Isolated Hip Fracture Protocol
Section One: Timing and Care Sequence:
1. Presentation to the Emergency Room
a. Assessment by the ED
b. Radiographs
i. Low AP pelvis, AP of affected hip, AP and lateral of affected femur
ii. MRI indicated if high suspicion but no clear fracture on x-ray, CT scan if MRI not available
2. Admission and Consultation
a. Patient admitted to Trauma
After tertiary survey
i. Trauma remains primary and SCM signs off
ii. Trauma signs off, Ortho takes primary, SCM remains on case
Trauma provider re-assigns primary treatment team so that all teams are aware of responsibilities.
b. Ortho consult (called by Trauma provider)
c. SCM consult (called by Trauma provider)
d. Pain consult - Ortho confirms with patient they consent to a block; then calls APS (@ 402-650-9676) for FIB to be done within 4 hours.
e. DEM consult (L. Armas will be contacted by Ortho)
f. consider palliative care consult- can be consulted by any service
g. SW consult (call not needed, just order)
h. PT/OT consult on admission but not to begin evaluation or treatment until the morning after surgery. If arthroplasty, pt will have posterior hip precautions in place
i. Foley only if clinically indicated
3. Orders
a. Preoperative labs drawn
i. CBC, CMP, PT/INR/PTT
ii. Type and Screen. If Hgb < 8 Type and Cross.
iii. Vitamin D: 25(OH)D level **Need to specify mass spect method
b. Chest radiograph if clinically indicated (hx of heart or lung problems or sx)
c. ECG if clinically indicated (hx of heart problems or new sxs)
d. Pain Control
i. Fascia Iliac block* see protocol below (The Ortho provider should call the Anesthesia Acute Pain Service 24/7 @ 402-650-9676 to notify them of the patient). Block should be placed within 4 hrs. of APS notification. (Catheter to be removed at end of OR case)
ii. Tylenol 1000mg TID scheduled; 650mg po TID if history of liver disease
iii. Celebrex 100mg BID scheduled
iv. If age>70, start Oxycodone 2.5mg po Q 3 hours prn, Dilaudid 0.4mg Q2hour prn severe pain
v. If age<70, start Oxycodone 5mg po Q 3 hours prn, Dilaudid 0.6 mg Q2 hours prn severe pain
vi. Weight-bearing Orders – toe touch weight-bearing
vii. Activity as tolerated
e. Warfarin
i. Hold warfarin
ii. If arthroplasty planned, give Vitamin K 2.5 mg IV x1 ASAP (Do not wait for labs)
f. For patients admitted in the evening, keep NPO in anticipation of OR next day, for patients admitted in the morning keep NPO for possibility of OR the same day. Allow Ensure Pre- Surgery CHO drink evening before; consume before midnight
g. Hold ACE-Is and ARBs at admission to decrease the risk of intraoperative hypotension, restart POD #1
