices (SCDs), injury permitting.
- SCDs should be worn while the patient is in bed or nonambulatory and may be removed when the patient is out of bed or ambulating.
- If the patient has sustained a lower extremity injury or has a known VTE in the lower extremity, a SCD should not be placed on the affected extremity.
-
- Pharmacologic VTE prophylaxis
-
- Enoxaparin is the preferred prophylaxis in trauma patients, as there are several studies showing superiority to unfractionated heparin in this patient population.
- All trauma patients, unless otherwise specified, should receive enoxaparin (Lovenox) dosed appropriately for weight every 12 hrs within 24 hrs of admission.
- If enoxaparin is contraindicated (renal insufficiency, history of HIT, etc), other options for pharmacologic prophylaxis include heparin or fondaparinux Please consult with the trauma attending and/or pharmacist if alternative VTE prophylaxis is being considered.
- VTE prophylaxis should not be held for operative procedures unless requested by the surgical attending.
-
- Weight Based Enoxaparin Dosing for VTE Prophylaxis in Trauma Patients:
-
- BMI < 30:
-
- Enoxaparin 30mg subcutaneous every 12 hours
- CrCl < 30 mL/min or renal replacement therapy: Heparin 5000units subcutaneous every 8 hours
-
- BMI < 30:
-
-
-
- BMI ≥30
-
- Enoxaparin 0.5mg/kg subcutaneous every 12 hours
- CrCl <30mL/min or renal replacement therapy: Heparin 7500 units subcutaneous every 8 hours
-
- BMI ≥30
-
- Utilize the pharmacist to assist with adjusting dose based on patient BMI, renal function, and anti-Xa levels.
Exceptions to VTE Prophylaxis Practice Managment Guidelines For Trauma Patients
-
-
· Traumatic Brain Injury
o VTE prophylaxis should be initiated within 48 hours following injury/procedure for patients with intracranial hemorrhages and after craniotomy unless CT head is not yet stable or otherwise stated by neurosurgical attending.
o VTE prophylaxis should be initiated 24 hours following last stable CT head unless specifically requested by the neurosurgical attending.
o TBI patients should initially be placed on enoxaparin 30 mg q12 hrs regardless of BMI with subsequent dose adjustments based on Anti-Xa levels.
o For patients with TBI requiring placement of an intracranial pressure (ICP) monitor, he/she should receive VTE prophylaxis with either enoxaparin 40 mg daily or heparin 5000 units q8hrs. After removal of the ICP monitor, prophylaxis should be changed back to enoxaparin dosed q12hrs.
o HOLD VTE prophylaxis 12 hours prior to removal of ICP monitor or EVD.
· Spinal cord injury
o VTE prophylaxis should be initiated on admission on those patients with a stable spinal cord injury requiring no surgical fixation.
o For patients requiring operative intervention for spinal cord injury, VTE prophylaxis should be initiated within 72 hours unless specifically requested to be held by the spine surgeon.
§ VTE prophylaxis should be held the morning of surgery and 48 hrs post-operatively initiate enoxaparin 40 mg daily for 5 days then transition to enoxaparin dosed appropriately for weight q12hrs.
o For patients with spinal drain in place, he/she should receive VTE prophylaxis with enoxaparin 40 mg daily. After removal of the spinal drain, prophylaxis should be changed back to enoxaparin dosed appropriately for weight q12hrs.
· Solid organ injury with non-operative management
o VTE prophylaxis should be initiated within 48 hours of admission for most solid organ injuries, unless specifically requested by the trauma attending.
· Pelvic fractures with active extravasation
o VTE prophylaxis should be initiated within 24 hours of admission for most pelvic fractures with active extravasation, unless specifically requested by the trauma attending.
· Patients presenting in hemorrhagic shock
o VTE prophylaxis should be initiated within 24 hrs of obtaining hemorrhage control, unless specifically requested by the trauma attending.
· Significant coagulopathy
o VTE prophylaxis should be initiated within 24 hrs of correcting coagulopathies, unless specifically quested by the trauma attending.
o Presence of underlying hepatic insufficiency resulting in ongoing coagulopathies may require the use of alternative pharmacologic VTE prophylaxis and should prompt a discussion between the trauma team and pharmacy.
· Epidural Placement
o Enoxaparin should be held 12 hours prior to epidural placement or removal.
o Enoxaparin should be held 4 hours following epidural removal.
o While the epidural is in place, enoxaparin should be dosed at 40 mg daily. Once epidural is removed, enoxaparin may be adjusted to the appropriate weight based dose q12hrs.
o Refer to MP02-Neuroaxial Procedure Policy for additional information.
· Renal Insufficiency
o For patients with a creatinine clearance <30mL/min, enoxaparin may be renally adjusted to 30mg daily or subcutaneous heparin dosed appropriately for weight q8hrs
o In patients receiving renal replacement therapy, subcutaneous heparin is recommended over enoxaparin.
· Pediatric patients
o Pediatric patients >15 yrs of age or younger patients in a postpubertal state and an ISS>25 should receive VTE prophylaxis with sequential compression devices (SCDs), injury permitting, and enoxaparin dosed appropriately for weight q12 hrs.
o Prepubescent patients <15 yrs of age should not routinely receive VTE prophylaxis.
-
LMWH Anti-Xa Level Monitoring
- Peak Anti-Xa levels will be drawn on the following trauma patients:
-
- Traumatic brain injuries with intracranial hemorrhage
- Orthopedic injuries requiring total joint replacements
- Patients with spinal cord injury
- Spine fractures requiring surgical fixation
- Renal insufficiency with creatinine clearance <50 ml/min or age >75 yrs.
- Prolonged ICU stay of 7 days or greater
-
- In these patients, the “Inpatient consult to pharmacist – Anticoagulation Other” order should be placed in EPIC. A pharmacist will assist in ordering levels at appropriate times, monitoring drug levels and adjusting dosages of medication as indicated.
- Peak Anti-Xa levels should be drawn 4 hours following the administration of enoxaparin. These labs should be ordered after the third or fourth dose of enoxaparin.
-
- Goal prophylaxis peak range is 0.2 to 0.4 IU/mL.
- Once the goal range is reached, no further monitoring is needed unless there is a change in the patient’s renal function (creatinine clearance).
- If the patient is not within the goal range and Anti-Xa level deemed to be drawn at appropriate time, the dose of enoxaparin may be adjusted up or down based on the desired effect.
