Documentation
Documentation
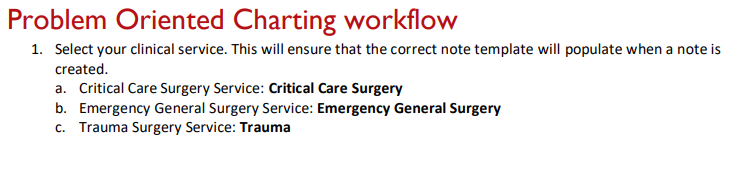
Accurate and complete documentation is necessary to ensure proper communication between members of the care team. There are also certain documentation requirements that might not seem clinically relevant, but that are required to maintain trauma program accreditation. The trauma service uses problem-based documentation for H&Ps and progress notes.
-
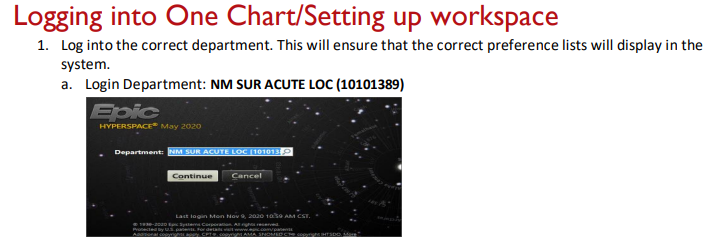
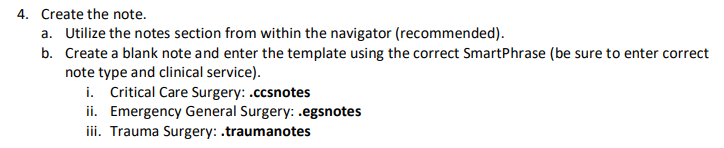
Do NOT use the "Generate Note" button!
-
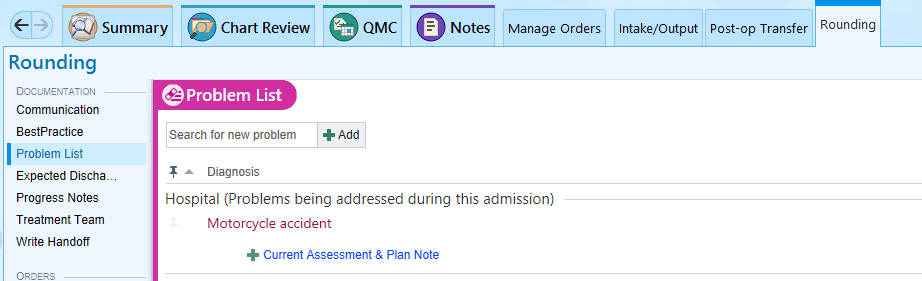
Use the Rounding tab and click on Progress Notes, or
-
Use the Admission tab and click H&P Notes, or
-
Use the Discharge tab and click Discharge Summary.
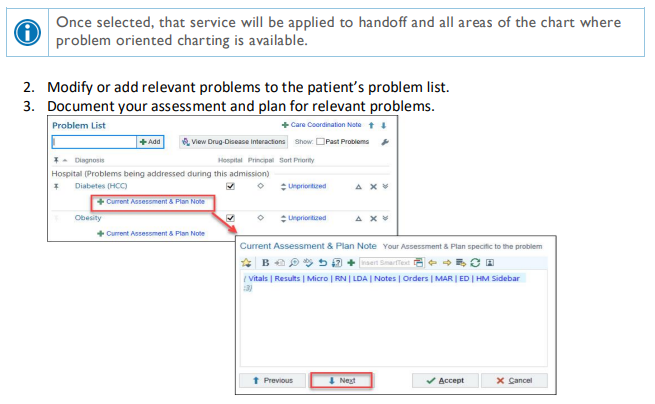
Update the problem list every day and every night, and whenever a new problem is identified.
Handoff Tool
Surg Trauma Check-In: This box of the handoff tool is intended to be used by the overnight APP/resident to communicate with the day team. Any events that occurred overnight or tests that require follow up should be documented in this box. Every order or page needs to be entered in this box. You should also document your decision making process. Include the date of the entry, so that old events can be deleted by the day team.
