Guidelines for Imaging the Pediatric Trauma Patient
Purpose:
These guidelines are meant to help guide the provider’s decision-making regarding imaging of the pediatric trauma patient during the initial trauma evaluation.
Background/Definitions:
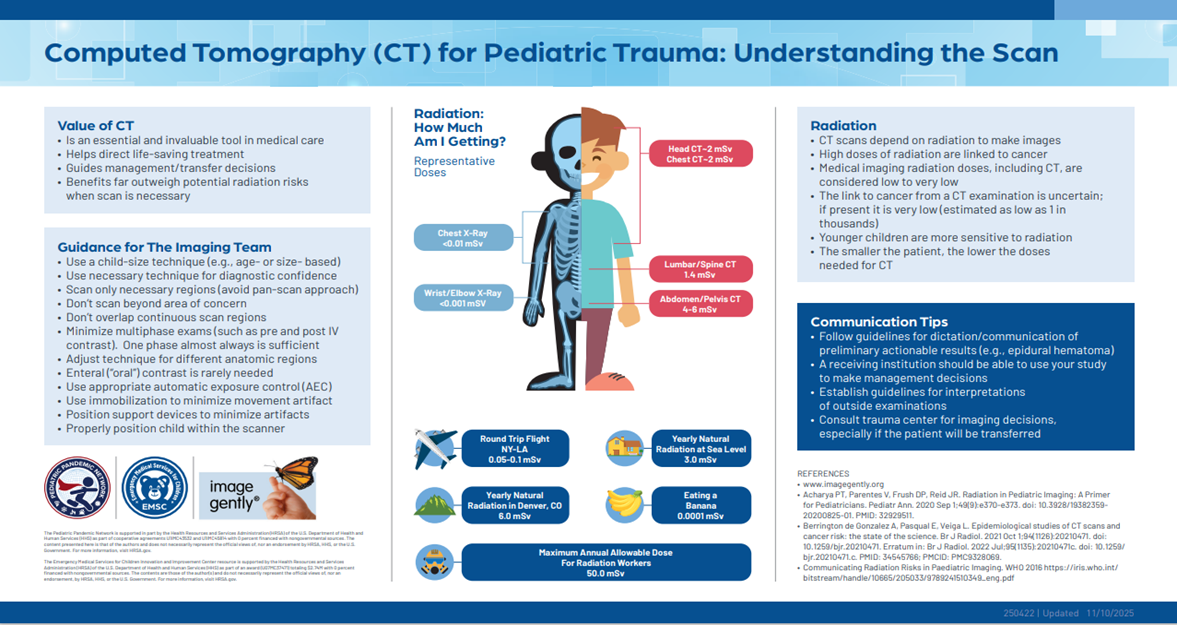
There is considerable agreement that diagnostic imaging, particularly with computed tomography (CT), results in significant radiation exposure in children. In addition, while the precise implications of this radiation exposure have not been defined, there is consensus that it is associated with a low, but real, increase in the long-term development of fatal malignancy. Children are particularly sensitive to the effects of radiation given their small size (increase dose per unit area) and the long latent times between exposure and the resultant cancer. Exposure to diagnostic radiation in children has increased dramatically in recent years with increasing use of CT. The primary indication for these scans is for the evaluation of trauma and appendicitis. Both the American Academy of Pediatrics and the American Pediatric Surgical Association have recently published statements encouraging their members to adhere to the ALARA principle, “As Low as Reasonably Achievable,” when obtaining imaging in pediatric patients (1, 2).
While the use of CT to diagnosis injuries in children has been increasing, there is a growing body of literature to suggest that CT is not required for routine evaluation resulting in the creation of several prediction rules to help guide the physician on what type and when imaging might be indicated to adequately assess the pediatric trauma patient.
In light of this evidence, we recommend adherence to the ALARA principle when imaging pediatric trauma patients. Specifically, we recommend:
- Avoidance of the use of protocols which automatically result in the performance of multiple CT scans (i.e. head, cervical spine, chest, and abdomen and pelvis) in pediatric patients.
- Avoid further CT imaging once the decision to transfer to definitive care is made, unless the accepting institution specifically requests a scan prior to transfer.
