Management of Blunt Cerebrovascular Injuries (BCVI)
Management of Blunt Extra – Cranial Carotid and Vertebral Artery Injury in Adults (BCVI)
PURPOSE:
To define guidelines in caring for the trauma patient with diagnosis of blunt extra – cranial carotid and vertebral artery injuries (BCVI)
GUIDELINE:
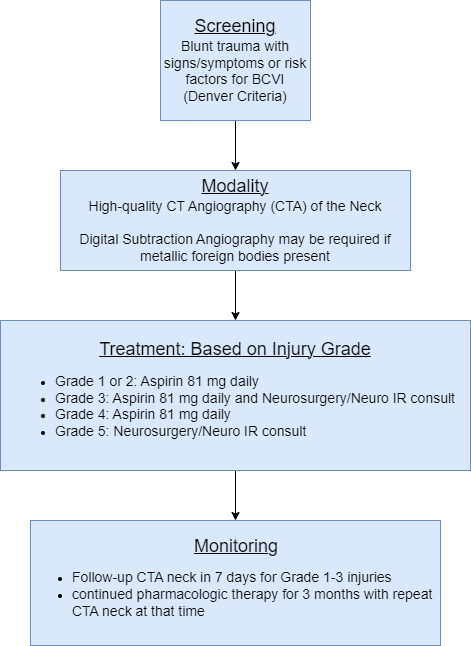
Screening (Denver Criteria)
Signs/Symptoms
· Potential arterial hemorrhage from neck/nose/mouth
· Cervical bruit (<50 years old)
· Expanding cervical hematoma
· Focal neurologic defect: TIA, hemiparesis, vertebrobasilar symptoms, Horner’s syndrome
· Neurologic deficit inconsistent with head CT
· Stroke on CT or MRI
Risk Factors for BCVI
· High-energy transfer mechanism
· Displaced midface fracture (Lefort II or III)
· Mandible Fracture
· Complex skull fracture/basilar skull fracture/occipital condyle fracture
· Severe TBI with GCS <6
· Cervical spine fracture, subluxation, or ligamentous injury at any level
· Near hanging with anoxic brain injury
· Clothesline type injury or seat belt abrasion with significant swelling, pain, or altered mental status
· TBI with thoracic injuries
· Scalp degloving
· Thoracic vascular injuries
· Blunt cardiac rupture
· Upper rib fracture
Screening Modality
High quality CT Angiography of the neck is an acceptable modality.
Digital subtraction 4-vessel angiography may be required if metallic foreign bodies prevent adequate visualization on CTA
Duplex Ultrasound is not adequate for screening for BCVI.
*** If CTA is ordered to screen for BCVI, a TEG needs to be drawn***
Grading Scale
Grade 1 – Intimal irregularity with < 25% narrowing.
Grade 2 – Dissection or intramural hematoma with > 25% narrowing
Grade 3 – Pseudoaneurysm
Grade 4 – Occlusion
Grade 5 – Transection with extravasation
Treatment
Patients with extracranial carotid and vertebral artery injuries should be treated as outlined below unless: Arterial transection with active hemorrhage is present and/or risk of bleeding from other traumatic injuries prohibits the use of anticoagulation.
Recommendation based on injury grade
Grade 1 and 2
· 81 mg Aspirin
Grade 3
· 81 mg Aspirin
· Neurosurgeon and/or Neuro Interventionalist consultation
· Unlikely to resolve spontaneously with antithrombotic therapy alone. Close follow-up needed.
· Stenting should be avoided due to increased risk for stent thrombosis.
Grade 4
· 81 mg Aspirin
· Neurosurgeon and/or Neuro Interventionalist consultation
· Goal to prevent propagation of thrombus
Grade 5
· Neurosurgeon and/or Neuro Interventionalist consultation
· Endovascular intervention depending on clinical picture:
-
-
-
- Cerebral ischemic events despite the use of anticoagulation or antiplatelet therapy.
- Progressing luminal stenosis despite adequate antithrombotic therapy
- Clinical or radiographic evidence of cerebral perfusion failure due to inadequate collateral blood flow.
