-
The Blue attending is the backup attending during the day, and the ICU attending is the backup at night. If a patient has a change in status (new tachycardia, arrhythmia, hypotension, hypoxia, altered mental status, hemorrhage, sepsis, etc), and the rest of the team is in the operating room, it is your responsibility to alert the backup attending immediately.
Red APP:
An APP is assigned to the Red service Monday-Friday. The primary role of the APP is to support the team, and not to serve as a primary rounder. The APP should:
The APP is responsible for rounding on patients when the Red census exceeds a 1:10 provider-to-patient ratio.
On the weekends, there is no Red APP, but the Blue APPs are expected to attend and assist with activations.
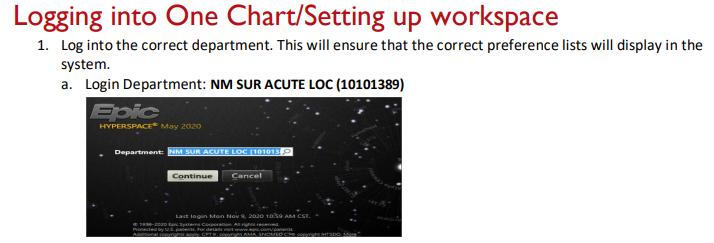
Workspace
The trauma APPs have workspace on MSB 4th fl. We also encourage regular use of the 9th floor trauma work room, so that you are immediately available to a large number of our patients.
Departmental Education
Tues: 7:30 am Acute Care Surgery education conference in the Chairman’s conference room MSB 45119
**This is mandatory for all residents on trauma and EGS. If there is an operative case, one resident can leave conference once the patient is being prepped. The attending is expected to get patients back to the OR without resident support for first start cases on Tuesday mornings.
Residents are required to attend their department’s regularly scheduled education conferences.
Wed: 7a-12noon General Surgery
Thurs: 8a-1p ER
Hand offs
6 am: Sign out from night resident and/or APP in 9th floor trauma room
6:00-8:30am: Preround on assigned patients. Ensure that your name is listed in the Epic column “Surg Pt Status” for the patients you are rounding on.
8:30am: Round with attending. This can be adjusted depending on OR schedule, activations, or at attending discretion. If there are significant changes in patient status, do not wait for rounds to tell your chief/senior/attending.
6 pm: Face-to-face handoff from day to night team in MSB 45119
Bedside Multidisciplinary Rounds
After sign out, begin pre-rounding
-
-See your patients in advance
-
-Know vital signs (Tmax, T current, HR, RR, BP, O2 saturation and oxygen needs)
-
-Know ins and outs (total ins/outs for 24 hour period, urine/ostomy/drain/tube outputs broken down by 12 hour shifts)
-
-Know today’s labs and imaging results
-
-Know up-to-date plans from consultants
-
-Know PT/OT recommendations for discharge (home vs SNF vs rehab)
-
-Examine every wound every day before attending rounds, unless specifically directed otherwise
Text or page Pharmacy just before start of rounds
Patient’s bedside RN should be involved in the patient’s discussion and engaged in rounds
Resident or APP must be logged into a computer at all times:
Daily Flow
Following bedside multidisciplinary rounds……….
If surgery residents are in the OR, APP and non-surgical residents are expected to carry the pager, continue responding to activations, and advance care for all patients on the entire service (even patients who were seen in the morning by an operating resident). Each resident is expected to know the general plan for every patient on service to ensure that all patients receive high-quality care at all times.