Continue ACE-Is and ARBs if systolic BP > 160
Continue ACE-Is and ARBs if LVEF know to be < 30%
h. Continue beta-blockers/rate control medications
i. Order 2000 IU Vitamin D3 daily
4. Patient taken to OR: Goal is patient in the OR next day after admission (Goal: 24-48 hrs.)
5. Postoperative Course
a. Standard postoperative antibiotics x 1 dose (orthopedics orders)
b. Postop CBC, BMP, other labs as needed or based on medical comorbidities, not routine
c. Evaluate pre op anticoagulation medication. Consider Lovenox 30 mg subQ q 12 hours (pharmacy consult for dosing) for VTE prophylaxis x 4 weeks to start POD#1
d. Calcium carbonate 1000 mg (400 mg of elemental calcium) start once daily with food
e. If arthroplasty - nursing communication order for arthroplasty- input full order set for mobility
f. If present, remove Foley on POD #1, straight cath. if retention
g. Goal discharge to home or facility is < 48 hours
h. Mobility: Encourage Dangle within 6-8 hours of surgery with QID ambulation beginning on POD 1, activity as tolerated, WB as tolerated
i. Diet: Patient may resume normal diet post op day 0, protein supplements with each meal/snacks
j. Patient up in chair for all meals x 3
k. Multimodal pain regimen to include combination of Tylenol/NSAIDs
iii. Tylenol 1000mg TID scheduled; 650mg po TID if history of liver disease
iv. Celebrex 100mg BID scheduled
v. Narcotic regimen per Arthroplasty Order Set
Oral Opioids - Moderate/Severe Pain (GFR 30 or less, age 79 yrs. or less)
oxycodone 5 mg, oral, every 2 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 12 hours PRN, moderate pain, severe pain
IV Opioids - Breakthrough Pain (GFR 30 or less, age 79 yrs. or less)
hydromorphone 0.5 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
Oral Opioids - Moderate/Severe Pain (GFR 30 or less, age 80 yrs. or more)
oxycodone 2.5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 12 hours PRN, moderate pain, severe pain
IV Opioids - Breakthrough Pain (GFR 30 or less, age 80 yrs. or more)
hydromorphone 0.2 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
Oral Opioids - Moderate/Severe Pain (GFR more than 30, age 79 yrs. or less)
oxycodone 5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
morphine 7.5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 6 hours PRN, moderate pain, severe pain
IV Opioids - Moderate/Severe Pain (GFR more than 30, age 79 yrs. or less)
morphine 2 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds OR
hydromorphone 0.5 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
Oral Opioids - Moderate/Severe Pain (GFR more than 30, age 80 yrs. or more)
oxycodone 2.5 mg, oral, every 4 hours PRN, moderate pain, severe pain OR
tramadol 50 mg, oral, every 6 hours PRN, moderate pain, severe pain
IV Opioids - Moderate/Severe Pain (GFR more than 30, age 80 yrs. or more)
morphine 1 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds OR
hydromorphone 0.2 mg, intravenous, every 2 hours PRN, breakthrough pain OR moderate to severe pain and unable to take oral pain meds
l. Vaccine reconciliation
m. Use of Recovery Milestone Checklist while in hospital
n. Develop Discharge Criteria
o. Gum chewing (sugar free) TID for 20 minutes
p. Utilize Static Meds Initiative (Early AM Meds to Beds delivery program)
6. Discharge: (3 appointments need to be made: bone health, orthopedics, primary care,
a. BONE HEALTH: with Dr. Armas
b. ORTHOPEDICS FOLLOW UP: Orthopedics team resident schedules Orthopedic Surgery
c. PRIMARY CARE: Primary team makes appointment with PCP within 2weeks
d. Primary service ensures detailed post-op instructions
i. Wound care/dressing
ii. PT/Activity
iii. Follow up anticipatory guidance
iv. Specific instructions on when to call the doctor (PCP vs Orthopedic Surgeon)
v. Updated medication list
vi. Continue calcium and vitamin D if they were on admission list or started inpatient.
Section Two: Specific Considerations for Anesthesia and Surgery
1. Anesthesia PreOp
a. Consider Neuraxial in all patients
b. Tranexemic Acid 1 gm IV at the beginning and end of the case
c. Any specific concerns for contraindications to surgery must be discussed between Attendings
2. Surgery
a. Arthroplasty: See pathway for anticoagulation
Case scheduled as Hip hemi-arthroplasty possible total hip.
b. CRPP/ORIF: See pathway for anticoagulation
Case scheduled as CRPP Hip, IMN Hip Fracture, Antegrade Femur Nail
c. Tranexemic Acid 1 gm IV at time of incision- same as spine
d. Standard preop antibiotics.
Section Three: Anticoagulation, Co-Morbidities and Specific Conditions
A. Anticoagulation
1. Anticoagulation for Arthroplasty (determined by Ortho upon eval in ED)
a. Antiplatelet agents
i. Continue Aspirin if history of CAD, stroke, TIA, or PAD. Irreversible antiplatelet effect persists for at least 5 days. If taking > 81 mg daily, reduce to 81 mg daily
ii. Discontinue P2Y12 inhibitors (clopidogrel, ticagrelor, or prasugrel) unless the patient is in the high risk window following coronary stent placement (policy MS54): Acute coronary syndrome within the past 12 months, bare metal stent in the past 1 month, or drug-eluting stent in the past 6 months
b. Warfarin (policy MP11)
i. If initial INR > 3, give additional Vitamin K 2.5 mg IV
ii. If initial INR > 1.5, type and cross for 2-4 units FFP
iii. Re-check INR 12 hours after vitamin K dose
iv. Goal INR for OR is 1.5 or less
v. Can proceed with surgery if INR 1.8 or less and patient can get FFP on the way to the OR (patient will receive GETA)
vi. Consider K Centra
d. DOACs (dibigatran, rivaroxaban, apixiban, edoxaban) (policy MS55)
i. Hold, clearly document time of last dose.
ii. Timing of surgery following last dose of DOAC
a. Factor Xa inhibitor (apixaban, edoxaban, rivaroxaban)
1. eGFR ≥ 30 = 24 hours
2. eGFR < 30 = 48 hours
b. Dabigatran
1. eGFR ≥ 80 = 24 hours
2. eGFR 30-80 = 48 hours
3. eGFR < 30 = 72 hours
c. Risks and benefits should be weighed by teams (ortho, medicine, geriatrics, and anesthesia) if delay > 24 hours is being considered.
