Evaluation and Management of Non-Accidental Trauma (NAT) in Children at Nebraska Medicine
Purpose:
To provide guidance and a standardized approach for the initial evaluation, management and reporting of children with injuries concerning for abuse.
Background/Definitions:
Annually, nearly 1 million children are victims of child maltreatment in the United States. It is estimated that 1:4 children will experience some form of child abuse or neglect in their lifetime (1:7 in the past year) accounting for a total lifetime economic cost upward of $124 billion.
The Centers for Disease Control (CDC) defines child maltreatment as “any act or series of acts of commission or omission by a parent or other caregiver that results in harm, potential for harm, or threat of harm to a child.”
- Physical abuse, sexual abuse, and psychological abuse are types of abuse resulting from acts of commission.
- Acts of omission or neglect (e.g. delays in seeking treatment/care, inappropriate supervision, not using vehicle restraints) can worsen outcomes when the child is abused.
The Child Abuse Prevention and Treatment Act (CAPTA) establishes that standard legal definition of child abuse and neglect as “any recent act or failure to act on the part of the parent or caretaker which results in death, serious physical or emotional harm, sexual abuse or exploitation; or an act or failure to act, which presents an imminent risk of serious harm.”
In 2019, there were approximately 656,000 victims of child abuse and/or neglect in the United States as confirmed by state child protective service agencies.
- This equates to a national rate of 8.9 victims per 1,000 children in the population.
- Approximately 28% of victims were in the range of birth through 2 years old. 14.9% of all victims were younger than 1 year. The rate is highest for children younger than 1 year old at 25.7 per 1,000 children in the population of the same age.
Nationally, there were an estimated 1,840 children who died from abuse and neglect in 2019.
- This is a rate of 2.5 deaths per 100,000 children in the population. This is an approximate 10.8% increase from the 2015 estimation.
- Approximately 70% of all child fatalities were younger than 3 years old and close to half (45.4%) of all child fatalities were younger than 1 year old.
- The child fatality rates mostly decrease with age. Younger children are the most vulnerable to death as the result of child abuse and neglect.
- Nearly 80% of all fatalities involved one or both of the parents.
Sentinel injuries are injuries suspicious for physical abuse with rates of abuse high enough to warrant routine evaluation of abuse if the injury is present. Sentinel injuries can seem minor, and high level of suspicion and familiarity with high-risk injuries is critical for identification.
For the purposes of this guidelines, a non-ambulatory child is a child who cannot take two independent steps without the assistance of a person or inanimate object for support. Cruising is not considered ambulatory.
Guideline Inclusion Criteria:
· Children from newborn through adolescence (18 years and younger) with an injury concerning for physical abuse.
Guideline Exclusion Criteria:
· Injured patients age >18 years.
· Children involved in a motor-vehicle collision, regardless of age or ambulatory status, are excluded from this guideline.
Diagnostic Evaluation:
While any injury can be the result of physical abuse, there are NO injuries that are pathognomonic. The following are reasons to be concerned that injuries could be related to physical abuse (this list is not exhaustive):
History:
- No explanation or vague explanation of injury.
- An important detail of the explanation changes significantly.
- An explanation that is inconsistent with the pattern, age or severity of the injury or injuries.
- An explanation that is inconsistent with the child’s physical and/or developmental capabilities.
- Different caregivers provide different explanations for the injury or injuries, or a single caregiver provides history that changes over time.
- Unwitnessed injury
- Delay in seeking care for an injury.
- Prior ED visits for injury
- Domestic violence in home
- Premature infant (<37 weeks)
- Low birth weight/IUGR
- Presence of chronic medical conditions
Physical Exam:
- Age:
-
- All ages
- Non-ambulatory and non-verbal children are particularly vulnerable.
- All ages
-
- Bruising:
-
- Bruising in children <9 months of age
- Any bruise in non-ambulatory children
- Patterned bruising
- Extensive or clustered bruising
- Intraoral injuries (i.e. frenulum tears, pharyngeal injury) <9 months or non-ambulatory
- The TEN-4-FACESp Bruising Clinical Decision Rule is a highly sensitive and specific tool in identifying bruising that is concerning for abuse.
-
- “TEN”: bruising on Torso (chest, abdomen, back buttocks, GU region, hips), Ears or Neck.
