Initial Management of Burns
Purpose:
Provide a brief overview of the classification of burns, initial resuscitation and management, as well as guidelines on triage.
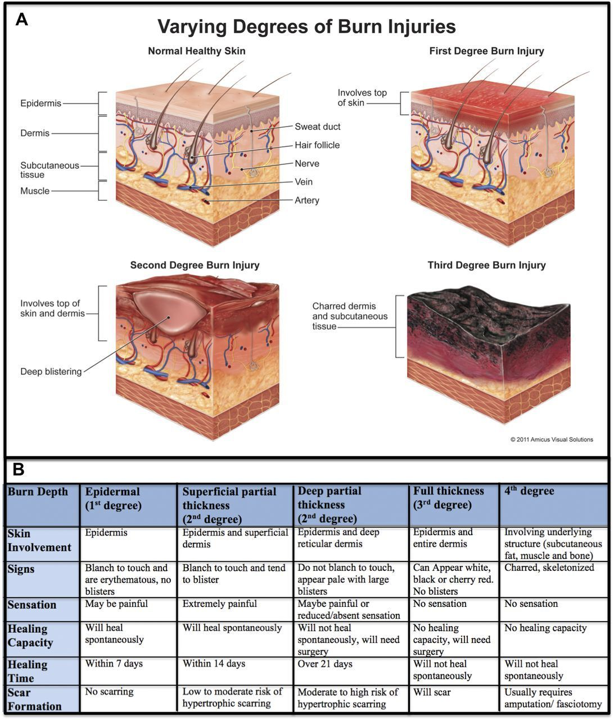
Classification of Burn Injuries:
- First Degree Burn (superficial)
- Involves only the epidermis (no penetration into the dermis)
- Skin appearance: warm, erythematous, no blistering or eschar present
- Painful
- Management: supportive cares (i.e. pain management, aloe vera or soothing lotions); these burns are typically self-limiting, do not scar and will heal without intervention.
- Second Degree Burns (partial thickness)
- Superficial Partial Thickness
-
- Involves the epidermis and papillary dermis
- Skin appearance: blistering, red or pink, moist, blanches with pressure
- Extremely painful
- Management: will usually heal with local wound care; low potential for scarring
-
- Deep Partial Thickness
-
- Involves epidermis, papillary dermis and reticular dermis
- Skin appearance: blistered, waxy, variable in color from red/pink to white, non-blanching
- Less painful
- Management: few smaller burns will heal with good wound care but most will require surgical excision and grafting; high risk for scarring and pigment changes
-
- Superficial Partial Thickness
- Third Degree Burn (full thickness)
- Penetration through epidermis/dermis and into subcutaneous tissues
- Skin appearance: dry, inelastic, waxy or leathery, non-blanching, white/yellow/brown in color with eschar.
- Insensate, not painful
- Management: will not heal without intervention, often requires surgical excision and grafting; high risk for scarring and contractures
- Fourth Degree Burn
- Extends down into the muscle, tendon, or bone
- Skin appearance: charred, black, skeletonized
- Insensate
- Management: will not heal without intervention; often requires surgery/amputation.
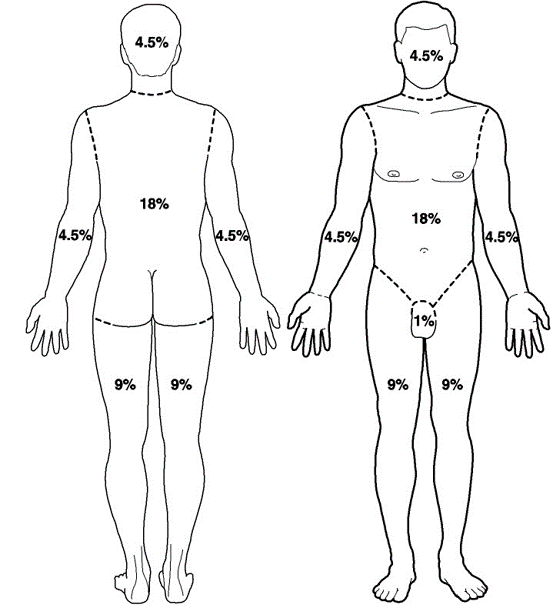
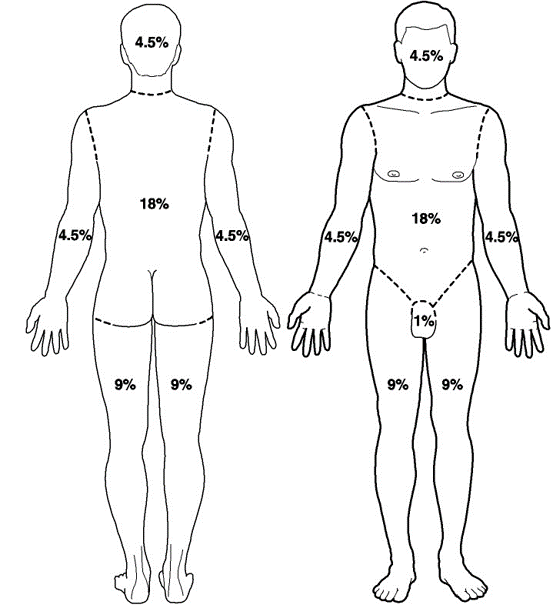
Extent of Burn Injuries
- Accurate determination of burn size ensures proper treatment and resuscitation
- The total body surface area (TBSA) of burns in adults can be estimated using the “Rule of Nines” or by using the patient’s open palm to equal approximately 1% TBSA.
