ACS Roles & Responsibilities (2025-2026)
Acute Care Surgery - Roles and Responsibilities
2025-2026
Purpose: The purpose of this document is to outline the roles and responsibilities for each team member providing patient care on the Acute Care Surgery service in order to provide coordinated and timely care. This document serves as a guideline that can and should be adjusted according to the needs of the patient and the needs of other patients requiring concurrent care.
Guiding Principles
· Teamwork: Acute Care Surgery includes multiple service lines, each unique to their patient population and staff coverage. In addition, we are one team with one mission- to offer the highest level of care to our patients. We will support each other in any way needed to achieve our mission.
· Communication: Caring for acutely injured and ill patients requires clear, closed loop communication delivered in a respectful and professional manner.
· Leadership: Acute Care Surgery is present in all arenas of Nebraska Medicine- including the ER, OR, floor, ICU and clinic. Given our large footprint, all members of the Acute Care Surgery team must act as leaders and a resource to any person or patient at Nebraska Medicine who asks for our help or input.

Contents
Faculty Commitments………..………………………………………………………………………....………..
ACS Residents…………………………………………………………………………………………......….………..
Weekdays flow- Monday thru Friday………………………………………………………………………
CCS Provider Team Roles and Responsibilities……………………………………………………….
CCS Attendings (Green and Yellow)……………………………………………………………
CCS Fellows…………………………………………………………………………………….………….
CCS Residents……………………………………………………………………………………..…….
CCS Advanced Practice Providers (APP)…………………………………………………..
ICU Presentations Format………………………………………………………………………....
Trauma Team Roles and Responsibilities ………………………………………………………….....
Red Team Attending………………………………………………………………………………....
Red Team Residents…………………………………………………………………………………….
Red Team residents – days………………………………………………………....
Red Team residents – nights……………………………………………………….
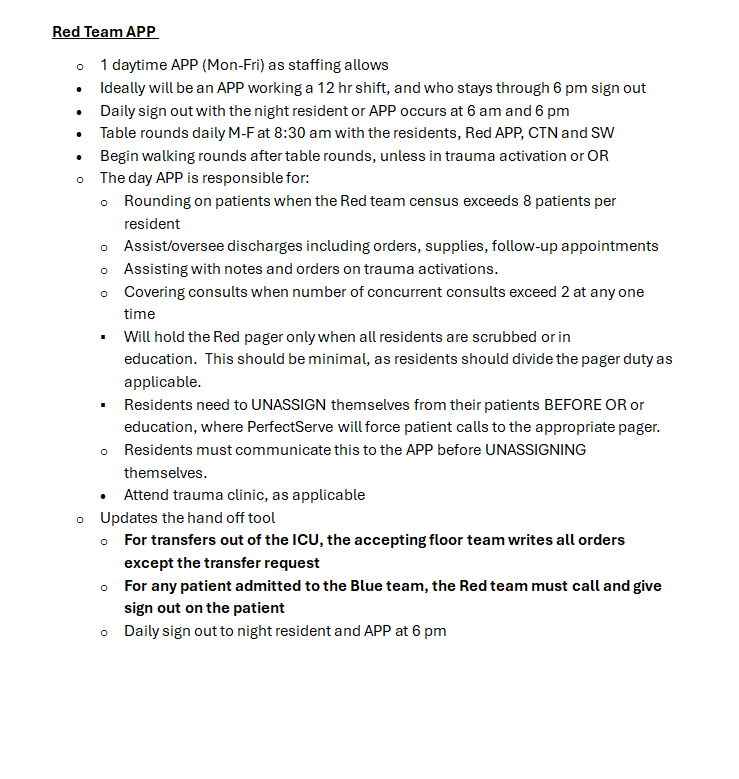
Red Team APP……………………………………………………………………………………………
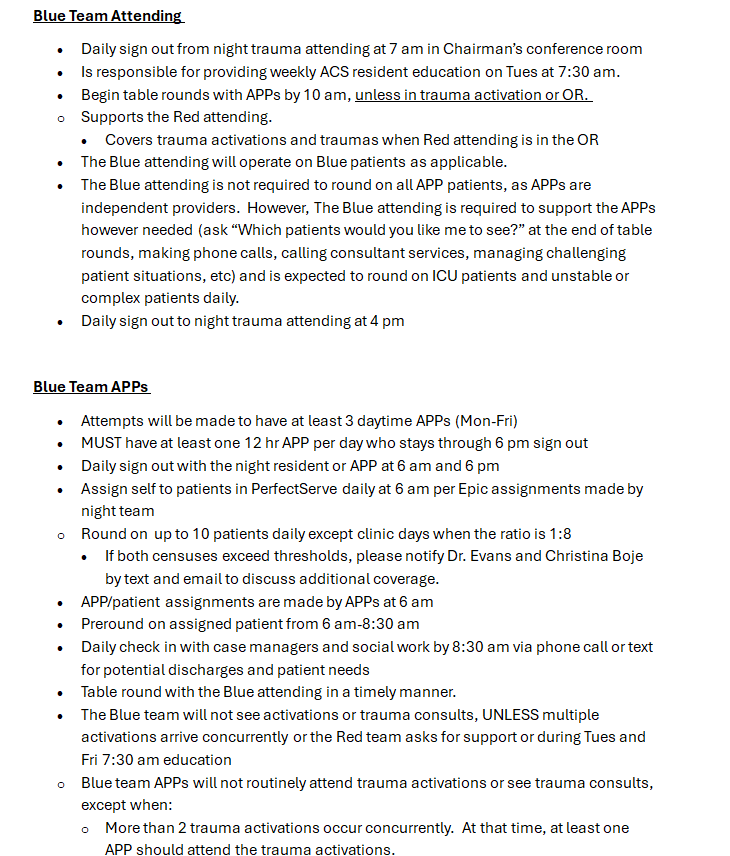
Blue Team Attending…………………………………………………………………………………..
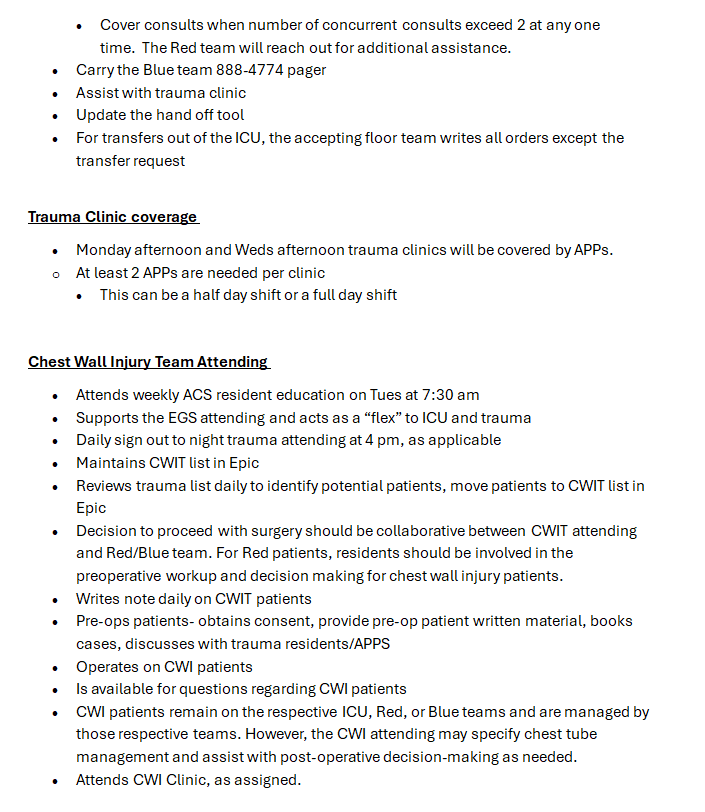
Blue Team APPs…………………………………………………………………………………………
Trauma Clinic Coverage……………………………………………………………………………
Chest Wall Injury Attending………………………………………………………………………
Nights APPs Roles and Responsibilities ..……………………………………………………….........
