Evaluation and Management of Blunt Solid Organ Injuries in Pediatric Trauma Patients
Purpose:
These guidelines are meant to help guide the provider through the initial evaluation and management of pediatric trauma patients sustaining blunt solid organ injuries to the liver, spleen, or kidney at Nebraska Medicine.
Background/definitions:
Solid organ injuries may occur to the liver, spleen or kidney. Non-operative management of solid organ injuries in the setting of blunt trauma is preferred when possible and is considered the standard of care in hemodynamically stable pediatric patients, irrespective of the grade of injury. Literature reveals that non-operative management of pediatric blunt solid organ injuries is associated with a low overall morbidity and mortality and does not result in increased length of stay, need for blood transfusions, bleeding complications or associated hollow viscous injuries as compared with operative management.
Guideline Inclusion Criteria:
- Pediatric trauma patients less than 15 years of age with a radiographically identified blunt liver, splenic or kidney injury at Nebraska Medicine.
Guideline Exclusion Criteria:
- Penetrating mechanism of injury
- Trauma patients 15 years of age and older (See separate adult guidelines for management of blunt solid organ injuries).
Diagnostic Evaluation:
- All trauma patients should be initially evaluated per ATLS guidelines with work-up as mechanism and clinical presentation dictate.
- Resuscitative measures should be initiated as clinical status/presentation dictates.
- Labs, imaging and additional tests should be obtained as clinical status/presentation dictates. (See “Guidelines For
- Imaging the Pediatric Trauma Patient”)
- If a patient is hemodynamically UNSTABLE, minimal testing/imaging should occur prior to interventions for hemorrhage control.
Practice Recommendations for Management:
- Once solid organ injury is suspected and/or confirmed, management of that injury is dictated largely by the clinical status of the patient.
- Initial Evaluation/Resuscitation:
-
- o Management of the hemodynamically UNSTABLE patient as evidence by moderate to severe tachycardia and/or hypotension
-
- Initial resuscitative measures should include the following:
-
- Placement of 2 large bore peripheral IVs (or equivalent central venous access as able)
- Bolus 20 ml/kg NS or LR (if blood not immediately available)
- Type and Cross 2-4 units PRBC (age and weight dependent)
- Transfuse uncrossed PRBC (or whole blood if age≥13 and available) 20mL/kg if hypotension unresponsive to crystalloid bolus.
- Obtain labs (VBG, CBC, PT/INR, etc.)
- Obtain eFAST.
- If eFAST is positive and/or patient remains UNSTABLE (i.e. tachycardia and hypotension persist) despite appropriate resuscitative measures:
-
- Activate the Massive Transfusion Protocol (MTP; see policy TX-36 “Massive Transfusion/Severe Coagulopathy/Emergency Release Blood” and PRO09 “Massive Transfusion in Trauma Guidelines”)
- Consider proceeding to OR for emergent laparotomy or IR for angioembolization.
-
-
- Initial resuscitative measures should include the following:
-
- o Management of the hemodynamically UNSTABLE patient as evidence by moderate to severe tachycardia and/or hypotension
-
- Management of the hemodynamically STABLE patient as evidenced by mild tachycardia without hypotension OR patients that become STABLE with initial resuscitative measures listed above (responders)
-
- Initial resuscitative measures as listed above should be performed as indicated based on clinical status of child. At minimum,
-
- Ensure and maintain IV access
- If fluid resuscitation not indicated, initiate maintenance IV fluids at weight-based rate, typically with NS or LR
- Send type and screen on all patients and consider type and cross 2 units PRBC depending on any patient with history of hemodynamic instability or those with higher grade injuries.
-
- Obtain multi-phase CT abdomen/pelvis with IV contrast as indicated by Imaging guidelines for pediatric trauma patients to diagnose/confirm presence of solid organ injury.
