Trauma orientation manual
Welcome to Trauma Surgery! Our vision for your rotation is to offer the highest level of care to our patients while teaching residents and students to provide outstanding clinical care to injured and critically ill patients. You will care for patients in a team comprised of residents from general surgery, surgical subspecialities, and emergency medicine, as well as advanced practice providers, and will interact regularly with a variety of consulting services. All residents are expected to be present and ready to work and function on the service on the FIRST day of the rotation.
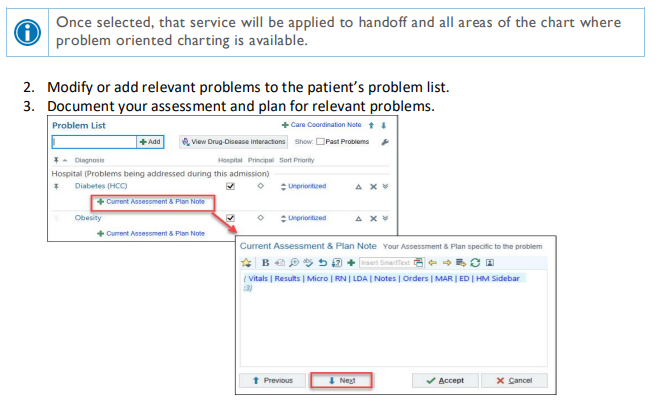
Our Team- Physicians
|
Attending |
Pager |
Cell |
|
Zachary Bauman, DO |
402-888-1131 |
712-251-0895 |
|
Chris Barrett, MD |
402-888-6080 |
651-497-7846 |
|
Joseph Baus, MD |
402-888-1800 |
614-975-5446 |
|
Bennett Berning, MD |
402-888-5527 |
312-208-7465 |
|
Keely Buesing, MD |
402-888-0563 |
402-312-0984 |
|
Emily Cantrell, MD |
402-888-1201 |
336-775-8889 |
|
Samuel Cemaj, MD |
402-888-1203 |
402-305-5809 |
|
Charity Evans, MD |
402-888-0525 |
312-231-0897 |
|
Matthew Goede, MD |
402-888-3770 |
402-881-7345 |
|
Mark Hamill, MD |
402-888-5484 |
843-324-8252 |
|
Reginald Henry, MD |
402-888-6336 |
408-203-8272 |
|
Abigail Josef, MD |
402-888-5525 |
402-715-0029 |
|
Andrew Kamien, MD |
402-888-1453 |
716-228-0118 |
|
Kevin Kemp, MD |
402-888-2545 |
510-378-2215 |
|
Gina Lamb, MD |
402-888-6333 |
802-681-5911 |
|
Mike Matos, DO |
402-888-5655 |
304-482-2712 |
|
David Mercer, MD |
402-888-3758 |
402-889-3431 |
|
Olabisi Sheppard, MD |
402-888-5034 |
913-271-7241 |
|
William (Hillman) Terzian, MD |
402-888-5526 |
703-505-1058 |
|
John Tierney, MD |
402-888-6079 |
480-703-4556 |
|
Jessica Veatch, MD |
|
303-726-0736 |
|
Brett Waibel, MD |
402-888-0698 |
252-414-8586 |
|
Levi Zehr, MD |
|
402-380-4086 |
Trauma Protocols/Patient Pathways
Current treatment protocols and guidelines for the service are available on the Acute Care Surgery pathways website, which is available at paths.trauma.ai
Login: trauma
Password: path402
PLEASE ADD THIS WEBSITE TO THE HOME SCREEN ON YOUR PHONE FOR QUICK ACCESS during the rotation.
This website is updated constantly. Please refer to it regularly to ensure that all trauma patients receive consistent high-quality care. Up-to-date contact information for trauma faculty, APPs, and support staff is also available on the website.
Trauma Services
There are two trauma services – the Red Resident Service and the Blue APP Service. Any patient can be admitted to either service. In general, however, the following criteria should be followed as a guideline:
Assignments to Red resident team
-
Operated on by Red Resident team, excluding PEGs and trachs
-
Injury patterns that will likely require a trauma surgery (excluding ribs, see below)
-
Requiring serial abdominal exams
-
Grade 3 or higher solid organ injuries
-
Greater than 5 rib fractures or bilateral (not all rib fractures go to red. Rib fractures can go to either team)
-
Pts which will greatly enhance the resident’s education
Assignments to Blue resident team
-
Operated on by Blue APP team
-
APPs should come to OR to assist with surgeries on Blue pts where residents are not assisting. Please communicate that day with the trauma attending to ensure operative coverage of those patients.
-
Isolated head or extremity injury
-
Blue team should carry more of the LTC patients
Patients can be moved between services on at the end of the day on Mondays and Fridays WITH ATTENDING APPROVAL if there is a significant imbalance between the censuses. Additionally, if a Blue patient undergoes an operation with resident support (excluding trach, PEG, and ribs), that patient should be moved to the Red service (e.g. a Blue patient admitted with a femur fracture develops a small bowel obstruction that requires an ex-lap).
Work Hours
Each resident is responsible for his or her own duty hours. It is expected and mandated by the ACGME, University of Nebraska Medical Center, the Department of Surgery, and the trauma service that residents will average no more than 80 hours per week averaged over four weeks, and receive one day off per week, averaged over four weeks. The call schedule has been designed so that all residents will be in compliance with duty hours. If you anticipate duty hour violations, you must communicate these issues with Dr. Tierney immediately.
