Pharmaceutical Management of Post-TBI Neuropsychiatric Symptoms
Definitions
1. Depression: TBI-associated depression is characterized by prolonged, persistent sadness associated with other symptoms such as anhedonia, lack of motivation, decreased self-care, variable sleep and/or appetite pattern, feelings of hopelessness, and/or suicidal thoughts. These symptoms may last for a couple of weeks to months (major depressive episode) or persist in a milder form for two or more years (dysthymia).
2. Mania/Agitation: Subtype of delirium unique to TBI which occurs during period of Post traumatic amnesia (PTA – period of time in which new memory formation is impaired), characterized by excess of behavior that includes some combination of aggression, disinhibition, akathisia, disinhibition, and emotional liability IN ABSENCE of other physical, medical or psychiatric causes.
3. Anxiety: A wide range of anxiety disorders may occur after TBI including generalized anxiety disorder, agoraphobia, social phobia, panic disorder, and obsessive-compulsive disorder.
4. PTSD: Symptoms may include nightmares or unwanted memories of the trauma, avoidance of situations that bring back memories of the trauma, heightened reactions, anxiety, or depressed mood.
5. Psychosis: There are predominantly 2 types of TBI-related psychosis: delusional disorders and schizophrenia-like psychosis.
6. Sleep disturbance: Sleep disturbances are common after TBI and can occur in isolation or as a symptom of a psychiatric disorder. Insomnia is the most common sleep disturbance, seen in about 50% of patients with TBI, although other disturbances such as hypersomnia, sleep apnea, and sleepwalking may also be present.
7. Executive function deficits: The constellation of cognitive impairments following TBI is variable and depends on the severity of the location of the injury on the brain. TBI can affect every cognitive domain, including attention, memory, visual-spatial processing, language, social cognition, and executive functioning.
Assessment and Diagnosis
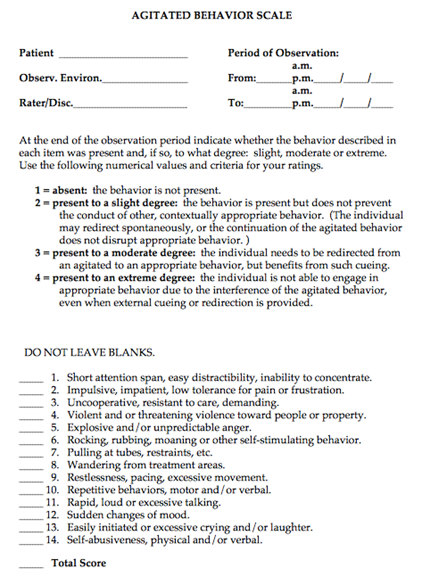
1. Mania/Agitation- Agitated Behavior Scale where 22-28 is mild agitation, 29-35 is moderate agitation, and 36-56 is severe agitation.
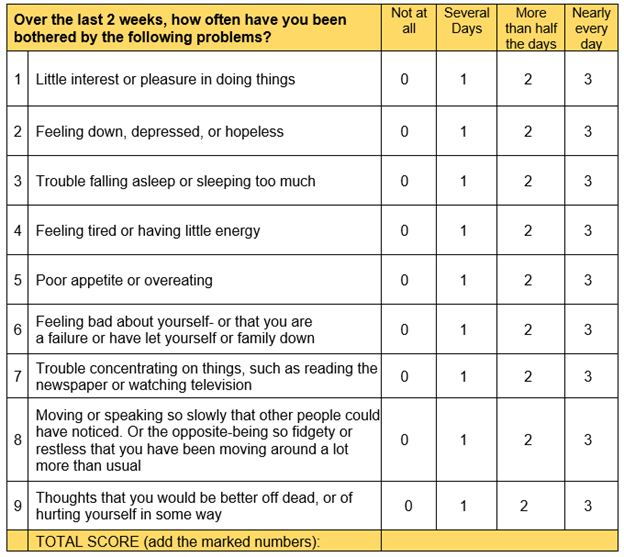
2. Depression- PHQ 9 where 1-4 is minimal depression, 5-9 is mild depression, 10-14 is moderate depression, 15-19 is moderately severe depression and 20-27 is severe depression
