Mental Health Screening and Intervention Guidelines for Pediatric Trauma Patients at Nebraska Medicine
Childhood traumatic stress happens when unexpected, violent, life-threatening, or devastating events overwhelm the ability to cope. The ACS reports that 20-30% of pediatric trauma patients report mental health symptoms and/or decreased quality of life following a traumatic event.
The purpose of this guideline is to identify pediatric trauma patients at high risk for post-trauma mental health adjustment disorder post-injury and facilitate brief interventions and appropriate referrals for longer term management and care.
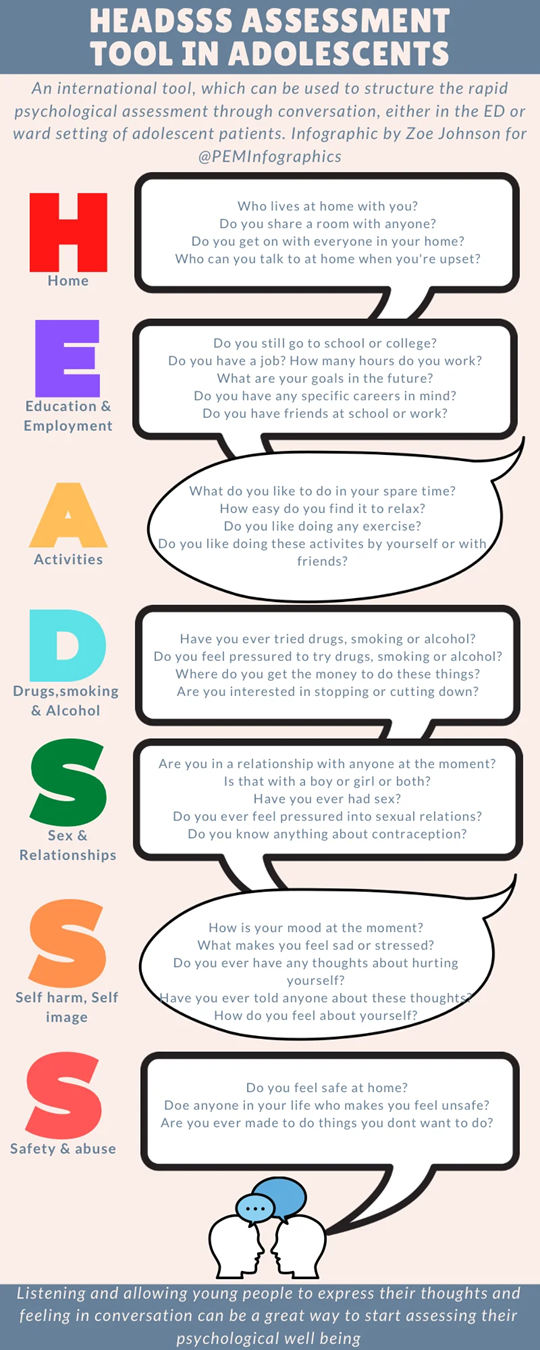
1. A HEADSS assessment will be performed on all admitted pediatric trauma patients age 11 years and older by the pediatric co-management team once the patient reaches floor status.
2. Patients with a positive HEADSS assessment in the mental health categories AND/OR any pediatric patient experiencing the following traumatic events:
a. Neglect and psychological, physical, or sexual abuse.
b. Victim of community and school violence.
c. Victim of gun-related violence (intentional self-inflicted GSW or suicidal attempt will prompt child psychiatry consult)
d. Serious traumatic event causing life-threatening and devastating injuries (traumatic brain injury, spinal cord injury, loss of limb, mutilating/deforming injuries, etc)
e. Prolonged hospital stay (longer than 1 week)
f. Death of family member in traumatic event
g. Care provider discretion.