Pagers/PerfectServe
888-1938 is the Red trauma pager- is carried by a Red resident during day and nights Fri-Mon. (APP will carry T, W, Th nights)
888-4774 is the Blue trauma pager- is carried by a Blue APP day and night
888-0282 is the Green SICU pager- is carried by a Green resident during day and night
888-3005 is the Yellow Non 8th Fl pager- is carried by an APP day and night
888-0447 is the EGS pager
All residents are required to have PerfectServe downloaded and active. All patient calls will go through PerfectServe. The pagers listed above serve as back up to PerfectServe.
One person is assigned daily per team in PerfectServe to receive patient inquires:
-Intern/junior on Red
-Senior resident on 8th floor ICU
-APP on Blue
-Backup in PerfectServe is senior resident
-Second backup is service pager
EVERYONE needs a trauma pager, because activations still go through the pager system and are not available on PerfectServe. See the Acute Care Surgery admins outside Dr. Bauman’s office to obtain one.
Equitable distribution of consults - run consults thru chief or upper level resident first, but ensure that they are staffed with attending in timely manner. If the Red attending is not available, please staff consults or urgent issues with the Blue, Green or Yellow attending. During sterile procedures or difficult conversations, you must ask a colleague or RN to return your pages in real time, as they are received, in order to facilitate care.
Team Member Responsibilities
Red Attending:
The Red attending is the primary attending who rounds on Red patients, covers activations, and does operative cases and procedures on all Red patients.
Blue Attending:
The Blue attending rounds on the Blue service with APP support, and also serves as the backup trauma attending for activations when the Red attending is not available. The Blue attending will operate on Blue patients who need operations. Typically, these are chest tubes, trachs, PEGs, wound debridements. Although the patients are admitted to the Blue service, these procedures and cases should still be covered by a resident.
Chest Wall Attending:
One attending is assigned to cover the Chest Wall Injury Team on weekdays. This attending will do any chest wall injury cases. The decision to refer a patient to the Chest Wall Injury Team should be discussed with the primary rounding Red or Blue attending. Chest wall cases on both Red and Blue patients should be covered by residents depending on the needs of the service.
Surgery Chief:
-
The on-call surgery chief is responsible for the workings of the entire service and should lead all activations.
-
The chief resident should be at the foot of the bed during activations and oversee the junior resident, who is performing the primary and secondary surveys.
-
Know all protocols/pathways and formulate workup plan for all patients, with attending supervision.
-
Perform or supervise all procedures in the ED and on the floor
-
Know all information about all patients on service prior to formal rounds with attending. (This does not require that you have seen every patient personally, but does require that you know information in the chart, have run the list with the team, and have assigned appropriate level providers to see each patient.)
-
Ensure that all OR cases are covered by an appropriate level resident.
-
Round on all ICU patients and communicate with the ICU team regarding plans.
Surgery Junior:
-
Preround on assigned patients. The surgery junior should in general be assigned to see post-operative patients.
-
Be at bedside during all activations to do the primary and secondary survey.
-
Assist with or perform all bedside procedures on the floor or in the trauma bay, with supervision from the chief resident.
Off-service Surgery Intern, EM Intern:
-
Preround on assigned patients.
-
Do primary and secondary surveys at bedside during activations when surgery junior is not available
-
-
Start H&P and problem list and place orders during activations when surgery junior is available to bedside
-
Be familiar with all patients admitted to the service and with their plans for the day, so that patient care is not compromised when the chief/junior are in the OR
-
Participate in bedside procedures
-
If the rest of the team is in the OR, work with the Red APP to ensure that the patient care continues to progress for the remainder of the service.
-
The Blue attending is the backup attending during the day, and the ICU attending is the backup at night. If a patient has a change in status (new tachycardia, arrhythmia, hypotension, hypoxia, altered mental status, hemorrhage, sepsis, etc), and the rest of the team is in the operating room, it is your responsibility to alert the backup attending immediately.
-
If you have a question regarding the existing plan of care that cannot be answered by the Red APP, go to the operating room to ask for help.
Red APP:
An APP is assigned to the Red service Monday-Friday. The primary role of the APP is to support the team, and not to serve as a primary rounder. The APP should:
-
Assist with notes and order on activations
-
Help facilitate communication with therapy, case management, and social work
-
Assist with discharges.
-
Be familiar with all patients on the service, and should hold the pager/PerfectServe and continue to advance care on the entire service when all residents are scrubbed or in education.
The APP is responsible for rounding on patients when the Red census exceeds a 1:10 provider-to-patient ratio.
On the weekends, there is no Red APP, but the Blue APPs are expected to attend and assist with activations.
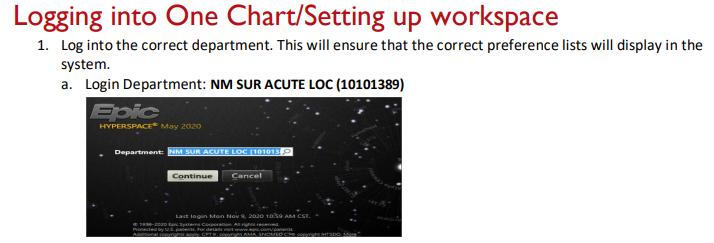
Workspace
The trauma APPs have workspace on MSB 4th fl. We also encourage regular use of the 9th floor trauma work room, so that you are immediately available to a large number of our patients.
Departmental Education
Tues: 7:30 am Acute Care Surgery education conference in the Chairman’s conference room MSB 45119
**This is mandatory for all residents on trauma and EGS. If there is an operative case, one resident can leave conference once the patient is being prepped. The attending is expected to get patients back to the OR without resident support for first start cases on Tuesday mornings.