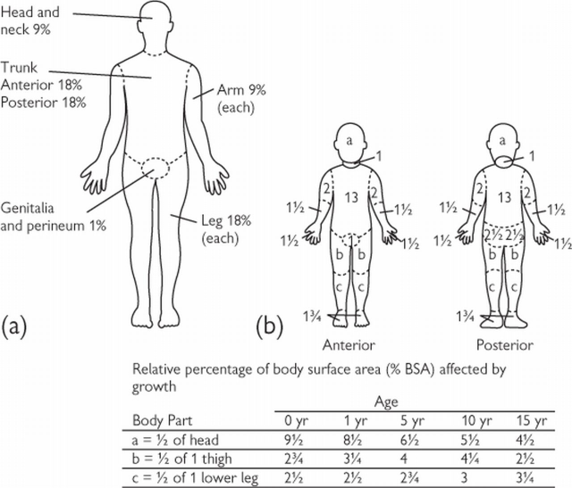
 \
\ - Since body proportions in children differ with age, TBSA in children should be estimated using a Lund-Browder chart (see below) or by using the patient’s open palm to equal approximately 1% TBSA.
Burn Resuscitation
- The initial approach to a burn resuscitation is similar to standard ATLS
- Please see Special Considerations regarding Inhalational Injury and Escharotomies
- Volume Resuscitation is based upon the % TBSA, age, and weight of the patient
-
- TBSA > 20% require formal resuscitation in all ages
- TBSA > 10% require resuscitation in children and elderly patients
-
- American Burn Association Consensus Formula
-
- 2-4 ml/kg/% TBSA (using LR) in the first 24 hours
- Give 1/2 in the first 8 hours
- Give 1/2 in the subsequent 16 hours
-
- Adults: 2 mL/kg/% TBSA
- Children: 3 mL/kg/% TBSA
-
- Adjust fluid rate for goal urine output 1 cc/kg/hr if child < 14 yr
- If child is < 30 kg, add maintenance fluids that include dextrose (D5LR or D5 1/2 NS) in addition to the consensus formula
-
- Electrical: 4 mL/kg/% TBSA
- Initial Wound Care
-
- Wrap wounds with clean, dry gauze, wrapped in Kerlix
-
- Please note that any dressings or wound care performed will be quickly removed upon transfer to the referring hospital
-
- Wrap wounds with clean, dry gauze, wrapped in Kerlix
-
- Other caveats
-
- Pain Control
- Clarify time of burn and crystalloid received prior to arrival into calculations for initial burn resuscitation
- Update Tetanus
- Consider Cyanokit with appropriate mechanism/circumstances of burn and/or markedly high lactic acidosis
-
Special Considerations
- Inhalational Injury
-
- Significantly increases morbidity and mortality of burn patients
- Present in approximately 1/3 of burn patients
- Injury due to 1. direct injury, 2. edema leading to airway obstruction, and 3. massive inflammatory response
- Diagnosis is subjective and objective
-
- History: mechanism, duration of exposure, location
- Exam: facial burns, singed facial/nasal hair, carbonaceous sputum, soot in oropharynx, voice hoarseness, stridor, erythema and/or edema of the oropharynx
- Work-up: carboxyhemoglobin, chest x-ray, ABG, oxygen saturations
- Flexible bronchoscopy is the gold standard for diagnosis.
