Nebraska Medicine Brain Death Criteria
Purpose
To give an accurate and complete description of all criteria required to establish a diagnosis of brain death, and to describe the roles and responsibilities of various clinicians and staff members in the process.
Scope
This Policy applies to all patients at Nebraska Medicine for whom a diagnosis of brain death is considered.
Background
Nebraska Medicine follows the definition of brain death in the statutes of the State of Nebraska: the complete and irreversible cessation of all functions of the brain, including the brain stem. A single evaluation demonstrating that all criteria is met is sufficient to establish a diagnosis of brain death in adults. A repeat evaluation is indicated if there is uncertainty about the irreversibility of findings on the initial exam. Special requirements apply to establish a diagnosis of brain death in an infant or child (see Special Circumstances below and Checklist Attachment B).
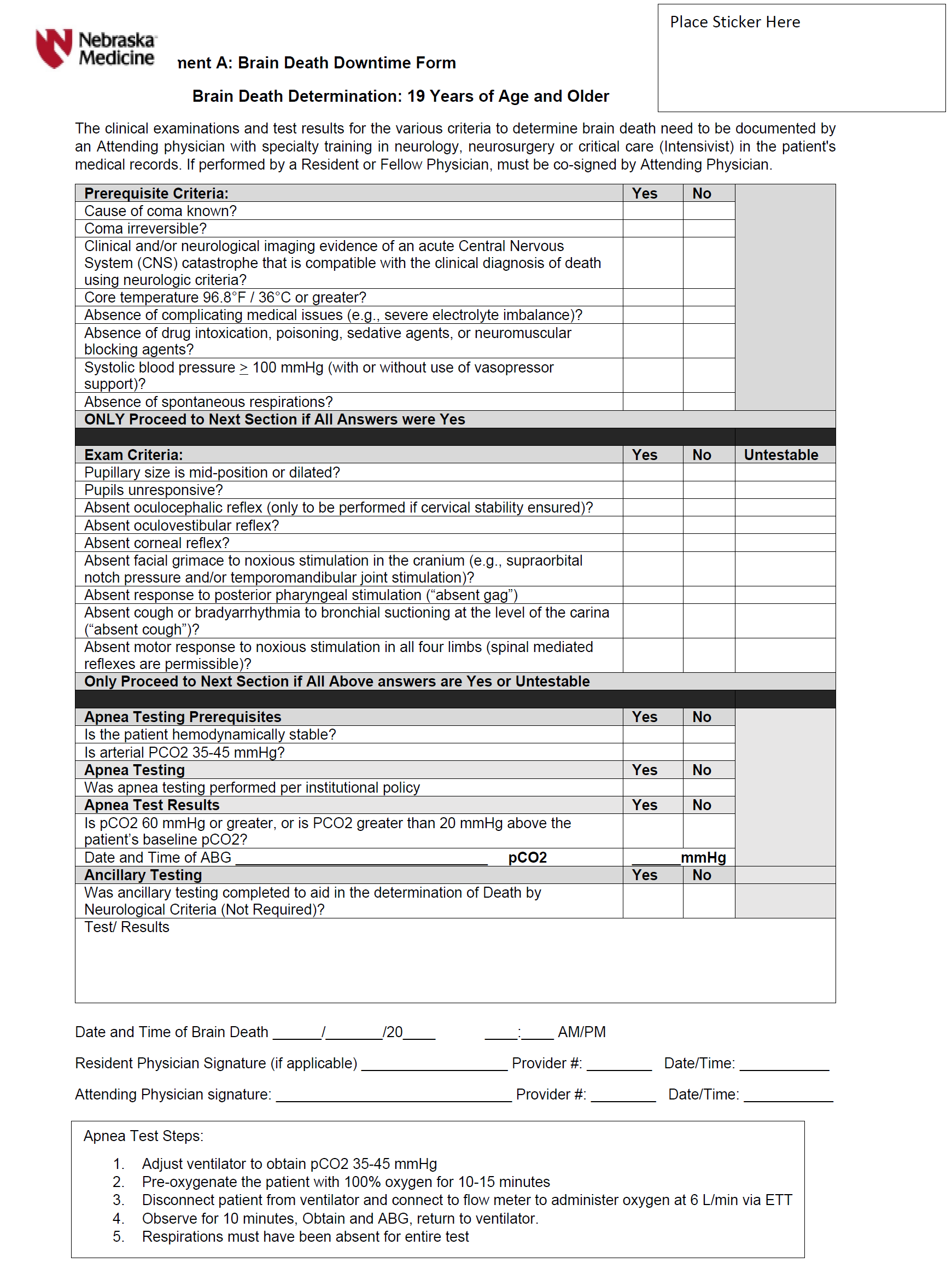
A diagnosis of brain death can only be established by a staff physician/surgeon with privileges in neurology, neurosurgery, or critical care (intensivist). The staff physician/surgeon will use the checklist that is an integral part of this policy (see Checklist Attachment A) to document the results of the brain death evaluation. The time of death is the time when a positive apnea test is documented, or at the time of a positive ancillary test result if the apnea test cannot be performed. Physicians or surgeons in training, who are at an advanced level of training deemed appropriate by the staff physician/surgeon and working under the staff physician's/surgeon's supervision can perform parts of the examination. The staff physician/surgeon is fully responsible for the diagnosis, declaration, and documentation of brain death.