- All CT scans on children should be performed using “pediatric” weight-based dose-reduction protocols per Nebraska Medicine radiology procedures.
- Accepting institution should avoid repeating scans unnecessarily and when possible utilize alternative imaging strategies.
Guideline Inclusion Criteria:
- Pediatric trauma patients less than 19 years of age.
Guideline Exclusion Criteria:
- Patients 19 years of age and older.
Practice Recommendations for Management:
Initial Assessment:
- Pediatric trauma patients should be assessed per ATLS guidelines on arrival to ED.
-
- Chest x-ray and pelvis x-ray should be used as adjuncts to the primary survey as indicated by patient’s clinical status and mechanism of injury.
-
- Can consider not obtaining chest x-ray in low-grade mechanisms of injury if patient is able to be observed following injury.
- Chest x-ray should be obtained in setting of high-grade mechanism of injury, abnormal physiology and/or intubation.
-
- Routine use of eFAST in pediatric trauma patients is not supported by literature due to decreased sensitivity and specificity in pediatric patients when compared to adults. eFAST, however, may still be beneficial in decision making for certain clinical scenarios (i.e. hypotensive, blunt trauma patient) and should be utilized at the discretion of the trauma provider.
- Chest x-ray and pelvis x-ray should be used as adjuncts to the primary survey as indicated by patient’s clinical status and mechanism of injury.
-
- The use of a skilled child life specialist to help minimize the injured child’s fear and anxiety can markedly reduce the amount of sedation required during the initial assessment and subsequent imaging. Their liberal use is recommended when available.
- If the child requires sedation to complete the trauma assessment or imaging, experienced pediatric personnel with credentials to administer sedation are recommended.
Additional Imaging:
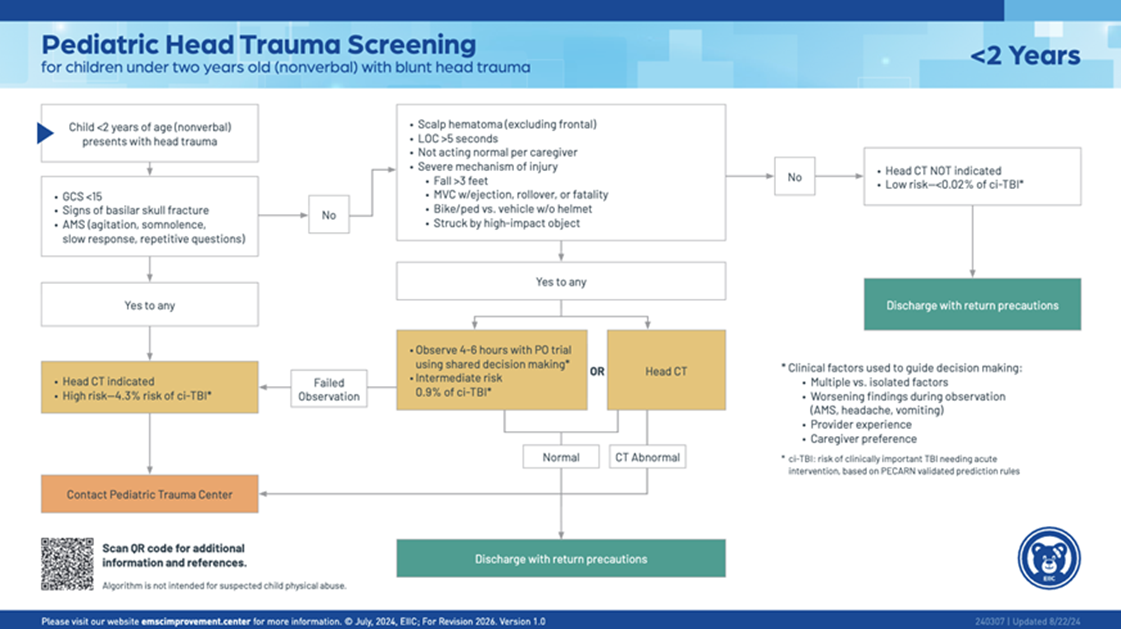
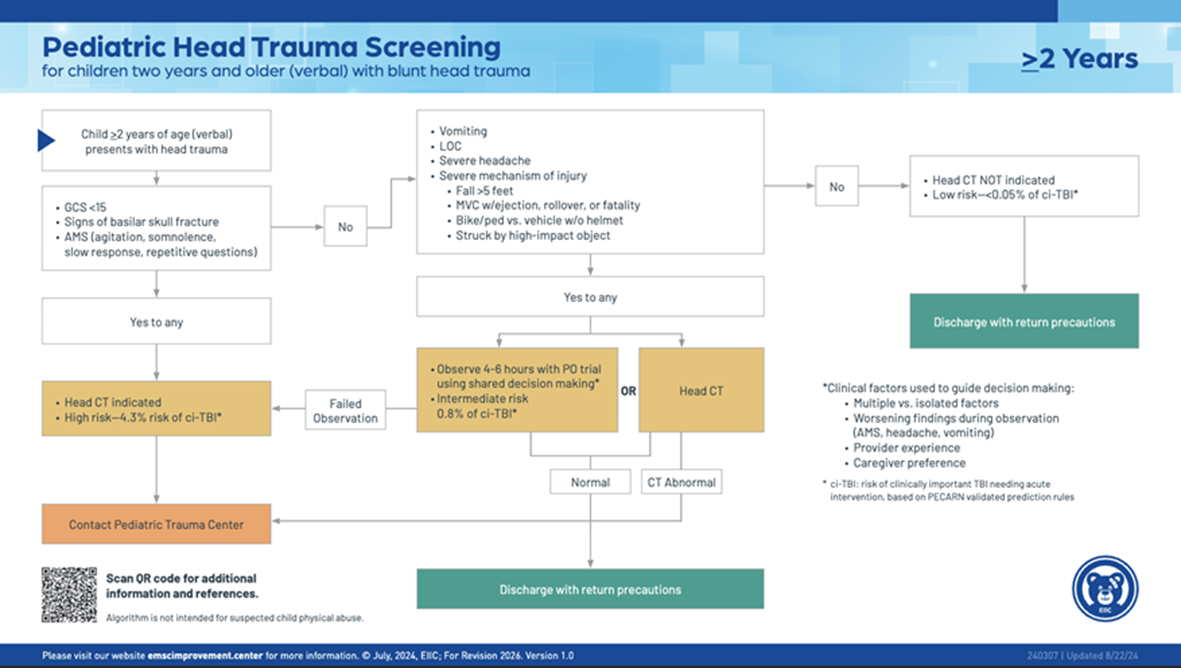