-
Screening Measures for Trauma Patients
- VTE screening is not performed routinely in our trauma patients.
- Given the increased risk of VTE in trauma patients, the clinician must always maintain a high index of suspicion.
- If VTE is suspected, the initial study of choice is a lower extremity ultrasound with additional imaging/work-up as clinically indicated.
IVC Filter Placement
- Indications for a therapeutic IVC filter placement include patients with known PE or lower extremity DVT and a contraindication, failure or complication of anticoagulation.
- A prophylactic IVC filter may be considered in patients with the following:
-
- Spinal cord injury with paraplegia or quadriplegia
- IVC, iliac, or femoral venous ligation or repair
- Severe pelvic fracture with lower extremity long bone fracture
- AIS head >/=3 with contraindication to anticoagulation
- High risk patients with contraindication, failure or complications of anticoagulation.
-
References
- Rogers FB, Cipolle MD, Velmahos G, Rozycki G, Luchette FA. Practice management guidelines for the prevention of venous thromboembolism in trauma patients: the EAST practice management guideline workgroup. J Trauma. 2002;53:142-164
- Mahajerin A, Petty JK, Hanson SJ, Thompson AJ, et al. Prophylaxis against venous thromboembolism in pediatric trauma: a practice management guideline from the Eastern Association for the Surgery of Trauma and the Pediatric Trauma Society. J Trauma Acute Care Surgery. 2017;82(3):627-636.
- Whiting PS, White-Dzuro GA, Greenberg SE, et al. Risk factors for deep venous thrombosis following orthopedic trauma surgery: an analysis of 56,000 patients. Arc Trauma Res. 2016;5(1):e32915
- Geerts WH, Jay RM, Code KI, et al. A comparison of low-dose heparin with low-molecular weight-heparin as a prophylaxis against venous thromboembolism after major trauma. N Engl J Med. 1996;335:701-707.
- Phelan HA, Wolf SE, Norwood SH, et al. A randomized, double blinded, placebo-controlled pilot trial of anticoagulation in low-risk traumatic brain injury: the Delayed versus Early Enoxaparin Prophylaxis I (DEEP I) Study. J Trauma and Acute Care Surgery. 2012;73:1434-1441.
- Koehler DM, Shipman J, Davidson MA, Guillamondequi O. Is early venous thromboembolism prophylaxis safe in trauma patients with intracranial hemorrhage. J Trauma. 2011;70:324-329.
- Christie S. Thibualt-Halman G, Casha S. Acute pharmacological DVT prophylaxis after spinal cord injury. Journal of Neurotrauma. 2011;28:1509-1514.
- Clark NP. Low-molecular-weight heparin use in the obese, elderly and in renal insufficiency. Thrombosis Research. 2008;123:S58-S61.
- Scholten DJ, Hoedema RM, Sholten SE. A comparison of two different prophylactic dose regimens of low-molecular weight heparin in bariatric surgery. Obesity Surgery. 2002;12:19-24.
- Constantini TW, Min E, Box K, et al. Dose adjusting enoxaparin is necessary to achieve adequate venous thromboembolism prophylaxis in trauma patients. J Trauma Acute Care Surgery. 2013;74(1):128-135.
- Chapman SA, Irwin ED, Reicks P, Beilman GJ. Non-weight based enoxaparin dosing subtherapeutic in trauma patients. Journal of Surgical Research. 2016;201:181-187.
Last Updated
July 2025
Last edited by Abby Josef, MD- Associate Trauma Medical Director and Shelby Wells, PharmD- Critical Care Pharmacy
14. Care of the Trauma Patient
Information and miscellaneous things involved in caring for trauma patients throughout their acute hospitalization and beyond
Advanced Care Planning and Palliative Care Consultation in Acute Care Surgery
Purpose
· To engage injured or ill patient’s and/or families in discussions regarding goals of care and advanced care planning early and provide guidelines for Palliative Care consultation to assist in facilitating discussions surrounding goals of care and expectations of recovery following injury.
Background/Definitions
· Injury and illness is sudden, unpredictable and often life-altering. Patients and families display a variety of reactions after trauma and understanding the patient’s pre-existing psychosocial functioning is imperative to providing complete holistic care. Palliative care consultation can be a helpful service to patients by providing in depth discussion on goals of care related to prognosis and patient preferences, transitional planning, family support and symptom relief management.
Inclusion Criteria
- Age 55 years old or older
- ICU or SDCC admission (all ages)
- Multisystem injuries, specifically an upper and lower extremity injury
- >5 comorbidities
- Or provider discretion (consider things like homelessness, mental health, low social support, challenging injury)
- Should be done once in the inpatient setting- ie. Should not be done upon injury/in ER
Exclusion Criteria
- No absolutes
Diagnostic Evaluation
· Patients should be assessed per ATLS guidelines with labs, imaging, consults, and interventions as deemed necessary by trauma team to determine extent of injuries, co-morbid conditions, and general prognosis.
Similarly, emergency general surgery patients should be evaluated and managed as deemed appropriate for the current clinical status/diagnosis.
Practice Recommendations for Management
All acute care surgery patients: WITHIN 24 HRS OF ADMISSION
- An advanced care planning discussion should be held with patients (and/or the patient’s decision-making proxy) admitted to the trauma or emergency general surgery services within 24 hours of admission.
-
- For patient’s less than 19 years of age, discussions should occur with the patient’s legal guardian/parent.
-
- This initial advanced care planning discussion should be led by an acute care surgery service provider (physician or APP).
- The initial advanced care planning discussion should address the following:
-
- Code status
- Identification of health care proxy and decision maker in event patient is unable to make decisions.
- Identification of any advanced directives
- Prognostication based on patient’s injuries, co-morbid conditions, and clinical status.
- Goals and expectations throughout hospitalization and upon discharge.
- Frailty assessment in all patients >60 years of age (see Table 1) or in younger patients who have more than 5 pre-existing chronic medical conditions
-
Palliative care consultation screening (see Table 2)
- Palliative care consultation indicated/not indicated
-
- All advanced care planning discussions should be documented in the electronic medical record under the note type “advanced care planning”.
-
- Note template: .ACSACPINITIALACPDISCUSSION
-
-
Please use the ACP as an opportunity for a therapeutic discussion about the patient’s injuries and prognosis, and likely need for additional support. The goal should be to help explain the patient’s injuries, and guide expectations. If they are likely to need a facility, you can set the expectation that they may not go home, but give them encouragement to return home.