Residents are required to attend their department’s regularly scheduled education conferences.
Wed: 7a-12noon General Surgery
Thurs: 8a-1p ER
Hand offs
6 am: Sign out from night resident and/or APP in 9th floor trauma room
6:00-8:30am: Preround on assigned patients. Ensure that your name is listed in the Epic column “Surg Pt Status” for the patients you are rounding on.
8:30am: Round with attending. This can be adjusted depending on OR schedule, activations, or at attending discretion. If there are significant changes in patient status, do not wait for rounds to tell your chief/senior/attending.
6 pm: Face-to-face handoff from day to night team in MSB 45119
-
Concise, focused (not rounds), discuss unstable patients in detail
-
Entire sign out should take less than 20 minutes
Bedside Multidisciplinary Rounds
After sign out, begin pre-rounding
-
Bedside Multi-disciplinary rounds will start around 8:30 am (at rounding attending’s discretion)
-
Expectations for rounds:
-
-See your patients in advance
-
-Know all injuries
-
-Know vital signs (Tmax, T current, HR, RR, BP, O2 saturation and oxygen needs)
-
-Know ins and outs (total ins/outs for 24 hour period, urine/ostomy/drain/tube outputs broken down by 12 hour shifts)
-
-Know today’s labs and imaging results
-
-Know up-to-date plans from consultants
-
-Know PT/OT recommendations for discharge (home vs SNF vs rehab)
-
-Examine every wound every day before attending rounds, unless specifically directed otherwise
Text or page Pharmacy just before start of rounds
Patient’s bedside RN should be involved in the patient’s discussion and engaged in rounds
Resident or APP must be logged into a computer at all times:
-
Laboratory results/trends
-
Pull up daily imaging and other data
-
Enter orders in real time
-
Resident or APP presenting the patient should not be the person entering orders at the computer
Daily Flow
Following bedside multidisciplinary rounds……….
-
Get work done.
-
Call Consults first
-
Then do Discharges- requires close collaboration with Case Management and Social Work
-
Attend trauma activations
-
Do tertiary exams – should occur as close to 24 hours after admission as possible
-
Do bedside procedures and operations (trauma floor residents operate on trauma ICU patients)
If surgery residents are in the OR, APP and non-surgical residents are expected to carry the pager, continue responding to activations, and advance care for all patients on the entire service (even patients who were seen in the morning by an operating resident). Each resident is expected to know the general plan for every patient on service to ensure that all patients receive high-quality care at all times.
4:00 PM - Afternoon rounds with APPs and residents
-
Review new patients
-
Swift and focused updates on stable existing patients
-
Address questions from RNs, RTs
-
New plans for unstable or deteriorating patient
Night Flow
-
APP coverage Tuesday-Thursday
-
Resident coverage Friday-Monday
-
Attend trauma activations
-
Complete items to assist day team:
-
Tertiary exams
-
Populate the problem list, update the patient list through the Problem List tab
-
Review all orders, cancel duplicate orders
Trauma Activations
-
All team members should respond to trauma activations
-
Once in activation, can determine if some members can return to other clinical duties. Upper-level residents and APPs will assist with this process
-
It is not uncommon to get multiple traumas at once. Dispatch will provide the following information over the pagers for full or limited activations as instructed by ED Lead/Charge RN or designee
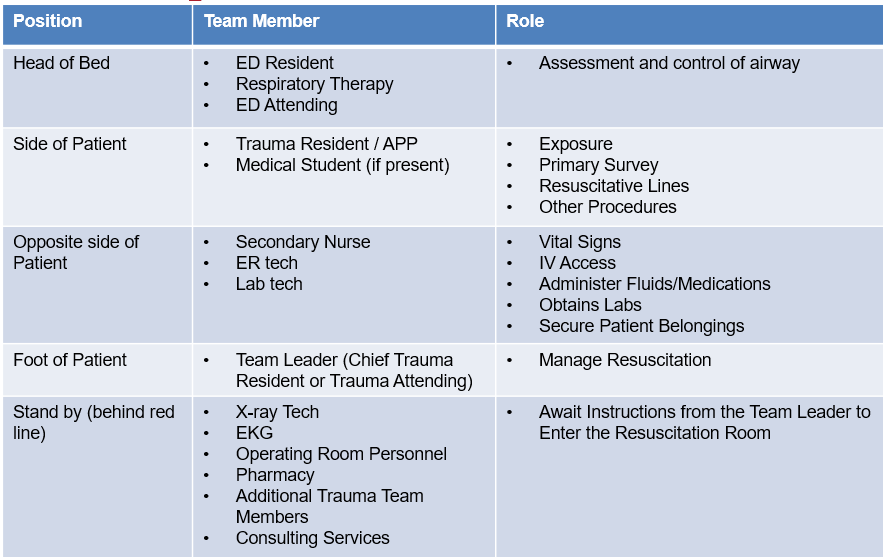
Trauma Roles and Responsibilities during Trauma Activation
-
Prior to patient arrival: Participate in the PreBrief (see poster on wall), introduce yourself and your position, preassign roles, ensure equipment is ready and available
-
Patient arrives: EMS providers give 30 second overview/report, during which there should be no talking
-
Pt moved to trauma bay bed: ABCDEs with closed loop communication and log roll with C spine precautions (for blunt trauma)
-
ER tech places pulse ox, then obtains first BP, then EKG monitor, then temperature
-
IVs placed, blood obtained
-
CXR for all blunt trauma patients, PXR for pts with unstable pelvis or pelvic pain (discuss with attending), FAST for blunt unstable or penetrating wounds to cardiac box.
