Airway Pressure Release Ventilation (APRV, Bivent)
Tips:Authors: Buesing, Bauman, Berning
Use Peak Airway Pressure in Pressure Modes and Plateau Pressures in Volume Modes of Ventilation to determine initial P1 setting.
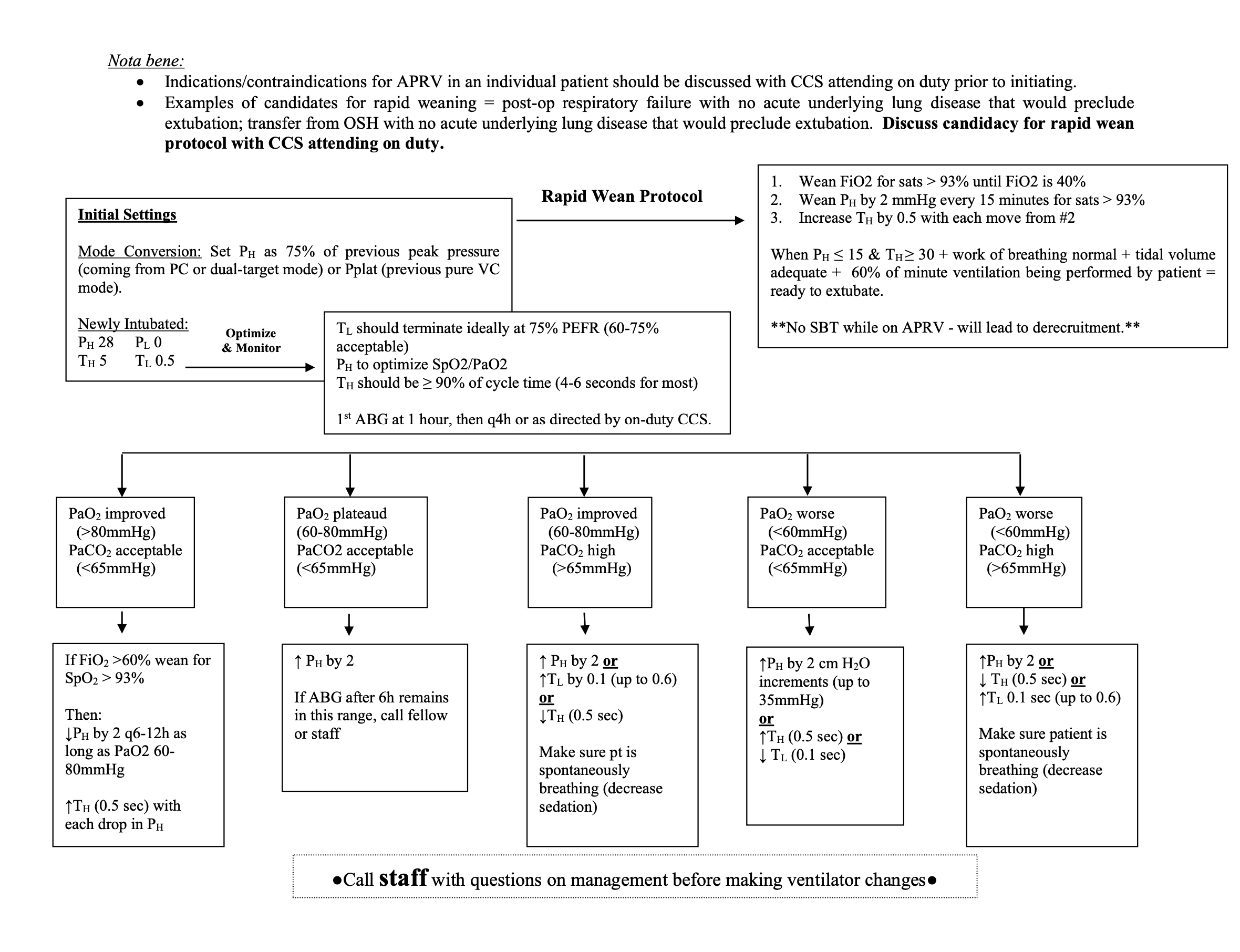
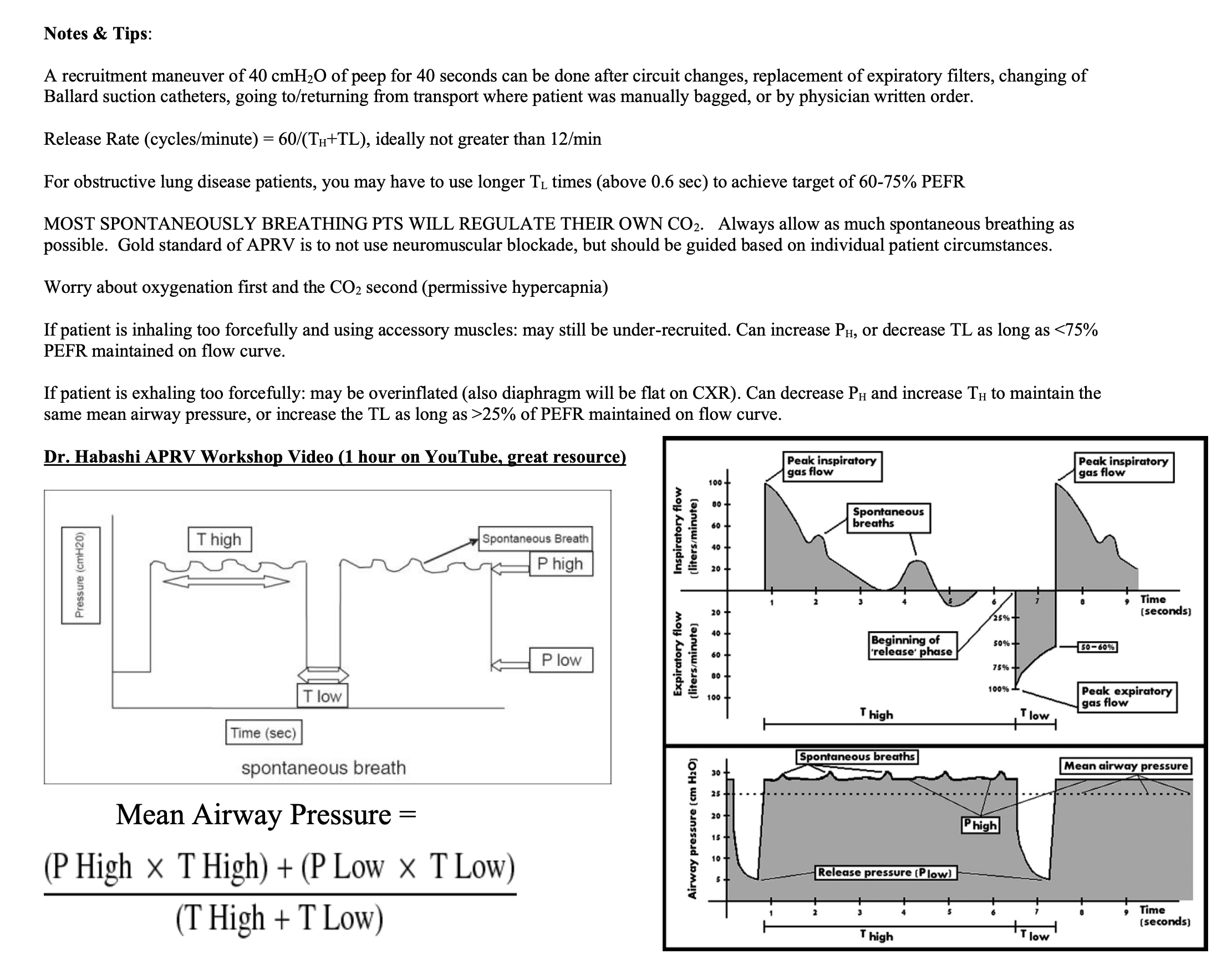
A recruitment maneuver of 40 cmH2O of peep for 40 seconds can be done after circuit changes, replacement of expiratory filters, changing of Ballard suction catheters, going to/returning from transport where patient was manually bagged, or by physician written order.
Initiate weaning for conventional management if:
Physiologic parameters are acceptable
Spo2 >92%, fio2 60%
EtCO2 <58 mmHg
ABG = pH >7.30, PaCO2 <50 mmHg, Pao2 >60 mmHg
Resolving disease / trauma process
“Drop and Stretch” method of weaning: reduce level of P high and increase T high until mode is converted to CPAP as a method of SBT before extubation. Dropping and stretching too quickly leads to derecruitment of alveoli.
Notes:
-T1 and T2 will need to be adjusted clinically.
-Release Rate(cycles/minute)=60/(T1+T2). This rate should not be>12