-
- Treatment
-
- Supplemental oxygen and pulmonary toilet
- Need for intubation/mechanical ventilation at discretion of the Trauma and ED providers
- Adjuncts: beta-agonists, nebulized acetylcysteine (NAC) and/or heparin, nebulized racemic epinephrine
-
-
- Electrical Burns
-
- Arc burn
-
- Generated by heat from an electrical arc
- Similar treatment to thermal burns
-
- Current burn
-
- Electrical current passes through the body
- Entrance and exit marks are common, as is history of tetany
- Risk for compartment syndrome; evaluation of compartments in an obtunded patient should be performed
-
- Arc burn
-
- Chemical Burn
-
- Identify the chemical, mechanism of exposure, and duration of exposure
- Remove contaminated clothing and follow decontamination protocol per hospital/facility policy
- Affected areas should be copiously irrigated with water
-
- Do not attempt to neutralize the solution as this can result in heat production and worsen injury
-
-
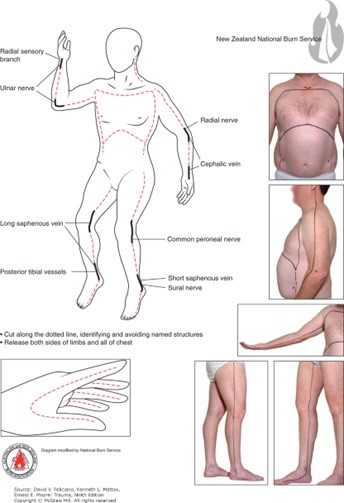
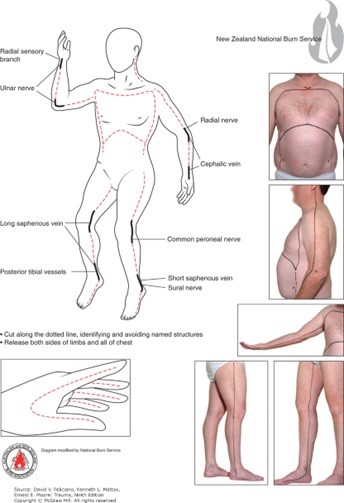
- Escharotomy
-
- Surgical division of nonviable eschar is sometimes required in deep partial and full thickness burns
- The inelastic tissue of the eschar can cause a tourniquet effect over inflamed extremities/compartments and body cavities
- Most commonly performed in extremities with circumferential deep partial or full thickness burns; but may also be required in the neck (airway compromise), chest (diminished chest wall compliance resulting in inadequate ventilation/oxygenation) and abdomen (abdominal compartment syndrome)
- Procedure:
- division through the epidermal and dermal layers (eschar) into the subcutaneous fat following the LAID pneumonic (Longitudinal incisions, axial planes, into normal skin, down into subcutaneous fat)
- usually performed at bedside with sterile drapping
- utilize electrocautery device
- have adequate analgesia and sedation available
-
- Non-Accidental Trauma
-
- Burns in children can be the result of child abuse or neglect
- Maintain a high index of suspicion for burns presenting with inconsistent stories for how burn occurred or those presenting in "stocking patterns" suggestive for water immersion burns that are uniform in nature and have a well demarcated line indicated depth of immersion
-
Burn Referral Criteria
- A burn center may treat adults, children, or both. Burn injuries that should be referred to a burn center include the following:
-
- Partial-thickness burns of > 10 % of the TBSA.
- Burns that involve the face, hands, feet, genitalia, perineum, or major joints.
- Third-degree burns in any age group.
- Electrical burns, including lightning injury.
- Chemical burns.
- Inhalation injury.
- Burn injury in patients with preexisting medical disorders that could complicate management, prolong recovery, or affect mortality.
- Burns and concomitant trauma (such as fractures) when the burn injury poses the greatest risk of morbidity or mortality. If the trauma poses the greater immediate risk, the patient’s condition may be stabilized initially in a trauma center before transfer to a burn center. Physician judgment will be necessary in such situations and should be in concert with the regional medical control plan and triage protocols.
- Burns in children; children with burns should be transferred to a burn center verified to treat children. In the absence of a regional pediatric burn center, an adult burn center may serve as a second option for the management of pediatric burns.
- Burn injury in patients who will require special social, emotional, or rehabilitative intervention.
- Trauma Surgeon Discretion
-
Regional Burn Centers Contact Information
- Isolated Burn
- St. Elizabeth’s Burn Center, Lincoln, NE
-
- Transfer Line 1st: (800) 877-2876
- Burn RN Station: (402) 219-7680
- Fax: (402) 219-8773
- Outpatient Burn Clinic: (402) 219-8770
-
- St. Elizabeth’s Burn Center, Lincoln, NE
- Burn with Traumatic Injuries
-
- University of Kansas (KU) Medical Center, Kansas City, KS: 1-877-738-7286
- University of Iowa Medical Center, Iowa City, IA: 1-866-890-5969
-
Note: Requests for photographic evidence of burns sent over SMS/Text are not HIPAA protected and therefore not permitted
Contributors
Last Updated: Feb 14, 2023
References:
1. Levi, Benjamin; Vercruysse, Gary. 2021. Chapter 51: Burns and Radiation. Trauma, 9e. Feliciano DV, Mattox KL, Moore EE. McGraw Hill.
2. Resources for Optimal Care of the Injured Patient. Guidelines for Trauma Centers Caring for Burn Patients. American College of Surgeons, Committee on Trauma, Chicago, Ill. 2014
3. Chapter 9: Thermal Injuries. Advanced Trauma Life Support (ATLS®): The Tenth Edition. 2018. ATLS Subcommittee. American College of Surgeons’ Committee on Trauma; International ATLS working group. Chicago, IL. American College of Surgeons