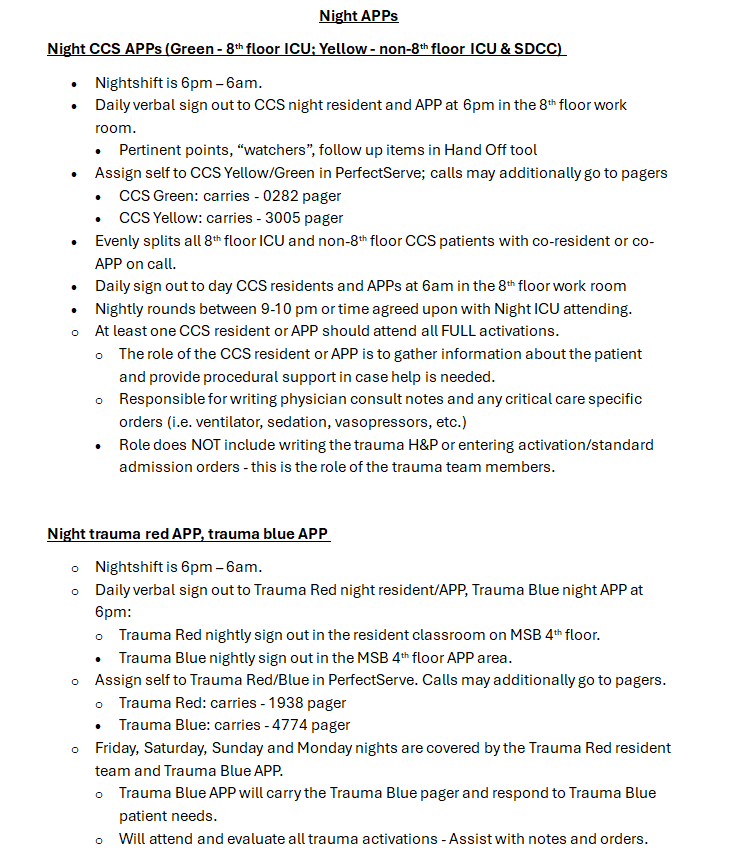
Night CCS APPs…………………………………………………………………………………………....
Night trauma red APP, trauma blue APP………………………………………………………
EGS Team Roles and Responsibilities ………………………….………………………..………..........
EGS team attending………………………………………………………………………….……….
EGS team APP-days…………………………………………………………………………..……….
EGS team clinic………………………………………………………………………………..………..
EGS team residents-days…………………………………………………………………………….
EGS residents-night……………………………………………………………………………..…….
Faculty Commitments
Faculty Commitments
Mission: Our mission is to provide the highest quality of care compassionately delivered for the traumatically injured, critically ill and emergency surgical patients, to educate tomorrow’s surgeons, and advance the field of acute care surgery through research and innovation.
Values:
• Patient Care: Providing safe, quality and compassionate care to each patient is the core of all we do.
• Education: We commit to a program of educational excellence to train the next generation of surgeons.
• Discovery: We perform innovative research and develop novel programs to enhance the practice of surgery.
• Culture: We value safety, teamwork and wellbeing in our behaviors and beliefs.
• Reputation: We uphold a national reputation of providing high-quality compassionate medical care, premier educational programs, and innovative research.
Baseline Professional Obligations:
· Maintain all clinical requirements- including but not limited to: bedside rounding on all resident patients, bedside rounding on all ICU patients, FCOTS, other aspects as described in Roles and Responsibilities documents
· Maintain all nonclinical requirements- including but not limited to ATLS instruction, attendance at M and M (division and departmental), Grand Rounds and weekly faculty meetings, division resident and fellow lectures
· Outlook email and Outlook calendar as a primary form of communication, including schedules, updates, announcements.
· Complete compliance training by due date
· Attend faculty meetings >50%
· 3-day documentation goal of 95% or greater
· Complete yearly ADIS evaluations by due date
· Be on time for 7 am and 4 pm faculty sign outs
· Assigned PI charts are completed within 2 weeks of assignment. Charts will be assigned on the 1st of each month.
o If a vacation or personal time falls within these two weeks, please notify PI and Dr Evans and give a completion date
· Attend weekly and monthly PI/PIPS > 50%
· Division chief will provide faculty scheduling 2 months in advance. In order to maintain ongoing schedules, faculty will:
o Email vacation and non clinical requests to division chief, lead administrative assistant, and personal assistant by 1st of month according to schedule
o Once approved, the request will be placed on the master calendar and faculty’s personal calendar.
o Errors made in scheduling will be corrected by division chief.
o Once a schedule is deemed final, it is the faculty’s responsibility to find their own replacement, except in cases of personal emergencies, where the division chief will assist.