- Pediatric Head Imaging
-
- Decision to obtain CT imaging of the head in pediatric trauma patients should be based on PECARN (Pediatric Emergency Care Applied Research Network) criteria which are as follows:
-

-
-
- Routine repeat CT head is not recommended but should be considered if there is a decline in GCS/worsening neurological exam, in sedated patients who cannot be evaluated, or at discretion of neurosurgical team.
-
- Pediatric Cervical Spine Imaging:
-
- The asymptomatic child with a reliable normal exam does not require imaging to clear the cervical spine, regardless of mechanism.
- The overall incidence of c-spine injury in children is low (<1%). However, may be seen in up to 30% of pediatric TBI patients and overall incidence of approximately 15% in non-accidental trauma.
- Injury is most difficult to assess in the 2-5 year age group.
- The risk for a higher anatomical injury is greater the younger the child.
-
- Younger children are more likely to suffer ligamentous injury than fracture.
-
- Canadian C-spine Rule (CCR) and NEXUS criteria are standard for adults but are not sensitive or specific enough to be used for children <10 years of age.
- Decision to obtain c-spine imaging in pediatric patients following blunt trauma should be based on PECARN criteria or the AAST scoring system for patients less than 3 years of age.
-
- PECARN Criteria:
-
- Consider CT c-spine in the following:
-
- GCS 3-8 or AVPU =U
- Abnormal airway, breathing, or circulation
- Focal neurologic deficits
-
- Consider c-spine x-rays in the following:
-
- GCS 9-14, AVPU=V or P, or other signs of altered mental status
- Self-reported neck pain or neck tenderness on examination
- “substantial” head or torso injury (“substantial” injuries defined as warranting inpatient observation or surgical intervention such as skull fracture, pneumothorax, solid organ injury, spine fracture, pelvic fracture)
-
- If none of the above listed risk factors are present, then consider clinical clearance.