4:00 PM - Afternoon rounds with APPs and residents
Night Flow
Trauma Activations
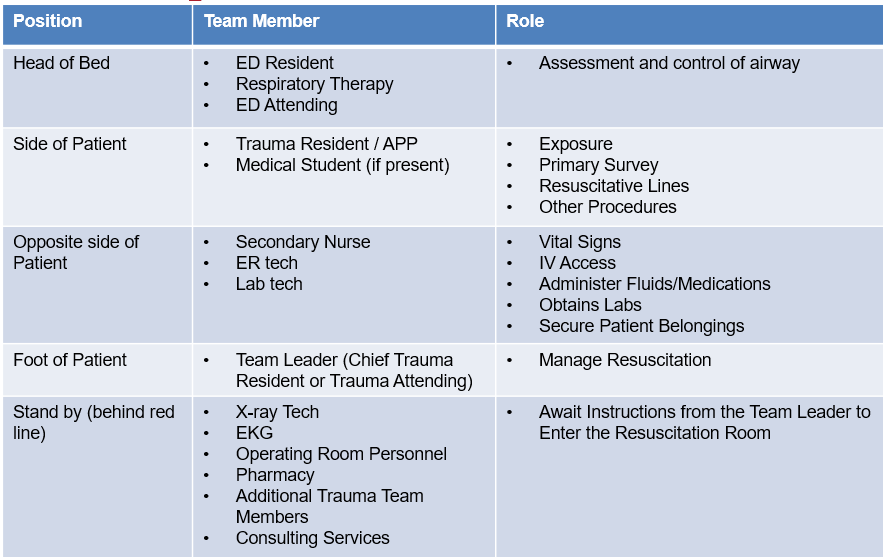
Trauma Roles and Responsibilities during Trauma Activation
-
Prior to patient arrival: Participate in the PreBrief (see poster on wall), introduce yourself and your position, preassign roles, ensure equipment is ready and available
H&P and Progress Notes
Tertiary Exams
New Patients/Consults
Requesting New Consults
-
If IR is consulted for emergent hemorrhage control, they have 60 minutes from the time of consult to sticking the patient. If you have any issues communicating with IR, notify the trauma faculty immediately.
-
If the consulting resident is unable to provide a plan regarding severely injured patients in a timely fashion (i.e. whether a patient with a severe TBI will get an ICP monitor or craniectomy, timing for fixation of unstable spine), obtain contact information for the consulting attending, and the trauma faculty will call them.
Procedures
-
Sterile technique is required for all invasive procedures (ie. arterial and CVC lines, chest tubes, suturing). Chest tubes and central lines should be done with full gown, gloves, mask, and drapes, if clinical condition allows.
Transferring Pts from one level of care to another
Documentation
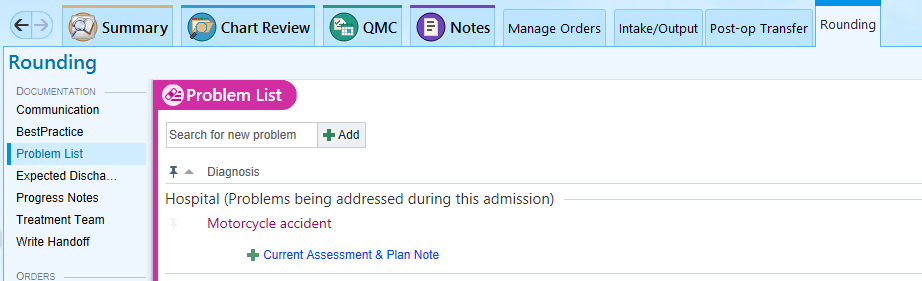
Accurate and complete documentation is necessary to ensure proper communication between members of the care team. There are also certain documentation requirements that might not seem clinically relevant, but that are required to maintain trauma program accreditation. The trauma service uses problem-based documentation for H&Ps and progress notes.
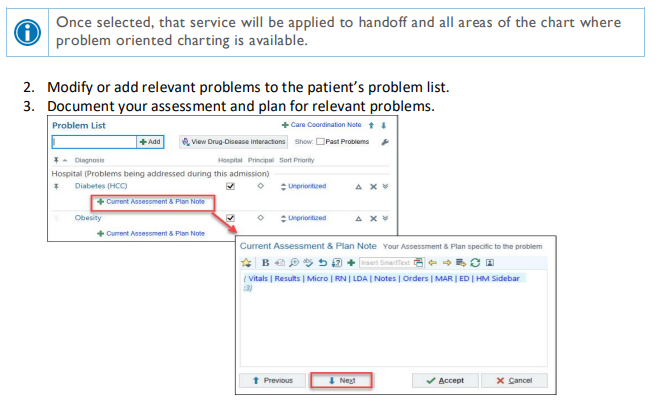
Update the problem list every day and every night, and whenever a new problem is identified.
