New Page
Objectives
• Describe the most current evidence-based medical practices pertaining to the treatment of critically ill patients in the SICU.
• Demonstrate knowledge and competency in resuscitation skills including advanced cardiopulmonary resuscitation, emergent airway management using bag and mask ventilation, and indications for intubation and mechanical ventilation.
• Demonstrate knowledge and competency in ventilator management including the use of PEEP, supplemental oxygen, lung protective ventilation strategies, pressure-cycled, volume-cycled and dual modes of ventilation
• Apply evidence-based guidelines to the care of patients with critical illness or injury such as ventilatory management for patients with ARDS, weaning from mechanical ventilation, hemodynamic monitoring, administration of nutritional support, renal failure, antibiotic administration, blood product transfusion and prevention of ICU related complications.
• Demonstrate knowledge and competency in the evaluation and non-operative management of severe closed head injury with or without intracranial hypertension.
• State the etiology, describe the pathophysiology, and demonstrate the appropriate management of patients with spinal cord injury
• Demonstrate proper performance of brain death certification and apply clinical criteria of brain death and basic principles of support for potential organ donors.
• Demonstrate competency in the performance of procedures, specifically central and arterial lines, and chest tubes and POCUS
• Demonstrate effective daily communication with consultants and other surgical services
• Demonstrate effective discussion of patient diagnosis, prognosis and management plan (including risks, benefits and side effects) with patient and family using simple, easily understood language
• Demonstrate the practice of ethical principals in relation to patient care and confidentiality, including obtaining informed consent, implementing “Do Not Resuscitate” orders, withholding or withdrawing life support, and clarifying goals of care from advanced directives
The Team
• Attending Intensivist (SCC, ACC)
• Advanced Practice Providers (Day and Night)
• Critical Care Fellows (Surgery, Medicine, Anesthesia, EM)
• Residents
• Medical Students
• SICU Nursing Manager
• Critical Care nurses
• Case managers and social workers
• Registered dietician
• Pharmacy
• Respiratory Therapy
• Physical, Occupational and Speech Therapy
Pagers and PerfectServe
888-0282 is the Green CCS (8th fl ICUs) pager
• Resident carries Green CCS pager during day and night
• New consults will route through the green pager - equitable distribution of consults between residents and APPs should occur
• 888-3005 is the Yellow CCS (non 8th fl ICUs) pager
• APP will carry Yellow CCS pager during day and night
• Both pagers are passed off during shift handoff.
• Utilization of PerfectServe is required.
Check to see that Perfect Serve is active on your phone!
SICU Workspace
• Constant physical presence in the SICU is required: Reduces pages, recognizes decline, promotes collaboration
• Workspace in the work room in hall on 8th floor (Across from family waiting room)
• CODE: 3005

CCS Day Flow
12-hour shift: 6AM to 6PM (You do not need to arrive before 6AM)
6AM – Night shift handoff in the Clarkson 8th fl ICU work room. Yellow and Green teams
6AM-8:30AM Preround on assigned patients, review labs and images, physical exam
Daily Rounds (8:30AM) – Multidisciplinary, Systems based rounding. Starting locations: Green – 8th floor SICU Yellow – Discretion of attending
Afternoons: Finish Notes, Bedside Procedures, Tertiary Exams, See new consults
6PM – Day shift handoff in the Clarkson 8th fl ICU work room. Yellow and Green teams.
CCS Day Attending shifts: 7AM – 4PM
Multidisciplinary Rounds
Rounding in the SICU begins @ 8:30 AM
- Multidisciplinary: Attending, Fellow, Residents, APP, Medical Students, Pharmacy, Dietitian, Nursing, PT/OT/ST.
- Systems based presentations
- One person responsible for placing orders in real time.
- If not presenting, stay engaged.
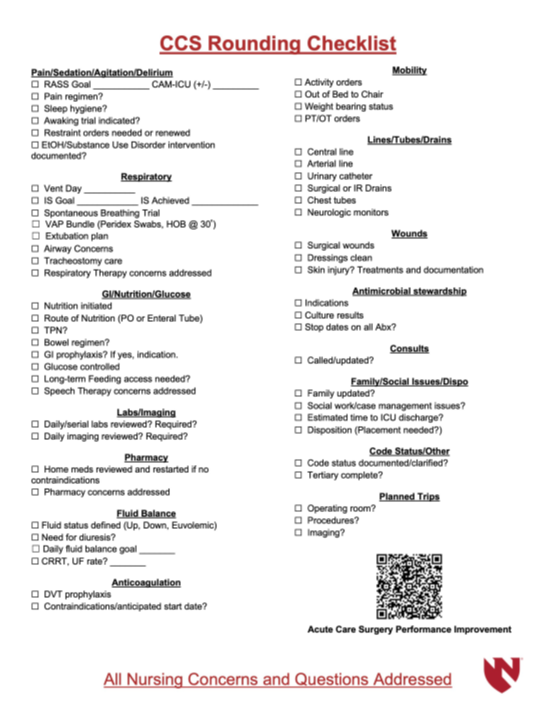
- CCS Rounding Checklist to be completed on every patient daily.