2. Anticoagulation for ORIF/CRPP/IMN (Not arthroplasty)
a. Antiplatelet agents
i. Continue Aspirin if history of CAD, stroke, TIA, or PAD. Irreversible antiplatelet effect persists for at least 5 days. If taking > 81 mg daily, reduce to 81 mg daily
ii. Continue P2Y12 inhibitors (clopidogrel, ticagrelor, or prasugrel) if any of the following. Irreversible antiplatelet effect persists for at least 5 days. Acute coronary syndrome within the past 12 months, any cardiac stent, any peripheral artery stent, history of stroke or TIA
b. Warfarin
i. If initial INR > 3.0, administer Vitamin K 2.5 mg IV x 1
ii. If initial INR > 3.0, type and cross for 2-4 units FFP
iii. Goal INR for OR is 3.0 or less
iv. Can proceed with surgery if INR 3.0 or less
c. DOACs (dibigatran, rivaroxaban, apixiban, edoxaban)
i. Hold
ii. Do not delay surgery
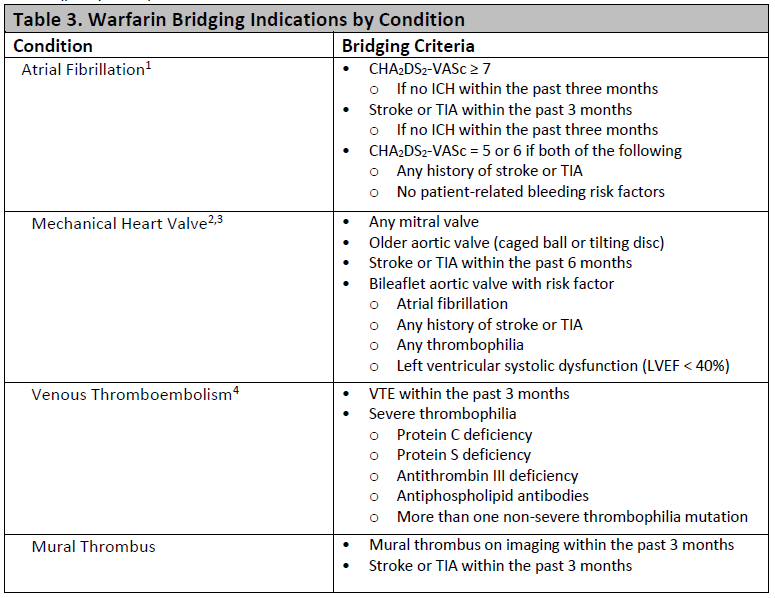
3. Bridging Anticoagulation
a. Bridging therapy applies only to patients taking warfarin
b. Bridging therapy with heparin indicated if any of the very high risk conditions below (policy MS55):
B. Comorbidity
Only unstable conditions should delay surgery. Evaluation of stable conditions must be completed within 24 hours of admission. If delay greater than 24 hours is anticipated, discussion between anesthesiology, Trauma, and hospital medicine is required within 8 hours of admission.
Statement of surgical readiness: One of these statements must be included in the SCM consultation report. If statement c is chosen, a discussion with anesthesiology, Trauma, and orthopedic surgery is required.
a. The patient is medically appropriate to proceed to surgery without further evaluation or management.
b. The patient will be medically appropriate to proceed to surgery when …
c. The patient is not medically appropriate to proceed to surgery. Delay or cancellation recommended.