Brain Death Evaluation
A complete brain death evaluation consists of three components. All three components must be completed to establish a diagnosis of brain death:
- Establish irreversible and proximate cause of coma (see Checklist Attachment A and Checklist Attachment B).
-
- The proximate cause of coma can usually be established by history and additional clinical data.
- Exclude the presence of any factures that can depress CNS function and/or interfere with neurologic examination, including hypothermia (temperature <36 degrees Celsisus), hypotension (systolic BP less than 100 mmHg), presence of drugs or medications that can affect CNS function (including but not limited to alcohol, sedatives, barbiturates, or neuromuscular blockers), and severe electrolyte, acid-base, or endocrine abnormalities.
-
- Establish absence of cortical function and brain stem reflexes by neurologic examination (see Checklist Attachment A and Checklist Attachment B).
-
- Absence of cortical function requires documentation of unresponsiveness to painful stimuli, and absence of spontaneous voluntary movements or seizures.
- Absence of brain stem reflexes requires documentation of absence of pupillary reflex, absence of corneal reflex, absence of gag/cough reflex, and absence of ocular movements in response to oculocephalic testing and oculovestibular reflex testing.
-
- Establish absence of spontaneous respirations by performing an apnea test (see Checklist Attachment A and Checklist Attachment B).
- Completion of the three components of the brain death evaluation is sufficient to establish a diagnosis of brain death.
- Ancillary tests may be used to support the diagnosis of brain death when uncertainty exists about the reliability of parts of the neurologic exam or when an apnea test cannot be performed. Cerebral angiography, cerebral scintigraphy, and electroencephalography are the ancillary tests most widely available. The interpretation of these tests requires special expertise and must be performed by a staff physician with the required level of expertise.
- Ancillary tests should not be ordered in any patient who does not meet any one of the clinical criteria for brain death outlined above (1-3). Please complete Checklist Attachment A or Checklist Attachment B when completing the evaluation.
Roles and Responsibilities
- Staff nurse will notify the local organ procurement organization of imminent death if applicable, per policy TX02.
- Staff nurse will notify Acute Bereavement Services of all imminent death or severe brain injury patients in accordance with policy TX02. This includes patients for whom brain death evaluation is scheduled or initiated.
- Neurologist, neurosurgeon, or intensivist reviews and interprets exam and test results, completes brain death evaluation documentation using electronic documentation of Checklist Attachment A or B, (in the event of electronic downtime, paper copies of Attachment A or B may be filled out), establishes brain death, completes the death certificate, and communicates findings and brain death with the family of the deceased.
- Local procurement organization representative approaches family about option of organ donation, obtains consent for organ procurement, confirms that checklist for brain death evaluation has been completed and signed by a staff neurologist, neurosurgeon, or intensivist.
