Advanced Care Planning and Palliative Care Consultation in Trauma
Purpose
· To engage injured patient’s and/or families in discussions regarding goals of care and advanced care planning early and provide guidelines for Palliative Care consultation to assist in facilitating discussions surrounding goals of care and expectations of recovery following injury.
Background/Definitions
· Trauma is sudden, unpredictable and often life-altering. Patients and families display a variety of reactions after trauma and understanding the patient’s pre-existing psychosocial functioning is imperative to providing complete holistic care. Palliative care consultation can be a helpful service to patients by providing in depth discussion on goals of care related to prognosis and patient preferences, transitional planning, family support and symptom relief management.
Inclusion Criteria
- All patients admitted to the trauma service
Exclusion Criteria
- None
Diagnostic Evaluation
· Patients should be assessed per ATLS guidelines with labs, imaging, consults, and interventions as deemed necessary by trauma team to determine extent of injuries, co-morbid conditions, and general prognosis.
Practice Recommendations for Management
All trauma patients: WITHIN 24 HRS OF ADMISSION
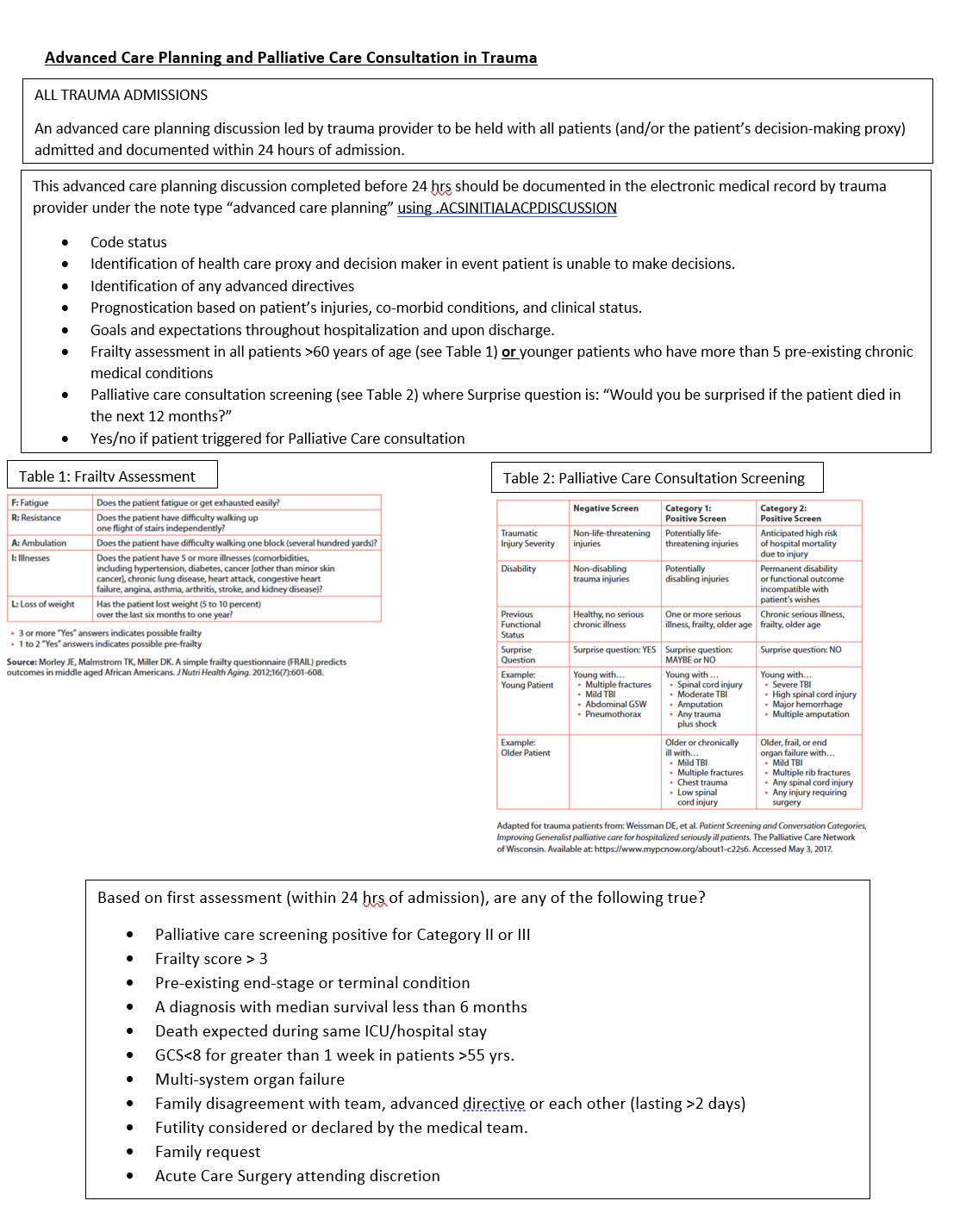
- An advanced care planning discussion should be held with all patients (and/or the patient’s decision-making proxy) admitted to the trauma service within 24 hours of admission.
