Evaluation and Management of Atrial Fibrillation
Purpose
- Establish a unified guideline for the diagnosis and treatment of new-onset atrial fibrillation (AF) in Acute Care Surgery patients.
Background/Definitions
- Primary AF: AF with no precipitating cause
- Secondary AF: AF precipitated by a secondary or reversible
causecondition (e.g.,volume overload,surgery, sepsis, acute MI, etc. --most ofyourour ICU patients)
Inclusion Criteria
- Patients with new onset atrial fibrillation.
Exclusion Criteria
- Patients with chronic atrial fibrillation.
Diagnostic Evaluation
- History:
- previous history of arrhythmia?
- currently on anticoagulation?
- Physical:
- irregular heart rhythm
- Imaging/Labs/Tests:
- ECG
- BMP+Mg+Phos
- Other labs at discretion of provider (CBC, blood cultures/infectious work-up, cardiac enzymes, etc)
Practice Recommendations for Management
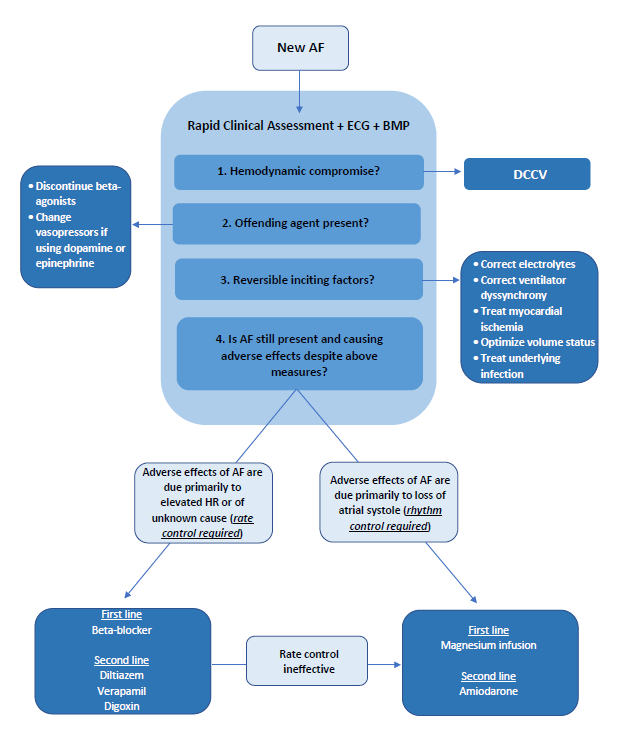
- New-onset, secondary AF is an organ dysfunction that signals something is wrong--need to address underlying cause while seeking to control rate/rhythm.
- Helpful questions to guide initial approach of patient with AF:
- 1) is the AF causing an immediate problem?
- 2)why is AF happening now (is this primary or secondary AF)?
- 3) should I worry about longer-term problems from the AF?
?
- Is the AF causing an immediate problem?
- When to consider rhythm control first:
-
- Emergent AF with severe decompensation:
-
- hypotension (SBP<100 or <110 for patients 65 and older), acute heart failure, altered mental status, cardiac ischemia
- if yes --> DCCV (direct current cardioversion)
- consider pairing DCCV with anti-arrhythmic such as amiodarone to increase probability of longer-term success.
-
- Non-emergent AF:
-
- consider a rhythm control strategy first if you think the patient needs atrial kick (i.e. severe mitral stenosis, aortic stenosis) or cannot tolerate nodal blocker (Wolf Parkinson White Syndrome)
-
- Emergent AF with severe decompensation:
-
- When to consider rate control first:
-
- Note: in most instances you can use rate control FIRST.
- Heart rate is higher than it would be with acute illness, but not immediately life threatening to require DCCV.
- Patient has contraindications to anticoagulation.
- Evidence to support a rate control strategy first during secondary AF: success of DCCV is low in secondary AF (as in ICU) --43% at 1 hr, 23% at 24 hrs remain in NSR.
-
- When to consider rhythm control first:
- Why is AF happening now?
- Fix electrolytes (magnesium is an effective rhythm control treatment).
- Fix volume status.
- Look for untreated infection.
- Remove beta-agonists.
- Should I worry about long-term problems from the AF?
- Arterial thromboembolism and AF recurrence are long-term concerns after new-onset AF in critically ill patients
- 44% af AF recurrence in 1 year after new-onset AF in sepsis.
- Arterial thromboembolism and AF recurrence are long-term concerns after new-onset AF in critically ill patients
- Cardiology follow-up (either inpatient or outpatient) for long-term rhythm monitoring and treatment plan should be considered.
Outcome Measures and Guideline Adherence
- AF (arrhythmia) is a PI filters for Trauma and Critical Care Surgery that is actively tracked/monitored.
Related Policies
Key Contributors
- Keely Buesing ,MD, FACS, Acute Care Surgery Division
Last Updated
February, 2023
References
- 2019 AHA/ACC/HRS Update
- 2014 AHA/ACC/HRS Guideline
- Um K et al. Pre- and post-treatment with amiodarone for elective electrical cardioversion of atrial fibrillation: a systematic review and meta-analysis. Europace. 2019;21(6):856-863.
- Arrigo M et al. Disappointing success of electrical cardioversion for new-onset atrial fibrillation in cardiosurgical ICU patients. Crit Care Med. 2015;43(11):2354-2359.
- Walkey AJ et al. Practice patterns and outcomes of treatments for atrial fibrillation during sepsis: a propensity-matched cohort study. Chest. 2016;149:74-83.
- Bosch NA et al. Comparative effectiveness of heart rate control medications for the treatment of sepsis-associated atrial fibrillation. Chest. 2021;159(4):1452-1459.
- Davey MJ et al. A randomized controlled trial of magnesium sulfate, in addition to usual care, for rate control in atrial fibrillation. Ann Emerg Med. 2005;45(4):347-353.
- Onalan O et al. Meta-analysis of magnesium therapy for the acute management of rapid atrial fibrillation. Am J Cardiol. 2007;99(12):1726-1732.
- Bosch NA et al. Atrial fibrillation in the ICU. Chest. 2018;154:1424-1434.
Supplemental Materials
- “Etiology of Atrial Fibrillation” schematic.