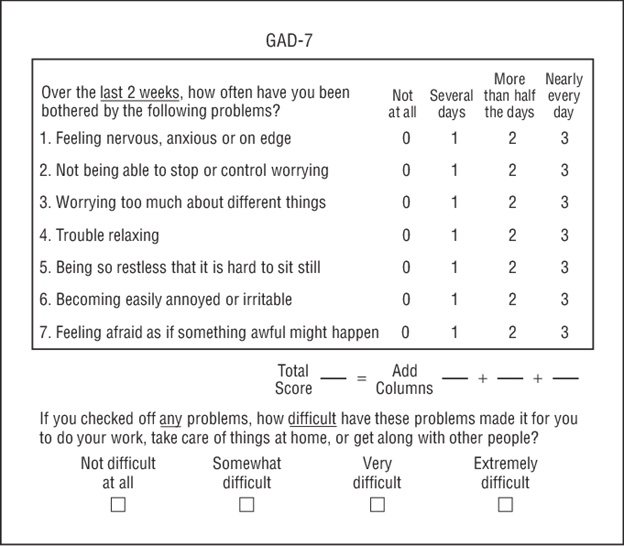
3. Anxiety: GAD-7 where 0-4 is minimal anxiety, 5-9 is mild anxiety, 10-14 is moderate anxiety, and 15-21 is severe anxiety
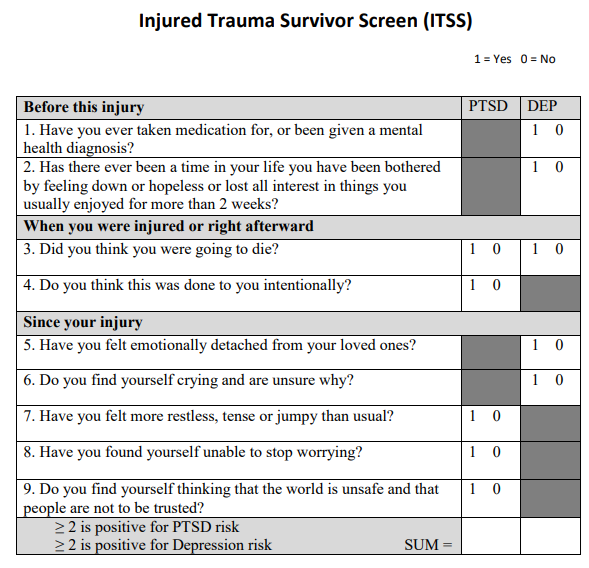
4. PTSD: ITSS where PTSD is evaluated in items 3, 4, 7, 8, 9 and Depression is evaluated in items 1, 2, 3, 5, 6. If the sum of questions 1, 2, 3, 5, and 6 is equal to or greater than 2, the screen is positive for PTSD risk. If the sum of questions 3, 4, 7, 8 and 9 is equal to or greater than 2, the screen is positive for depression risk.
5. Memory deficits, executive function deficits, and inattention: consult Speech Therapy for cognitive evaluation
Pharmacologic Management
General Considerations for all patients:
Propranolol - Patients with TBI by CT and GCS <12, hemodynamically stable at 24 hrs after admission (BP>100, not requiring vasopressor or blood transfusion) should be started on propranolol 20 mg po q12hrs . If patient develops bradycardia (HR<50 bpm) or hypotension (SBP <100mmHg), then propranolol should be stopped. Increase the dose from 20 mg BID to 40 mg BID based upon SBP>140s, and HRs> 110-120s. (Of note, if BP remains high, consider adding another agent). Propranolol should be stopped upon discharge or after 7 days, whichever is sooner.
In patients on home beta-blockers (for hypertension, heart failure, afib rate control), switch to propranolol temporarily and stop the home beta blocker (avoid ordering 2 beta blockers on the same patient). Propranolol dose can be titrated up if needed for BP or HR) or a second antihypertensive ordered.
Clonidine – has unclear role for use in TBI patients for agitation or storming. Its use as adjunct therapy in withdrawal syndromes is longstanding. It is explored for use as a transition-off agent in patients on dexmedetomidine and as an adjunct in treating PSH. Thus, practical uses for clonidine include: treating agitation in conjunction with withdrawal syndromes, treating agitation/delirium in a patient weaning off dexmedetomidine or whom dexmedetomidine was effective, 3-4th line in PSH (after gabapentin, opiates, benzos have been tried/considered). Initial dosing should be 0.1 mg PO TID. If patient is already on dexmedetomidine, the dose can be started at 0.2-0.3 mg TID and the dexmedetomidine can be decreased. Side effects include: hypotension, rebound hypertension, withdrawal.
