Management of Pediatric Pelvic Fractures
Purpose:
Provide guidance on the initial evaluation and management of pediatric trauma patients with pelvic fractures.
Background:
Injures to the pelvis range from benign to life threatening. They include pelvic ring fractures, acetabular fractures, avulsion, and iliac wing fractures. The pelvis in children consists of high cartilaginous volume with greater elasticity at the sacroiliac joints and symphysis. Therefore, the pediatric pelvis is less prone to fracture and more able to dissipate a relatively large amount of energy. Most pediatric pelvic injuries are due to high-energy blunt trauma, which increases the likelihood of concomitant injuries to the head, chest, abdomen, and extremities.
Guideline Inclusion Criteria:
- Pediatric trauma patients age 18 years and younger with confirmed or suspected pelvic fractures
Guideline Exclusion Criteria:
- Trauma patients >18 years of age
Practice Management Guidelines:
- Orthopedic surgery will evaluate the patient within 30 minutes of consultation request; interventional radiology (IR) should be notified if there is any consideration for embolization.
- Initial evaluation
-
- Patient should be assessed and managed per ATLS guidelines. Physical examination should be performed by the trauma team in conjunction with the orthopedic team to specifically include:
-
- Urologic/vaginal exam
- Perineum exam
- Rectal exam
-
- An AP pelvis x-ray will be obtained in the trauma bay. The decision to forego AP pelvis x-ray and proceed directly to CT imaging is at the discretion of the trauma surgery attending.
- Pediatric trauma patients that require pelvic stabilization via binder or sheet are limited to: unstable pelvic fracture and hemodynamically unstable patient
-
- This includes patients who arrived hemodynamically unstable and have since stabilized.
- The pelvic binder or sheet should be placed at the level of the greater trochanters
- Patients who arrive to the trauma bay with a pelvic binder or stabilization sheet already in place should not have it removed until either AP pelvis x-ray is obtained to determine necessity, or unless directed by Orthopedic Surgery.
-
- It is acceptable to briefly remove the binder or stabilization sheet for adequate patient assessment.
-
-
- CT scan of the pelvis, including reconstructions, are obtained to evaluate for associated injuries.
- Initial evaluation should include determination if a urinary catheter is necessary.
-
- The Orthopedic Surgery team will include any recommendations for urinary catheterization in the consult note, and either Orthopedic Surgery or Trauma Surgery will place the order for urinary catheter in the electronic medical record.
- Timely urinary catheter insertion is essential. Any barriers to insertion should be promptly escalated to Orthopedic Surgery or Trauma Surgery.
- Questions related to permissible patient positioning during urinary catheter insertion should be directed to Orthopedic Surgery. If there are difficulties in obtaining proper positioning or if there is concern related to fractures as it relates to positioning, Orthopedic Surgery may be contacted for bedside assistance.
- Consider urology consult if there are concerns related to urethral injury or if urinary catheterization attempts are unsuccessful.
- External catheters, such as Pure Wick, are not an acceptable substitution and should not be utilized in acute pelvic fracture management.
- Mobile patients without activity restrictions may utilize a bedpan.
-
- Patient should be assessed and managed per ATLS guidelines. Physical examination should be performed by the trauma team in conjunction with the orthopedic team to specifically include:
-
- Management is based upon hemodynamic stability
-
- Ultimate decision for fracture treatment is determined by the Orthopedic Surgeon
- Volume resuscitation with appropriate blood products and maintenance of core temperature must be continued during all phases of resuscitation. Activation of Massive Transfusion Protocol (MTP) will be utilized as indicated per policy (PRO 09- Massive Transfusion in Trauma Guidelines). Blood products will be administered via rapid transfuser.
- For patients in a pelvic binder:
-
- Repeat AP pelvic x-ray should be obtained to assess reduction
- Binder should not remain in placed for longer than 48 hours unless there are extenuating circumstances that prevent operative intervention.
- Skin checks should be performed by the orthopedic surgery service ever 12 hours while the binder is in place, with removal of the binder ever 24 hours for more thorough skin check (maintaining precautions to prevent movement of the pelvis).
- Skeletal traction may be placed at the discretion of the orthopedic surgery attending.
-
- For hemodynamically unstable patients despite adequate resuscitation and/or patients with evidence of contrast extravasation on CT imaging related to pelvic fractures, consider consultation of IR for possible angioembolization.
