Trauma Team Activations (TTA) Criteria
Purpose
Provide guidelines for trauma team activations in order to facilitate care of the critical or seriously injured patient to promote optimal outcomes.
Procedure
Dispatch will provide the following information over the paging system for FULL or LIMITED activations as instructed by the ED lead/charge nurse, trauma surgeon or designee.
Trauma activation level (full or limited)Mechanism of injuryAgeVital signsLoss of consciousnessEstimated time of arrival (ETA)
Trauma team to be activated for any of the following regardless of mode of arrival. 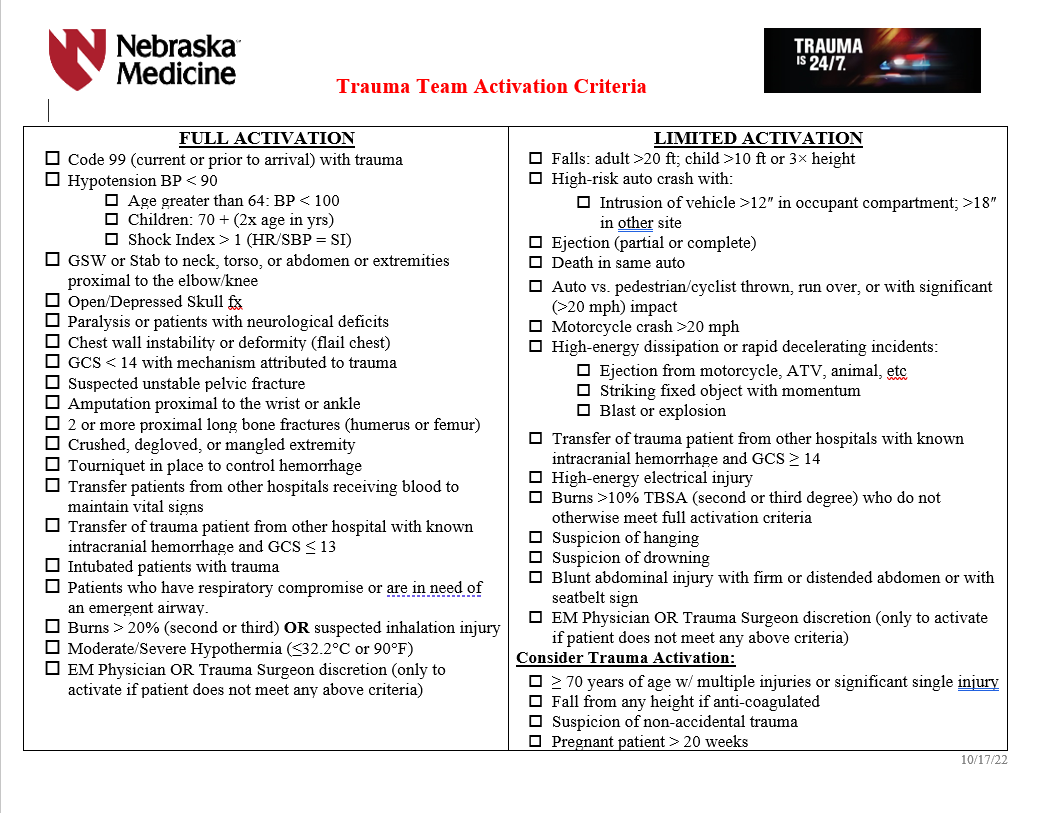
FULL Trauma Team Activation
These patients are critically ill. The trauma team, including the trauma attending, are expected to arrive prior to patient arrival or within 15 minutes of patient arrival.