· Requests to attend meetings will be prioritized according to those with: podium presentations, committee obligations, poster presentations followed by those wishing to go for educational purposes
· Requests for vacation/time off will be on a first come, first served basis
· Non-clinical days (days where you are not assigned rounding or clinic or call) are administrative days, created to allow time for education, research, administrative work, further contribution to the division/department/university/hospital.
o Available for meetings in person or via zoom, with response within 2 hrs to request
o If you are not available administratively on a nonclinical day, that day should be taken as Paid Time Off.
§ To ensure adequate time off, place Out of Office automatic reply on email with other contact information
§ Recruit a partner to cover your Epic inbox while away
§ Complete all required tasks PRIOR to leaving on vacation
· Act as an ATLS instructor or director twice per year
· Contribute two fellow lectures per year
· Contribute to the creation or editing of 2 patient pathways per year.
· Baseline medical student and resident education obligations, set by the department.
Acute Care Surgery faculty members must meet the baseline professional expectations outlined by Nebraska Medicine, the Department of Surgery, and the Division of Acute Care Surgery to be eligible for the Value Based Incentive Payment based on the Corporate Scorecard metrics and metrics listed above.
ACS Residents
ACS Residents
Residents are an integral part of all acute care surgery service lines, and none of our services can function without resident support. The educational goal for all ACS service lines is to learn how to take care of some of the sickest patients in the hospital, both in and out of the operating room. Success on ACS services requires the ability to triage, as we frequently have long lists, multiple operating rooms, and multiple admissions. In general, the expectation of residents on all services include:
· Review orientation materials prior to starting on service
· Obtain signout on the service from the resident you’re replacing; this should include information about the structure of the service as well as the specific patients
· Obtain morning signout and give evening signout
· Round on your assigned patients, but be familiar with all patients on the service. We work as a team, and everyone is expected to be able to provide care for any patient at any time.
· Ensure all operative cases are covered by an appropriate level resident
· Run the list and round with the attending
· Communicate with all consultants and/or primary services
· Complete all notes in a timely manner
· Be familiar with ACS pathways and apply them when indicated
· Attend required education for your residency program/department
· Attend scheduled ACS educational conferences
· Work collaboratively on a multidisciplinary team
· Read about relevant pathology during your time on service. Resources to consider reading include: Marino’s ICU Category, Trauma (the red category), Top Knife (for trauma intraoperative decision making), in addition to the general surgical textcategory of your choice such as Cameron’s/Schwartz/Sabiston’s. 
Weekday Flow - Monday thru Friday
Weekdays flow- Monday thru Friday
· 7 am- night attending sign out to day attending in Chairman’s conference room
o ALL day/night rounding faculty should attend- serves as our sounding board
o Any additional faculty are encouraged to attend
· Night ICU to day 8th fl ICU attending and non-8th fl ICU attending
· Night EGS/Trauma to day EGS attending and day Trauma attending
· 7:30am-8:30am Tuesdays- RESIDENT EDUCATION in Chairman’s conference room. ALL ACS faculty will attend, as available. Educating the residents will be a group effort.
· Green and yellow rounds start at 9:00am all week in their respective units
· Red trauma rounds start at 8:30 am in the Chairman’s conference room for talking rounds with the CTN and SW (M-F). This will be followed by walking rounds at 9 am. On Sat/Sun, walking rounds start at 8:30 am.
· Blue trauma rounds will start by 10 am- continue to check in with the APPs that morning for optimal time to meet.
· EGS rounds start at 8:30 am.
· On Weds with Grand Rounds, all rounds pushed back to 9 am, with walking rounds at 9:30 am for Red Trauma
· Fellow education scheduled for Tuesdays at 12 noon
· ALL ACS faculty will attend, as available. Educating the fellows will be a group effort.
· 4 pm-day attending sign out to night attending in individual faculty offices
· Day ICU to and non-8th fl ICU attending to night 8th fl ICU attending
· Day EGS attending and day Trauma attending to night EGS/trauma attending
· No formal 6 pm sign out. EGS, trauma and ICU teams will sign out independently. 