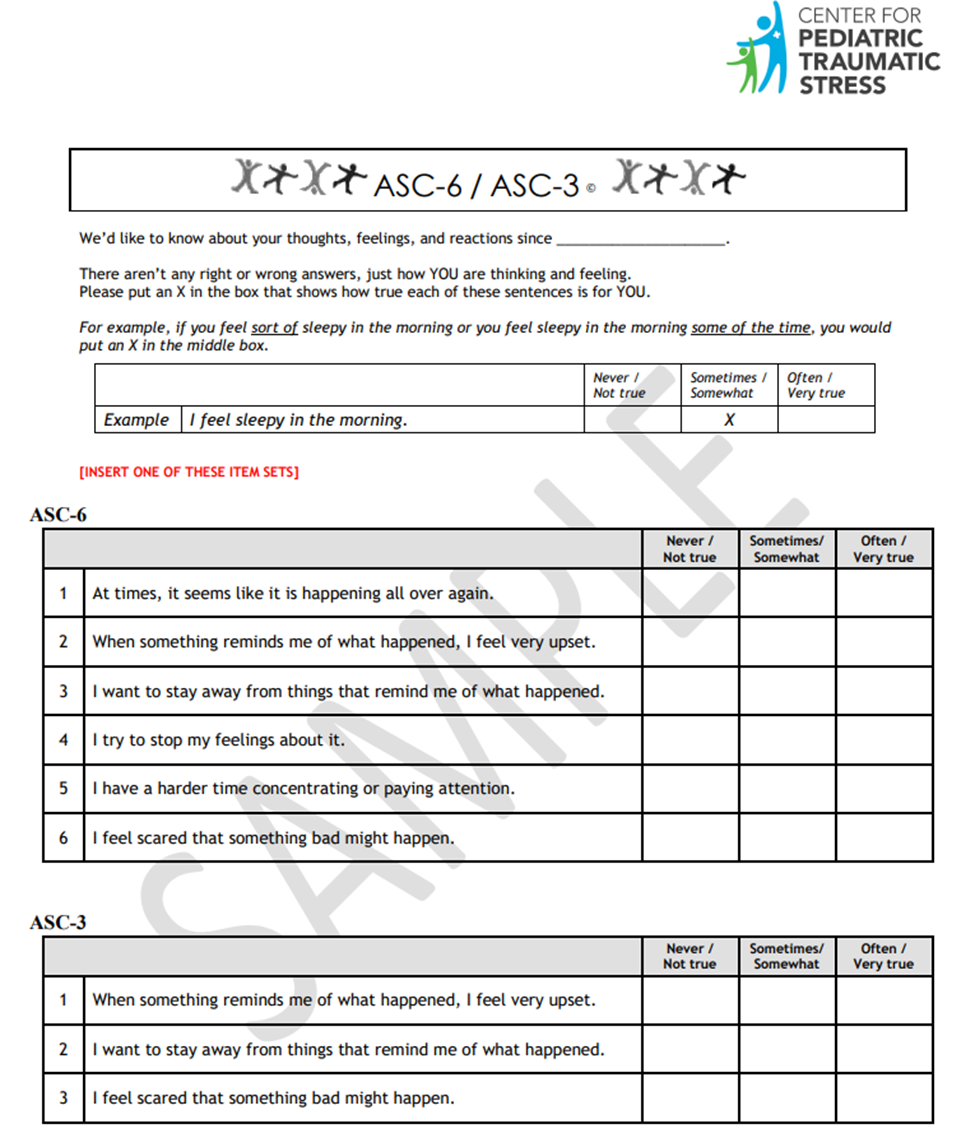
These patients are identified as high risk for post-injury mental health disorder(s) will undergo additional screening using the ASC6/ASC3 screening tool derived from the Acute Stress Checklist (ASC-Kids).
3. Patients admitted following self-inflicted injury or suicide attempt as well as patients with suicidal or homicidal ideation will receive inpatient consultation with child psychiatry.
4. Patients who screen positive on the ASC6/ASC3 will receive one or more of the following intervention(s):
a. Consultation of child psychiatry for inpatient assessment of mental health concerns
b. Referral to child psychiatry or psychology for outpatient assessment and management of mental health concerns
c. Notification of primary pediatrician of mental health concerns for assistance in longer term follow-up and/or outpatient mental health referrals as indicated
5. For patients who do not screen positive but have experienced one of the above traumatic events, the patient’s primary pediatrician should be notified with the recommendation to perform a repeat assessment of the patient’s mental health in 4-6 weeks time.
Documentation
The HEADDS, ASC6/ASC3 assessment (if performed), and interventions provided will be documented in a progress note by the pediatric co-management teams in the patient’s electronic medical record when consulted. For those patients remaining in the ICU for entire hospital course, mental health screening will be performed as indicated by the trauma service.
References:
1. American College of Surgeons. (2022, December). Best Practices Guidelines: Screening and Intervention for mental health disorders and substance use and misuse. https://www.facs.org/media/nrcj31ku/mental-health-guidelines.pdf
2. The Acute Stress Checklist (ASC-kids) (2016), https://www.healthcaretoolbox.org/acute-stress-checklist