e-FAST for Trauma
Purpose
To standardize the application of e-FAST in the seriously injured patient, the technique employed, and the quality of standards by which they are retrospectively evaluated.
Background
e-FAST is a valuable diagnostic tool in the evaluation of traumatically injured patients that is able to detect life threatening inra-abdominal hemorrhage, pericardial effusion and hemo/pneumothoraces. An e-FAST exam is non-invasive, does not expose the patient to radiation, can rapidly be performed concurrently with other resuscitative measures, and is repeatable. e-FAST has a sensitivity between 73-88%, a specificity between 98-100%, and an accuracy of 96-98%.
Indications for an e-FAST Exam at UNMC/Nebraska Medicine
- Hemodynamically unstable patients as defined by a systolic blood pressure <90 mmHg for adults and <70mmHg + (2x age in years) for pediatric patients.
- At the discretion of the Emergency Medicine or Trauma attending.
Patients in whom e-FAST should strongly be considered
- Pregnant patients
In these special patient populations, if an e-FAST is performed:
- a repeat abdominal ultrasound should be performed 4 hours after the initial e-FAST or sooner if the patient becomes hypotensive.
- a repeat hemoglobin at the time of repeat ultrasound
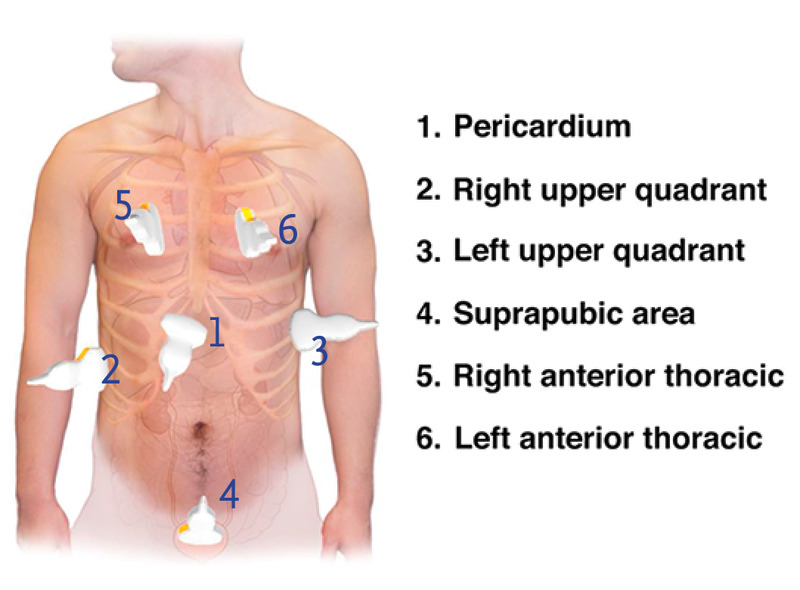
Six views of a complete e-FAST Exam
- pericardial or subxiphoid view
- Right upper quadrant: Lung base and hepatorenal recess
- Left upper quadrant: Lung base and splenorenal recess
- Pelvic: suprapubic view of bladder/Pouch of Douglass
- Right anterior thorax
- left anterior thorax
Ordering and Documentation of e-FAST exams
For all patients undergoing an e-FAST exam for trauma:
- Place an order in the electronic medical record (EPIC) for an e-FAST exam (POC ED US E-FAST, aka FAST)
- A procedure note will be documented by the provider performing the exam, including indication and interpretation of images.
-
- the performance of an e-FAST, the indication for exam and results of the exam should also be documented in the trauma H&P.
-
- Images will be saved with the patient's MRN.
Internal review of e-FAST exams:
The patients in whom e-FAST exams are indicated will be queried and the percentage of those receiving e-FAST exams reported. The documentation, image views and quality, and interpretation of images will be reviewed. Findings will be compared with CT or operative findings. Data will be presented at the monthly Performance Improvement Patient Safety (PIPS) meeting.
References
- AIUM Practice Parameter for the Performance of the Focused Assessment with Sonography for Trauma (FAST) Examination. American Institute of Ultrasound Medicine in collaboration with the American College of Emergency Physicians. http://www.aium.org/resources/guidelines/fast.pdf.
- Branney SW, Moore EE, Cantrill SV, et al. Ultrasound based key clinical pathway reduces the use of hospital resources for the evaluation of blunt abdominal trauma. J Trauma 42:1086-1090, 1997.
- Healey MA, Simons RK, WInchell RJ, et al. A prospective evaluation of abdominal ultrasound in blunt trauma: Is it useful? J Trauma 40:875-883, 1996.
- Glaser K, Tschmelitsch J, Klingler P, et al. Ultrasonography in the management of blunt and thoracic trauma. Arch Surg 129:743-747, 1994.
- Liu M, Lee CH, P'eng FK. Prospective comparison of diagnostic peritoneal lavage, computed tomographic scanning and ultrasonography for the diagnosis of blunt abdominal trauma. J Trauma. 35:267-270 1993.
- Boulanger BR, McLellan BA, Brenneman FD, et al. Emergent abdominal sonography as a screening test in a new diagnostic algorithm for blunt trauma. J Trauma. 40;867-874, 1996.
- Boulanger BR, Brenneman FD, McLellan BA, et al. A prospective study of emergent abdominal sonography after blunt trauma. J Trauma. 39;325-330, 1995.
- Ma OJ, Kefer MP, Mateer JR, et al. Evaluation of hemoperitoneum using single vs multiple ultrasonographic examination. Acad Emerg Med. 2:581-586, 1995.
- Rozycki GS, Oshsner MG, Jaffin JH, et al. Prospective evaluation of surgeons' use of ultrasound in the evaluation of trauma patients. J Trauma. 34:516-527, 1993.
- Smith SR, Kern SJ, Fry WR, et al: Institutional learning curve of surgeon-performed trauma ultrasound. Arch Surg. 133:530-536, 1998.
- McKenney MG, Martin L, Lentz K, et al. 1000 consecutive ultrasounds for blunt abdominal trauma. J Trauma. 40:607-612, 1996.
- Kem SJ, Smith RS, Fry WR, et. al. Sonographic examination of abdominal trauma by senior surgical residents. Am Surg. 63:669-674, 1997.
- Rozycki GS, Ochsner MG, Schmidt JA, et al. A prospective study of surgeon-performed ultrasound as the primary adjuvant modality for injured patient assessment. J Trauma. 39;492-500, 1995.
- Ong A, McKenney MG, McKenney KA, et al. Predicting the need for laparotomy in pediatric trauma patietns on the basis of ultrasound score. J Trauma. 2003;54:503-508.
- Soudack M, Epelman M, Maor R, et al. Experience with focused abdominal sonography for trauma (FAST) in 313 pediatric patietns. J Clin Ultrasound. 2004;32(2):53-61.
- McPartland SJ, Jackson C-CA, Gilchrist BF. "Pediatric Blunt Trauma". Trauma, Critical Care and Surgical Emergencies. Eds. Rabinovici R, Frankel HL, Kirton O. London:Informa, 2010203-226. Print.
UNMC/NM Policy last updated
August, 2019
May, 2025