Triggers for Palliative Care Consultation based on initial advanced care planning discussion:
- Palliative care consultation should be considered if any of the following are present:
-
- Positive palliative care screen (Category 1 or 2)
- Frailty score greater than 3 (based on Frail Questionnaire, Table 1)
- Pre-existing end-stage or terminal condition
- A diagnosis with median survival less than 6 months
- Death expected during same ICU/hospital stay
- GCS<8 for greater than 1 week in patients >55 yrs.
- Multi-system organ failure
- Family disagreement with team, advanced directive or each other (lasting >2 days)
- Futility considered or declared by the medical team.
- Family request
- Acute Care Surgery attending discretion
-
- Palliative Care consultation ideally should occur early in patient's hospital course with a goal of assessing and managing the patient via "palliative care bundle" (see Table 3) within 72 hours of admission.
Triggers for Geriatrics Consultation for trauma patients based on initial advanced care planning discussion:
- All patients >75 years of age at admission
- Age 65-75, consider geriatric consultation if conditions listed below are present:
-
- dementia
- 10 or more home prescription medications
- 2 or more ED visits or inpatient admission in past 6 months
- not living independently or residents of nursing homes or assisted living facilities
- provider discretion
-
- in cases where patient's meet criteria for both Geriatrics and Palliative Care consultation:
-
- Request consultation of both services. Geriatrics will primarily assist with geriatric medical conditions, whereas Palliative Care will primarily assist with advance care planning/goals of care.
- This should occur with ongoing communication between Geriatric Medicine, Palliative Care and Trauma teams.
-
Triggers for Family Meeting WITHIN 72 HRS OF ADMISSION
- All Category II patients require a family meeting within 72 hrs of admission.
- Any patient lacking an advanced directive or healthcare proxy AND potential for challenging hospitalization or disposition.
- Family meeting may be led by Palliative Care, Geriatric Medicine or Trauma.
-
- An acute care surgery provider should be present for this discussion regardless of who leads the meeting.
-
- This advanced care planning discussion should be documented in the electronic medical record under the note type “advanced care planning”.
-
- Note template: .ACSACPFOLLOWUP
-
- The 72hr family meeting/follow-up discussion should address the following:
-
- Update on patient’s current clinical status with prognostication based on patient’s injuries, co-morbid conditions, and clinical status.
- The patient and/or family’s insight into the current problem(s).
- Hopes and fears for current hospitalization.
- Focused care plans based on patient’s injuries, co-morbid conditions, and clinical status (i.e. best case scenario, more-likely scenario, worst case scenario) with a set time-frame for when we will re-evaluate the situation.
-
- This should also include potential “what if’s” (e.g. trachs, PEGs/Feeding tubes, etc)
-
-
Follow-up Care
- Significant changes in a patient’s clinical status, should prompt additional advanced care planning discussions as needed.
- If consulted, palliative care will continue to follow the patient throughout his/her hospital course as indicated.
Outcome Measures and Guideline Adherence
- Timing and documentation of initial advanced care planning discussions will be monitored on 80% of all trauma patients
- Timing and utilization of palliative care services will be monitored on all trauma mortalities and hospice/CMO discharges.
- Pathway will be re-assessed following a 3 month pilot study.
Key Contributors
- Emily Cantrell, MD | Division of Acute Care Surgery | Author
- Charity Evans, MD | Division of Acute Care Surgery | Author
- Elizabeth Mahal, MD | Department of Emergency Medicine | Author
- Carrie Siedlik, APRN-NP | Palliative Care Medicine | Author
- Remy Kaslon, APRN-NP | Palliative Care Medicine | Author
- Katie Circo, RN | Nursing Professional Development Specialist MICU and SICU, Nebraska Medicine | Author
- Katherine Maliszewski, MD | Internal Medicine/Geriatric Medicine | Author
- Abby Josef, MD | Division of Acute Care Surgery | Updates Author
Last Updated
October, 2024
References
- American College of Surgeons. Trauma Quality Improvement Program Palliative Care Best Practice Guidelines. https://www.facs.org/media/g3rfegcn/palliative_guidelines.pdf
- American College of Surgeons. Trauma Quality Improvement Program Geriatric Trauma Management Guidelines. https://www.facs.org/media/314or1oq/geriatric_guidelines.pdf
- Fiorentino M, et al. Palliative care in trauma: Not just for the dying. J Trauma and Acute Care Surg. 2019:87(5):1156-1163.
Appendix and Supplemental Materials
Figure 1. Model for advanced care planning discussions and consultation of palliative care in trauma.
Table 1. 5 item FRAIL Questionnaire
Table 2. Palliative Care Screening in Trauma
*Surprise question example: “Would you be surprised if the patient died in the next 12 months?”
Table 3. Palliative Care Bundle
Guideline Algorithm
Alcohol Withdrawal Pathway- PAWSS
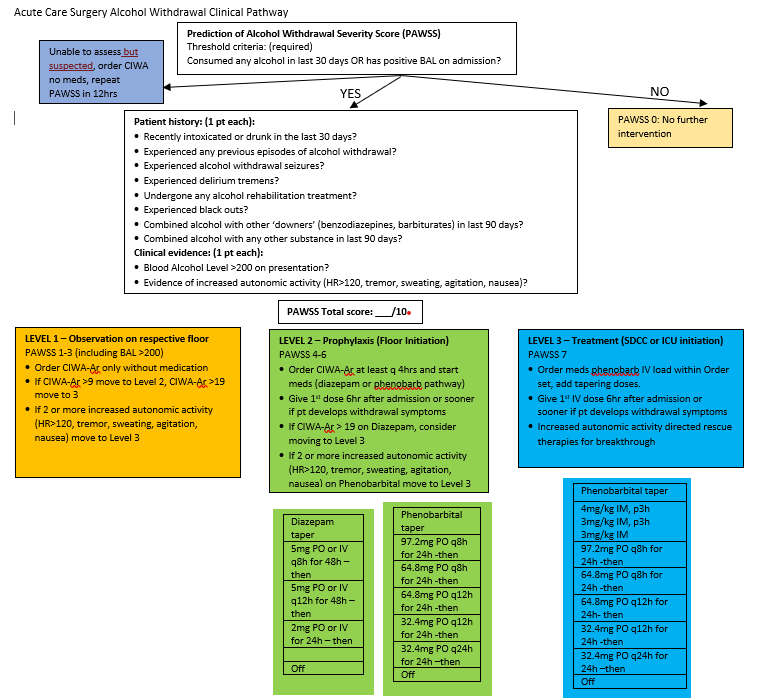
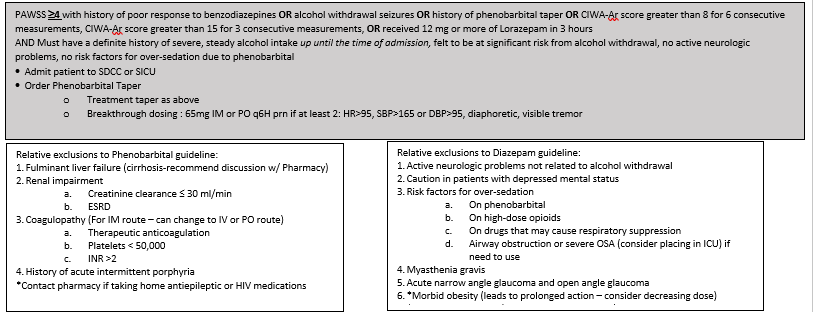

Date: January, 24, 2022
Key Contributor(s): Olabisi Sheppard, MD
Assessing Capacity
Why assess capacity? Informed consent promotes individual autonomy and fosters rational decision-making, and is founded on the right of self-determination and physician’s fiduciary responsibility to the patient. Informed consent requires disclosure of information, voluntary choice and capacity to decide. Therefore, determining a patient’s capacity is of utmost importance during a patient’s hospitalization.
