Alcohol and Substance Misuse Screening, Brief Intervention and Referral for Treatment (SBIRT) Guidelines for Pediatric Trauma Patients at Nebraska Medicine
Policy and Procedure Statement
The pediatric co-management team will be consulted on all pediatric trauma patients (18 years and younger) admitted to Nebraska Medicine following injury.
As part of their role in the patient’s care, pediatric co-management will assist the trauma team in performing alcohol and substance misuse screening, brief intervention and treatment (SBIRT) as indicated on pediatric trauma patients age 11 years and older.
Screening:
- Pediatric trauma patients age 12 years and older will be routinely screened for alcohol and substance use on admission by laboratory screening using blood alcohol level and/or urine drug screen (UDS). Pediatric trauma patients less than 12 years of age will undergo laboratory screening as needed based on history or suspicion of alcohol or substance misuse.
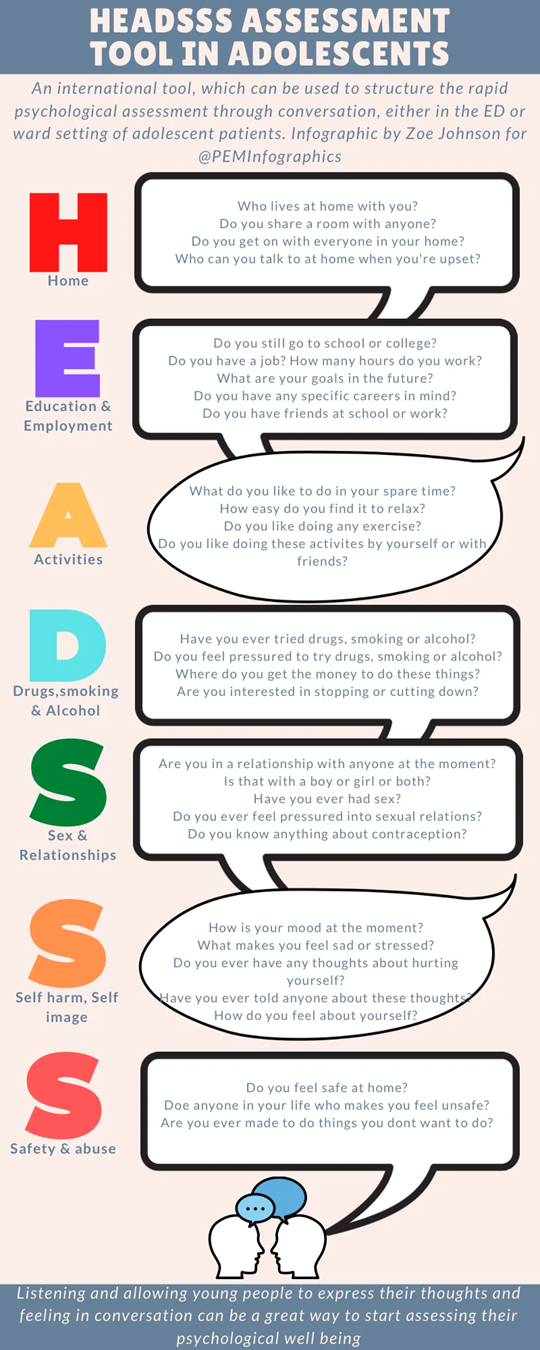
- A HEADSS assessment will be performed on all admitted pediatric trauma patients age 11 years and older by the pediatric co-management team once the patient reaches floor status.