-
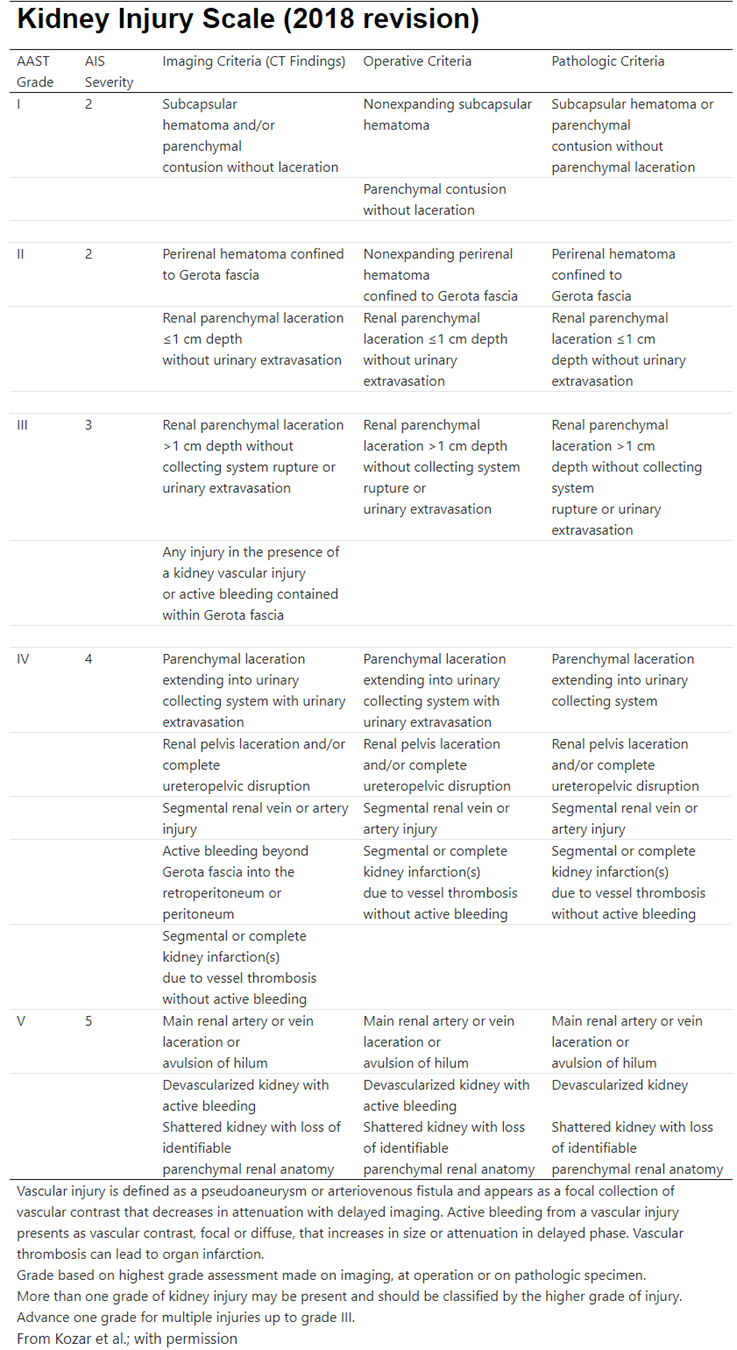
- If renal injury identified, also obtain a delayed imaging phase to assess for involvement of the collecting system.
-
- Determine appropriate management strategy based on grade of injury, presence of blush/contrast extravasation on imaging, and clinical status/injury burden of the patient.
- Consult urology for renal injuries with disruption/involvement of the collecting system
- Initial resuscitative measures as listed above should be performed as indicated based on clinical status of child. At minimum,
-
- Management of the hemodynamically STABLE patient as evidenced by mild tachycardia without hypotension OR patients that become STABLE with initial resuscitative measures listed above (responders)
-
- Disposition and cares following initial resuscitation:
-
- Admission Level of Care
-
- Decision for level of care should be based on clinical status of patient, not grade of injury, and is ultimately at the discretion of the trauma attending.
- ICU admission is indicated for the following patients
-
- Patients with current hemodynamic instability
- Patients with transient response to initial volume resuscitation
- Patients requiring intervention for hemorrhage control (i.e. IR angioembolization or operative intervention)
-
- Floor or Progressive Care should be considered for hemodynamically stable patients or those who become stable with sustained response to initial volume resuscitation.
-
- Activity
-
- Bedrest until vitals normal
- Once hemodynamically stable, activity as tolerated with no restrictions.
-
- Labs
-
- CBC on admission and Q6hr until vitals normal and Hb/HCT stable x 2
- Renal function should be monitored with BUN/CRT in setting of kidney injury.