CCS Provider Team Roles & Responsibilities
CCS Provider Team Roles and Responsibilities***
CCS Attendings (Green and Yellow) 
CCS Green Attending - Responsible for all patients on the CCS service located on the 8thfloor of Clarkson TowerCCS Yellow Attending - Responsible for all patients on the CCS service located in locations outside the 8thfloor of Clarkson TowerAttend daily morning sign-out from night CCS attending in Chairman’s conference roomAttends weekly ACS Resident and CCS Fellow educationCCS rounds begin by 9:00 am daily. Deviations from this time should be limited, but if done, the time should be clearly communicated to the rounding team.The CCS Attending facilitates and encourages good communication regarding daily plans and clinical status changes to the primary surgical services.The CCS Attending is responsible for seeing all new admissions on the CCS service in a timely manner.The CCS Attending is responsible for communicating with members of the CCS team anytime a patient transitions out of the operating room. If the patient is unstable, physical presence at bedside to facilitate appropriate transition of care is appropriate.If a patient on the CCS service is undergoing evaluation for organ donation, the CCS attending is responsible for facilitating and encouraging good communication with the OPO team.The CCS Attending is responsible for mediating any conflict that arises while on service and elevating any problems to the CCS medical director or ACS division chief and/or the SICU Nurse Manager if necessary.Each CCS attending (Green and Yellow) supports and provides back up for each other if neededCCS attending should afternoon round prior to 4pm sign-outAfternoon sign-out to night CCS attending at 4 pm daily. The night CCS Attending covers both CCS services (Green and Yellow).The night CCS Attending carries the ACS transfer phone and is responsible for communicating any transfer requests to the surgical service as appropriate.
***
o The CCS ICU attendings are expected to be physically present, as needed, in the ICU. To support this:
o The CCS attending will not operate in OR, unless needed. 
o The CCS attending will be responsible for all bedside procedures (percutaneous trach, PEGs, central lines, etc.) 
o Bedside exploratory laparotomies will be performed by the respective surgical service attending with the assistance of the surgical intensivist.
CCS Fellows
· The CCS Fellow should take leadership in all aspects of the critical care team. The CCS attending will be present and provide support as needed.
· Attend daily sign out from night CCS Attending at 7 am in Chairman’s conference room. Daily sign out to night CCS attending occurs at 4 pm in faculty office
· Attend weekly CCS Fellow education.
· Prepare for and lead monthly CCS M&M
· The CCS Fellow facilitates and encourages good communication regarding daily plans and clinical status changes to the primary surgical services.
· The CCS Fellow is responsible for seeing all new admissions on the CCS service in a timely manner.
· The CCS Fellow is responsible for communicating with members of the CCS team anytime a patient transitions out of the operating room and be present at bedside when the patient arrives.
· If a patient on the CCS service is undergoing evaluation for organ donation, the CCS Fellow is responsible for facilitating and encouraging good communication with the OPO team.
· The CCS Fellow is responsible for mediating any conflict that arises while on service and elevating any problems to the CCS Attending, CCS Medical Director or ACS Division Chief and/or the SICU Nurse Manager if necessary.
· The CCS fellow’s primary responsibility is for the CCS team they are assigned to (yellow or green) but will provide support and back up if needed for all patients on the CCS service.
· The CCS Fellow will supervise APPs and Residents during all bedside procedures.
· CCS fellows to provide support as needed to cover resident patients while residents are absent for required education days.
· The CCS Fellow is to attend monthly ICU leadership meetings with CCS Medical Director.
CCS Residents
· Attend daily sign out from night resident and APP at 6 am in the SICU provider work room.
· Assign self to PerfectServe daily at 6 am at start of shift. The CCS Resident will be primarily assigned to patients on the CCS green team. If needed, the CCS resident will provide patient care support to patients on the yellow service based on census, acuity and APP coverage needs.
· Preround on assigned patient prior to formal CCS rounds at approximately 9:00 am.
· CCS rounds begin at 9:00 am daily. Patients will be presented in a systems-based format. See the template below.