- Vertebral artery pseudoaneurysms, as they can rupture into the spinal canal producing epidural and subarachnoid hemorrhage
- Carotid pseudoaneurysms do not require urgent endovascular therapy, as they pose no significant risk of bleeding.
-
-
***Should results of TEG reveal a hypercoagulable state in the setting of BCVI (MA >63 or angle > 77), strong consideration for early initiation of antithrombotic therapy should be made despite competing risk factors due to increased risk for CVA***
Monitoring
· Repeat CTA at 7-days post injury for injury grades 1-3 to assess for resolution of injury and monitor for any progression of luminal stenosis despite antithrombotic therapy, which may benefit from endovascular intervention
· Continued aspirin for 3 months
· CTA is recommended at 3 months to determine the status of the BCVI and the need for further medical or endovascular therapy.
APPROVAL:
Reviewer: Division of Acute Care Surgery, University of Nebraska Medical Center
Approval Date: 1/12/2022
References:
- Cogbill TH, Moore EE, Meissner M, et al. The spectrum of blunt injury to the carotid artery: a multicenter perspective. J Trauma. 1994;37(3):473-479. doi:10.1097/00005373-199409000-00024
- Biffl WL, Moore EE, Ryu RK, et al. The unrecognized epidemic of blunt carotid arterial injuries: early diagnosis improves neurologic outcome. Ann Surg. 1998;228(4):462-470. doi:10.1097/00000658-199810000-00003
- Mutze S, Rademacher G, Matthes G, Hosten N, Stengel D. Blunt cerebrovascular injury in patients with blunt multiple trauma: diagnostic accuracy of duplex Doppler US and early CT angiography. Radiology. 2005;237(3):884-892. doi:10.1148/radiol.2373042189
- Miller PR, Fabian TC, Croce MA, et al. Prospective screening for blunt cerebrovascular injuries: analysis of diagnostic modalities and outcomes. Ann Surg. 2002;236(3):386-395. doi:10.1097/01.SLA.0000027174.01008.
- Burlew CC, Sumislawski JJ, Behnfield CD, et al. Time to stroke: A Western Trauma Association multicenter study of blunt cerebrovascular injuries. J Trauma Acute Care Surg. 2018;85(5):858-866. doi:10.1097/TA.0000000000001989
- Biffl WL, Moore EE, Offner PJ, Brega KE, Franciose RJ, Burch JM. Blunt carotid arterial injuries: implications of a new grading scale. J Trauma. 1999;47(5):845-853. doi:10.1097/00005373-199911000-00004
- Russo RM, Davidson AJ, Alam HB, et al. Blunt cerebrovascular injuries: Outcomes from the American Association for the Surgery of Trauma PROspective Observational Vascular Injury Treatment (PROOVIT) multicenter registry. J Trauma Acute Care Surg. 2021;90(6):987-995. doi:10.1097/TA.0000000000003127
- Bromberg WJ, Collier BC, Diebel LN, et al. Blunt cerebrovascular injury practice management guidelines: the Eastern Association for the Surgery of Trauma. J Trauma. 2010;68(2):471-477. doi:10.1097/TA.0b013e3181cb43da
- Kim DY, Biffl W, Bokhari F, et al. Evaluation and management of blunt cerebrovascular injury: A practice management guideline from the Eastern Association for the Surgery of Trauma [published correction appears in J Trauma Acute Care Surg. 2020 Aug;89(2):420]. J Trauma Acute Care Surg. 2020;88(6):875-887. doi:10.1097/TA.0000000000002668
- Biffl WL, Moore EE, Offner PJ, et al. Optimizing screening for blunt cerebrovascular injuries. Am J Surg. 1999;178(6):517-522. doi:10.1016/s0002-9610(99)00245-7
- Sumislawski JJ, Moore HB, Moore EE, Swope ML, Pieracci FM, Fox CJ, Campion EM, Lawless RA, Platnick KB, Sauaia A, Cohen MJ, Burlew CC. Not all in your head (and neck): Stroke after blunt cerebrovascular injury is associated with systemic hypercoagulability. J Trauma Acute Care Surg. 2019 Nov;87(5):1082-1087. doi: 10.1097/TA.0000000000002443. PMID: 31453984.