Handoff Tool
Surg Trauma Check-In: This box of the handoff tool is intended to be used by the overnight APP/resident to communicate with the day team. Any events that occurred overnight or tests that require follow up should be documented in this box. Every order or page needs to be entered in this box. You should also document your decision making process. Include the date of the entry, so that old events can be deleted by the day team.
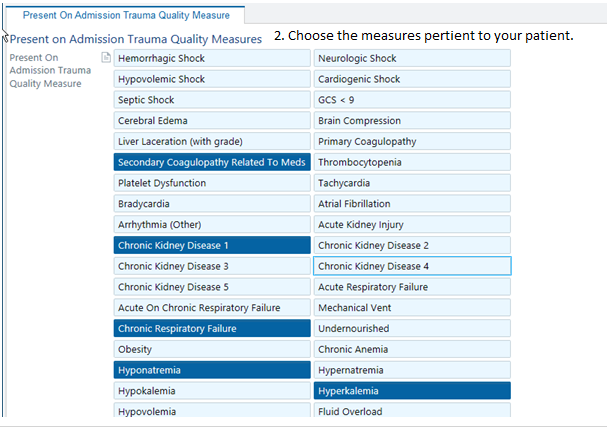
Present on Admission Trauma Quality Measure 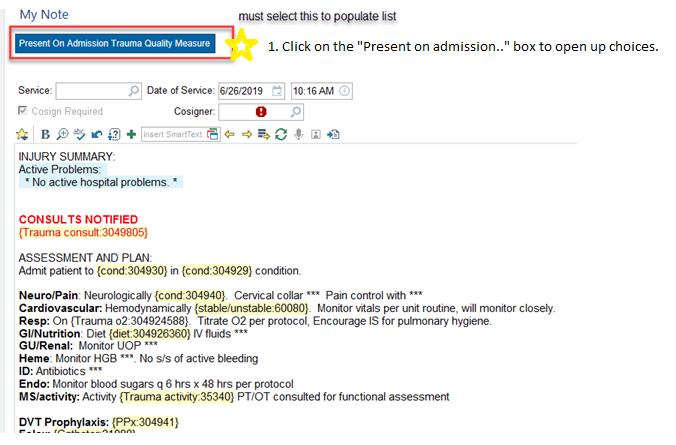
PAWS: Alcohol withdrawal is potentially lethal, but is preventable. Accurately assessing whether a patient is at risk for withdrawal is essential. A PAWS Score must be