-
Penetrating trauma patients need early exposure to look for wounds. Wounds should be marked with paper clips, then x-rays should be obtained of all cavities with a wound.
-
CXR must be reviewed by senior resident before CT
-
Secondary survey then CTs (only when patient is stable)
-
Trauma team member must accompany patient to CT
-
Follow up FINAL reads on all patients; go to radiology to review scans
-
ADD PATIENT TO Epic Trauma list
-
Participate in DeBrief (see poster on wall)
H&P and Progress Notes
-
Full = Full trauma activation
-
Limited = Limited trauma activation
-
Consult = No trauma activation but seen in the ED. This includes patient worked by EM first AND transfers from outside that are seen in the ED by trauma. The ED does not see transfers that are “consults.”
-
Direct Admit = Transfer from outside that goes directly to an inpatient bed, never seen in ED at any point.
-
Any trauma patient with a traumatic injury or physical/social circumstance which requires observation is admitted to Trauma
-
Outside hospital transfers: If you receive a page or call regarding an outside hospital transfer, please refer the caller to the attending on call. All transfers need to be approved by the Attending on call.
Tertiary Exams
-
Must be done within 24 hrs.
-
AND repeat once the patient can participate (specifically, in head injured or intubated patients)
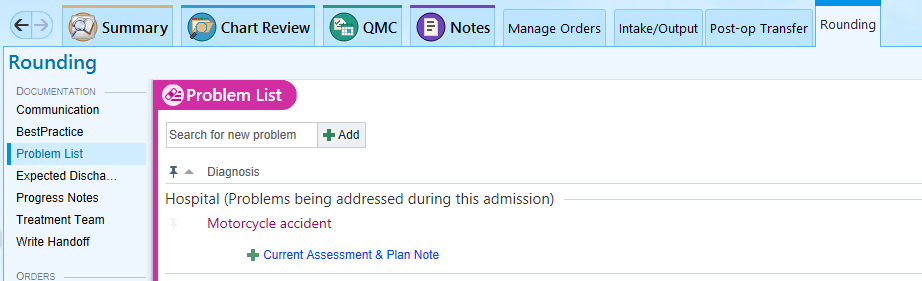
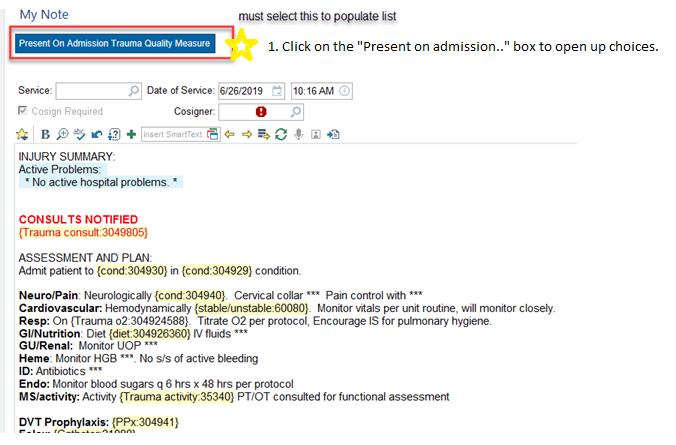
-
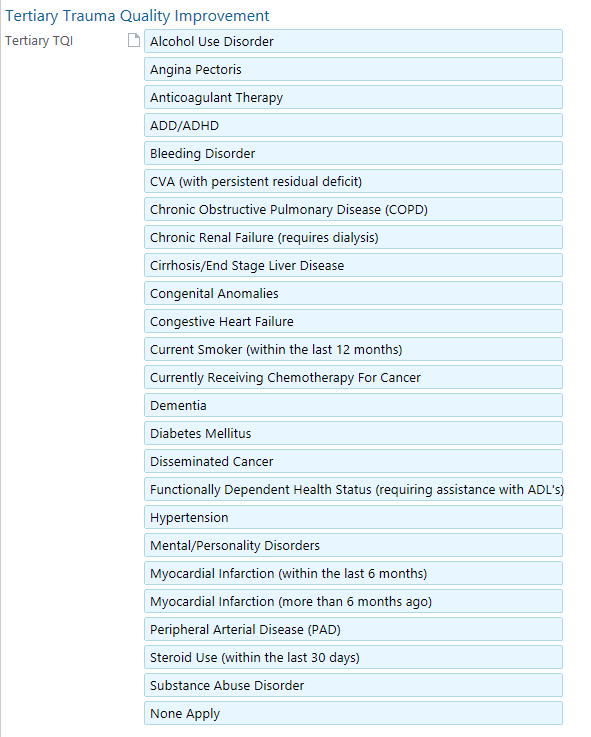
Use the tertiary note template. Include preexisting conditions by clicking on the Tertiary Trauma Quality Improvement button
New Patients/Consults
-
Respond quickly and professionally to ALL requests for patient evaluation
-
Physically go see the patient in their current location
-
Make sure they are added to the Trauma team list
-
NO “FYI” or curbside consults and no consults are turned down without attending approval
Requesting New Consults
-
Before calling a consult, make sure:
-
Faculty are aware
-
You have enough patient information to adequately answer consultant questions
-
Know what you are asking the consultant to do
-
Enter an order in the computer AND
-
Make verbal contact with MD or APP on consult team
-
No consults should be called without discussing with trauma faculty first
-
Neurosurgery and ortho have 30 minutes to see the patient
-
If IR is consulted for emergent hemorrhage control, they have 60 minutes from the time of consult to sticking the patient. If you have any issues communicating with IR, notify the trauma faculty immediately.