Special Circumstances
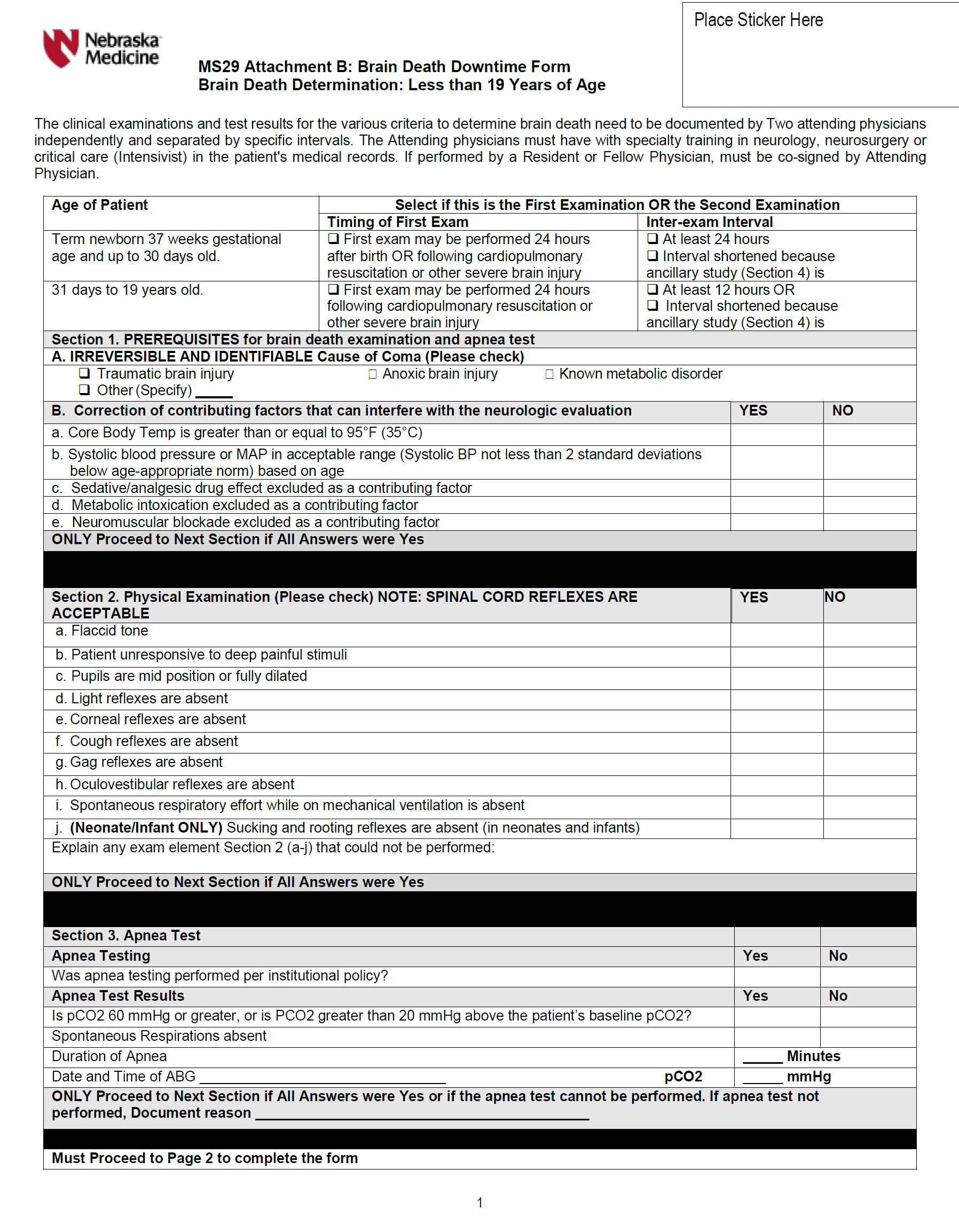
- Infants and children (i.e., term newborns and children up to 19 years of age) require a waiting period of 24 hours before an initial brain death examination is performed following a cardiopulmonary resuscitation or severe acute brain injury. Please complete Checklist Attachment B electronically (unless in a downtime situation) when completing the evaluation. Two brain death examinations, separated by an age-dependent observation period are required as outlined below. Apnea testing is required for each examination.
-
- Term newborns (37 weeks gestation or more) to 30 days of age: it is recommended that two examinations be performed at least 24 hours apart.
- 31 days to 19 years of age: it is recommended that two examinations be performed at least 12 hours apart.
-
- In pediatric cases, the clinical examinations should be carried out by experienced clinicians who are familiar with infants and children and have specific training in neurocritical care. It is recommended that these clinicians be pediatric neurologists, neurosurgeons, or critical care clinicians with training in neurocritical care. The guidelines for brain death determination in infants and children recommend that one qualified physician perform the first brain death exam and a second qualified physician perform the second brain death exam. However, the attending physician who is managing the ventilator of the child may perform both apnea tests.