- “FACES”: bruising on Frenulum, Angle of jaw, Cheek (fatty portion), Eyelids, Subconjunctivae
- “4”: “TEN-FACES” bruising on a child younger than 4 years old or any bruising in an infant 4 months or younger.
- “p”: Patterned bruising
-
-
- Burns
-
- Patterned burns (i.e. suspected cigarette burns or other burns with a particular shape)
- Stocking or glove immersion burns
- Burns in non-ambulatory patients.
-
- Fractures (Highly specific for physical abuse)
-
- Classic metaphyseal lesions (i.e. long bone fractures at the infant growth plate)
- Rib fractures (particularly posteromedial)
- Scapular or sternal fractures
- Spinous process fractures
-
- Fractures (moderately specific for physical abuse)
-
- Non-ambulatory child
- Digit fractures
- Complex skull fractures
- Vertebral body fractures/subluxations
- Epiphyseal separations
- Fractures of varying ages
- Multiple fractures, especially bilateral
- Pelvic fractures
-
- Abusive head trauma (AHT)
-
- Vague presenting signs and symptoms may be associated with AHT. AHT should be considered in the differential diagnoses of young children with non-specific history of/findings such as:
-
- Altered mental status (lethargy, fussiness)
- Seizures/seizure-like activity
- Vomiting
- Cyanosis
- Marked change in muscular tone
- Apnea/reported apnea
- Decreased or irregular breathing
- Enlarging head circumference
- Diffuse intracranial hemorrhage
- Mixed density intracranial hemorrhage
- Bilateral intracranial hemorrhage
- Intracranial hemorrhage with altered mental status
- Intracranial hemorrhage with no history of trauma
- Intracranial hemorrhage with ischemic parenchymal injury
- Intracranial hemorrhage with spinal/paraspinal hemorrhage and/or spinal ligamentous injury
- Intracranial hemorrhage with other evidence of injury (cutaneous, skeletal, intraabdominal)
- Parenchymal injury (contusion, tear, diffuse axonal injury)
- Diffuse cerebral edema without identifiable intracranial hemorrhage on head CT.
- Retinal hemorrhages (those that are too numerous to count/diffuse in one or both eyes, present in multiple layers of retina, and extending into the retinal periphery are most concerning)
-
- Vague presenting signs and symptoms may be associated with AHT. AHT should be considered in the differential diagnoses of young children with non-specific history of/findings such as:
-
Practice Recommendations for Management:
Injured children presenting to Nebraska Medicine should be initially evaluated and managed in accordance with ATLS guidelines. Clinicians should first ensure the child is medically stable. If during the assessment concerns for physical abuse/non-accidental trauma are raised, the following additional work-up should ensue as early as practical based on the severity of injuries and clinical status of the child.
Initial Management:
Children 0 to 24 months meeting at least one of the following criteria:
- Less than 24 months with an injury concerning for abuse
- Non-ambulatory with a skeletal fracture
- Less than 12 months with a skeletal fracture
- Thorough history
-
- Detailed description of illness/injury from the time the child was last well. Include any history of trauma as well as circumstances leading to the discovery of the injury.
- It is important to document the history as early as practical in the process.
- Note inconsistencies and changing histories as well as delays in care.
- Full medical history of the child (birth history, prior hospitalizations/ED visits/injuries/wellness visits), development (normal vs abnormal) and social history (all caregivers and other who live in household, domestic violence prior CPS/police contact)
-
- Head to toe physical assessment
-
- Review vital signs, neurologic exam, thorough skin assessment including ears and frenula.
- Detailed documentation of all the abnormal findings.
-
- Social work consultation.
-
- Social worker can assist in obtaining a detailed psychosocial history and assessment from family/caregivers, assist in communication with law enforcement and CPS as indicated, and communication with the Children’s Advocacy Team.
-
- Children’s Advocacy Team (CAT) consultation (Most consults can be called during regular business hours, M-F, 8am-5pm).
- Make report to Child Protective Services (CPS).
-
- Report may be made by any provider/person involved in child’s care who has reasonable cause to believe that the child subjected to abuse or neglect. It is a criminal offense to NOT report if abuse/neglect is suspected.