-
- For trauma patient’s less than 19 years of age, discussions should occur with the patient’s legal guardian/parent.
-
- This initial advanced care planning discussion should be led by a trauma service provider (physician or APP).
- The initial advanced care planning discussion should address the following:
-
- Code status
- Identification of health care proxy and decision maker in event patient is unable to make decisions.
- Identification of any advanced directives
- Prognostication based on patient’s injuries, co-morbid conditions, and clinical status.
- Goals and expectations throughout hospitalization and upon discharge.
- Frailty assessment in all patients >60 years of age (see Table 1) or in younger patients who have more than 5 pre-existing chronic medical conditions
- Palliative care consultation screening (see Table 2)
- Palliative care consultation indicated/not indicated
-
- All advanced care planning discussions should be documented in the electronic medical record under the note type “advanced care planning”.
-
- Note template: .ACSINITIALACPDISCUSSION
-
Triggers for Palliative Care Consultation based on initial advanced care planning discussion:
- Palliative care consultation should be considered if any of the following are present:
-
- Positive palliative care screen (Category 1 or 2)
- Frailty score greater than 3 (based on Frail Questionnaire, Table 1)
- Pre-existing end-stage or terminal condition
- A diagnosis with median survival less than 6 months
- Death expected during same ICU/hospital stay
- GCS<8 for greater than 1 week in patients >55 yrs.
- Multi-system organ failure
- Family disagreement with team, advanced directive or each other (lasting >2 days)
- Futility considered or declared by the medical team.
- Family request
- Acute Care Surgery attending discretion
-
- Palliative Care consultation ideally should occur early in patient's hospital course with a goal of assessing and managing the patient via "palliative care bundle" (see Table 3) within 72 hours of admission.
TraumaTriggers for Geriatrics Consultation based on initial advanced care planning discussion:
- All patients
who>75triggeryears of age at admission - Age 65-75, consider geriatric consultation if conditions listed below are present:
-
- dementia
- 10 or more home prescription medications
- 2 or more ED visits or inpatient admission in past 6 months
- not living independently or residents of nursing homes or assisted living facilities
- provider discretion
-
- in cases where patient's meet criteria for
aboth Geriatrics and Palliative Care consultation:-
- Request consultation of both services. Geriatrics will primarily assist with geriatric medical conditions, whereas Palliative Care will primarily assist with advance care
consult:planning/goals of care. - This should occur with ongoing communication between Geriatric Medicine, Palliative Care and Trauma teams.
- Request consultation of both services. Geriatrics will primarily assist with geriatric medical conditions, whereas Palliative Care will primarily assist with advance care
-
Triggers for Family Meeting WITHIN 72 HRS OF ADMISSION