-
- Diet and IV fluids
-
- NPO until vitals normal and Hb/HCT stable
- Once hemodynamically stable, regular diet as tolerated
- Continue maintenance IV fluids until meeting oral hydration goals
-
- Vital Signs
-
- Per unit protocol (ICU-q1hr, Progressive Care-q2hr, Floor-q4hr)
-
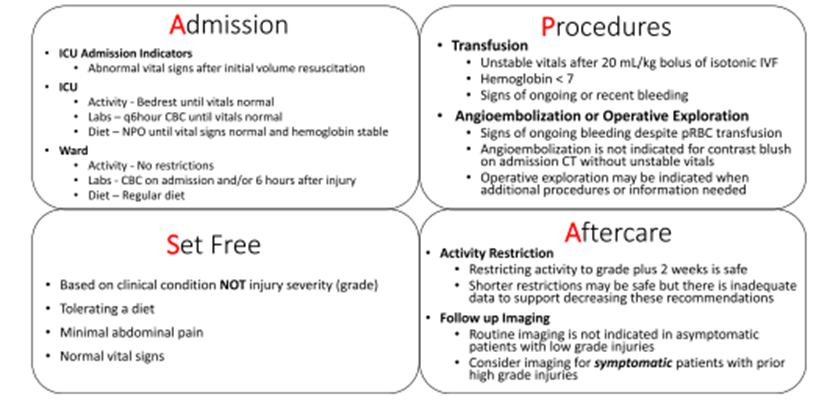
- Transfusion
-
- Unstable vitals after 20 mL/kg bolus of isotonic IVF
- Hemoglobin <7
- Signs of ongoing or recent bleeding
-
- Other Orders
-
- Strict Intake and Output (I&O)
- Pain control: Tylenol PRN, additional medications at discretion of trauma provider.
- Be mindful of using aspirin or ibuprofen/NSAIDs and limit use when able.
- VTE prophylaxis per “VTE prophylaxis in Trauma Patients” (PRO 10) guidelines
-
- Angioembolization or Operative Exploration
-
- Should be considered in patients with signs of ongoing bleeding despite blood product transfusion
- Angioembolization is NOT indicated for contrast blush on admission CT without unstable vitals
- Operative exploration may be indicated when additional procedures or information are needed
- Patients presenting with or who develop peritonitis should undergo operative exploration.
-
- Discharge Criteria
-
- Hb/HCT stable x 2
- Acceptable pain control with oral pain medications
- Tolerating diet
- Vital signs within normal limits
-
- Admission Level of Care
-
- Late Presentation
-
- Management of stable patients presenting 24-48 hours post injury is at the discretion of the trauma surgeon and may be based on the reason for finally seeking care (pain, ileus, etc.)
- Consider observation for serial exams vs discharge home with follow up and ground level activity.
- Hemoglobin rechecks are optional and based on clinical status
- Diet and activity restrictions are based on clinical status
-
- Repeat Imaging
-
- Routine follow-up imaging is not required. Decision to obtain repeat imaging should be based on clinical status of patient and at discretion of trauma attending.
-
- Post splenectomy vaccines
-
- Patients undergoing splenectomy as management of their splenic injury should obtain the following vaccines prior to discharge or at 14 days post-op (whichever date comes first)
-
- Quadravalent meningococcus (Menactra or Menomune)
- Pneumococcus (Pneumovax 23)
- H.influenzae B (HIB, ActHIB)
- Viral influenza vaccine (depending on time of year)
-
- Patients undergoing splenectomy as management of their splenic injury should obtain the following vaccines prior to discharge or at 14 days post-op (whichever date comes first)
-
Follow-up Care:
- Upon discharge from hospital, patient may return to school and resume ground level activities with restrictions as noted below:
-
- Grade of Injury + 2 weeks = # weeks of activity restrictions (for example: Grade 2 injury + 2 weeks = 4 weeks of activity restrictions)
- Activity restrictions include: no gym/PE, recess, playground play, sports, no wheeled equipment, manual labor, farm labor, large animal care, or other activities where one could fall/sustain blow to abdomen.
-
- Patient should be instructed to call trauma surgery with any increasing pain, pallor, dizziness, vomiting, worsening shoulder pain, GI bleeding or black tarry stools, or jaundice.
- Follow-up in trauma surgery clinic:
-
- Grade 1 and 2 injuries = 2 weeks or with a follow up phone call
- Grade 3, 4, or 5 injuries or those undergoing operative/IR intervention = 2 weeks.
-
- Routine follow-up imaging is not required. Repeat imaging should be based on clinician determination and clinical situation.
- For kidney injuries, refer to primary care provider/pediatrician for ongoing blood pressure monitoring.