-
If the consulting resident is unable to provide a plan regarding severely injured patients in a timely fashion (i.e. whether a patient with a severe TBI will get an ICP monitor or craniectomy, timing for fixation of unstable spine), obtain contact information for the consulting attending, and the trauma faculty will call them.
Procedures
-
Notify faculty before performing any invasive procedure
-
After procedure, write a procedure note
-
READ your note and make it accurate
-
Assign note to attending who oversaw the procedure
-
Order and follow up on appropriate post-procedural testing (CXR after bronch or CVC placement). You should not go home after completing a procedure until you review post-procedural imaging.
-
Sterile technique is required for all invasive procedures (ie. arterial and CVC lines, chest tubes, suturing). Chest tubes and central lines should be done with full gown, gloves, mask, and drapes, if clinical condition allows.
Transferring Pts from one level of care to another
-
Call the receiving team to communicate comprehensive handoff information
-
CCS will enter floor orders on ICU patients leaving the ICU for the floor
-
Do not transfer patients to the ICU without discussing with attending
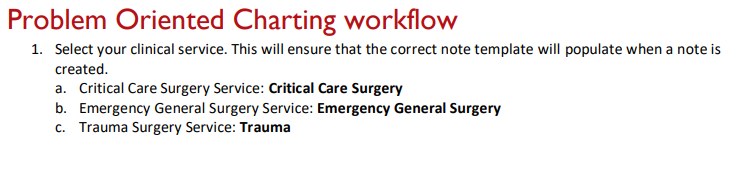
Documentation
Accurate and complete documentation is necessary to ensure proper communication between members of the care team. There are also certain documentation requirements that might not seem clinically relevant, but that are required to maintain trauma program accreditation. The trauma service uses problem-based documentation for H&Ps and progress notes.
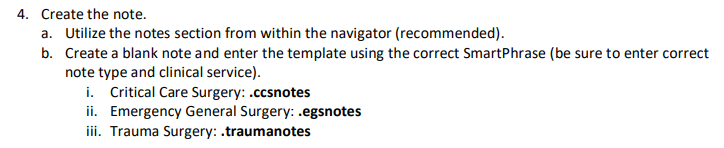
-
Do NOT use the "Generate Note" button!
-
Use the Rounding tab and click on Progress Notes, or
-
Use the Admission tab and click H&P Notes, or
-
Use the Discharge tab and click Discharge Summary.
Update the problem list every day and every night, and whenever a new problem is identified.
Handoff Tool
Surg Trauma Check-In: This box of the handoff tool is intended to be used by the overnight APP/resident to communicate with the day team. Any events that occurred overnight or tests that require follow up should be documented in this box. Every order or page needs to be entered in this box. You should also document your decision making process. Include the date of the entry, so that old events can be deleted by the day team.
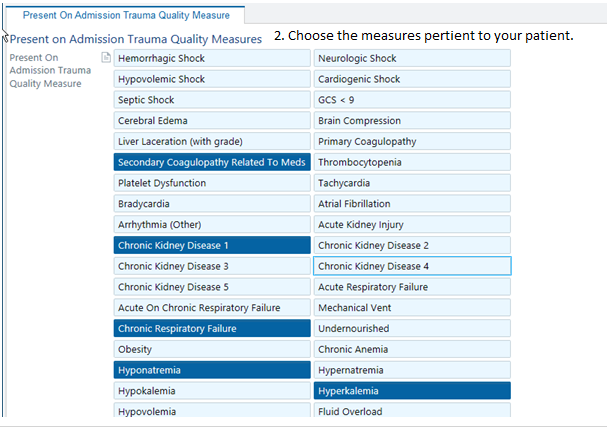
Present on Admission Trauma Quality Measure
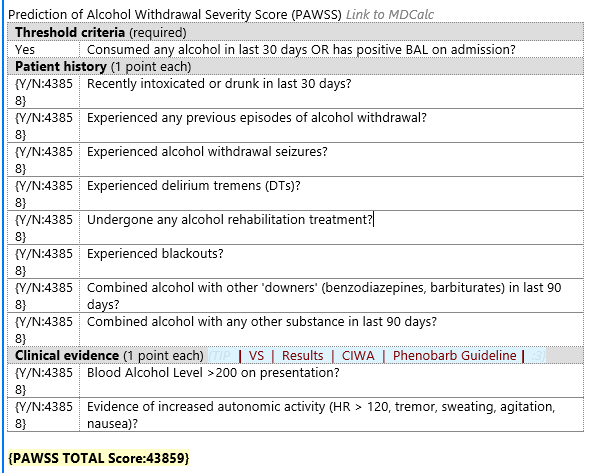
PAWS: Alcohol withdrawal is potentially lethal, but is preventable. Accurately assessing whether a patient is at risk for withdrawal is essential. A PAWS Score must be documented on every trauma patient. If unable to be obtained at the time of admission, it should be documented in tertiary note.