- Consider CT c-spine in the following:
-
- PECARN Criteria:
-
-

-
-
-
-
- AAST scoring system for patients less than 3 years:
-
- Criteria examined:
-
- GCS<14 = 3 points
- GCS (eye criterion) =1 = 2 points
- Motor vehicle crash (MVC), fall from height>10ft, intentional injury as mechanism of injury = 2 points
- Age 24-36 months = 1 point
-
- Scoring:
-
- 0-1 = no imaging
- 2-4 = imaging a clinician discretion
- 5-8 = imaging (CT c-spine) recommended
-
- Criteria examined:
-
- Non-contrast CT c-spine is generally the recommended study of choice for evaluating the cervical spine, as the sensitivity and specificity of c-spine x-rays is inconsistent.
- Consider MRI c-spine if neck pain is out of proportion to CT results or concerned for spinal cord injury or ligamentous injury.
- SCIWORA—(spinal cord injury without radiographic abnormality) term used to descript neurologic deficit in the absence of findings on plain radiographs or CT scan. MRI is recommended next, but up to 40% of affected patients do not have an injury detected by MRI.
- AAST scoring system for patients less than 3 years:
-
-
-
- Screening for Blunt Cerebrovascular Injury (BCVI) in pediatric trauma patients
-
- Routine use of CTA neck for BCVI screening in pediatric trauma patients should be avoided due to the associated radiation exposure and low incidence of BCVI in the population.
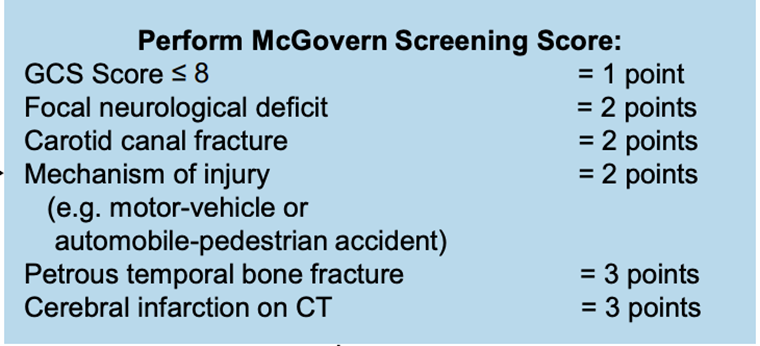
- The McGovern Score should be utilized to help determine if a patient should undergo CTA neck for screening of BCVI.
-
- A score of ≥3 points is high-risk for BCVA and CTA neck should be performed.
-
- Routine use of CTA neck for BCVI screening in pediatric trauma patients should be avoided due to the associated radiation exposure and low incidence of BCVI in the population.
-
- Pediatric Chest Imaging
-
- X-ray
-
- Chest x-ray is recommended in the initial evaluation of all pediatric trauma patients, regardless of age, in the presence of abnormal physiology, high-grade mechanism of injury, or intubation.
-
- Ultrasound
-
- a pericardial US should be considered if the chest x-ray reveals a normal mediastinum, but other injuries (e.g. rib fractures, sternal fracture, scapula fracture, pneumothorax or contusion) are present.
-
- CT scan
-
- CT chest should be used selectively in the evaluation of pediatric trauma patients to reduce unnecessary imaging.
-
- A CT chest is reported to have no impact on management of the pediatric trauma patient with absent or minor abnormalities on chest x-ray (ex. simple pneumothorax, simple hemothorax, pulmonary contusion, or isolated rib fractures).
- if indicated, a CT chest should be obtained with IV contrast.
- A CT chest is reported to have no impact on management of the pediatric trauma patient with absent or minor abnormalities on chest x-ray (ex. simple pneumothorax, simple hemothorax, pulmonary contusion, or isolated rib fractures).