-
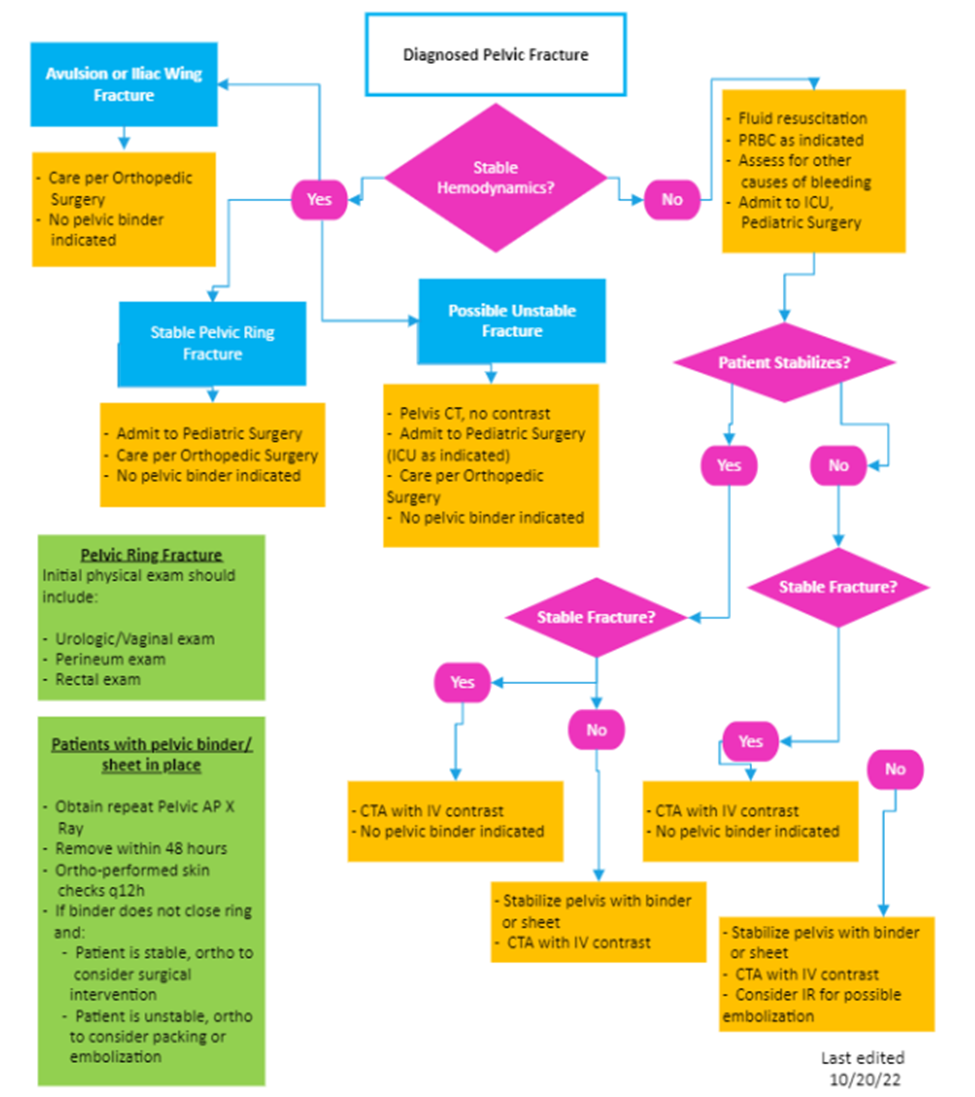
Pediatric Pelvic Fracture Pathway
Key Contributors:
- Emily Cantrell, MD | Division of Acute Care Surgery, Faculty | Principle Author
- Lora Hofstetter, MSN, RN, CCRN, C-NPT | Pediatric Trauma Program Manager | Co-Author
- Sara Putnam, MD, ABOS MD| Department of Orthopedic Surgery, Faculty | Reviewer
Last updated:
· July, 2024
References:
- Coccolini, F. (2017) Pelvic Trauma: WSES classification and guidelines, World Journal of Emergency Surgery, 12(5), 1-18.
- DeFrancesco CJ, Sankar, WN. (2017). Traumatic pelvic fractures in children and adolescents. Seminars in Pediatric Surgery, 26(1), 27-35.
- Hermans E, Cornelisse ST, Biert J, et al. (2017) Paediatric pelvic fractures, how do they differ from adults? Journal of Children’s Orthopeadics, 11, 49-56.
- Swaid F, Peleg K, Alfici R, et al. (2017). A comparison study of pelvic fractures and associated abdominal injuries between pediatric and adult trauma patients. Journal of Pediatric Surgery, 52, 386-389.
- Swenson SJ, Otsuka NY. (2022) Pelvic Fractures. Pediatric Orthopedic Society of North America. Pelvic Fractures | Pediatric Orthopaedic Society of North America (POSNA).
- Tosounidis TH, Sheikh H, Giannoudis PV. (2015). Pelvic fractures in paediatric polytrauma patients: Classification, concomitant injuries and early mortality. The Open Orthopedics Journal. 9(1), 303-312.