-Results are not instantaneous. The PaO2 will continue to improve as more alveoli are recruited. (PaO2 of 60mmHg is low end)
-For obstructive lung disease patients, use longer T2 times
-T2 should be titrated to allow between 50% and 75% of the volume out of the lung (look at the flow waveform)
-Patients will have retained lung volume, (This is not true auto-PEEP and is a desired effect of APRV)
-LONGER T1 AND SHORTER T2 = MORE RECRUITMENT/OXYGENATION AND LESS CO2 CLEARANCE
-SHORTER T1 AND LONGER T2 = LESS RECRUITMENT AND MORE CO2 CLEARANCE
-MOST SPONTANEOUSLY BREATHING PTS WILL REGULATE THEIR OWN CO2. Always allow as much spontaneous breathing as possible.
-Do not use neuromuscular blockade.
-Worry about oxygenation first and the CO2 second. (ph of 7.20, think permissive hypercapnia.)
-If patient is inhaling too forcefully and using accessory muscles: may still be under-recruited. Can increase P1, or decrease T2 as long as <75% PEFR maintained on flow curve.
-If patient is exhaling too forcefully: may be overinflated (also diaphragm will be flat on CXR). Can decrease P1 and increase T1 to maintain the same mean airway pressure, or increase the T2 as long as >25% of PEFR maintained on flow curve.