CPR in progress or CPR at scene and/or en route with return of vital signs with any traumatic mechanism of injuryConfirmed hypotension (BP less than 90 mmHg) at any time except in geriatrics and children (parameters listed below)SBP less than 100 in patients >64 years of ageAge specific hypotension in children (SBP less than 70 mmHg + 2x age in years)Consider if shock index >1 (shock index = HR/SBP)
Gunshot or stab wound to the neck, torso, abdomen, or extremities proximal to the elbow/kneeTransfer of trauma patients from other hospitals receiving blood to maintain vital signs.Transfer of trauma patient from other hospitals with known intracranial hemorrhage and Glasgow Coma Scale (GCS) less than 14Intubated patients transferred from the sceneTrauma patients who have respiratory compromise or are in need of an emergent airway. This includes intubated patients who are transferred from another facility with ongoing respiratory compromise (does not include patients intubated at another facility who are now stable from a respiratory standpoint.)Open or depressed skull fractureParalysis or patients with neurological deficitsChest wall instability or deformity (flail chest)GCS less than 14 with mechanism attributed to traumaSuspected unstable pelvic fracturesAmputation proximal to the wrist or ankleTwo or more proximal long bone fractures (humerus or femur)Crushed, degloved, or mangled extremityTourniquet in place to control hemorrhageBurns greater than 20% TBSA (2nd and 3rd degree burns) or suspected inhalational injuryModerate to severe hypothermia (less than or equal to 32 deg Celsius or 90 deg Fahrenheit)Emergency medicine or trauma attending discretion
Full trauma team includes:
- Trauma attending
- Emergency medicine (EM) attending and resident
- PGY 4 or 5 surgical resident when available in house
- Junior surgical or EM residents on trauma service
- Trauma advanced practice providers (APP)
- Anesthesia resident (with immediate backup by anesthesia attending)
- Emergency department nurses and technicians
- Pharmacy
- Radiology technician
- Lab technician
- OR RN
- Blood bank (receives page to alert-do not respond in person)
- Spiritual care
- Respiratory therapy
LIMITED Trauma Team Activation
While these patients are stable, they have potential for becoming critically ill. These patients may be upgraded to a FULL activation at any time based on the professional judgement of the EM or Trauma attnending.
Falls: adult > 20ft; Child > 10ft or 2-3x heightHigh-risk auto crash with:Intrusion of vehicle >12" in occupant compartment; >18" in other siteEjection (partial or complete) from automobileDeath in same passenger compartment
Auto vs pedestrian/cyclist thrown, run over or with significant (>20mph) impactMotorcycle crash >20mphHigh-energy dissipation or rapid decelerating incidents, for example:Ejection from motorcycle, ATV, animal and so onStriking fixed object with momentumBlast or explosion
High-energy electrical injuryBurns >10% TBSA (2nd and 3rd degree) who do not otherwise meet full activation criteriaSuspicion of hangingSuspicion of drowningBlunt abdominal injury with firm or distended abdomen or with seatbelt sign
Limited trauma team includes:
- EM attending and resident
- General surgery resident(s)
- Trauma advanced practice provider(s) (APP)
- Emergency department nurses and technicians
- Pharmacy
- Radiology technician
- Lab technician
- OR RN (receives page to alert--do not respond in person)
- Spiritual care
- Respiratory therapy
- Trauma attending must respond if PGY4 or 5 surgical resident is not available and must evaluate the patient within 30 minutes of patient arrival.
- If the trauma attending is not in attendance, the EM attending has overall responsibility.
Once a full or limited activation has been called, these patients will be managed by the trauma service for subsequent care in the ED and radiology until admission or discharge from the ED.
If the trauma attending feels that the patient does not require trauma team activation, the activation may be discontinued after arrival.
Special Considerations for activation:
The EM attending should consider a limited activation or trauma consultation for the following patients:
Patient age greater than or equal to 70 years of age with significant single system injury or multiple injuresPregnant patient greater than 20 weeksSuspicion of non-accidental trauma (NAT)EM attending or trauma attending taking into account fall from any height if anticoagulated.
Trauma CONSULTATION
These patients do not meet trauma activation criteria, but merit the expertise of trauma surgeon consultation and/or evaluation, i.e. isolated/single system injuries. A trauma service resident or APP will evaluate these patients within 30 minutes of consult being called and disposition of the patient will be determined within 60 minutes. If the patient requires admission, the trauma attending will evaluate these patients within 8 hours of consult regardless of patient location.
The EM physician or admitted physician will consult the trauma team for any patient requiring admission to the hospital for any traumatic injury that does not meet trauma activation criteria. This will include but is not limited to the following patinets:
- Any patient with significant single system injury or multiple injuries
- Stable pelvic fractures (excludes isolated hip fractures)
- Stable chest injuries--rib fracture, sternal fracture, pneumothorax, seatbelt sign
- Minor brain injury (confirmed or suspected) with GCS 13-15
- Abdominal pain with significant mechanism of injury or seatbelt sign
- Spine fractures
- Pregnant patients who require admission to the OB floor for fetal monitoring
- Frostbite
- Any patient returning to the ED for care following treatment for a traumatic injury within the last 60 days
Patients who bypass the ED as a direct admit who are admitted for any injury meeting trauma criteria, will require a trauma consultation after notification of the admitting physician.