-
- CPS report number should be documented in a progress note in the patient’s electronic medical record.
-
- Trauma attending must be notified that a CPS report has been filed.
- Inform parents/caregivers of child if a CPS referral has been filed and should ideally be done by trauma attending or next most senior provider or social worker involved in child’s care.
- Report may be made by any provider/person involved in child’s care who has reasonable cause to believe that the child subjected to abuse or neglect. It is a criminal offense to NOT report if abuse/neglect is suspected.
-
- If child is felt to be in imminent danger, involve law enforcement/police (based on location of where the alleged abuse/neglect occurred)
- Skeletal survey
- Transaminase levels (AST/ALT) and serum lipase
- Head CT without contrast
-
- All children less than 6 months
- Children 6-12 months with neurologic abnormality and/or external evidence of head injury.
- See “abusive head trauma” (AHT) section
-
- Photo documentation in the electronic medical record of all external injuries, including burns, if the injury is concerning for abuse.
Children >24 months with an injury concerning for abuse will receive the following:
- Thorough history
-
- Detailed description of illness/injury from the time the child was last well. Include any history of trauma as well as circumstances leading to the discovery of the injury
- It is important to document the history as early as practical in the process.
- Note inconsistencies and changing histories as well as delays in care.
- Full medical history of the child (birth history, prior hospitalizations/ED visits/injuries/wellness visits), development (normal vs abnormal) and social history (all caregivers and other who live in household, domestic violence prior CPS/police contact)
-
- Head to toe physical assessment
-
- Review vital signs, neurologic exam, thorough skin assessment including ears and frenula.
- Detailed documentation of all the abnormal findings.
-
- Social work consultation.
-
- Social worker can assist in obtaining a detailed psychosocial history and assessment from family/caregivers, assist in communication with law enforcement and CPS as indicated, and communication with the Children’s Advocacy Team.
-
- Children’s Advocacy Team (CAT) consultation (Most consults can be called during regular business hours, M-F, 8am-5pm).
- Make report to Child Protective Services (CPS).
-
- Report may be made by any provider/person involved in child’s care who has reasonable cause to believe that the child subjected to abuse or neglect. It is a criminal offense to NOT report if abuse/neglect is suspected.
-
- CPS report number should be documented in a progress note in the patient’s electronic medical record.
-
- Trauma attending must be notified that a CPS referral has been filed.
- Inform parents/caregivers of child if a CPS referral has been filed and should ideally be done by trauma attending or next most senior provider or social worker involved in child’s care.
- Report may be made by any provider/person involved in child’s care who has reasonable cause to believe that the child subjected to abuse or neglect. It is a criminal offense to NOT report if abuse/neglect is suspected.
-
- If child is felt to be in imminent danger, involve law enforcement/police (based on location of where the alleged abuse/neglect occurred).
- Skeletal survey—recommended only in children up to 5 years on a case by case basis:
-
- i.e. unconscious patient, non-verbal patient, non-ambulatory patient, or inadequate exam.
-
- Transaminase levels (AST/ALT) and serum lipase
-
- Recommended with multiple or severe injuries or with concern for abdominal or pelvic trauma
-
- Head CT without contrast
-
- Children with neurologic abnormality and/or external evidence of head injury.
- See “abusive head trauma” (AHT) section
-
- Photo documentation in the electronic medical record of all external injuries, including burns, if the injury is concerning for abuse.
Additional Laboratory and Diagnostic Evaluation
Additional labs, imaging and testing may be obtained as indicated specific to the injury or individual circumstances. If there are questions regarding what additional testing is needed, please discuss with the CAT.
- Laboratory:
-
- Urine and serum toxicology
-
- Concern for ingestion
- Evidence of neurologic abnormality
-
-
- If CT head is obtained due to concerns for abusive head trauma (fussiness, vomiting, seizures, brief resolved unexplained event (BRUE), etc.), urine and serum toxicology is also indicated.
-
-
- Report or suspicion of substance abuse in caregiver, either by history or presentation.
-
- CBC, PT/INR, PTT, vW panel, Factor VIII and IX levels
-
- Intracranial hemorrhage (ICH) concerning for abusive head trauma
- Consider in patient with diffuse cerebral edema without identifiable ICH on CT head.