Capacity refers to the ability to accept or refuse treatment recommendations. Capacity is determined by a clinician upon specific elements of a mental status exam. Capacity does not have to be a psychologist or psychiatrist.
Capacity differs from competency. Competency is defined as “the ability of an individual to participate in legal proceedings”. Legal competence is presumed - to disprove an individual's competence requires a hearing and presentation of evidence. Competence is determined by a judge. This legal determination is never determined by medical providers. Because this determination is not made by providers we will not use this term further in this pathway.
- Any patient who is observed to have functional deficits judged to be sufficiently great that the patient currently cannot meet the demands of a specific decision making situation and its inherent consequences SHOULD be assessed for capacity.
- Capacity is determined for individual decisions, and may vary by risk involved. For example, a patient may have capacity to refuse a bowel regimen but lack capacity to leave the hospital against medical advice.
- Capacity should be reassessed as decision-making abilities deteriorate or improve. Capacity also needs to be documented each time it is assessed.
- Speech therapy can provide the treatment team with additional information and expertise on cognition, to assist with the capacity assessment. However, cognition testing is not required for capacity assessment.
Discussions regarding a patient's capacity to make a decision should be documented in the electronic medical record in a short progress note using the assessing capacity note template.
The template can be found using the dot phrase = .acscapacityassessment
Example of note template in electronic medical record:
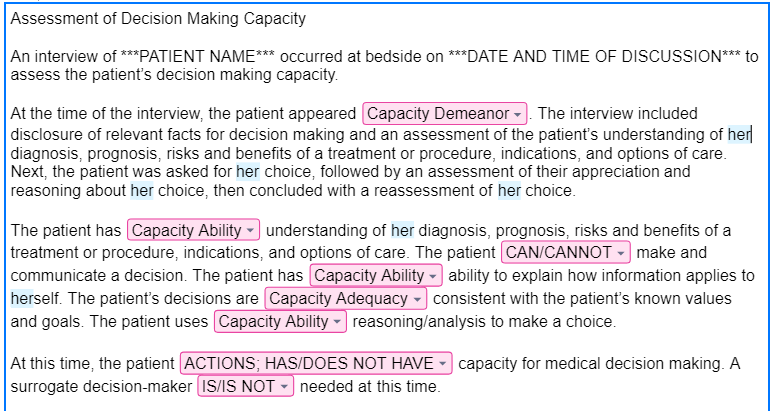
Evaluation and Management of Delirium
Purpose
Provide guidance on the evaluation, diagnosis, and management of hospitalized patients who develop delirium.
Background/Definitions
Delirium is a neuropsychiatric disorder that is characterized by a disturbance in attention, consciousness and cognition with a reduced ability to focus, sustain or shift attention. It can develop over a short period of time, is a change from baseline, and fluctuates in severity. The clinical presentation varies but usually presents with psychomotor behavioral disturbances such as hyperactivity or hypoactivity and with impairment in sleep duration and quality.
Delirium is caused by an underlying medical condition that is not better explained by another preexisting, evolving, or established neurocognitive disorder. The underlying cause of delirium can vary widely and involve anything that stresses the baseline homeostasis of a vulnerable patient. Examples include: substance abuse intoxication and withdrawal, medication side effects, infection, surgery, metabolic derangements, pain, constipation, and urinary retention.
There are 3 subtypes of delirium:
- Hyperactive: patients present with restlessness, purposeless and uncontrollable movements, agitation, hallucinations, and behaviors
- Hypoactive: patients appear calm, lethargic, and have slowed mentation and slow/decreased movements.
- Mixed: fluctuation between hyperactive and hypoactive states.
Delirium has consistently shown to be associated with higher mortality rates, longer ICU and hospital lengths of stay, increased morbidity, and cognitive and psychiatric sequelae that can persist weeks to months following hospital discharge.
The elderly, polytrauma patients and those critically ill in the ICU are all groups that have been identified as particularly susceptible to developing delirium. The incidence of delirium in trauma patients admitted to the ICU has been reported as up to 67%, with increased risk for elderly and those requiring mechanical ventilation.
In light of this, it is critical for trauma and critical care providers to be well versed in screening for and identifying delirium as well as implementing preventative strategies against delirium in order to optimize patient outcomes and reduce healthcare costs.
Guideline Inclusion Criteria
All admitted trauma patients
Guideline Exclusion Criteria
none
Diagnostic Evaluation
· Risk factors for delirium development:
Each trauma patient should be assessed for nonmodifiable and modifiable risk factors that may contribute to the development of delirium.
|
Nonmodifiable Risk Factors |
Modifiable Risk Factors |
|
Increased age |
Restraints |
|
Depressed GCS on arrival |
Ventilator days |
|
Increased blood product transfusion |
Increased sedation |
|
Multisystem organ failure |
Infection/sepsis |
|
Traumatic brain injury (TBI) |
Indwelling urinary catheters/lines |
|
History of substance abuse |
Medications |
|
Frailty |
|
|
Comorbidities (hypertension, dementia) |
|
|
Nutritional impairment |
|
|
Medications known to be associated with increased delirium can include: |
||||||||||||||||
|
· Patient care should be centered around optimizing modifiable risk factors as able in hopes of minimizing the risk of delirium development.
