Guidelines for the Initial Management of Frostbite
Purpose:
- Provide guidance on the initial evaluation and management of patients sustaining frostbite injuries as well as recommendations regarding wound care and soft tissue management.
Background/definitions:
- Frostbite is the tissue damage resulting from exposure to cold temperatures, usually from freezing of tissues, which results in cellular damage and tissue necrosis. The extent of frostbite depends on the temperature and duration of exposure.
Guideline Inclusion Criteria:
- Patients with history of recent cold exposure with evidence of soft tissue injury (frostbite) presenting to UNMC/NM emergency department
Guideline Exclusion Criteria:
- Patients without history of recent cold exposure
- Patients with history of cold exposure but without evidence of soft tissue injury 72 hrs after exposure.
- Referrals/transfers from outside hospitals—These patients should be referred to closest regional burn center.
Diagnostic Evaluation:
- Diagnosis of frostbite is based on history and clinical exam.
- History:
- Patients should have clinical history consistent with diagnosis of frostbite (i.e. exposure to cold or wet environment)
- Physical exam:
- Frostbite most commonly occurs on hands, feet, ears, and nose. However, can be present on any part of the body exposed to cold or wet conditions for a period of time.
- Findings consistent with frostbite include:
-
- Initially reddish (lighter skin), grayish (darker skin), pale/white or bluish/cyanotic discoloration in involved tissues.
- Tingling, stinging sensations or decreased/loss of sensation
- Involved tissues feel cold, stiff, or woody to palpation
- Blisters may or may not be present on initial examination but often develop over first 24-48 hours
-
- Additional labs and imaging should be obtained at physician discretion based on clinical status of patient, length of cold exposure, associated trauma, need for resuscitation, etc.
Practice Recommendations for Management:
- Initial frostbite management:
- Remove any wet clothing.
- Assess and resuscitate hypothermic patients as indicated (see hypothermia guidelines)
- Avoid re-freezing.
- Rapid re-warming of injured parts
-
- Water baths at temperatures of 37⁰-39⁰ C (98.6⁰-102.2⁰F) over 30 minute intervals is recommended.
- Other methods for active re-warming include: warm IV fluids, warm blankets, Bair hugger, etc.
- Clinical findings, such as the return of sensation, presence of flushing in involved tissues, and involved tissues are pliable or soft (i.e. not hard and frozen), will determine the length of time of rewarming.
-
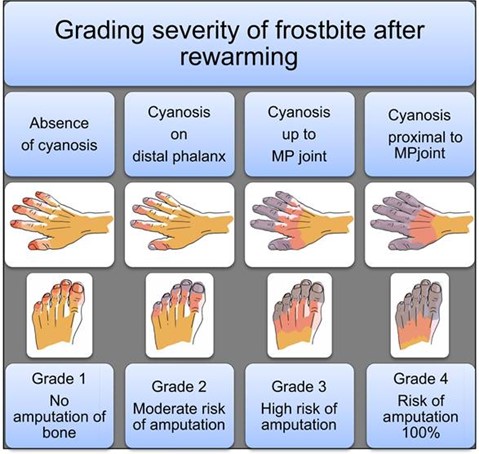
- Determine grade and depth of frostbite
-
-
-
-
- Depth
-
- Superficial – no blisters present
- Partial thickness – serous blisters present
- Full thickness – hemorrhagic blisters present
-
- Depth
-
-
-
-
-
-
-
- patients with grade 3 or 4 frostbite (cyanosis persisting proximal to the distal phalanx after rewarming) and/or demonstrated loss of perfusion at or proximal to the proximal interphalangeal joint of a finger or toe, or the interphalangeal joint of the great toe or thumb immediately after rewarming, consider thrombolytic therapy. (see Guidelines for Thrombolytic Therapy for Frostbite)
-
-
- Pain control:
-
- The re-warming process is often painful and analgesics (including narcotics) should be provided on an as needed basis.
-
- Tetanus prophylaxis should be provided if not up to date/given in the last 5 years.
- Patients should be kept NPO until initial evaluation is complete and need for thrombolytic therapy ruled out.
- Determine need for admission.
-
- If admission required, patients should be admitted to the trauma service.
-
-
- Photos:
- Photo documentation of wounds should be obtained on admission, 24 hours following admission and then serially every 2 days thereafter until discharge.
- Initial Wound care of frostbite
- Wound Care consult should be placed on admission.
- Wound care should be performed twice daily with nursing orders for wound care as indicated.
- Suggested soft tissue management:
-
- Recommendations regarding wound care and activity are based on depth of injury.
- Of note, frostbite may take up to 72 hrs before the depth of frostbite becomes apparent. (i.e. blisters form)
- Superficial thickness:
-
- No blisters present
- Wound care: consider aloe vera, place dry dressings, keep warm
- Activity: limited/gentle weight bearing of affected extremity for the first 48 hrs until soft tissue has fully declared. Following this, may weight bear as tolerated. Keep affected extremity elevated as able.