documented on every trauma patient. If unable to be obtained at the time of admission, it should be documented in tertiary note. 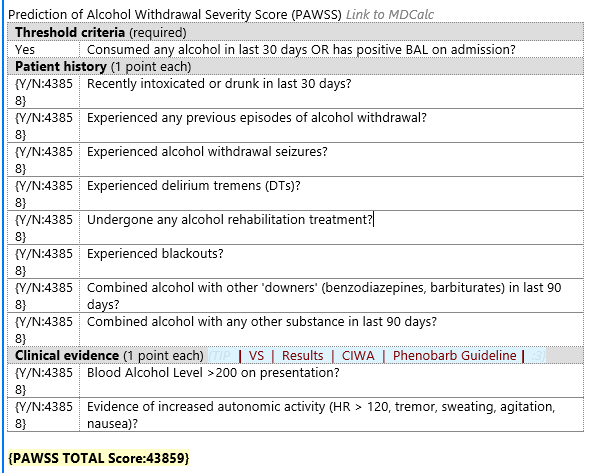
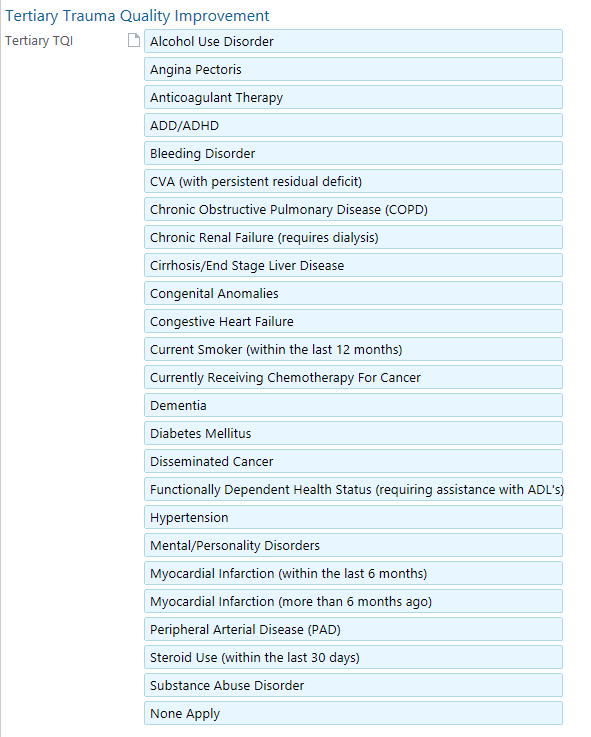
Tertiary Exam
Note type “Trauma Tertiary Survey”
“Tertiary Trauma Quality Improvement” hyperlink located within note or box at the top 
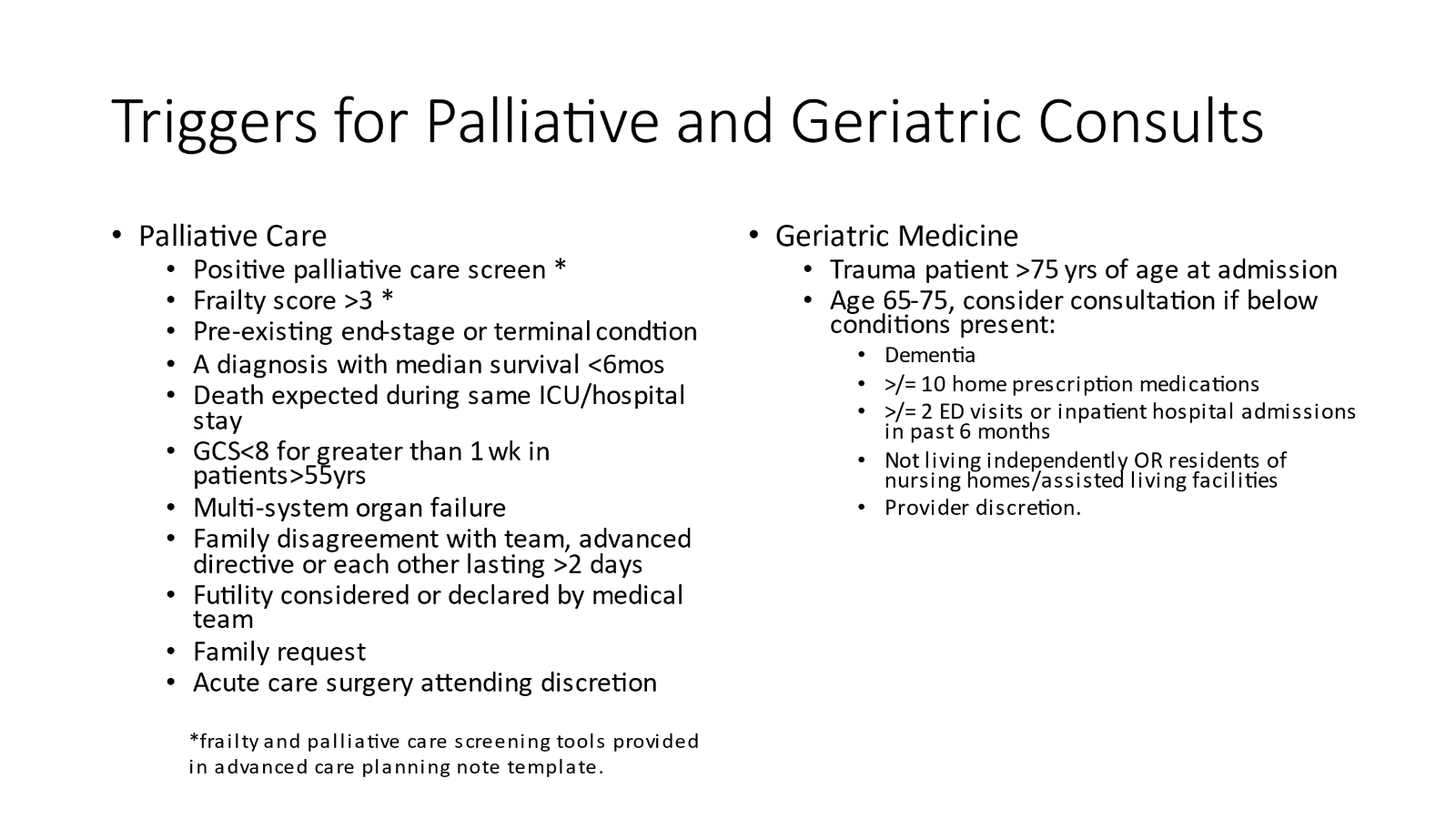