· Delirium Detection and monitoring:
The most reliable method for detecting delirium is with the use of externally validated screening tools. One of the more widely used screening tool is the Confusion Assessment Method for ICU (CAM-ICU) which is applied primarily to patients in the ICU. Alternatively, a Brief Confusion Assessment Method (bCAM) is primarily used for delirium screening on floor patients. (see Figure 1)
Practice Recommendations for Management
- All trauma patients should be assessed for delirium risk and development daily and as needed when a change in clinical status occurs and delirium is suspected. This includes optimizing modifiable risk factors and medication regimens as able and implementing delirium prevention strategies. (see Figure 2)
- If delirium is suspected, diagnosis should be confirmed by using the CAM-ICU or bCAM screening tools.
- Once delirium is confirmed, provider should examine/evaluate the patient for possible causes and contributing factors to delirium (i.e. infection, electrolyte abnormalities, medication side effects, substance intoxication/withdrawal, etc) and treat/correct as indicated by work-up (See FIGURE 3).
- In addition to correcting/treating contributing factors, provider should also implement delirium treatment interventions beginning with non-pharmacologic interventions first and escalating to pharmacologic interventions as needed. (see FIGURE 4)
-
-
- There are currently no pharmacologic agents shown to prevent the development of delirium or shorten the course of delirium. Pharmacologic agents should be used as needed to treat symptoms of delirium and prevent harm to patient and/or staff.
- If pharmacologic interventions are required, they should be preferentially used on an as needed basis with the minimal dose required to achieve the desired effect (i.e. not agitated or at risk to harm self/staff).
- If scheduled pharmacologic interventions are used, medications should be assessed daily for need and weaned/discontinued once delirium has resolved.
-
-
Follow-up Care
- All patients diagnosed with delirium during his/her hospital stay should be assessed daily and as needed for ongoing signs and symptoms of delirium and potential opportunities to optimize delirium prevention and treatment.
- Diagnosis of delirium should be well documented in the patient’s hospital discharge summary so that post-discharge cognitive and psychiatric sequelae may be assessed at follow-up visits with either trauma providers or patient’s primary care providers.
Outcome Measure and Guideline Adherence
- Diagnosis of delirium is actively tracked through our trauma performance improvement initiatives.
-
-
- Each case will be reviewed by our PI coordinators and TMD/aTMD at a primary and/or secondary review level to confirm diagnosis and assess for opportunities for improvement.
- If opportunities for improvement or trends identified, cases will be further examined at a secondary and/or tertiary review level in our weekly trauma performance improvement conference or monthly multi-disciplinary trauma meetings.
-
-
Related Policies