-
- Partial thickness:
-
- Serous blisters present
- Wound care:
- Activity: Avoid ambulation if on plantar aspects of feet. Otherwise, limited/gentle weight bearing and active range of motion of affected extremity for the first 48 hrs until soft tissue has fully declared. Following this, may weight bear as tolerated. Keep affected extremity elevated as able.
-
- Full thickness
-
- Hemorrhagic blisters present
- Wound care:
-
- blisters do not generally require debridement.
- Dress blisters and open areas in bacitracin followed by xeroform and gently secured with gauze. Avoid tight dressings.
-
- Activity: No weight bearing on the affected extremity for 72 hours. Active range of motion only. Keep affected extremity elevated.
-
- Additional topical agents:
-
- Choice of topical agents may vary between providers and can include (but are not limited to) the following:
-
- Aloe vera – topical thromboxane inhibitor
- Bacitracin – topical antibiotic
- Silver sulfadiazine – topical antibiotic
-
- Choice of topical agents may vary between providers and can include (but are not limited to) the following:
-
-
-
-
-
- Cotton, web roll, or lambs wool should be placed between digits/toes for extra protection and warmth.
- Affected extremities should be elevated with splinting/padding (i.e. Rooke boots) as needed
- For those patient’s with frostbite of the feet, ambulation should occur in protective footwear (i.e. off-loading shoe)
- PT/OT consults should be placed on admission to assist in mobility, range of motion and splinting of the affected extremity as indicated.
- In general, similar to burns, frostbite injuries will evolve over the first 72 hours and can take an extended period of time to demarcate. Waiting until the full extent of necrosis is apparent is recommended prior to surgical amputation (if needed) to allow for as much tissue salvage as possible.
- For patients with Grade 2, 3, and 4 frostbite where amputations may be required, inpatient consultation of orthopedic or plastic surgery may be obtained as needed at the discretion of the trauma attending.
-
-
- Medications for frostbite injury:
- Anti-platelet plus analgesia therapies
-
- The following regimen should be initiated on admission for any frostbite patient NOT undergoing thrombolytic therapy or AFTER completion of thrombolytic therapy/therapeutic anticoagulation in grade 3 or 4 frostbite patients unless contraindicated by medical history (i.e. renal insufficiency, h/o PUD/GI bleed, recent intracranial hemorrhage, etc.)
-
- Aspirin 81mg PO daily x 30 days
- Gabapentin 300 mg q8 hrs x 30 days
- Ibuprofen 600 mg q6 hrs x 14 days
-
- The following regimen should be initiated on admission for any frostbite patient NOT undergoing thrombolytic therapy or AFTER completion of thrombolytic therapy/therapeutic anticoagulation in grade 3 or 4 frostbite patients unless contraindicated by medical history (i.e. renal insufficiency, h/o PUD/GI bleed, recent intracranial hemorrhage, etc.)
-
- Additional multi-modal pain control should be provided as needed.
- In general, prophylactic antibiotics are not indicated.
- Anti-platelet plus analgesia therapies
Follow-up Care:
- Patients with frostbite injuries will follow-up in trauma surgery clinic for ongoing wound care with referrals to orthopedic or plastic surgery clinics as needed.
Outcome Measures and Guideline Adherence:
- Track patients with Grade 2 and higher frostbite every 6 months for adherence to guidelines
- Measures: status of wounds, need for amputation, need for thrombolytic therapies, involvement of consulting services (orthopedics, plastic surgery, wound care clinic, etc)
Related Policies:
- Hypothermia Guidelines
- Thrombolytic Therapy for the Management of Severe Frostbite
Key Contributors:
· Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
· Abby Josef, MD | Division of Acute Care Surgery, Faculty | Author
· Zach Bauman, MD | Division of Acute Care Surgery, Faculty | Author
· Karen Saxton | Division of Acute Care Surgery, Trauma Program Manager | Reviewer
· Meghan Blais, PharmD | Clinical Pharmacist, Nebraska Medicine | Reviewer
Last updated:
· 1/12/2023
References:
- Zaramo TZ, Green JK, Janis JE. Practical review of the current management of frostbite injuries. Plast Reconstr Surg Glob Open. 2022 Oct 24;10(10):e4618
- Murphy JV, Banwell PE, Roberts AH, McGrouther DA. Frostbite: Pathogenesis and treatment. J Trauma. 2000 Jan;48(1):171-8.
- Hickey S, et. al. Guidelines for thrombolytic therapy for frostbite. J Burn Care Res. 2020 Jan 30;41(1):176-183.
- Lacey AM, et al. An institutional protocol for the treatment of severe frostbite injury—A 6-year retrospective analysis. J Burn Care Res. 2021 Aug 4;42(4):817-820.