· The CCS resident will provide support to other residents and APPs while not presenting by putting in orders/pulling up images/finding answers and updating the hand off tool.
· Complete ACP note on new CCS admissions within the first 24 hours of admission. Mark as completed on the handoff tool
· Pay attention during rounds. The overall expectation is that everyone on the team knows pertinent details about every patient.
· The CCS resident will complete the daily progress note documentation using the CCS note template. It is the responsibility of the CCS Resident to document a unique note daily to ensure an accurate clinical narrative and promote effective communication. Along with documentation of the daily note, the resident should also update the problem list and rounding tab accordingly.
· Responsibility for new CCS consults should be shared between CCS residents and APPs, no matter if the patient is going to be admitted to yellow or green.
o A CCS Resident or APP should attend all FULL trauma activations.
· Role of the ICU resident or APP is to gather information about the patient, provide procedural support in case where help is needed.
· The CCS Resident facilitates and encourages good communication regarding daily plans and clinical status changes to the primary surgical services.
· The CCS Resident is responsible for seeing any new admissions in a timely manner along with presentation of that patient to the fellow/attending.
· The CCS Resident is responsible for communicating with members of the CCS team anytime a patient transitions out of the operating room and should be present at bedside when the patient arrives for handoff.
· The CCS resident is responsible for communicating any change in patients’ status to the CCS fellow and/or the CCS attending in a timely manner, especially if the patient has a change in neurologic/respiratory status and/or becomes hemodynamically unstable.
· It is the responsibility of the CCS resident to document any significant patient event or status change in the medical record as appropriate via the progress note or short progress note.
· The CCS resident is responsible for performing bedside procedures under the supervision of the CCS Attending and/or CCS Fellow. The CCS Attending and Fellow should be informed about any bedside procedure being performed. The CCS Attending/Fellow will be present and supervising as appropriate.
o Carries the CCS Green pager (0282)
o Consults will be called through the pager or PerfectServe
o The person who is carrying the pager is not solely responsible for all consults.
· Consults should be delegated based on workload and availability.
o Daily sign out to night resident and APP is at 6 pm in the SICU provider work room.
o If a night CCS resident is present, they will be assigned to patients on the CCS Green team.
· Pertinent points, “watchers”, follow up items should be documented in the Hand Off tool
· Attends weekly ACS Resident and CCS Fellow education
o ICU residents and APPs will place the Bed Request when a patient is ready for transfer out of the ICU. The floor residents and APPs will reconcile the orders, upon bed transfer.
o CCS residents and APPs will CALL (text message is not sufficient) the floor resident or APP at time of decision to transfer to floor status to provide updates/handoff on that patient
o Identify FLOOR STATUS on the handoff and remove CCS from the handoff tool as well. MUST go in and transition primary team to trauma red/blue/EGS, whatever applies to that patient.
· Transfer to floor status on non-ACS patients should be a joint discussion with primary team (such as CRS, MIS, Urology, etc.)
o Residents are required to attend their respective departments education.
o CCS Resident is still responsible to be present at both hand off at 6AM and 6PM even on education days.
o On assigned education days, CCS Resident should still pre-round and see their patients prior to leaving for education. They should hand off to another Resident, APP, or Fellow system-based rounding with pertinent information for rounds on all patients while they are gone.
CCS Advanced Practice Providers (APP)
· Attend daily sign out from night resident and APP at 6 am in the SICU provider work room.
· Assign self to PerfectServe daily at 6 am at start of shift. The CCS APP will be assigned to patients on both the CCS yellow and CCS green teams.
· MUST have at least one 12 hr. APP per day who stays through 6 pm sign out
· Daily sign out from night resident and APP at 6 am in the SICU provider work room
· Preround on assigned patient prior to formal CCS rounds at approximately 9:00 am
· CCS rounds begin at 9:00 am daily. Patients will be presented in a systems-based format. See the template below.
· The CCS APP will provide support to other residents and APPs while not presenting by putting in orders/pulling up images/finding answers and updating the hand off tool.
· Complete ACP note on new CCS admissions within the first 24 hours of admission. Mark as completed on the handoff tool
· Pay attention during rounds. The overall expectation is that everyone on the team knows pertinent details about every patient.