- Pharmaceutical Management of Post-TBI Neuropsychiatric Symptoms, Acute Care Surgery Patient Pathway, Nebraska Medicine.
Key Contributors
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Erin Panowicz, APRN | Division of Acute Care Surgery | Author
- Rebecca Sedlak, PharmD, BCCCP | Critical Care Pharmacy, Nebraska Medicine | Author
Last Updated
February, 2024
References
- Williams EC, Estime S, Kuza CM. Delirium in trauma ICUs: a review of incidence, risk factors, outcomes, and management. Curr Opin Anesthesiol. 2023 Apr;36(2):137-146.
- Devlin JW, Skrobik Y, Gelinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018 Sep;46(9):e825-e873.
- Shoulders BR, Elsabagh S, Tam DJ, et al. Risk factors for delirium and association of antipsychotic use with delirium progression in critically ill trauma patients. Am Surg. 2023 May;89(5):1610-1615.
- Ely EW, et al. Confusion Assessment Method for the Intensive Care Unit. JAMA. 2001; 286:2703-2710.
- Inouye SK, et al. Confusion Assessment Method. Ann Intern Med. 1990; 113:941-948.
Appendix/Supplemental Materials
FIGURE 1--Delirium Screening Tools
(a) Confusion Assessment Method for ICU (CAM-ICU)
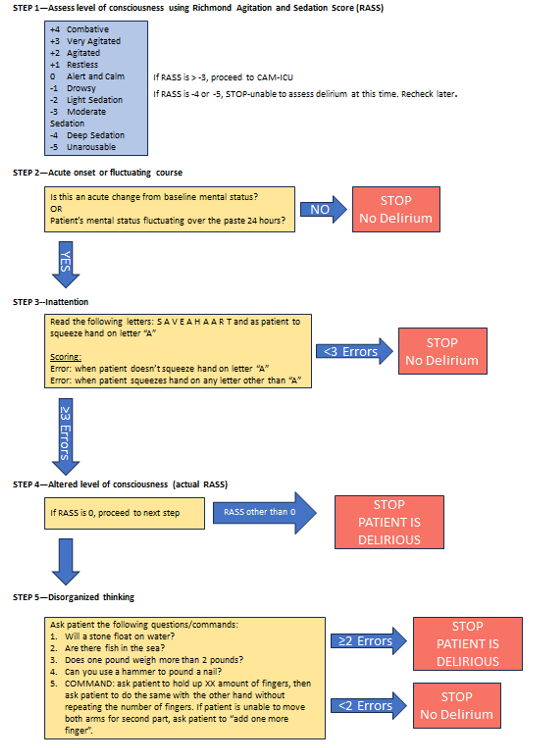
(b) Brief Confusion Assessment Method (bCAM) Flow Sheet
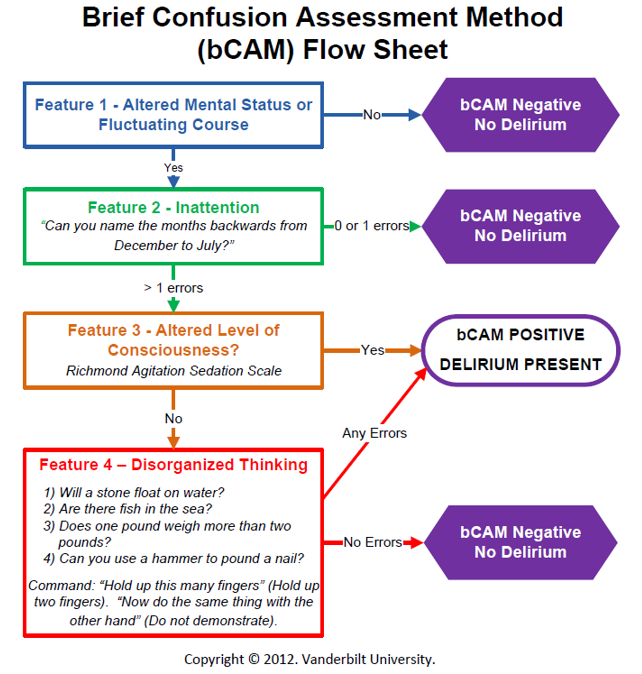
FIGURE 2-- Delirium Prevention Strategies
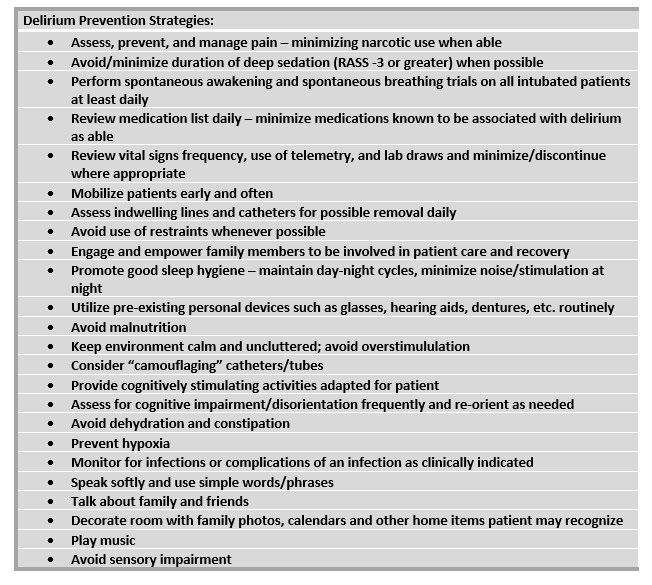
FIGURE 3--Suggested algorithm for management of delirium
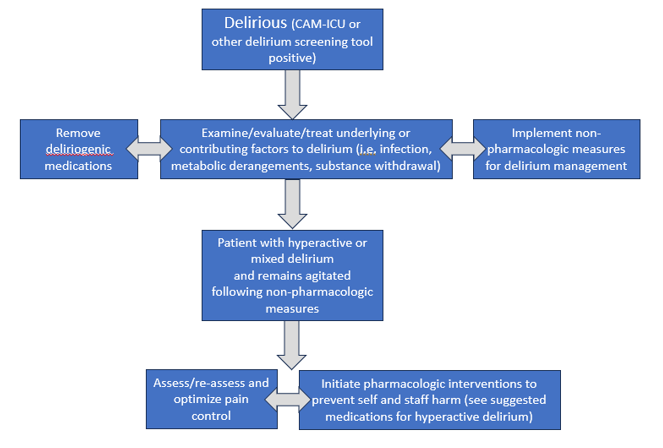
FIGURE 4--Non-pharmacologic and pharmacologic interventions for delirium
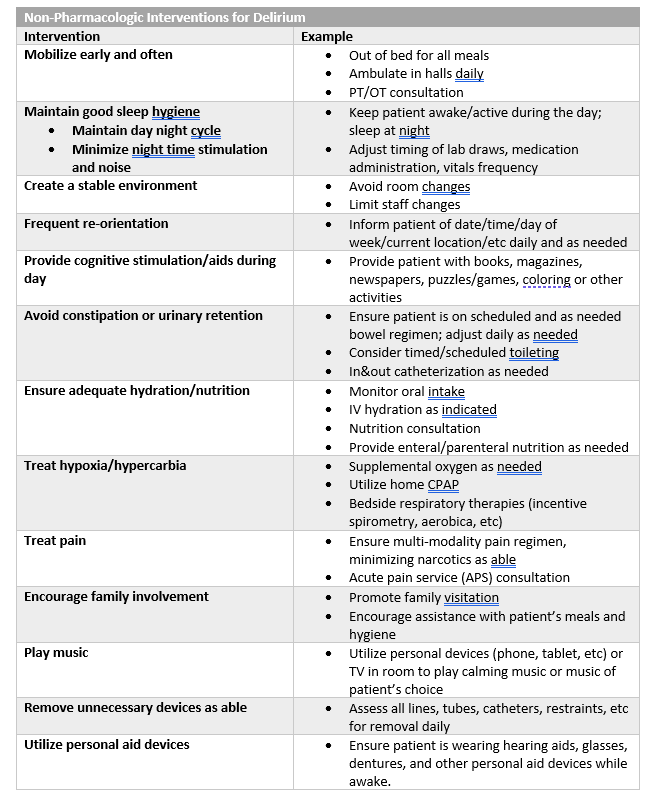
|
Pharmacologic Interventions for Delirium
|
|||
|
Class/Drug |
Suggested Use |
Dosing |
Adverse Effects |
|
Typical Antipsychotic: Haloperidol (Haldol)
|
Controlling acute severe agitation |
2.5-10 mg (usual dose 5 mg) IV/IM. May repeat Q15min (up to 20 mg) until calm achieved |
Oversedation, QT prolongation, arrythmia, extrapyramidal symptoms, dopaminergic antagonism (avoid in Parkinsons), may lower seizure threshold |
|
Controlling intermittent (or breakthrough) agitation |
2.5- 5 mg Q4H PRN agitation |
||
|
Atypical Antipsychotics: |
|
||
|
Quetiapine (Seroquel) |
Maintaining control of agitation associated with hyperactive/ mixed delirium
|
Typical start: 50 mg PO/perFT Q8-12hr. If effect not achieved at 24 hours, may increase dose (max 400 mg/day). |
Oversedation, QT prolongation (less than IV haloperidol), extrapyramidal symptoms (less than haloperidol) |
|
Olanzapine (Zyprexa) |
Typical start: 5 mg PO/perFT daily. If effect not achieved at 24 hours, may increase dose (max of 20 mg/day). |
||
|
Risperidone (Risperdal) |
Controlling acute agitation |
1-2 mg PO/per FT. May repeat dose in 1-2 hours, up to 6mg in 24 hours.
|
|
|
Central Alpha-2 Agonist: Dexmedetomidine (Precedex) |
Maintaining control of agitation associated with delirium |
If intubated: 0.2-1.5 mcg/kg/hour continuous infusion
If extubated: 0.2-0.7 mcg/kg/hour continuous infusion, order expires at 24-hours, must reassess and reorder if still indicated. |
Restricted to ICU and SDCC. No bolus dosing allowed.