- Bruising concerning for inflicted injury
-
-
- Factors which increase the likelihood of abusive bruising include:
-
- <9 months of age
- Non-ambulatory child
- Bruising which meets the TEN-4-FACESp Bruising Clinical Decision Rule Criteria.
-
- Factors which increase the likelihood of abusive bruising include:
-
-
- Other injuries associated with bleeding
-
- Solid organ injury concerning for inflicted trauma
-
- Children with clinically significant bleeding
-
- Bone abnormality evaluation (25-hydroxy-Vit D, bioactive PTH, Alkaline Phosphatase, Calcium, Phosphorus levels)
-
- Recommended in children with >1 skeletal fracture concerning for abuse
- Recommended in children with a skeletal fracture(s) with radiographic concern for osteopenia or metabolic bone disease
- Special consideration (after discussion with CAT team)
-
- Ionized calcium
-
- Children with hypoalbuminemia or who appear malnourished or concern for failure to thrive
-
- Serum copper, ceruloplasmin, and vitamin C
-
- Consider in children at risk for scurvy or copper deficiencies in the setting of metaphyseal irregularities
-
- Ionized calcium
-
-
- Urine and serum toxicology
-
- Imaging:
-
- CT Abdomen/Pelvis with IV contrast
-
- Abnormal abdominal exam such as bruising, distention, tenderness, vomiting
- Consider with >10 RBCs per HPF on urinalysis
- ALT or AST >80 mg/dL or Lipase >100
-
- Or admit to trauma service for observation and serial abdominal exams.
-
- May be indicated as per CAT.
-
- MRI/MRV brain with and without contrast
-
- May be indicated with ICU to further delineate injury, per Trauma, Neurosurgery, or CAT.
-
- MRI cervical, thoracic, lumbar spine without contrast
-
- May be indicated with ICU to further delineate injury, per Trauma, Spine (neurosurgery or orthopedic surgery), or CAT.
-
- CT Abdomen/Pelvis with IV contrast
-
Consultation
Admission/Disposition
- For children with injuries requiring admission for medical or surgical management, the TRAUMA SERVICE will be the primary admitting service with CAT, Pediatrics (either pediatric critical care or pediatric co-management team depending on level of care), and subspecialty consultation as indicated.
-
-
-
- The family should be informed of the plan to involve CAT if applicable.
-
- Isolated injuries with no ongoing concerns for abuse may be admitted to the appropriate surgical subspecialty as appropriate (i.e. orthopedics, neurosurgery, etc.).
- Other considerations:
-
- Non-surgical admissions
-
-
-
- In general, children with traumatic injury felt to be secondary to abuse should NOT be admitted to a non-surgical service unless it is felt to be in the best interest of the patient (i.e. medically complex with minor traumatic injury not requiring intervention). If the child is being admitted to a non-surgical service, the attending trauma surgeon must explicitly document why he/she feels the child would be better served by a non-surgical service.
-
-
-
- Children admitted for a medical/non-traumatic diagnosis (i.e. seizures, failure to thrive, etc.) and are later suspected or discovered to have a traumatic injury should have a trauma consultation as soon as the injury is discovered. Trauma team consultation should not be delayed for a sub-specialty surgical consult.
- Non-surgical admissions
-
-
-
- For children with injuries that do NOT require admission for medical/surgical management but have reasonable concern for abuse,
-
- Consult the ED social worker who will email CAT ([email protected]) with details of the case for review.
-
- CAT will contact the family if follow-up is indicated.
- Do not instruct the family to call CAT.
-
- CPS report is made.
-
- Request CPS involvement for discharge. If/when a safe disposition has been established by CPS and agreed upon by ED/Trauma/SW providers, the patient may be discharged from the ED.
- If a safe disposition cannot be developed by CPS in the ED in a timely fashion, the patient will be admitted to the Trauma Service for observation until a plan is in place.
-
- Consult the ED social worker who will email CAT ([email protected]) with details of the case for review.
-
- For children with injuries that do NOT require admission for medical/surgical management, but provider is unsure if there is reasonable concern for abuse,
-
-
-
- During normal business hours (M-F, 8a-5p), provider to call CAT at 402-955-6250 or by calling the Children’s Physician Priority line at 855-850-KIDS (5437) and asking for provider on call for CAT.
