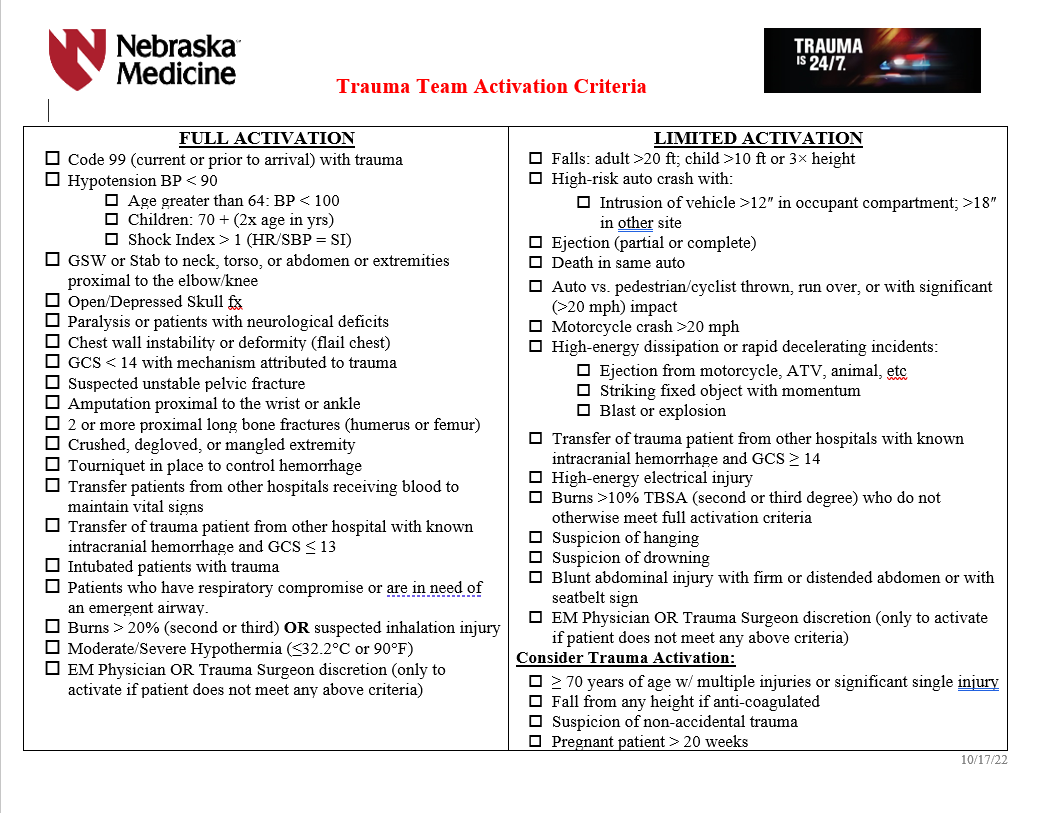
Trauma Team Activation (TTA) Criteria
FULL trauma team includes:
- Trauma attending
- Emergency medicine (EM) attending and resident
- PGY 4 or 5 surgical resident when available in house
- Junior surgical or EM residents on trauma service
- Trauma advanced practice providers (APP)
- Anesthesia resident (with immediate backup by anesthesia attending)
- Emergency department nurses and technicians
- Pharmacy
- Radiology technician
- Lab technician
- OR RN
- Blood bank (receives page to alert-do not respond in person)
- Spiritual care
- Respiratory therapy
LIMITED trauma team includes:
- EM attending and resident
- General surgery resident(s)
- Trauma advanced practice provider(s) (APP)
- Emergency department nurses and technicians
- Pharmacy
- Radiology technician
- Lab technician
- OR RN (receives page to alert--do not respond in person)
- Spiritual care
- Respiratory therapy
- Trauma attending must respond if PGY4 or 5 surgical resident is not available and must evaluate the patient within 30 minutes of patient arrival.
- If the trauma attending is not in attendance, the EM attending has overall responsibility.
Trauma CONSULTATION
These patients do not meet trauma activation criteria, but merit the expertise of trauma surgeon consultation and/or evaluation, i.e. isolated/single system injuries. A trauma service resident or APP will evaluate these patients within 30 minutes of consult being called and disposition of the patient will be determined within 60 minutes. If the patient requires admission, the trauma attending will evaluate these patients within 8 hours of consult regardless of patient location.
The EM physician or admitted physician will consult the trauma team for any patient requiring admission to the hospital for any traumatic injury that does not meet trauma activation criteria. This will include but is not limited to the following patinets:
- Any patient with significant single system injury or multiple injuries
- Stable pelvic fractures (excludes isolated hip fractures)
- Stable chest injuries--rib fracture, sternal fracture, pneumothorax, seatbelt sign
- Minor brain injury (confirmed or suspected) with GCS 13-15
- Abdominal pain with significant mechanism of injury or seatbelt sign
- Spine fractures
- Pregnant patients who require admission to the OB floor for fetal monitoring
- Frostbite
- Any patient returning to the ED for care following treatment for a traumatic injury within the last 60 days
Patients who bypass the ED as a direct admit who are admitted for any injury meeting trauma criteria, will require a trauma consultation after notification of the admitting physician.