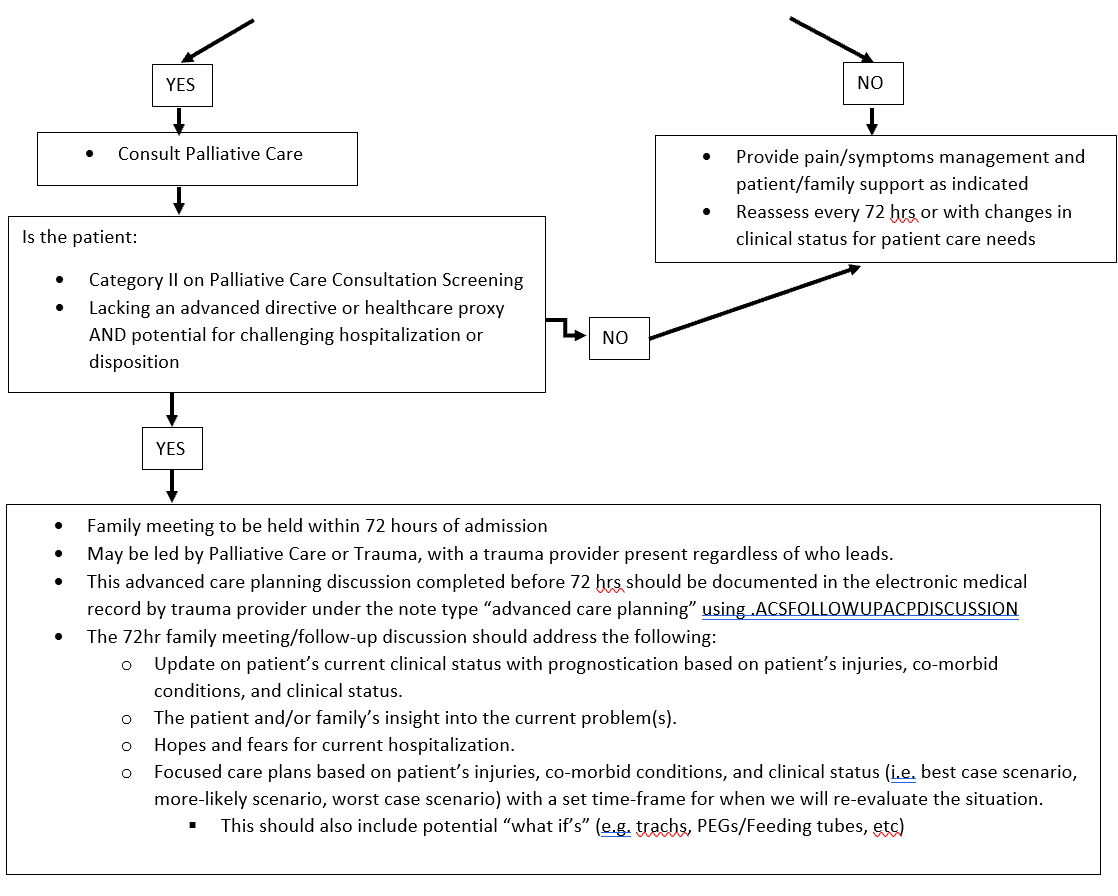
Palliative Care consultation ideally should occur early in patient’s hospital course with a goal of assessing patient and completing “palliative care bundle” (see Table 3) within 72 hour of admission.In addition to bundle, allAll Category II patients require a family meeting within 72 hrs of admission.- Any patient lacking an advanced directive or healthcare proxy AND potential for challenging hospitalization or disposition.
- Family meeting may be led by Palliative
CareCare, Geriatric Medicine or Trauma.-
- A trauma provider should be present for this discussion regardless of who leads the meeting.
-
AllThisfamilyadvanceddiscussionscare planning discussion should be documented in the electronic medical record under the note type “advanced care planning”.-
- Note template: .ACSFOLLOWUPACPDISCUSSION
-
- The 72hr family meeting/follow-up discussion should address the following:
-
- Update on patient’s current clinical status with prognostication based on patient’s injuries, co-morbid conditions, and clinical status.
- The patient and/or family’s insight into the current problem(s).
- Hopes and fears for current hospitalization.
- Focused care plans based on patient’s injuries, co-morbid conditions, and clinical status (i.e. best case scenario, more-likely scenario, worst case scenario) with a set time-frame for when we will re-evaluate the situation.
-
- This should also include potential “what if’s” (e.g. trachs, PEGs/Feeding tubes, etc)
-
-
Follow-up Care
- Significant changes in a patient’s clinical status, should prompt additional advanced care planning discussions as needed.
- If consulted, palliative care will continue to follow the patient throughout his/her hospital course as indicated.
Outcome Measures and Guideline Adherence
- Timing and documentation of initial advanced care planning discussions will be monitored on 80% of all trauma patients
- Timing and utilization of palliative care services will be monitored on all trauma mortalities and hospice/CMO discharges.
- Pathway will be re-assessed following a 3 month pilot study.
Key Contributors
- Emily Cantrell, MD | Division of Acute Care Surgery | Author
- Charity Evans, MD | Division of Acute Care Surgery | Author
- Elizabeth Mahal, MD | Department of Emergency Medicine | Author
- Carrie Siedlik, APRN-NP | Palliative Care Medicine | Author
- Remy Kaslon, APRN-NP | Palliative Care Medicine | Author
- Katie Circo, RN | Nursing Professional Development Specialist MICU and SICU, Nebraska Medicine | Author
- Katherine Maliszewski, MD | Internal Medicine/Geriatric Medicine | Author
Last Updated
June, 2023
References
- American College of Surgeons. Trauma Quality Improvement Program Palliative Care Best Practice Guidelines. https://www.facs.org/media/g3rfegcn/palliative_guidelines.pdf
- American College of Surgeons. Trauma Quality Improvement Program Geriatric Trauma Management Guidelines. https://www.facs.org/media/314or1oq/geriatric_guidelines.pdf
- Fiorentino M, et al. Palliative care in trauma: Not just for the dying. J Trauma and Acute Care Surg. 2019:87(5):1156-1163.