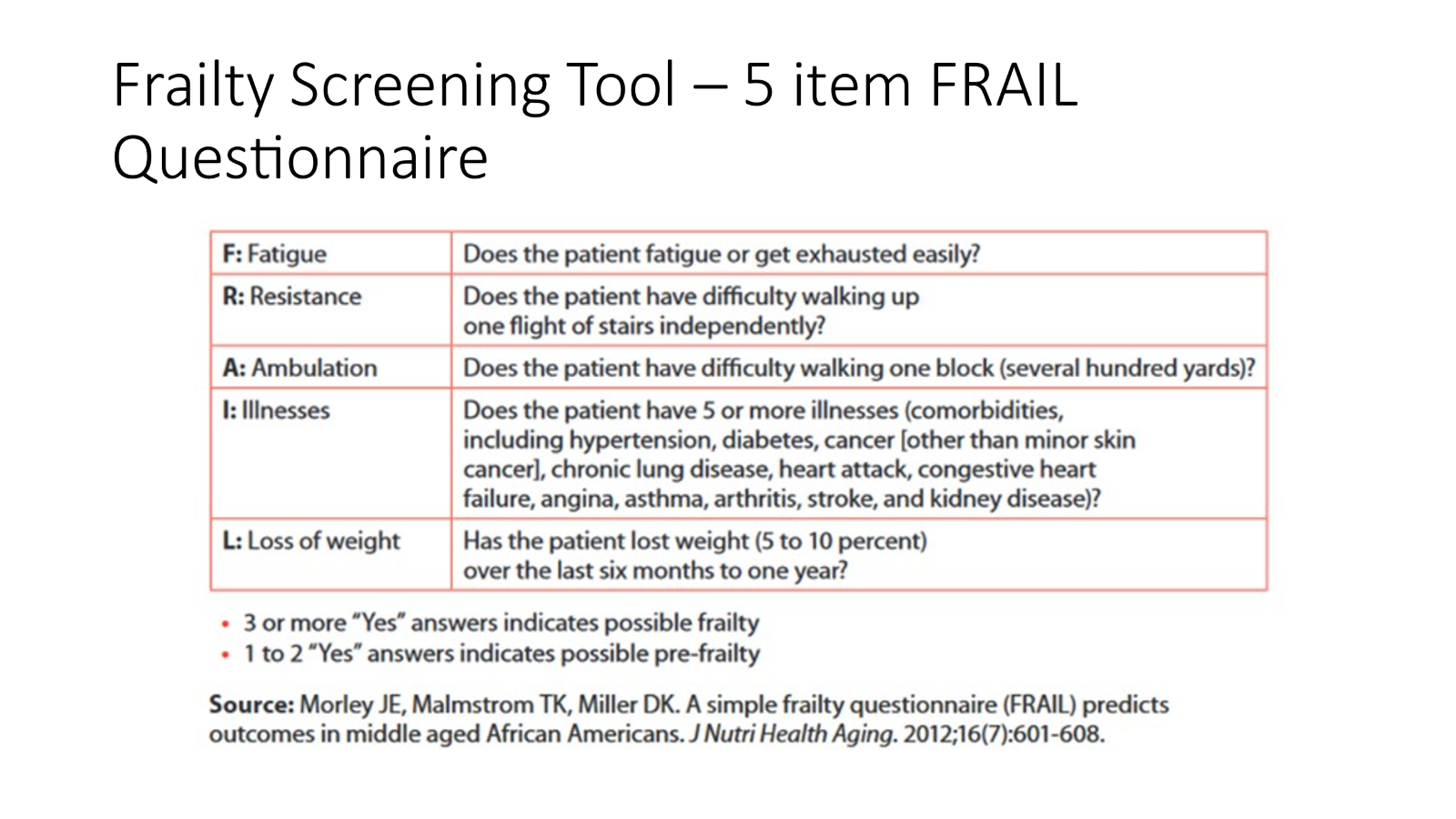
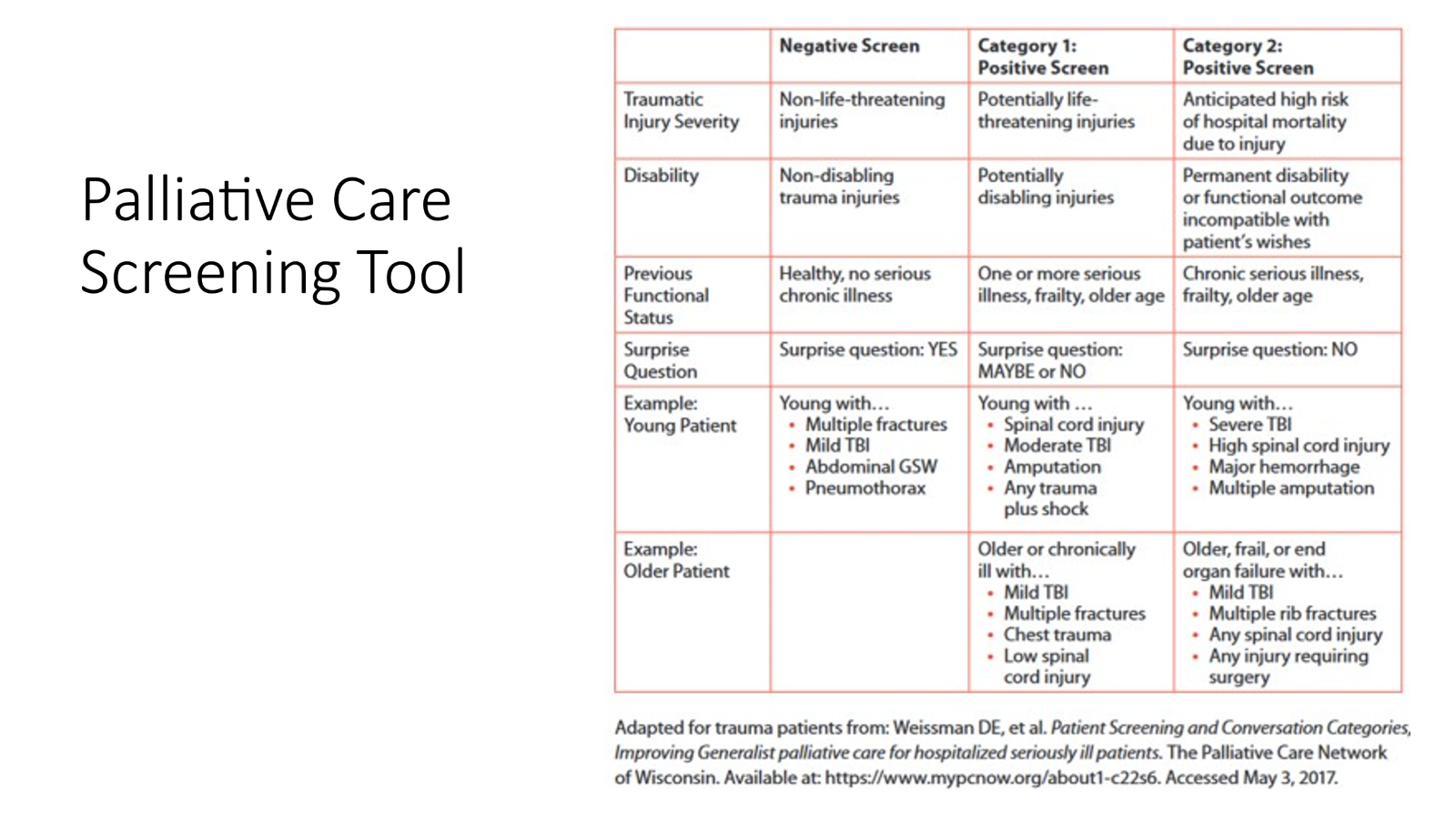
Advanced Care Planning
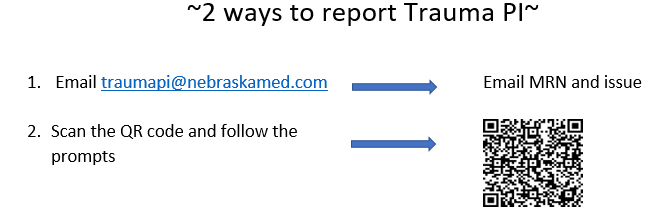
Trauma PI
The trauma team is mandated by American College of Surgeons to review all trauma morbidities and mortalities. In order to review, we need you to report that a morbidity or mortality has occurred.