Tertiary Exam
Note type “Trauma Tertiary Survey”
“Tertiary Trauma Quality Improvement” hyperlink located within note or box at the top

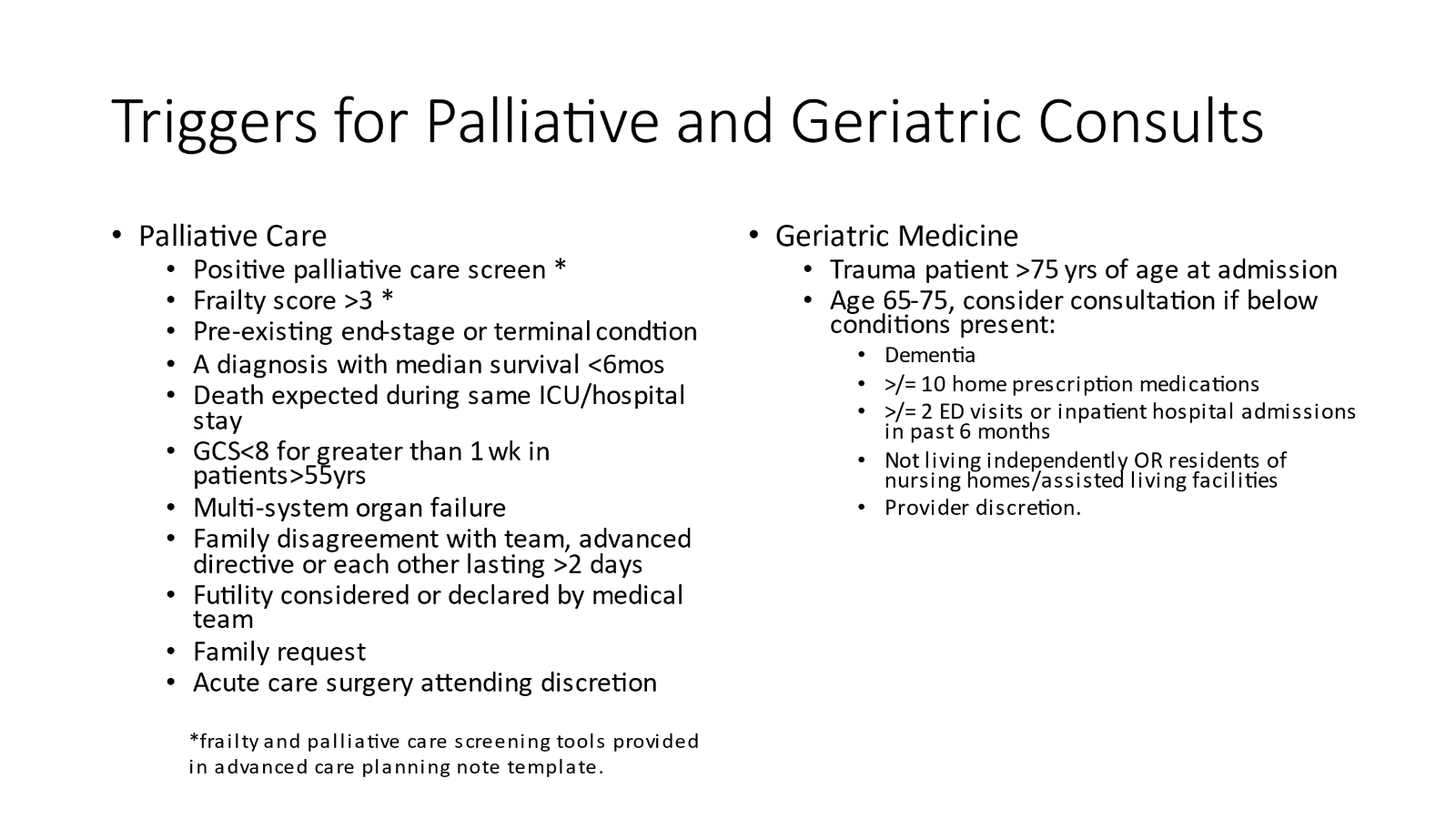
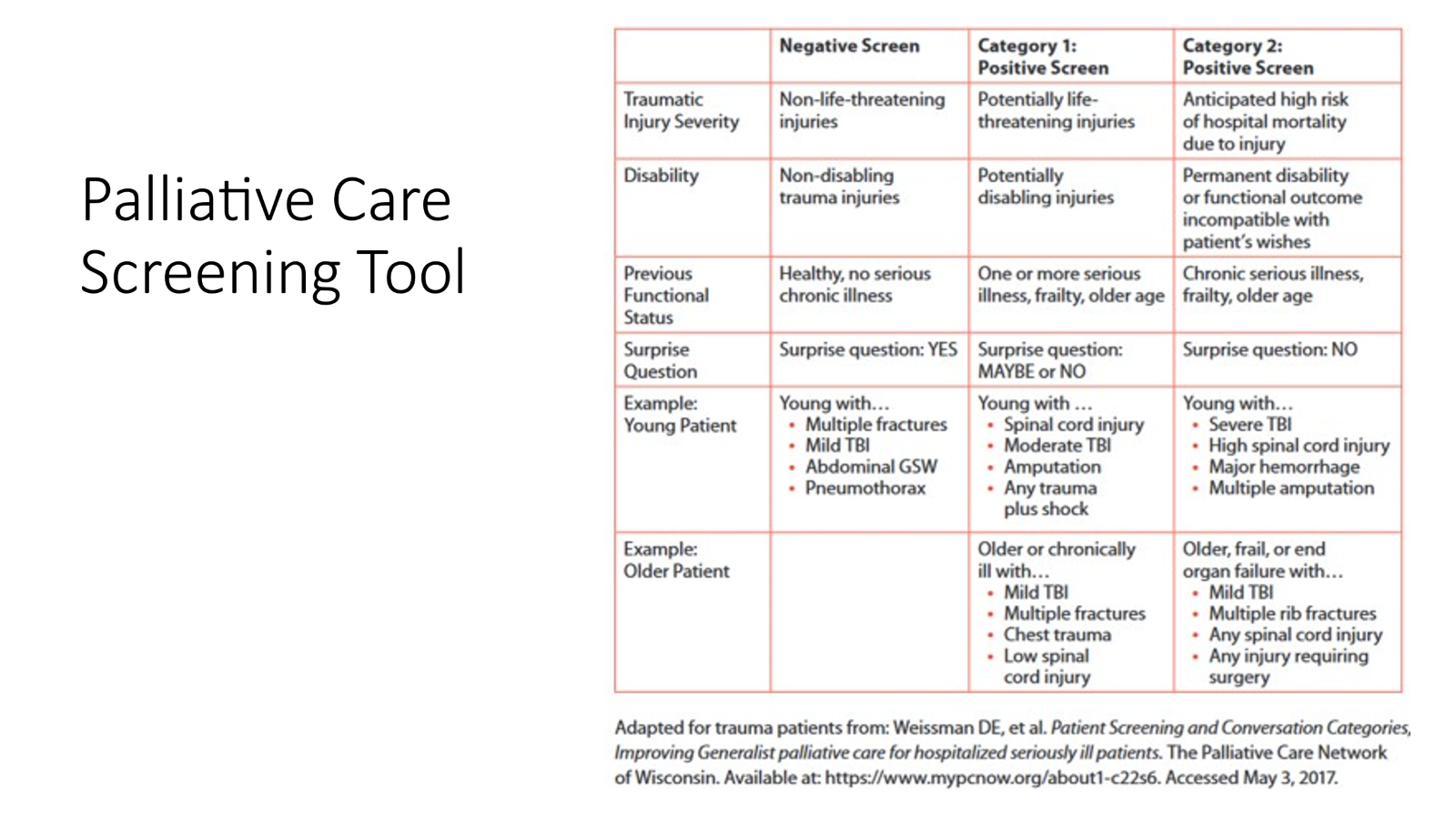
Advanced Care Planning
-
Within first 24 hrs of admission (ideally, at time of trauma tertiary), complete an advanced care planning discussion and assessment with every patient.
-
The ACP discussion should be documented in EPIC under the note type “advanced care planning” using the dotphrase .ACSACPINITIALDISCUSSION
-
All Category II patients require a family meeting within 72 hrs of admission. This follow-up ACP discussion should be documented in EPIC using the note type “advanced care planning” using the dotphrase “.ACSACPFOLLOWUP”
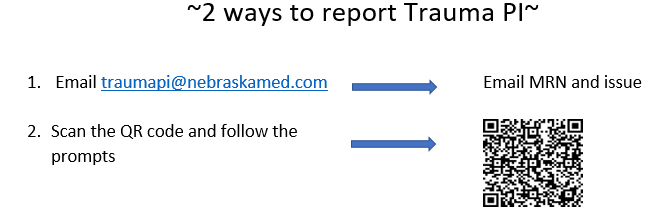
Trauma PI
The trauma team is mandated by American College of Surgeons to review all trauma morbidities and mortalities. In order to review, we need you to report that a morbidity or mortality has occurred.
Hospital Based Violence Intervention Program EncompassOmaha
Refer patients by emailing [email protected]
This program is available for any victim of violence (GSW, SW, assault, etc). It provides culturally competent case management, trauma psychology, and violence intervention resources to patients both in the hospital and in long-term follow up.