· The CCS APP will complete the daily progress note documentation using the CCS note template. It is the responsibility of the CCS APP to document a unique note daily to ensure an accurate clinical narrative and promote effective communication. Along with documentation of the daily note, the APP should also update the problem list and rounding tab accordingly.
· Responsibility for new CCS consults should be shared between CCS residents and APPs, no matter if the patient is going to be admitted to yellow or green.
o A CCS Resident or APP should attend all FULL trauma activations.
· Role of the ICU resident or APP is to gather information about the patient, provide procedural support in case where help is needed.
· The CCS APP facilitates and encourages good communication regarding daily plans and clinical status changes to the primary surgical services.
· The CCS APP is responsible for seeing any new admissions in a timely manner along with presentation of that patient to the fellow/attending.
· The CCS APP is responsible for communicating with members of the CCS team anytime a patient transitions out of the operating room and should be present at bedside when the patient arrives for handoff.
· The CCS APP is responsible for communicating any change in patients’ status to the CCS fellow and/or the CCS attending in a timely manner, especially if the patient has a change in neurologic/respiratory status and/or becomes hemodynamically unstable.
· It is the responsibility of the CCS resident to document any significant patient event or status change in the medical record as appropriate via the progress note or short progress note.
· The CCS APP is responsible for performing bedside procedures under the supervision of the CCS Attending and/or CCS Fellow. The CCS Attending and Fellow should be informed about any bedside procedure being performed. The CCS Attending/Fellow will be present and supervising as appropriate.
o Carries –0335 yellow pager
o Consults will be called through the pager or PerfectServe
o The person who is carrying the pager is not solely responsible for all consults.
· Consults should be delegated based on workload and availability.
· Attendance to weekly CCS Fellow education highly recommended
· Assist with covering resident patients and round presentations when residents are at required education days
o Daily sign out to night resident and APP is at 6 pm in the SICU provider work room.
o If a night CCS resident is present, they will be assigned to patients on the CCS Green team.
o AT LEAST ONE DAY ICU APP needs to stay for 6 pm sign out. Day APPs cannot sign out their patients to the residents, or vice versa.
· Pertinent points, “watchers”, follow up items should be documented in the Hand Off tool
o ICU residents and APPs will place the Bed Request when a patient is ready for transfer out of the ICU. The floor residents and APPs will reconcile the orders, upon bed transfer.
o CCS residents and APPs will CALL (text message is not sufficient) the floor resident or APP at time of decision to transfer to floor status to provide updates/handoff on that patient
o Identify FLOOR STATUS on the handoff and remove CCS from the handoff tool as well. MUST go in and transition primary team to trauma red/blue/EGS, whatever applies to that patient.
o Transfer to floor status on non-ACS patients should be a joint discussion with primary team (such as CRS, MIS, Urology, etc.)
ICU Presentations Format
Presentation in the ICU should be systems-based for all patients. Within each system, problems should be identified and addressed, and a plan should be proposed.
The following format should be used:
Neurologic – including pain/sedation, RASS goals, home medications, brain/spine injuries
Cardiovascular – including HR/BP, pressor requirement, PMH, home medications
Pulmonary – including vent settings, oxygen needs, chest wall/pulmonary injuries, chest tubes, SBT plan and results
Gastrointestinal – including diet, GI prophylaxis, abdominal injuries/pathology/operations
Genitourinary – including foley, ins and outs, electrolyte abnormalities, diuresis
Hematologic – including Hb/Hct, platelets, coagulopathy, home anticoagulation and indication, DVT prophylaxis
Infectious disease – WBC, temperature, active infections, culture results and sensitivities, antibiotic indication/duration/end of therapy
Endocrine – including glucose control, PMH, home medications, steroid use
Musculoskeletal – including orthopedic injuries and facial fractures, PT, OT, activity orders
Lines/tubes/drains - central line location/indication/duration, arterial line location/indication/duration, foley indication
Prophylaxis – GI and DVT
Disposition – Indication for continued ICU care vs transfer to floor
Family message – brief status update for the day that can be conveyed to family by any team member
Trauma Team Roles and Responsibilities
Nights APPs Roles and Responsibilities
EGS Team Roles and Responsibilities