-
- A CT chest is recommended for children with abnormal mediastinal contour of an age-appropriate shaped chest, more significant abnormalities on chest x-ray or an abnormal pericardial US.
- CT chest should be used selectively in the evaluation of pediatric trauma patients to reduce unnecessary imaging.
-
- X-ray
-

- Pediatric Abdominal Imaging
-
- Ultrasound
-
- Routine use of eFAST in pediatric trauma patients is not supported by literature due to decreased sensitivity and specificity in pediatric patients when compared to adults.
- eFAST, however, may still be beneficial in decision making for certain clinical scenarios and IS RECOMMENDED for the assessment of pediatric trauma patients presenting in shock (i.e. hypotensive), when CT is not available or feasible or at the discretion of the trauma provider.
-
- CT scan
-
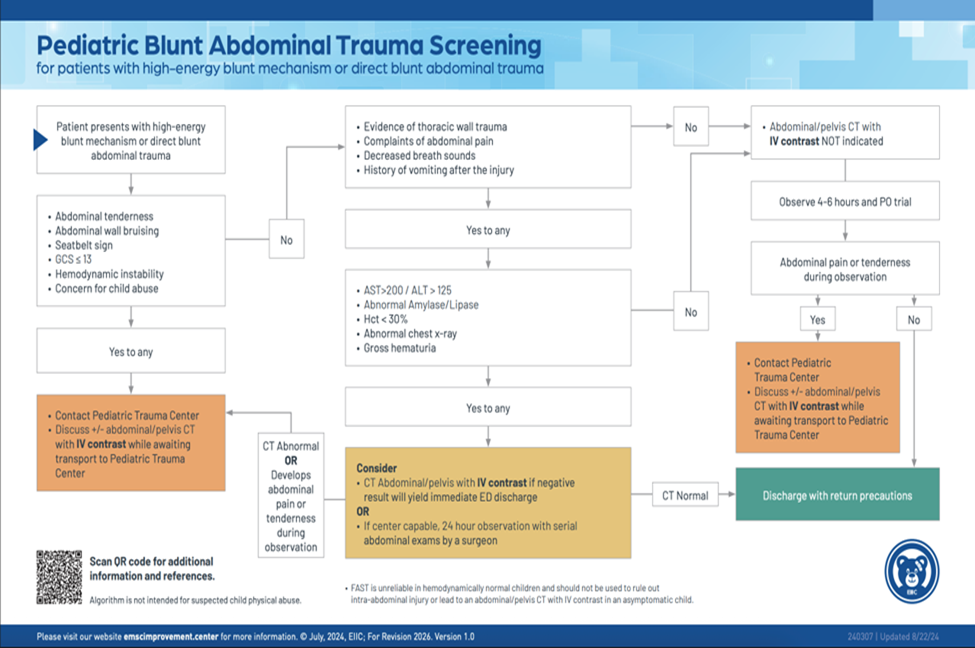
- The PECARN Prediction Rule or the Streck Criteria should be applied to pediatric patients presenting after high-energy blunt mechanism or with blunt abdominal trauma to help determine when CT scans are indicated
- CT abdomen/pelvis should be used selectively in the evaluation of pediatric trauma patients to reduce unnecessary imaging.
- If indicated, a CT abdomen/pelvis should be obtained with IV contrast in at least 2 phases (typically arterial and venous) to help identify and distinguish active hemorrhage.
-
- The portal venous phase is optimal for evaluation of visceral parenchyma.
- delayed excretory phase images are essential for the evaluation of genitourinary trauma (e.g. renal collecting system or bladder injuries) and should be considered in the setting of gross hematuria or microscopic hematuria with hypotension.
- oral contrast is typically not indicated unless there is concern for duodenal injury.
-
-
- Ultrasound
-
- Pediatric Thoracic and Lumbar Spine imaging
-
- Routine imaging of the spine based on mechanism of injury alone is generally not recommended.
- AP and lateral x-rays are indicated for physical examination findings or symptoms.
-
- Obesity/body habitus and other factors may affect the quality of the x-rays.
-
- If a patient is undergoing CT chest, abdomen or pelvis, obtain thoracic and lumbar spine reconstructions.
- If patient has a neurologic deficit/abnormality, consider obtaining MRI for evaluation of the spine.