Hypotension, bradycardia, withdrawal (if use prolonged) |
|
Benzodiazepine: Lorazepam (Ativan) |
Controlling severe acute agitation—not typically used as 1st line
|
0.5-1 mg IV/PO/perFT, may repeat in 15 min |
AVOID if able as BZDs causes/exacerbate delirium.
Oversedation |
|
Acceptable option for alcohol withdrawal, agitation in patient with chronic benzo use, agitation in Parkinson’s |
0.25-1 mg IV/PO/perFT Q4-6H PRN agitation |
||
|
Anticonvulsant: Valproic Acid (Depakote) |
For agitation refractory to other agents (ie adequate analgesia/ sedation, antipsychotics). May be especially useful when associated with substance withdrawal or untreated mood (ie bipolar) disorder
|
Typical start: 250 mg IV/PO/perFT Q8H. If effect not achieved at 24 hours, may increase by 250 mg increments.
May use loading dose for acute control: 15 mg/kg (~ 1000 mg)
|
Hepatotoxicity, hyperammonemia, thrombocytopenia, drug interaction with carbapenems
Safe therapeutic range: 50-125 mcg/mL |
|
Endogenous Hormone: Melatonin |
Consider if insomnia is contributing to delirium |
3 mg PO/perFT QHS, may increase to 9 mg |
Daytime drowsiness, limited side effects |
|
SSRI: Trazodone
|
Potentially useful if insomnia is contributing to delirium (2nd line) |
25-50 mg PO/perFT QHS |
Daytime drowsiness, antihistamine effects, sensory distortion, sleep walking |
|
For all added medications for delirium/agitation: · Start at lowest (or a 50% reduced dose) in elderly (ie >65 yoa). · These medications are not for long-term use, reassess daily. Delirium often resolves/improves over several days and the agents should be weaned/discontinued if no longer indicated. |
|||
Forensic Examiner Program Nebraska Medicine

Summary – Law Enforcement Requests for Patient Information
| Law Enforcement Request | NM Staff Response | |
| 1 |
Staff safety/security concerns |
Staff may always request law enforcement’s presence when concerned for their safety/security. |
| 2 |
Requests for patient information, general rule | Ok to disclose patient information as permitted in this chart, by our policies (see policy IM12), or with written patient authorization (form CON MR 0074) |
| 3 |
Patient condition | Ok to disclose one-word condition status without patient authorization: undetermined, good, fair, serious, or critical |
| 4 |
Date of birth (DOB) |
Ok to disclose if:
|
| 5 |
Blood or urine test specimen/results |
Do not provide test specimen or test results to law enforcement UNLESS:
|
| 6 |
Notify law enforcement when patient is discharged | Ok if provided court order that requires such notification or patient is in police custody. Otherwise, decline to provide this notification. See policy LD-12. |
| 7 |
Forms • Court order • Subpoena • Warrant |
Ok to provide information specifically referenced in any of these documents. Forward document to HIM for processing. If urgent request that can’t wait for HIM, Nebraska Medicine staff may contact Risk (consult Web On Call or hospital operator to reach on-call Risk staff) or Legal with any questions. |
| 8 |
Victims of Crime |
If patient is victim of crime and unable to authorize disclosure because incapacitated or there are other emergency circumstances, NM staff may disclose patient info to law enforcement if law enforcement: • states information is needed to determine whether someone other than patient violated law, |
| 9 |
Identification of: • suspect • fugitive • material witness • missing person |
Ok to disclose only the following information if requested by law enforcement to identify suspect, fugitive, material witness, or • name and address |
| 10 |
Interviews Patient is in police custody |
Ok for law enforcement officer to be present/ask patient questions UNLESS presence would impede staff’s ability to provide patient care or compromise sterilization/infection control procedures |
| 11 |
Interviews Patient is not in police custody |
Ok for law enforcement officer to be present/ask patient questions IF patient agrees and presence would not impede staff’s ability to provide patient care or compromise sterilization/infection control |
| 12 |
Visitation restrictions Patient is in police custody |
Ok to restrict visitor access per law enforcement officer’s direction. |
| 13 |
Visitation restrictions Patient is not in police custody |
Ok to grant law enforcement officer’s request to speak with patient before visitors are allowed to visit patient in two situations: 1. patient agrees to request and honoring request does not impede patient care or compromise sterilization/infection control |
| 14 |
Wounds of Violence (excluding sexual assault) |
If NM staff suspect patient injury caused by crime (excluding sexual assault), must report to law enforcement: victim’s name, description of victim’s physical injury, and, if ascertainable, victim’s residential address and location of offense. See policy PE 03. |
| 15 |
Sexual assault | If patient was 18+ years at time of sexual assault and provides written consent or patient is suffering from serious bodily injury or any bodily injury caused by deadly weapon, which appears to have been received in connection with or as a result of sexual assault, must report following to law enforcement: victim’s name, description of victim’s physical injury, and, if ascertainable, victim’s residential address and location of the offense. |
| 16 |
Child Abuse or Neglect | For suspected child abuse or neglect, see the following policies for related reporting obligations and permitted disclosures: • PE 03 (Reporting of Abuse, Neglect or Injury) • SH21 (Infant Drug Testing Guidelines for Providers) • AD48 (Drug Testing Guidelines for Providers: Pregnant and Postpartum Patients) |
15. Recovery of the Trauma Patient
Indications to Consult Physiatry (PMR)
Purpose
To identify criteria for early physiatry (PMR) consultation and expertise on the multidisciplinary trauma care team following admission.
PMR Consult Service
The PMR consult service is ran by Dr. Dan Pierce. He is available to see consults on patients admitted to the trauma service on Monday, Wednesday, and Fridays and provide additional expertise the management and care of various injury as treatment moves from the acute phase to the recovery and rehabilitation phase.