Hospital Based Violence Intervention Program EncompassOmaha
Refer patients by emailing [email protected]
This program is available for any victim of violence (GSW, SW, assault, etc). It provides culturally competent case management, trauma psychology, and violence intervention resources to patients both in the hospital and in long-term follow up.
Initial Management and Resuscitation
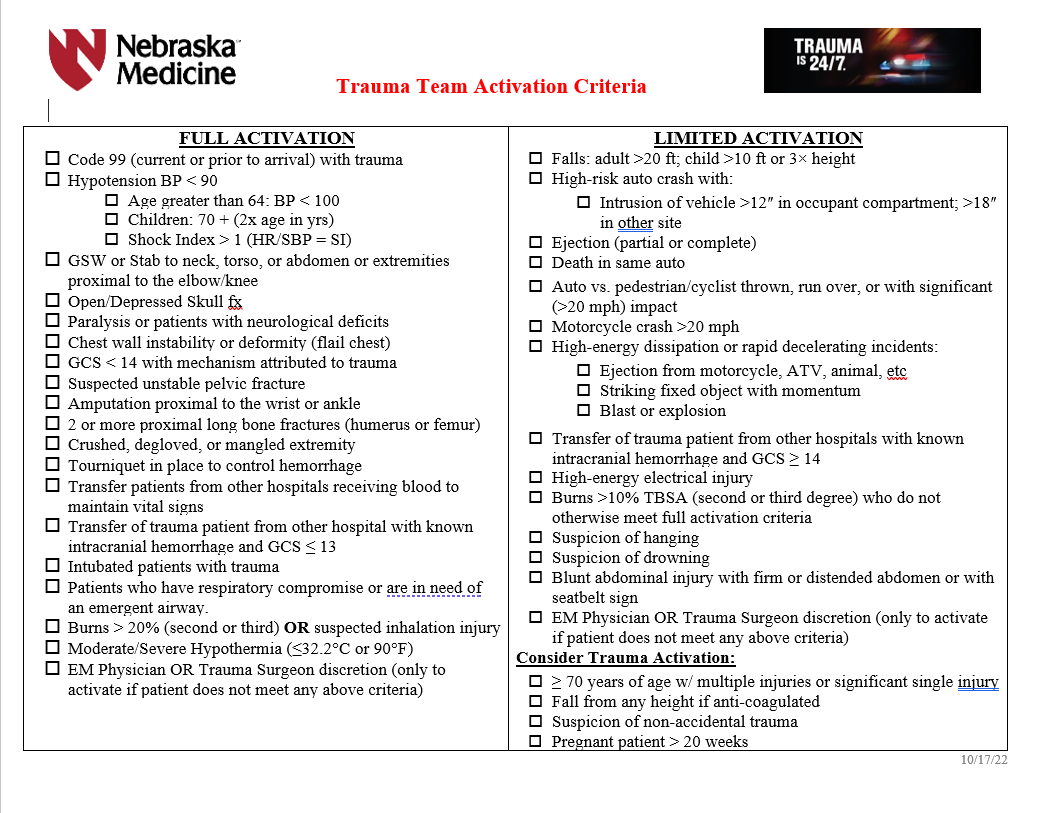
Trauma Team Activation Criteria
Admission Criteria
ICU ADMISSION
SDCC Admission
FLOOR Admission
Isolated hip fractures requiring total or partial joint replacement may be transferred to Bellevue Medical Center by Orthopedics after full trauma evaluation---Refer to Isolated Orthopedic Transfers to Bellevue Medical Center Requiring Joint Replacement pathway on trauma website
Some isolated pediatric fractures may be transferred to Children’s Nebraska by Orthopedics after full trauma evaluation---this needs to be verbally approved by Dr. Bauman or Dr. Evans before transfer is initiated. Talk to Red attending.