Outcome Measures and Guideline Adherence:
- Time to OR/IR and interventions for all hemodynamically unstable patients and patients failing non-operative management will be tracked through our performance improvement process.
- Adult guidelines for management of blunt solid organ injuries
- Guidelines For Imaging the Pediatric Trauma Patient
- Massive Transfusion for Trauma Guidelines (PRO 10)
Key Contributors:
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Abby Josef, MD | Division of Acute Care Surgery, Faculty | Reviewer
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Coordinator | Reviewer
Last updated:
· August, 2024
References:
- Williams RF, Grewal H, Jamshidi R et al. Updated APSA guidelines for the management of blunt liver and spleen injuries. J Pediatr Surg. 2023; 58:1411-1418.
- Gates RL, Price M, Cameron DB, et al. Non-operative management of solid organ injuries in children: an American pediatric surgical association outcomes and evidence based practice committee systemic review. J Pediatr Surg.2019 Aug: 54(8):1519-1526.
- Linnaus MR, Langlais ME, Garcia NM, et al. Failure of nonoperative management of pediatric blunt liver and spleen injuries: A prospective Arizona-Texas-Oklahoma-Memphis-Arkansas Consortium Study. J Trauma and Acute Care. 2017; 82(4):672-679.
Appendix/supplemental materials:
- Updated American Pediatric Surgical Association (APSA) Blunt Liver/Spleen Injury Guidelines
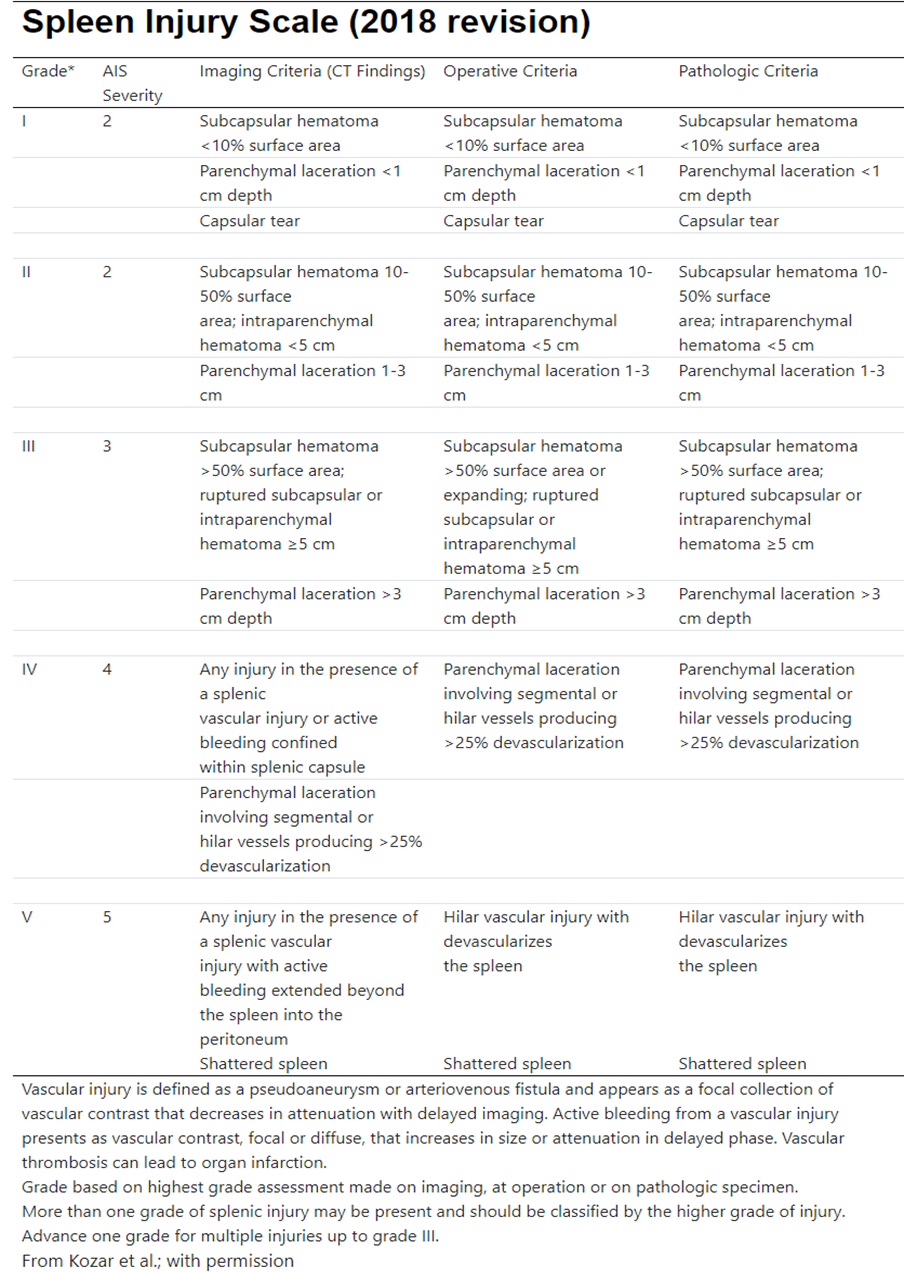
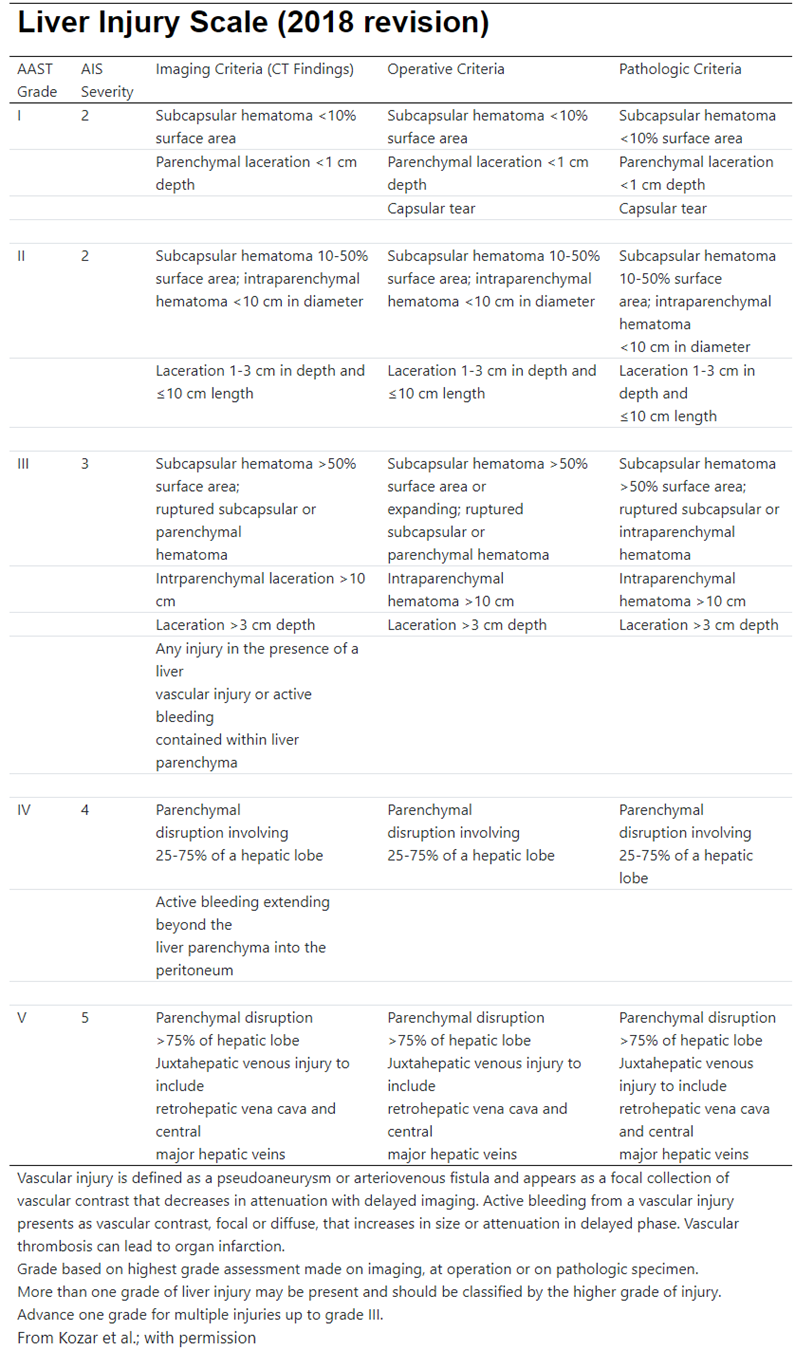
2. AAST Injury Grading Scales