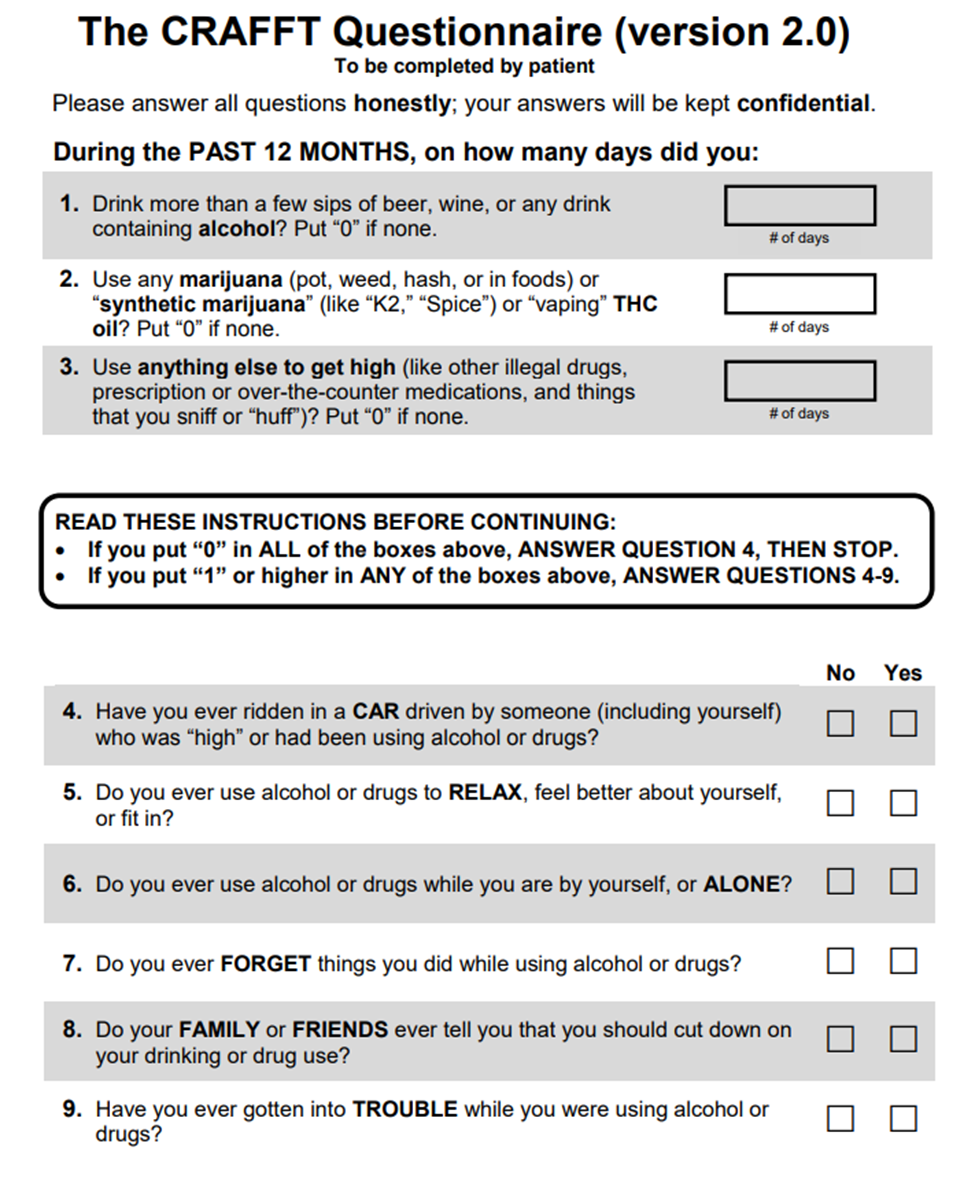
- If HEADSS assessment is positive for the questions pertaining to drug/alcohol use and exposure AND/OR if blood alcohol (ETOH) or urine drug screen (UDS) testing is positive on admission labs, a CRAFFT screening questionnaire will also be administered.
-
- If the patient is unable to be screened due to the medical condition or refuses, this will be documented in the medical record.
-
Intervention and Referral for Treatment:
- A CRAFFT score of 2 or higher indicates a positive screen. Patients with a positive screen will receive a brief intervention conducted and documented by the pediatric co-management provider, social worker or member of child psychiatry team with referrals for outpatient treatment as indicated.
-
- All pediatric patients who screen positive will receive a social work consult for information on area alcohol/substance misuse programs and assistance with referrals as indicated.
- Child psychiatry may be consulted at the discretion of the trauma or pediatric co-management providers for either inpatient or outpatient assessment of alcohol/substance misuse.
-
Documentation:
The HEADDS assessment, results of alcohol and urine drug screen and CRAFFT assessment (if performed) will be documented in a pediatric co-management team progress note in the patient’s electronic medical record when consulted. For those patients remaining in the ICU for entire hospital course, alcohol and substance misuse screening and interventions will be performed and documented as indicated by the trauma service.
Performance Improvement:
Per American College of Surgeons (ACS) Standards, a minimum of 80% of trauma patients with a hospital stay of >24 hours must be screened for alcohol misuse and a minimum of 80% of patients screening positive must receive an intervention.
Documentation of SBIRT will be done in the trauma registry database.
Any patients that had missed screenings or interventions will be reviewed in the trauma performance improvement process.
References:
- Cohen E, MacKenzie RG, Yates GL. HEADSS, psychosocial risk assessment instrument: Implications for designing effective intervention programs for runaway youth. J Adolesc Health (1991); 12(7):539-544.
- Katzenellenbogen R, HEADSS: The “Review of systems” for adolescents. Virtual Mentor (2005) Mar 1; 7(3): virtualmentor.2005.7.3.cprl1-0503.
- Knight JR, Sherritt L, Shrier LA, Harris SK, Chang G. Validity of CRAFFT substance abuse screening test among adolescent clinic patients. Arch Pediatr Adolesc Med. (2002) Jun;156(6):607-614.
- American College of Surgeons, Resources for the Optimal Care of the Injured Patient, 2022 Standards.