Appendix and Supplemental Materials
Figure 1. Model for advanced care planning discussions and consultation of palliative care in trauma.
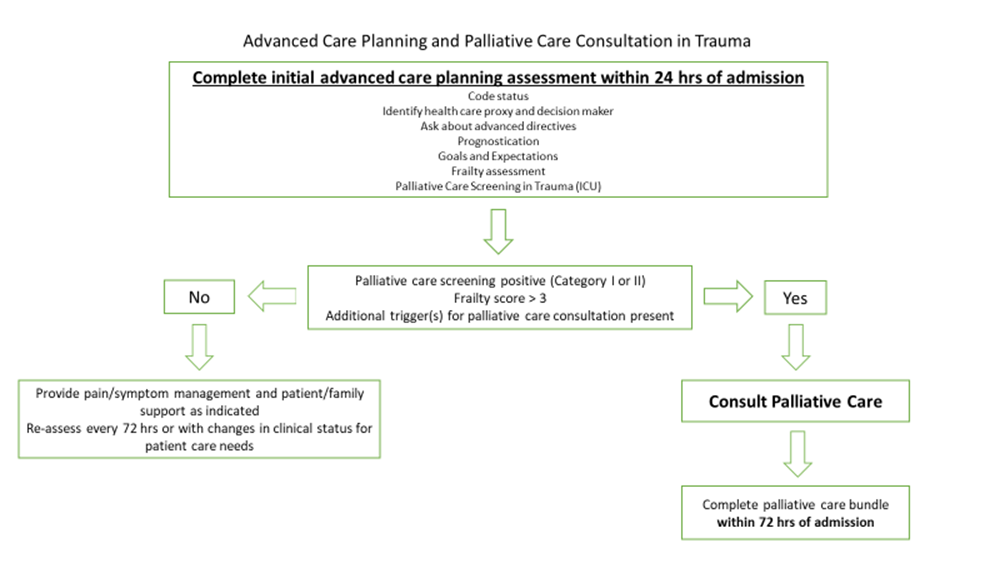
Table 1. 5 item FRAIL Questionnaire
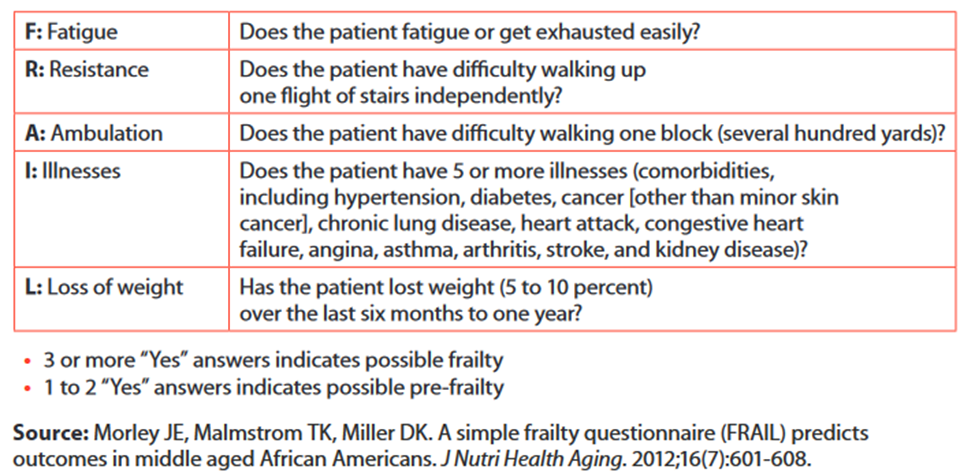