Indications for Consult
1. Spinal cord injury (timing: ideally as soon after admission as possible)
- All acute spinal cord injured patients (cervical/thoracic/lumbosacral and conus medullaris/cauda equina), including pediatrics
-
- Perform ISNCSCI (ASIA Impairment Scale) exam
- Management of physiatry-related complications following trauma
-
- Neurogenic bowel/bladder
- Orthostatic Hypotension/Autonomic Dysreflexia
- Concomitant brain injury care
- Spasticity management/contracture prevention
- Pulmonary/vent weaning
- Prevention of skin breakdown
- Pain
-
- Assist in transition to post-acute care
-
- Including insurance denials/peer-to-peer
- Coordinate rehabilitation care (PT/OT/ST) prior to discharge
-
- Patient/family education
-
- Including presence at family meetings and prognosis discussions
-
-
- All chronic spinal cord injured patients if they have a new injury and are admitted to trauma service
2. Traumatic Brain Injury (timing: ideally as soon after admission as possible)
- Severe and moderate brain injuries, including pediatrics
-
- Management of physiatry-related complications following trauma
-
- Arousal
- Agitation secondary to post-traumatic amnesia
- Paroxysmal Sympathetic Hyperactivity (“neurostorming”)
- Neurogenic bowel/bladder
- Spasticity management/contracture prevention
- Prevention of skin breakdown
- Pain
-
- Assist in transition to post-acute care
-
- Including insurance denials/peer-to-peer
- Coordinate rehabilitation care (PT/OT/ST) prior to discharge
-
- § Patient/family education
-
- Including presence at family meetings and prognosis discussions
-
- Management of physiatry-related complications following trauma
-
3. Traumatic limb loss (timing: ideally as soon after admission as possible)
- Upper and Lower extremity, including pediatrics
-
- Management of physiatry-related complications following trauma
-
- Contracture prevention
- Pain
-
- Assist in transition to post-acute care
-
- Including insurance denials/peer-to-peer
- coordinate rehabilitation care (PT/OT/P&O) prior to discharge
-
- Patient/family education
-
- Including presence at family meetings and prognosis discussions
-
- Management of physiatry-related complications following trauma
-
Consultations for the following injuries may also be considered and will be seen on an as needed basis during the patient's hospital admission:
- multiple musculoskeletal trauma
- traumatic peripheral nerve injuries, including crush
- pediatric traumas
- mild-moderate brain injury
- burns
- other injuries requiring post-acute rehabilitation
Author(s)
Dan Pierce, MD, Department of Physical Medicine and Rehabilitation
Last Updated
June, 2023
17. Trauma Resident Resources
Frequently Used Pages
Day-to-day guides
Trauma Patient Admission Criteria
Frequent Clinical Pathways
C-spine evaluation and management
Care of patients with rib fractures
Neurotrauma Quick Reference
Head injury:
All adult patients with blunt traumatic brain injury should be classified according to the mBIG criteria. Neurosurgical consultation is indicated for all patients who are mBIG 3. mBIG 1 and 2 patients should be managed according to the pathway.
Penetrating traumatic brain injury mandates neurosurgical consultation.
Cervical spine:
All blunt trauma patients should be placed in cervical spine precautions until the cervical spine can be appropriately evaluated. The cervical spine can be cleared clinically using established criteria such as the NEXUS or Canadian C-spine criteria. If the cervical spine is imaged, a CT c-spine should be performed. If imaging identifies a cervical spine fracture, the remainder of the spine must be imaged and a CT angiogram of the neck must be performed. Spine must be consulted for all cervical spine fractures (including spinous processes and transverse processes).
If there is no cervical spine fracture, the cervical spine must be cleared by a clinical exam. If the patient has persistent pain on exam without fracture, a second attempt should be made to clear the cervical spine within 12-24 hours. If they still have pain, they can continue to wear a cervical collar and follow up in spine clinic in two weeks. MRI of the cervical spine should be reserved for patients where the presence of a c-collar may result in significant morbidity, such as elderly patients or those at risk for dysphagia. MRI c-spine should be approved by the trauma attending prior to ordering.
Blunt cerebrovascular injury:
Patients with the follow injuries require CTA neck to screen for BCVI:
· High-energy transfer mechanism
· Displaced midface fracture (Lefort II or III)
· Mandible Fracture
· Complex skull fracture/basilar skull fracture/occipital condyle fracture
· Severe TBI with GCS <6
· Cervical spine fracture, subluxation, or ligamentous injury at any level
· Near hanging with anoxic brain injury
· Clothesline type injury or seat belt abrasion with significant swelling, pain, or altered mental status
· TBI with thoracic injuries
· Scalp degloving
· Thoracic vascular injuries
· Blunt cardiac rupture
· Upper rib fracture
BCVI should be managed according to the grade of the injury (see pathway). Neurosurgery consultation is only absolutely required for grade 3-4 injuries.
Thoracic/Lumbar spine:
Spinous and transverse process fractures only require spine consultation if they meet the following criteria:
· 4 or more contiguous TP fractures / SP fractures
· Bilateral TP fractures / SP fractures (regardless of the # of fractures)
· All C-spine TP fractures / SP fractures
Fractures read as subacute or chronic should be discussed with the attending prior to consulting the spine service.
Trauma Resident Week at a Glance
Trauma week at a glance:
Monday:
6am signout
8:30am – run list with team + Molli (case manager); Red Couch Room
9am – Rounds
6pm signout – resident night coverage
Tuesday:
6am signout
7:30am – trauma resident education lecture; Chair Conference Room
8:30am – run list with team + Molli (case manager); Red Couch Room
9am - Rounds
12pm – SICU Conference; Chair Conference Room
1pm – trauma resident weekly checkin with Bauman/Cantrell/Josef/Tierney; Chair Conference Room
6pm signout – APP night coverage
Wednesday:
6am signout
7am-noon – general surgery resident education
9am – run list with team + Molli (case manager); Red Couch Room
9:30am – rounds
6pm signout – APP night coverage
Thursday:
6am signout
7am – Trauma Performance Improvement; Chair Conference Room (not the first week of the month)
8am-noon – EM resident education
8:30am – run list with team + Molli (case manager); Red Couch Room
9am - Rounds
6pm – signout – APP night coverage
Friday:
6am signout
8:30am – run list with team + Molli (case manager); Red Couch Room
9am – Rounds
12pm – SICU Ultrasound Conference; Chair Conference Room
6pm – signout – resident night coverage
Saturday
6am signout
8:30 AM – run list with attending, followed by rounds
6pm signout – resident night coverage
Sunday:
6am signout
8:30 AM – run list with attending, followed by rounds
6pm signout – resident night coverage