Indications for surgical delay
a. Active Acute Coronary Syndrome (EKG changes or elevated troponin)
i. Cardiology consult
ii. Delay OR until optimized
b. Unstable Arrhythmia (hypotension or significantly uncontrolled)
i. Cardiology consult
ii. Delay OR until optimized
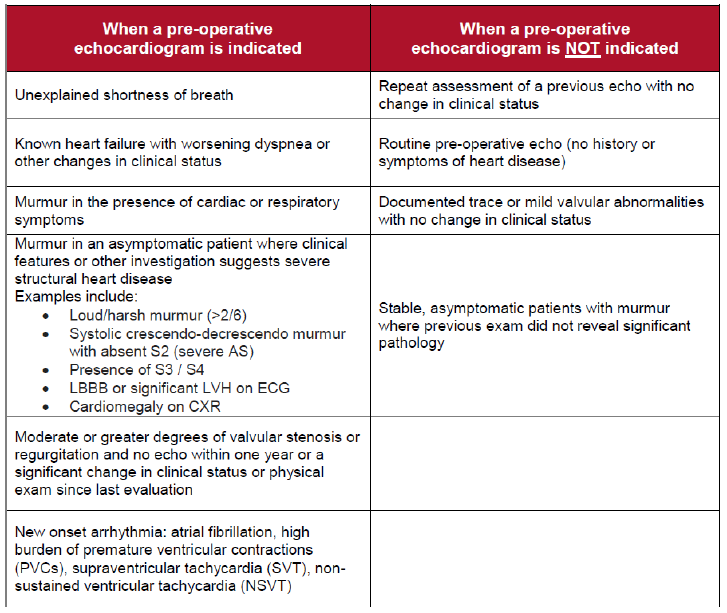
c. Decompensated CHF with new symptoms: see “Patients requiring an echo”
i. Obtain TTE,
ii. Cardiology consult
iii. delay OR until optimized
d. Acute respiratory failure
i. Obtain ABG for diagnosis of acute respiratory failure
a. SaO2 < 89
b. PO2 < 55
c. PCO2 > 55 with pH < 7.35
ii. Obtain pa/lat CXR, procalcitonin, b-natriuretic peptide
iii. Delay OR until optimized
e. Sepsis
i. Follow sepsis bundle for evaluation and treatment
ii. Delay OR until optimized
Other Comorbidity (not a reason to delay surgery)
a. Cardiac
i. Revised Cardiac Risk Index (RCRI) score: {NUMBERS 0 TO 6)
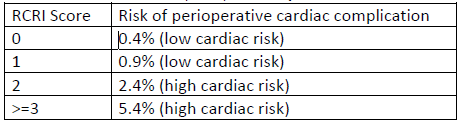
ii. Based on RCRI score and exercise tolerance:
a. Beta blockade indicated: continue if currently taking
b. Statin therapy indicated: continue if currently taking, start if indicated based on 10-year ASCVD risk
c. Inpatient telemetry monitoring recommendation: indicated if significant arrhythmia or RCRI score > 2
iii. Echocardiogram indications
b. Pulmonary
i. STOP-BANG score, OSA risk: (high risk if STOP-BANG > 5 or if known OSA not treated with CPAP)
ii. Management of high risk patients
a. Continuous oximetry
b. Continuous elevation of the head of the patient's bed
c. Complete avoidance of benzodiazepines and sedatives
iii. Management of home CPAP while inpatient
a. Begin CPAP therapy at home settings in the PACU and don't remove it for 48 hours unless the patient is eating or is out of bed.
b. After 48 hours, CPAP with sleep only
c. Diabetes or hyperglycemia (glucose > 180)
i. Avoid dextrose-containing IV fluid
ii. Hold oral diabetes medications while inpatient
iii. Institute basal-bolus insulin therapy
iv. Goal glucose 100-180
d. Hypertension
i. See above for ACEI and ARB management
ii. Continue other antihypertensive medication without interruption
iii. Goal BP < 180/105
e. Delirium
i. High risk for delirium if any of the following
a. Diagnosis of dementia or mild cognitive impairment
b. History of delirium
c. Age ≥ 80 years
e. Transfer from a facility
ii. Prevention of delirium in high risk patients
a. Avoid sedatives (including benzodiazepines and sleep aids) and anticholinergics (including scopolamine patch)
b. Minimize opioids as able.
c. Frequent re-orientation and opening of window shades during the day recommended.
d. Allow sleep
f. Stress dose steroids
i. Continue the patient's home oral steroid regimen without interruption perioperatively
ii. If the patient takes > 7.5 mg prednisone (or equivalent dose of another steroid) daily, administer stress dose steroids. Hydrocortisone 100 mg IV in pre-op followed by 50 mg IV every 8 hours for 3 total doses.
g. Alcohol Use- see CIWA and Phenobarbital protocols
Key Contributors
Zach Bauman,
UNMC Division of Acute Care Surgery, 2024