Table 2. Palliative Care Screening in Trauma
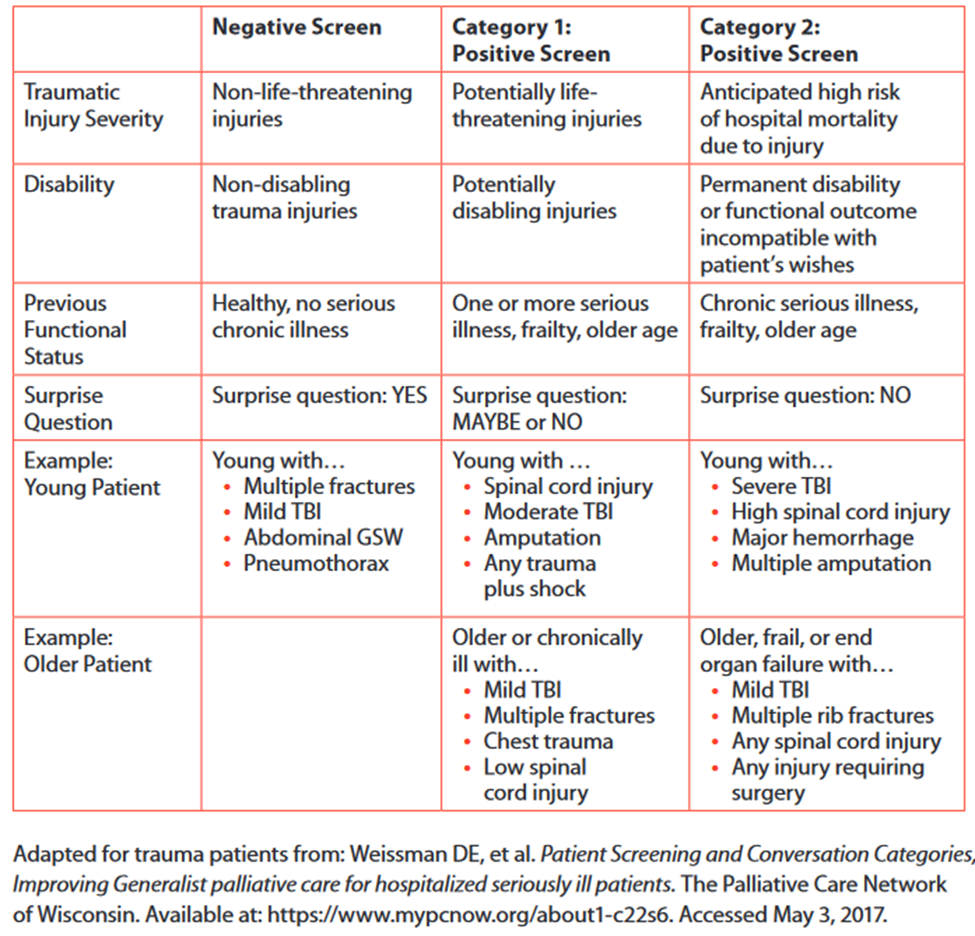
*Surprise question example: “Would you be surprised if the patient died in the next 12 months?”
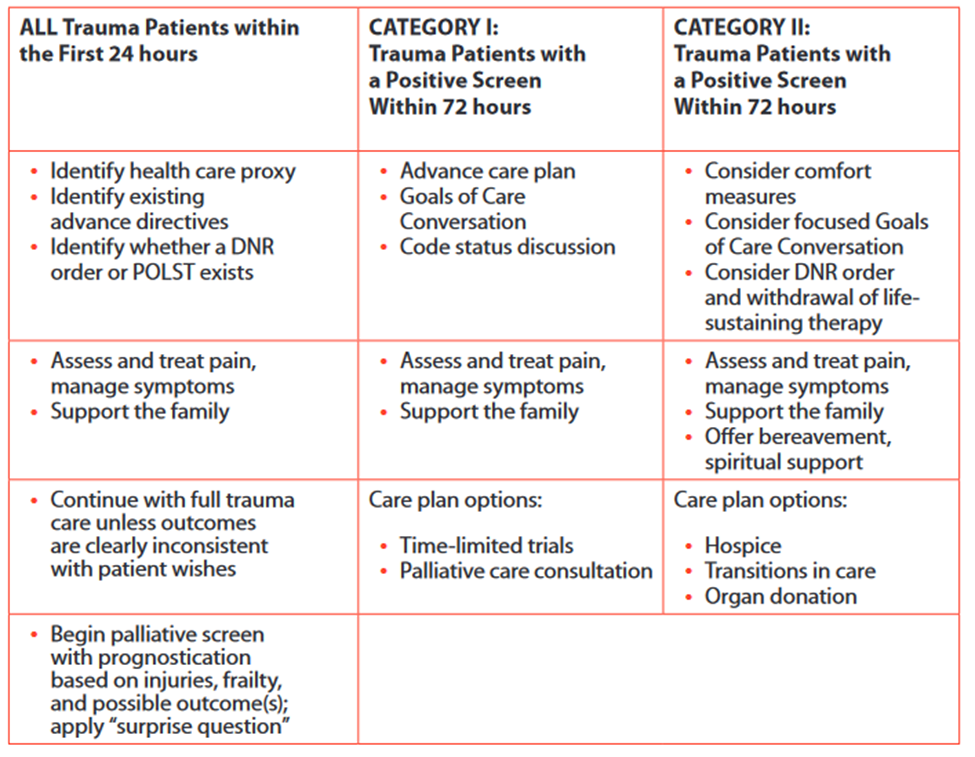
Table 3. Palliative Care Bundle
Guideline Algorithm