Antipsychotics and stimulants– Generally for short-term use, should be tapered when symptoms resolve. Use assessment tools prior to initiation of pharmacologic agents to ensure you are treating the correct symptom.
All new antipsychotics and stimulants should be reviewed and weaned (if possible) at time of transfer from ICU to floor, and again, at time of discharge from hospital.
|
Assessment tool |
First line medications |
Standard dosage |
Common adverse effects |
|
|
Depression |
PHQ 9 |
Sertraline |
Start: 25 or 50 mg daily.
May double dose after 1 week, assess for effect in 4 weeks before further increasing. |
Nausea, diarrhea, sexual dysfunction |
|
Manic: acute |
Agitated Behavior Scale |
Quetiapine |
Start: 25-50 mg BID
Increase to effect to maximum of 400 mg/day |
Sedation, Parkinsonism, weight gain, QTc prolongation |
|
Mania: maintenance |
Agitated Behavior Scale |
Valproate |
Start: 250 mg TID
May load with 15 mg/kg for rapid symptom control
May increase every 2-3 days, checking level to ensure not above range |
Hepatotoxicity, hyperammonemia, thrombocytopenia, drug interaction with carbapenems
Safe therapeutic range: 50-125 mcg/mL |
|
Anxiety |
GAD-7 |
Sertraline |
Start: 25 mg daily
May double dose every 2 weeks until 100 mg daily reached. Assess in 4 weeks before further increasing. |
Nausea, diarrhea, sexual dysfunction
Low dosing to avoid worsening anxiety during initiation period |
|
PTSD |
ITSS |
Sertraline or paroxetine |
Sertraline Follow anxiety dosing
Paroxetine Start: 20 mg daily, may increase in 10 mg increments per week up to 60 mg daily. |
Nausea, diarrhea, sexual dysfunction
Paroxetine has higher sedating effect. |
|
Psychosis |
|
Risperidone or quetiapine |
Quetiapine Acute dose: 25 mg If scheduled dose indicated, same as above.
Risperidone Acute dose: 1-2 mg, up to 6 mg in 24 hours |
Parkinsonism, sedation |
|
Apathy |
|
Methylphenidate |
Start: 5 mg BID
|
Agitation, anxiety, insomnia, palpitations, tachycardia |
|
Sleep disturbance |
|
Melatonin
2nd line: Trazodone |
Melatonin 3-9 mg nightly
Trazadone 50 mg nightly |
Daytime drowsiness, sensory distortion, sleep walking |
|
Executive function deficits |
Consult Speech Therapy for cognitive evaluation |
Amantadine |
Start 100 mg BID
May increase in 50 mg increments weekly to max of 200 mg BID |
Headache, nausea, diarrhea, insomnia, orthostasis, psychosis at high doses |
|
Inattention |
Consult Speech Therapy for cognitive evaluation |
Methylphenidate |
Start: 5 mg BID, start >7-10 days post injury
|
Agitation, anxiety, insomnia, palpitations, tachycardia |
Appendix A: Agitated Behavior Scale where 22-28 is mild agitation, 29-35 is moderate agitation, and 36-56 is severe agitation.
Appendix B: PHQ 9 where 1-4 is minimal depression, 5-9 is mild depression, 10-14 is moderate depression, 15-19 is moderately severe depression and 20-27 is severe depression
Appendix C: GAD-7 where 0-4 is minimal anxiety, 5-9 is mild anxiety, 10-14 is moderate anxiety, and 15-21 is severe anxiety
Appendix D: ITSS where PTSD is evaluated in items 3, 4, 7, 8, 9 and Depression is evaluated in items 1, 2, 3, 5, 6. If the sum of questions 1, 2, 3, 5, and 6 is equal to or greater than 2, the screen is positive for PTSD risk. If the sum of questions 3, 4, 7, 8 and 9 is equal to or greater than 2, the screen is positive for depression risk.
Authors:
Charity Evans, Abby Josef Trauma and Acute Care Surgery
Becca Sedlak, Pharmacy
Last Updated: January 2024