Management of the Pregnant Trauma Patient
Purpose
Purpose:
Pregnancy alters baseline physiology and anatomy. These changes can influence the evaluation of a traumatically injured pregnant patient. The signs and symptoms of injury can be confusing. The pregnant patient has abnormal baseline laboratory values. There are special considerations in the approach and response to resuscitation. While there are two patients--patients – mother and fetus--fetus, the initial treatment priorities are the same, focusing on the optimal treatment of the mother. To provide safe care to the pregnatpregnant trauma patient, a collaborative effort between Emergency Medicine, the Trauma Service,Service and the Department of Maternal Fetal Medicine should occur.
Policy StatementStatement:
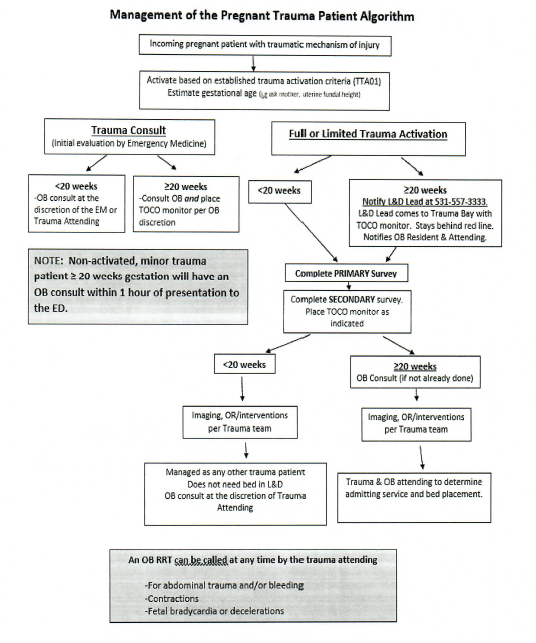
This guideline is a supplement to and is to be used in conjunction with the policy Trauma Team Activations (TTA01).
Non-trauma activated/minor trauma patients > 20 weeks seen in the Emergency Department (ED) by Emergency Medicine should have an OB consult within 1 hour of presentation to the ED even for minor trauma.
All pregnant trauma patients will be evaluated in an organized fashion whether they be evaluated in the ED, on the floor, or in Labor and Delivery. Obstetrics, including Maternal Fetal Medicine, is available to consult on any pregnant patient <20 weeks at any time to discuss medication risks or risk of surgery in pregnancy. Additionally, if a pregnant trauma patient at any gestational age cannot be bedded on the trauma floor, contact Labor and Delivery.

References
-
1. American College of Surgeons Committee on Trauma. (2025). ATLS, Advanced Trauma Life
Support,Support:10thStudentEd.Course2018.Manual. 11th ed. American College of Surgeons.
Author(s)
- Acute Care Surgery/Trauma Leadership
- Emergency Medicine Leadership
- Maternal Fetal Medicine Division Leadership
Last Updated
February, 20202026