- If after hours/weekends, provider to call the on-call CAT provider by calling the Children’s Physician Priority line at 855-850-KIDS (5437)
- ED social worker emails CAT ([email protected]) with details of case for review.
- Provider is to call the on-call CAT provider to discuss and develop a plan.
-
- CAT will contact the family if follow-up is indicated.
- Do not instruct the family to call CAT.
-
- CPS report at discretion of providers/SW/CAT
-
- If CPS is notified, request CPS involvement for discharge. Once a safe disposition has been established by CPS and agreed upon by ED/Trauma/SW providers, the patient may be discharged from the ED.
- If a safe disposition cannot be developed by CPS in the ED in a timely fashion, the patient will be admitted to the Trauma Service for observation until a plan is in place.
-
-
-
-
***Please see algorithm from Pediatric Trauma Society and Western Trauma Association below as an additional guide to what is stated above***
Reminders:
- Do not accuse or treat families/caregivers any differently than others. Keep the discussion neutral and patient centered/focused.
- Discuss suspected abuse reporting requirements with family/caregivers.
- Consider having the senior staff (APP or attending) or senior resident as the primary providers for these cases.
Important phone numbers:
- Nebraska Child Protective Services Hotline: 800-652-1999
- Iowa Department of Human Services Hotline: 800-362-2178
- Children’s Advocacy Team: 402-955-6250
- Children’s Social Work Department: 402-955-5418
- Children’s Physician Priority Line: 855-850-KIDS (5437)
- Omaha Police Department, Child Victim/Sexual Assault Unit: 402-222-5636 or 402-444-4135
- Bellevue Police Department: 402-293-3100
- Children’s Advocacy Team (CAT) email: [email protected]
Follow-up Care:
- Injured children may follow-up with trauma and consulted subspecialty teams as indicated for injuries.
- Children’s Advocacy Team as indicated for all aspects of care related to and sequela of abuse/neglect.
Outcome Measures and Guideline Adherence:
- All cases of traumatic injury secondary to non-accidental trauma will be reviewed by the pediatric trauma medical director and pediatric trauma program manager at a primary level. Additional levels of review will be performed on a case-by-case basis and involve consultant teams and Child Advocacy Team as needed.
- Nebraska Medicine Policy PE02, “Identification of Abuse or Neglect”
- Nebraska Medicine Policy PE 03, “Reporting of Abuse, Neglect, or Injury”
Key Contributors:
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principal Author
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Coordinator | Co-Author
- Suzanne Haney, MD, MS, FAAP | Division Chief, Child Abuse Pediatrics | Reviewer
Last updated:
· June 2024
References:
- Prevention CDCa. Child Maltreatment: Fact-Sheet. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention; 2014. http://www.cdc.gov/ncipc/factsheets/cmfacts.htm.
- Prevention CDCa. Child Abuse and Neglect Prevention. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention; 2017. http://www.cdc.gov/violenceprevention/childmaltreatment/.
- Finkelhor D, Turner HA, Shattuck A, Hamby SL. Violence, crime, and abuse exposure in a national sample of children and youth: an update. JAMA Pediatr. 2013;167(7):614-21.
- Leeb RT, Paulozzi L, Melanson C, et al. Chile Maltreatment Surveillance: Uniform Definitions for Public Health and Recommended Data Elements, Version 1.0. In: Center for Disease Control and Prevention NCflPaC, editor. Atlanta, GA. 2008.
- U.S. Department of Health and Human Services ACYF, Administration on Children, Youth and Families, Children’s Bureau. Child Maltreatment 2016. Washington, D.C.: Children’s Bureau (Administration for Children, Youth, and Families, Administration for Children and Families) of the U.S. Department of Health and Human Services, 2018.
- Berger RP, Lindberg DM. Early recognition of physical abuse: Bridging the gap between knowledge and practice. J Pediatr. 2018; 204:16-23.
- Pierce MC, Kaczor K, Aldridge S, O’Flynn J, Lorenz DJ. Bruising characteristics discriminated physical child abuse from accidental trauma. Pediatrics, 2010: 125(1); 67-74.