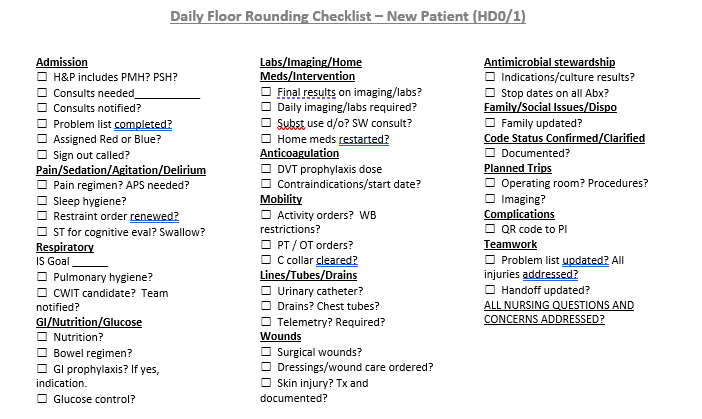
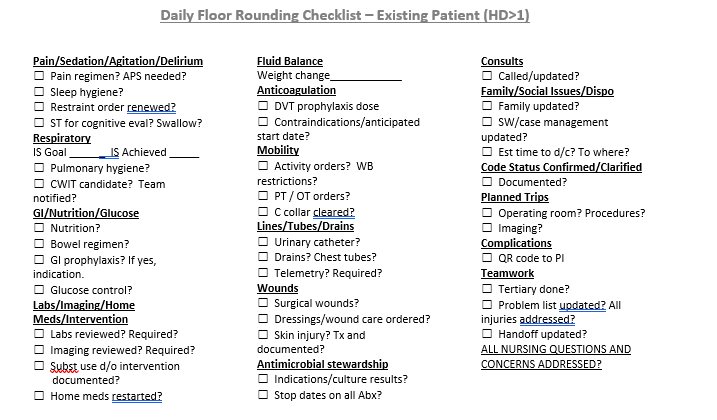
Daily Floor Rounding Checklist for Trauma Patients
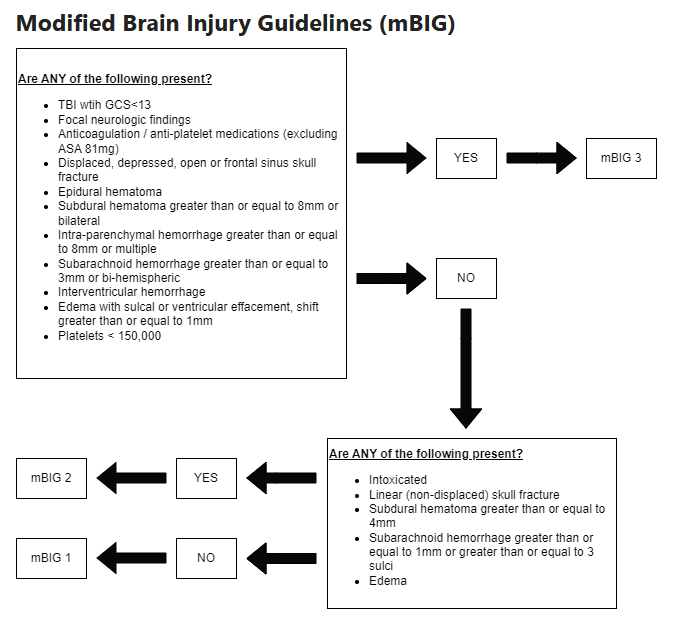
Neurological Trauma
All blunt trauma patients should be placed in c-spine precautions until the cervical spine can be appropriately evaluated and cleared---Refer to Cervical Spine Evaluation and Management on trauma website for C spine precautions, evaluation and clearance