-
- Pediatric Orthopedic Injury Imaging
-
- Plain x-rays of the injured area are the standard for initial assessment of possible orthopedic injury.
-
- Use “rule of twos” when ordering x-rays:
-
- Two views – at least obtain an AP and lateral view of the injured limb/area
- Two joints—consider obtaining x-rays of the joints above and below the site of injury to rule out an potential associated fracture or dislocation.
- Two limbs—after consultation with orthopedic surgery, a request for x-rays of the injured and non-injured limb is made to aid in evaluation/diagnosis of certain injuries.
- Two times—pre- and post- reduction x-rays are needed to assess the adequacy of any fracture or dislocation manipulation or reduction.
-
- Use “rule of twos” when ordering x-rays:
-
- CT is not indicated for the routine evaluation of many orthopedic injuries and should only be ordered following consultation with orthopedic surgery when needed for pre-operative planning of complicated fractures.
- MRI of affected area can be helpful in identifying occult injuries or further evaluating certain injuries. MRI is rarely indicated in the acute setting and should be considered following consultation with orthopedic surgery.
- Plain x-rays of the injured area are the standard for initial assessment of possible orthopedic injury.
-
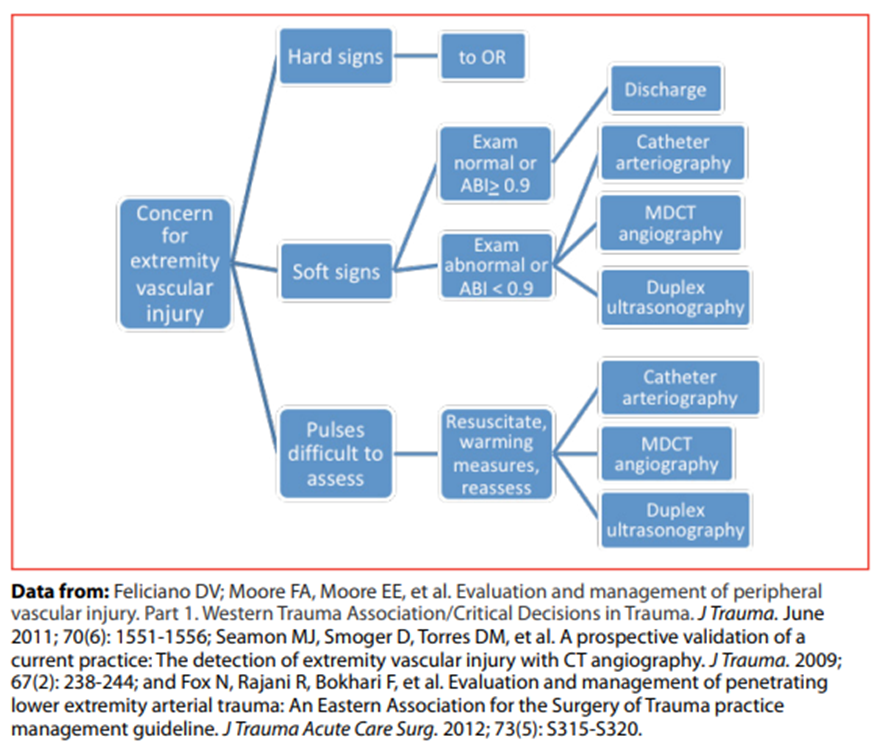
- Imaging for pediatric extremity vascular injury
-
- Extremity vascular imaging in the pediatric population is similar to that of adults.
- CTA of affected extremity remains the gold standard to evaluate for vascular injury in extremity trauma in the hemodynamically stable patient without hard signs of vascular injury.
-
- Vasospasm cannot be reliably diagnosed by CTA and may require catheter angiography.