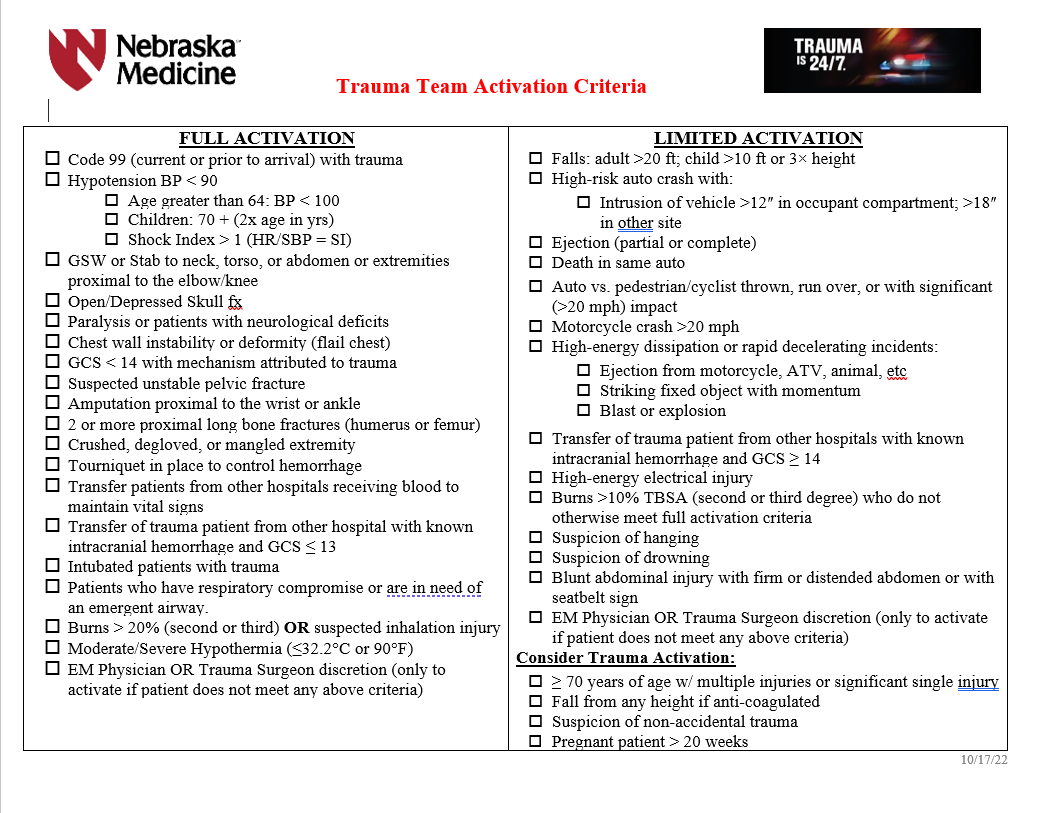
Initial Management and Resuscitation
Trauma Team Activation Criteria
Admission Criteria
ICU ADMISSION
-
Grade IV or greater solid organ injury or Grade III injury with blush/active extravasation
-
Any hemodynamic instability
-
Base deficit >6
-
Pelvic fractures requiring blood transfusion or IR angiogram/embolization
-
Any spine fracture with neurologic deficit
-
Mandible fracture with edema or hematoma
-
Traumatic brain injury with GCS<13
-
Patient >55 yrs of age, on anticoagulation with abnormal CT head
-
Risk of airway compromise
-
High risk rib fracture patient with FRC<1000mL
-
Presence of pulmonary co-morbidities
-
Blunt myocardial injury with new
-
arrythmia
-
hemodynamic instability
-
cardiac failure
-
Unstable spine injury
-
Frontal contusions >2cm
-
Solid organ/pelvis/abdominal injuries with evidence of active extravasation on CT scan
-
Need for q1hr vital signs/neuro-vascular checks/interventions/etc.
-
Trauma attending discretion
SDCC Admission
-
Grade II/III solid organ injury without blush/active extravasation on CT
-
presence of multiple injuries
-
Rib fractures with FRC between 1000mL—1500mL
-
Any patient on pre-injury anticoagulation therapy with an injury not requiring ICU
-
Major soft tissue trauma in patients on anticoagulation therapy
-