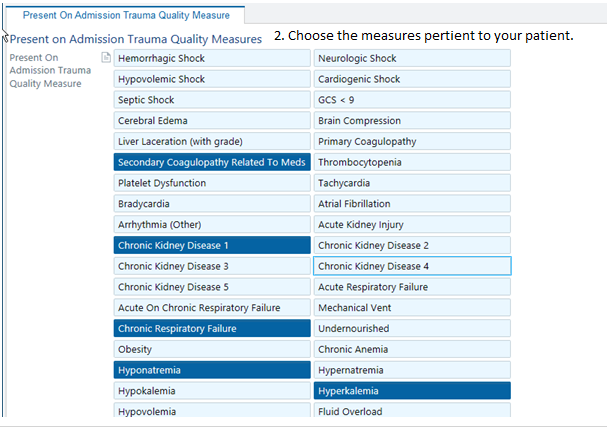
Present on Admission Trauma Quality Measure 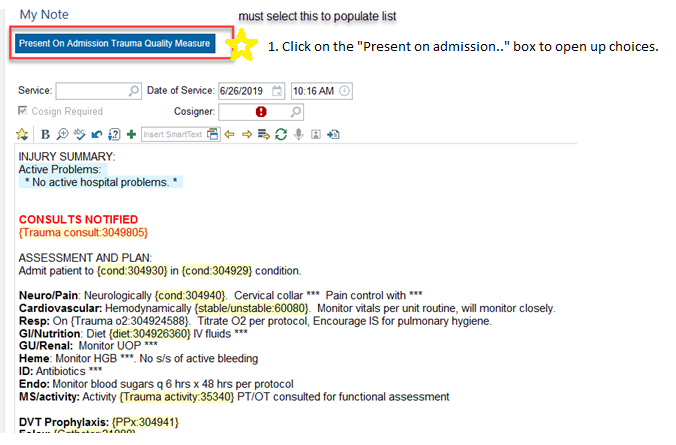
PAWS: Alcohol withdrawal is potentially lethal, but is preventable. Accurately assessing whether a patient is at risk for withdrawal is essential. A PAWS Score must be documented on every trauma patient. If unable to be obtained at the time of admission, it should be documented in tertiary note. 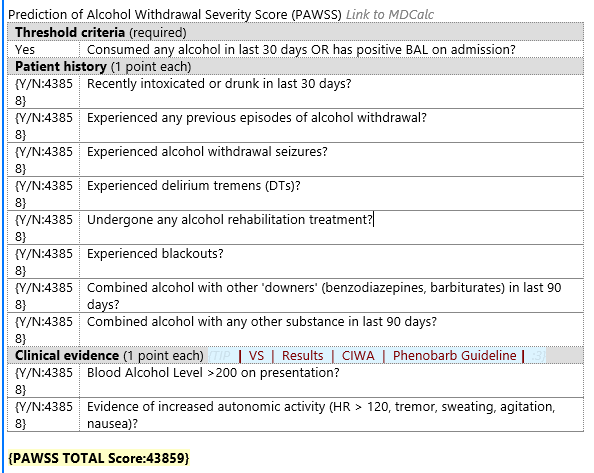
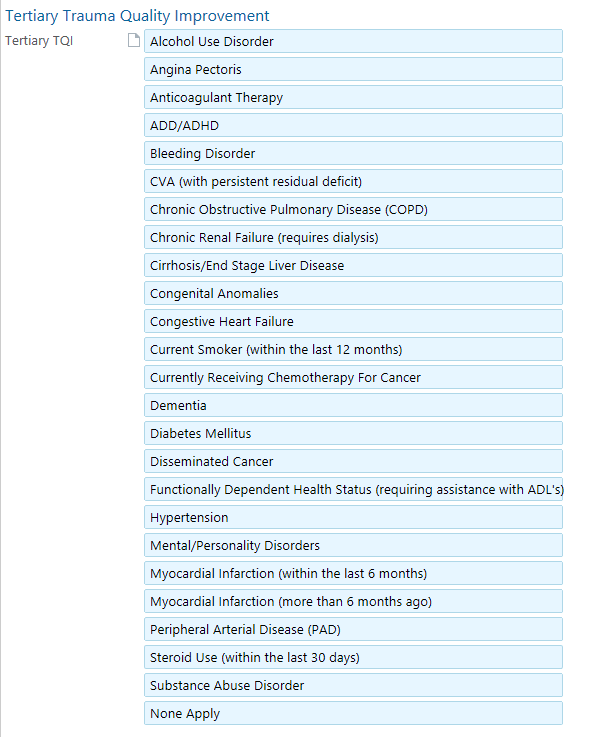
Tertiary Exam
Note type “Trauma Tertiary Survey”
“Tertiary Trauma Quality Improvement” hyperlink located within note or box at the top 