-
- Hard signs of vascular injury
-
- Bruit/thrill
- Active/pulsatile hemorrhage
- Pulsatile/expanding hematoma
- Signs of limb ischemia and/or compartment syndrome including the 5 “P’s” (pallor, paresthesia, pulse deficit, paralysis, and pain on passive extension)
- Diminished or absent pulses
-
- Soft signs of vascular injury
-
- Hypotension or shock
- Neurologic deficit
- Nonexpanding/nonpulsatile hematoma
- Proximity of wound to major vascular structures
-
-
Outcome Measures and Guideline Adherence:
- All pediatric trauma patients will be reviewed for imaging obtained and adherence to above stated imaging guidelines. Deviations from guidelines will be investigated further for with intervention and education as needed when trends or opportunities for improvement are identified.
- Adherence to guidelines will be reported in the Pediatric Performance Improvement Process (PIPs) meeting.
Key Contributors:
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Abby Josef, MD | Division of Acute Care Surgery, Faculty | Reviewer
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Coordinator | Co-Author
-
Megan Samland, DNP, APRN-NP, AGACNP-BC, FNP-BC | Division of Acute Care Surgery, APP | Co-Author
Last updated:
· February, 2026
References:
- Brody, Frush, Huda, Brent, and the Section of Radiology, “Radiation Risk to Children from Computed Tomography,” Pediatrics 120: 677-682, 2007.
- Rice, Frush, Farmer, Waldhausen, and the APSA Education Committee, “Review of radiation risks from computed tomography: essential for the pediatric surgeon. J Pediatr Surg 42: 603-7, 2007.
- Kupperman N, Holmes JF, Dayan PS, et al. Pediatric Emergency Care Applied Research Network (PECARN). Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet. 2009; 374(9696): 1160-70.
- Pieretti-Vanmarcke R, Velmahos GC, Nance ML, et al Clinical clearance of the cervical spine in blunt trauma patients younger than 3 years: A multi-center study of the American Association for the Surgery of Trauma. J Trauma 2009; 67(3):543-550.
- Markel, Kumar, Koontz, et al. The utility of computed tomography as a screening tool for the evaluation of pediatric blunt chest trauma. J Trauma 67:23-28, 2009.
- Singh, Kalra, Moore, et al. Dose reduction and compliance with pediatric CT protocols adapted to patient size, clinical indication, and number of prior studies. Radiology 252: 200-208, 2009.
- Chwals, Robinson, Sivit, et al. Computed tomography before transfer to a level I pediatric trauma center risks duplication with associated increased radiation exposure. J Pediatr Surg 43 2268-2272, 2008.
- ACS Trauma Quality Programs Best Practice Guidelines in Imaging. imaging_guidelines.pdf (facs.org) October, 2018.
- Holmes JF, Yen K, Ugaldge IT, et al. PECARN prediction rules for CT imaging of children presenting to the emergency department with blunt abdominal or minor head trauma: a multicentre prospective validation study. Lancet Child Adolesc Health. 2024 May; 8(5):339-347.
- Leonard JC, Harding M, Cook LJ, et a.l PECARN prediction rule for cervical spine imaging of children presenting to the emergency department with blunt trauma: a multicentre prospective observational study. Lancet Child Adolesc Health. 2024 Jul; 8(7):482-490.
- Chung S, Mikrogianakis A, Wales PW, et al. Trauma Association of Canada Pediatric Subcommittee National Pediatric Cervical Spine Evaluation Pathway: Consensus guidelines. J Trauma. 2011; 70(4):873-884.
- Nigrovic LE, Rogers AJ, Adelgais KM, et al. Pediatric Emergency Care Applied Research Network (PECARN) Cervical Spine Study Group. Utility of plain radiographs in detecting traumatic injuries of the cervical spine in children. Pediatr Emerg Care. 2012; 28(5):426-432.
- Herbert JP, Venkataraman SS, Turkmani AH, Zhu L, et al. Pediatric blunt cerebrovascular injury: The McGovern screening score. J Neurosurg Pediatr. 2018; 21(6):639-649.
- Venkataraman SS, Herbert JP, Ravindra VM, et al. Multi-center validation of the McGovern Pediatric Blunt Cerebrovascular Injury Screening Score. J Neurotrauma. 2023; 40(13-14):1451-1458.
- Emergency Medical Services for Children Innovation and Improvement Center (EIIC) (2025). EIIC: Best Practices in Pediatric Trauma Imaging. https://emscimprovement.center/education-and-resources/peak/multisystem-trauma/imaging/