Need for q2hr vital signs/neuro-vascular checks/interventions/etc.
-
Presence of multiple co-morbidities
-
Age > 70
-
C-spine fractures exclusive of spinous and transverse process fractures (without neurologic injury)
-
History of sleep apnea who needs narcotics
-
New CPAP/BiPAP requirements
-
Trauma attending discretion
FLOOR Admission
-
All other trauma patients who do not meet criteria for ICU or SDCC admission
Isolated hip fractures requiring total or partial joint replacement may be transferred to Bellevue Medical Center by Orthopedics after full trauma evaluation---Refer to Isolated Orthopedic Transfers to Bellevue Medical Center Requiring Joint Replacement pathway on trauma website
Some isolated pediatric fractures may be transferred to Children’s Nebraska by Orthopedics after full trauma evaluation---this needs to be verbally approved by Dr. Bauman or Dr. Evans before transfer is initiated. Talk to Red attending.
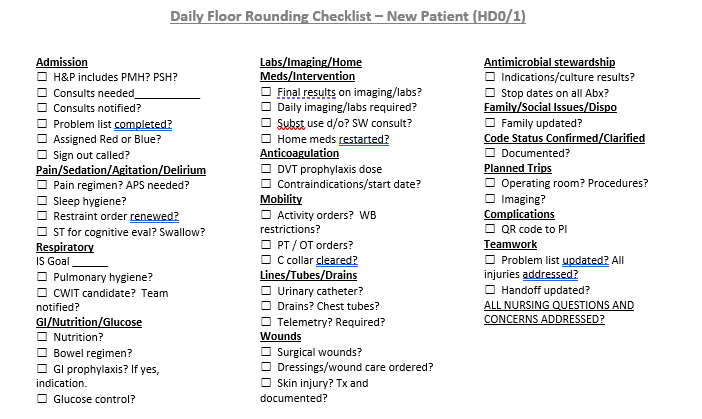
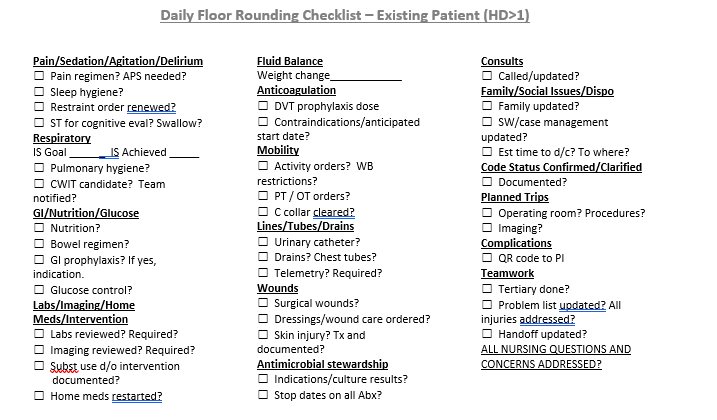
Daily Floor Rounding Checklist for Trauma Patients
Neurological Trauma
All blunt trauma patients should be placed in c-spine precautions until the cervical spine can be appropriately evaluated and cleared---Refer to Cervical Spine Evaluation and Management on trauma website for C spine precautions, evaluation and clearance
-