1:00 PM Case Management SICU RADAR Rounds
• Attending/Fellow must attend
• SICU Workroom
• Communicate with case managers and social work for potential discharges
and patient needs
Trauma Care Transition Nurses
• Terese Koubsky- care transitions 402-672-0274
• Molli Kies- care transitions 402-990-0874
1:30 pm Transplant rounds (except Weds, at 1:00 pm)
• One member of the SCC team must be present, and must have adequate
knowledge about every transplant patient
• Can be earlier or later, make friends with the transplant residents and
APPs
• Be engaged, provide additional patient information as needed
CCS is a consult service
- All patients on the CCS service require a consult note.
For important issues, text/call collaborators to discuss before orders are executed
– Examples: Activity, Diet, Transfusions - At least once per day…
CCS must touch base with services (Transplant, Trauma, EGS, MIS, Colorectal) for to discuss issues and plans related to our shared patients
New Patients
• Respond quickly and professionally to ALL requests for patient evaluation
• Physically see the patient in their current location
• Plan formulated as a collaborative effort between both the ICU and primary teams.
• Communicate with attending intensivist
• Call for help if needed early.
• Add to CCS list, place ICU admission orders, write consult note.
Requesting New Consults
• Before calling a consult, make sure:
• Faculty/Fellow is aware
• Is patient following a UNMC physician as an outpatient?
• You have enough patient information to adequately answer consultant questions
• Know what you are asking the consultant to do
• Enter an order in the computer AND
• Make verbal/PerfectServe contact with MD or APP on consult team
Daily Progress Notes
• All patients on the CCS service require a daily progress note.
• Patients with consult note after 12:00 am still require a daily progress note to communicate updated plans.
• Procedural notes, discharge summaries due at time of event
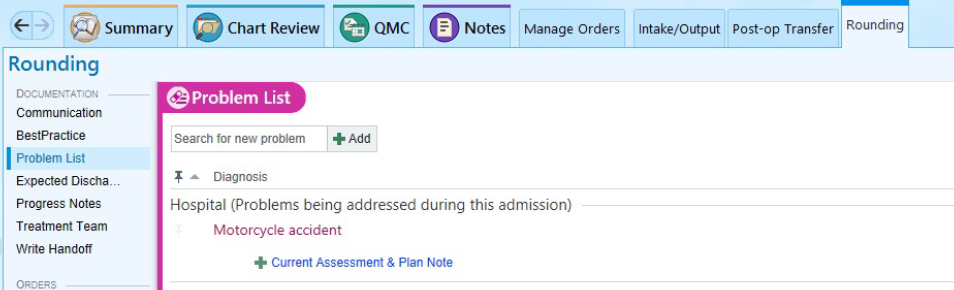
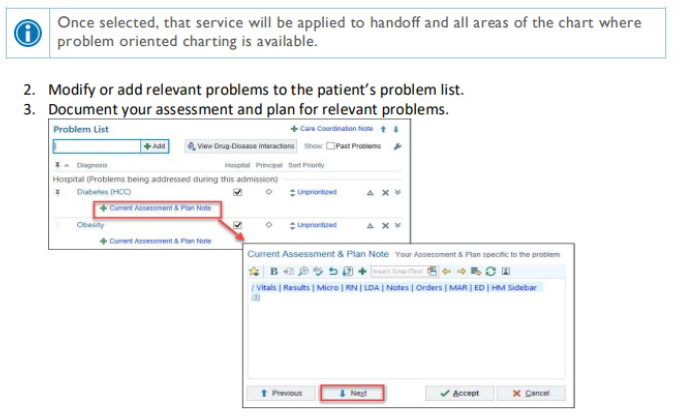
• Create daily progress note through rounding tab. Problem based charting.
• Update problem list frequently.

Daily Review of All Orders
• Review orders and remove unnecessary orders daily
• Do not use Nursing Communication or verbal order to
modify orders or hold medications
• Do not use Nursing Communication or verbal order to
change target RASS.
• Enter new target RASS in Ventilator
Management order set.
• Restraint Orders expire every 24 hours
• Address all expiring orders during rounds each
day (Re-order or D/C)
• When restraints are first ordered:
• Set “Hours” so order will expire around 7 AM
next day