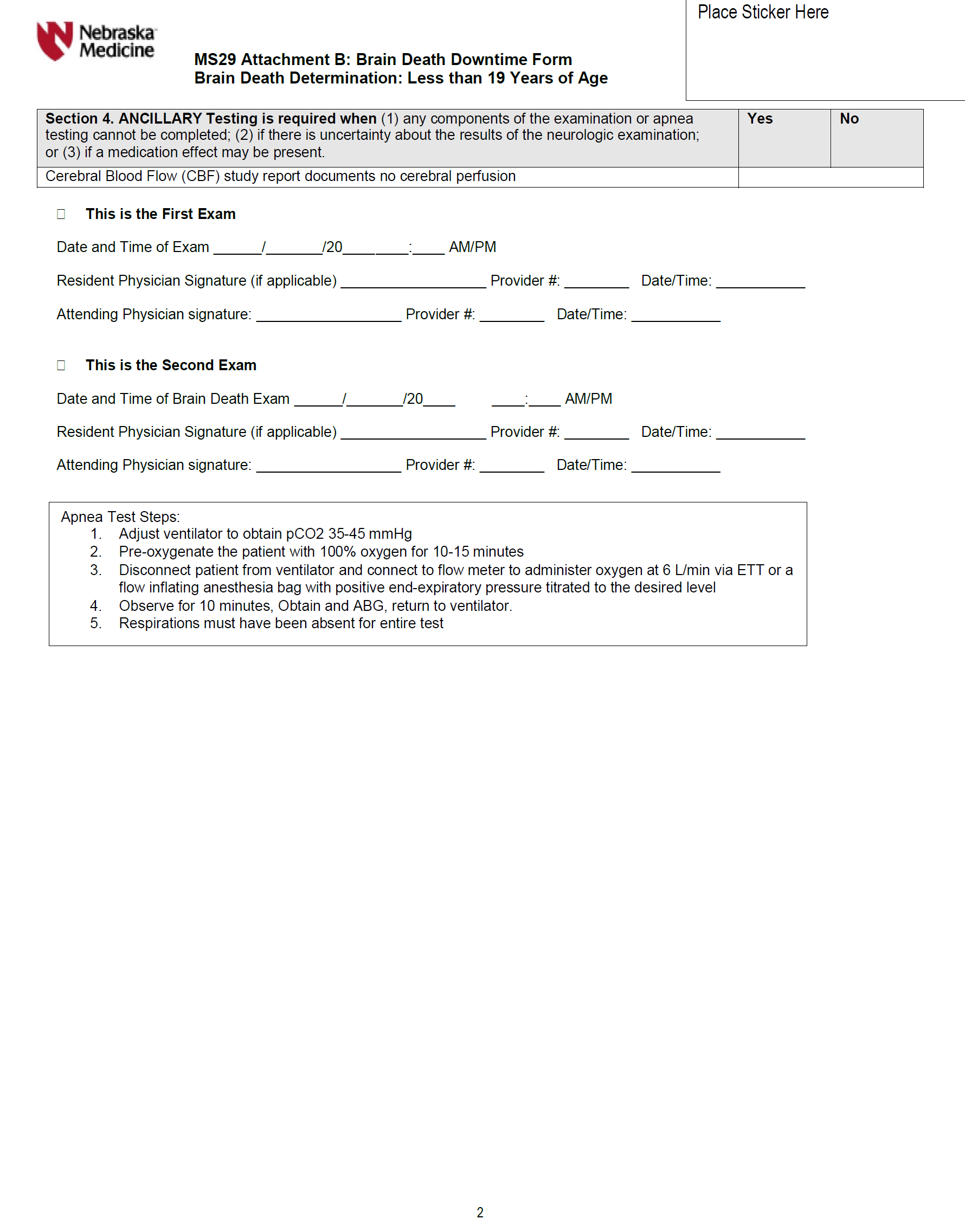
- In pediatric cases, ancillary tests are not required unless there is uncertainty about the results of the neurological examination, or the apnea test cannot be completed. The choice of ancillary test may be influenced by the age of the patient. Specifically, in term newborns (37 weeks gestation ro more) to 30 days of age, the EEG and cerebral blood flow (CBF) study may be less accurate, but the CBF may be preferred. From 31 days of age to 18 years of age, either test can be used. The observation period between brain death exams may be reduced for both age groups if the ancillary test is consistent with brain death. In this setting, the second clinical exam and apnea test can be performed after the results of the ancillary tests are available.
- Physicians with recognized or potential conflicts of interest in relation to the outcome of the patient's care must remove themselves from the determination of brain death. For instance, a transplant service whose patient expires and has the potential for organ donation should excuse himself/herself from declaring the patient brain dead.
References
- Evidence based guideline update: Determining brain death in adults. Neurology 2010;74;1911-1918. Wijdicks EF, Veralas PN, Gronseth GS, Greer DM. This update is supported by the American Academy of Neurology.
- Guidelines for determination of brain death infants and children: An update of the 1987 taskforce recommendations. Pediatric 2011:128(3):e720-e740. This report was developed and is supported by the Society of Critical Care Medicine, American Academy of Pediatrics and Child Neurology Society.
- For practical purposes, Nebraska Medicine uses the American Academy of Neurology Practical Guidance for Determination of Brain Death criteria (Wijdicks EFM et al. Neurology 2010;74:1911-1918).
Related Policies and Procedures
Acute Bereavement Care -- TX02
Reviewed by
- Neurology/Neurosurgery/Critical Care Medicine (12/2021)
- Medical Ethics Committee (12/2021)
- Pediatric Quality Committee (12/2021)
- Bylaws Committee (12/2021)
- Medical Executive Committee (12/2021)
- Board of Directors (12/2021)
Attachment A
Attachment B