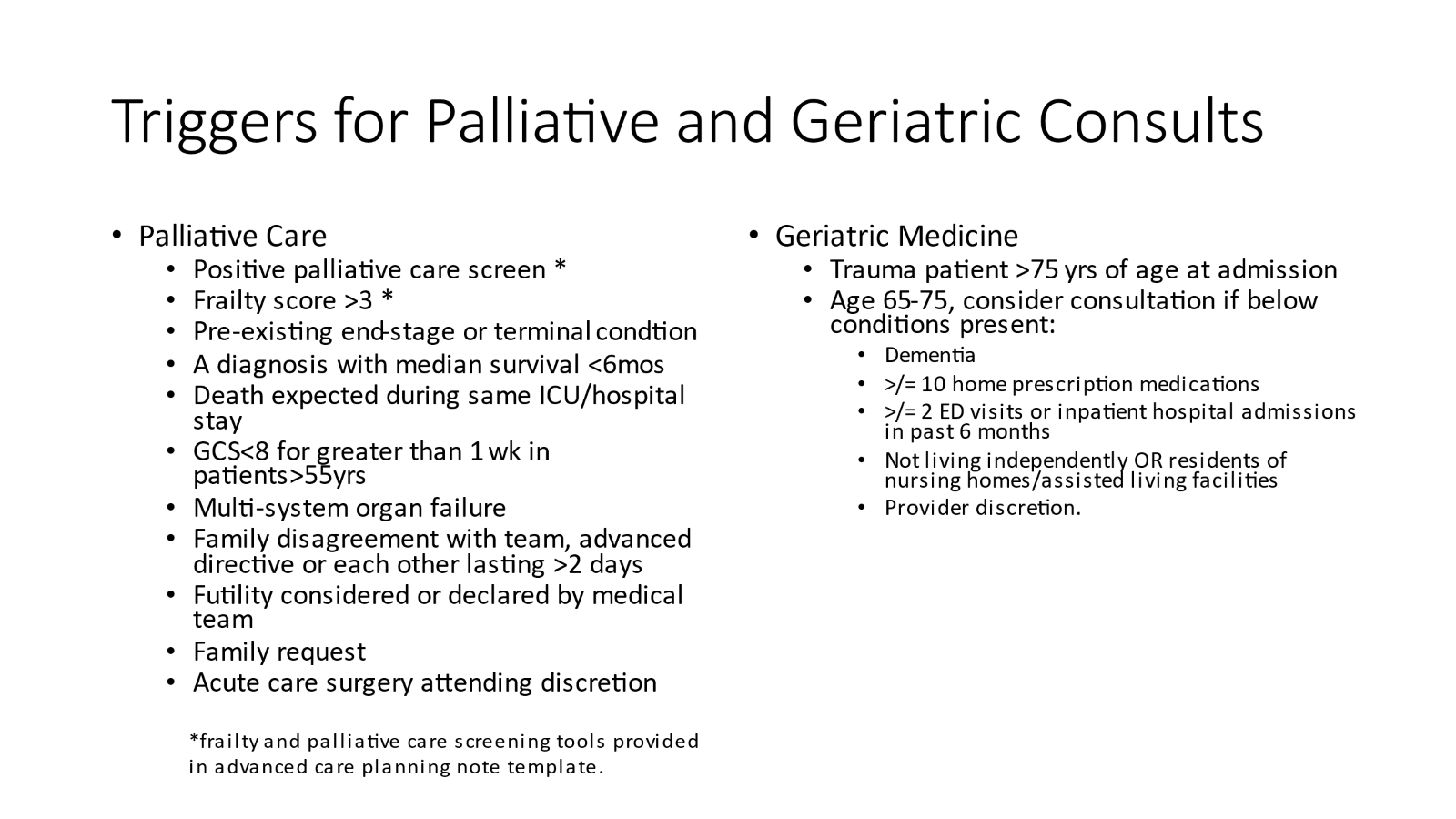
Advanced Care Planning
-
Within first 24 hrs of admission (ideally, at time of trauma tertiary), complete an advanced care planning discussion and assessment with every patient.
-
The ACP discussion should be documented in EPIC under the note type “advanced care planning” using the dotphrase .ACSACPINITIALDISCUSSION
-
All Category II patients require a family meeting within 72 hrs of admission. This follow-up ACP discussion should be documented in EPIC using the note type “advanced care planning” using the dotphrase “.ACSACPFOLLOWUP”