- Pierce MC, Kaczor K, Lorenz DJ, Bertocci G, Fingarson AK, Makoroff K, Berger RP. Validation of a clinical decision rule to predict abuse in young children based on bruising characteristics. JAMA Netw Open. 2021; 4(4):e215832.
- Kleinman PK, ed. Diagnostic Imaging of Child Abuse. 3rd ed. Cambridge University Press, 2015.
- ACS Trauma Quality Programs Best Practice Guidelines for Trauma Center Recognition of Child Abuse, Elder Abuse, and Intimate Partner Violence. abuse_guidelines.pdf (facs.org) November, 2019.
- Burg B, Dougherty M, Snyder K, Shanghvi D, Naiditch J, et al. Dell Children’s Medical Center, Evidence-based Outcome Center, “Evaluation for Occult Injury Guideline”. February, 2022.
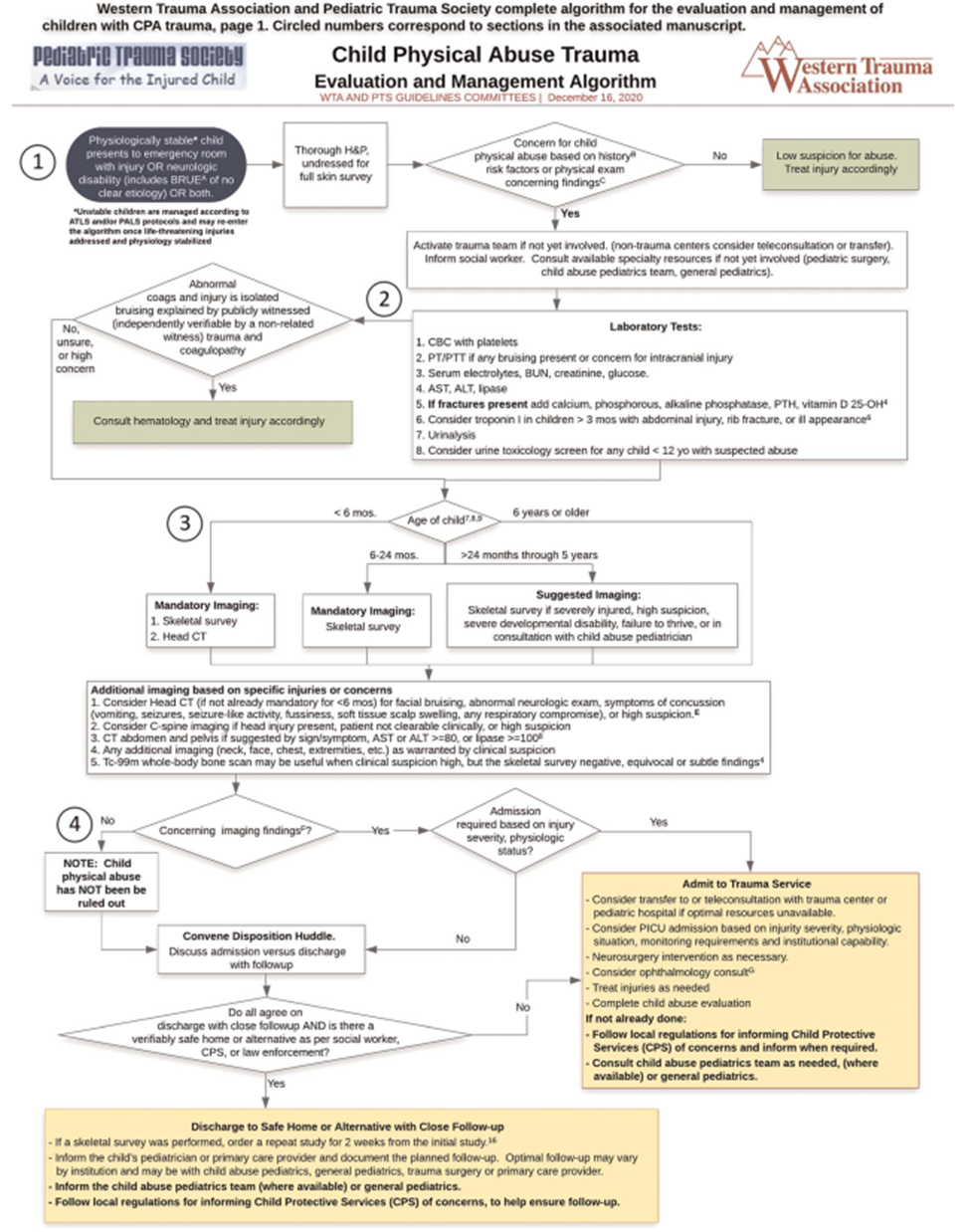
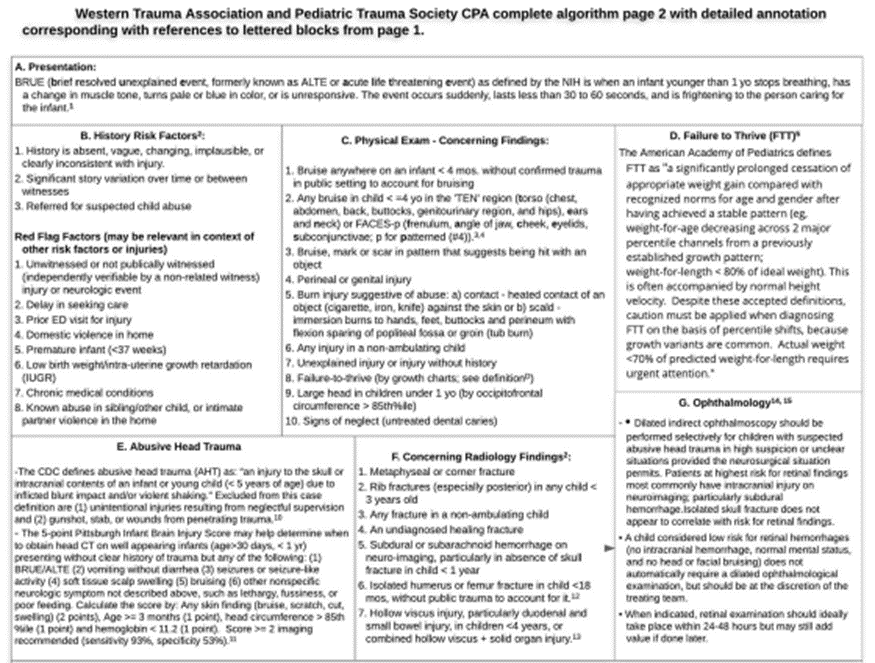
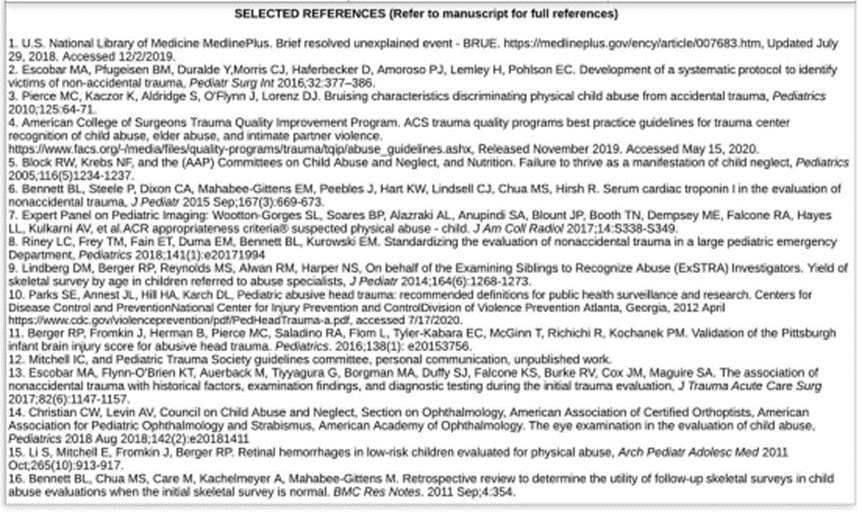
- Rosen NG, Escobar MA, Brown CV, et al. Child physical abuse trauma evaluation and management: A Western Trauma Association and Pediatric Trauma Society critical decisions algorithm. J Trauma Acute Care Surg.2021; 90(4): 641-651.
Western Trauma Association and Pediatric Trauma Society complete algorithm for the evaluation and management of children with Child Physical Abuse (CPA) trauma.